



Novel Technique of Interproximal Enamel Reduction Based on Computer-Aided Navigation Technique—An In Vitro Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Experimental Procedure
2.3. Interproximal Enamel Reduction Procedure
2.4. Digital Measurement Procedure
2.5. Statistical Tests
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sheridan, J.J. Air-rotor stripping. J. Clin. Orthod. 1985, 19, 43–59. [Google Scholar] [PubMed]
- Peck, H.; Peck, S. An Indexfor assessing tooth shape deviations as applied to the mandibular incisors. Am. J. Orthod. 1972, 61, 384–401. [Google Scholar] [CrossRef] [PubMed]
- Zachrison, B.; Nyoygaard, L.; Mobarak, K. Dental health assessed more than 10 years after interproximal enamel reduction of mandibular anterior teeth. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Stroud, J.L.; English, J.; Buschang, P.H. Enamel thickness of the posterior dentition: Its implications for nonextraction treatment. Angle Orthod. 1998, 68, 141–146. [Google Scholar]
- Chudasama, D.; Sheridan, J.J. Guidelines for contemporary air-rotor stripping. J. Clin. Orthod. 2007, 41, 315–320. [Google Scholar]
- Kailasam, V.; Rangarajan, H.; Easwaran, H.N.; Muthu, M.S. Proximal enamel thickness of the permanent teeth: A systematic review and meta-analysis. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 793–804.e3. [Google Scholar] [CrossRef]
- Baysal, A.; Uysal, T.; Usumez, S. Temperature rise in the pulp chamber during different stripping procedures. Angle Orthod. 2007, 77, 478–482. [Google Scholar] [CrossRef]
- d’Ornellas Pereira, J.C., Jr.; Weissheimer, A.; de Menezes, L.M.; de Lima, E.M.; Mezomo, M. Change in the pulp chamber temperature with different stripping techniques. Prog. Orthod. 2014, 15, 55. [Google Scholar] [CrossRef]
- Sehgal, M.; Sharma, P.; Juneja, A.; Kumar, P.; Verma, A.; Chauhan, V. Effect of different stripping techniques on pulpal temperature: In vitro study. Dent. Press J. Orthod. 2019, 24, 39–43. [Google Scholar] [CrossRef]
- Gazzani, F.; Bellisario, D.; Fazi, L.; Balboni, A.; Licoccia, S.; Pavoni, C.; Cozza, P.; Lione, R. Effects of IPR by mechanical oscillating strips system on biological structures: A quantitative and qualitative evaluation. Prog. Orthod. 2023, 24, 9. [Google Scholar] [CrossRef] [PubMed]
- Kaaouara, Y.; Mohind, H.B.; Azaroual, M.F.; Zaoui, F.; Bahije, L.; Benyahia, H. In vivo enamel stripping: A macroscopic and microscopic analytical study. Int. Orthod. 2019, 17, 235–242. [Google Scholar] [CrossRef]
- Sarment, D.P.; Sukovic, P.; Clinthorne, N. Accuracy of implant placement with a stereolithographic surgical guide. Int. J. Oral Maxillofac. Implant. 2003, 18, 571–577. [Google Scholar]
- De Kok, I.J.; Thalji, G.; Bryington, M.; Cooper, L.F. Radiographic stents: Integrating treatment planning and implant placement. Dent. Clin. N. Am. 2014, 58, 181–192. [Google Scholar] [CrossRef]
- Gao, J.; He, J.; Fan, L.; Lu, J.; Xie, C.; Yu, H. Accuracy of reduction Depths of Tooth Preparation for Porcelain Laminate Veneers Assisted by Different Tooth Preparation Guides: An in vitro study. J. Prosthodont. 2022, 31, 593–600. [Google Scholar] [CrossRef]
- Arroyave Franco, M. Revista Universidad; EAFIT: Medellín, Colombia, 2011; Volume 44, pp. 68–83. [Google Scholar]
- Suga, M.; Asahina, S.; Sakuda, Y.; Kazumori, H.; Nishiyama, H.; Nokuo, T.; Alfredsson, V.; Kjellman, T.; Stevens, S.M.; Cho, H.S.; et al. Recent progress in scanning electron microscopy for the characterization of fine structural details of nano materials. Prog. Solid State Chem. 2014, 42, 1–21. [Google Scholar] [CrossRef]
- Eghiaian, F.; Rico, F.; Colom, A.; Casuso, I.; Scheuring, S. High-speed atomic force microscopy: Imaging and force spectroscopy. FEBS Lett. 2014, 588, 3631–3638. [Google Scholar] [CrossRef]
- Arango, C.; Paz Quintero, C. Technique for computerized measurement of occlusal areas and perimeters on standardized photographic images. Measurement technique and design of the photostandardizer. CES Dent. 1993, 6, 117–119. [Google Scholar]
- Richert, R.; Goujat, A.; Venet, L.; Viguie, G.; Viennot, S.; Robinson, P.; Farges, J.C.; Fages, M.; Ducret, M. Intraoral Scanner Technologies: A Review to Make a Successful Impression. J. Healthc. Eng. 2017, 2017, 8427595. [Google Scholar] [CrossRef] [PubMed]
- Conry, J.P.; Beyer, J.P.; Pintado, M.R. Technical note: An initial comparison of odontometric methods: Caliper versus computer guided profilometry. Am. J. Phys. Anthropol. 1992, 87, 231–233. [Google Scholar] [CrossRef] [PubMed]
- Sugsompian, K.; Tansalarak, R.; Piyapattamin, T. Comparison of the Enamel Surface Roughness from Different Polishing Methods: Scanning Electron Microscopy and Atomic Force Microscopy Investigation. Eur. J. Dent. 2020, 14, 299–305. [Google Scholar] [CrossRef] [PubMed]
- ISO 14801:2016; Dentistry. Implants. Dynamic Loading Test for Endosseous Dental Implants. ISO: Geneva, Switzerland, 2016.
- Comuzzi, L.; Tumedei, M.; Pontes, A.E.; Piattelli, A.; Iezzi, G. Primary Stability of Dental Implants in Low-Density (10 and 20 pcf) Polyurethane Foam Blocks: Conical vs. Cylindrical Implants. Int. J. Environ. Res. Public Health 2020, 17, 2617. [Google Scholar] [CrossRef]
- Renne, W.; Ludlow, M.; Fryml, J.; Schurch, Z.; Mennito, A.; Kessler, R.; Lauer, A. Evaluation of the accuracy of 7 digital scanners: An in vitro analysis based on 3-dimensional comparisons. J. Prosthet. Dent. 2017, 118, 36–42. [Google Scholar] [CrossRef]
- Medina-Sotomayor, P.; Pascual-Moscardo, A.; Camps, A.I. Accuracy of 4 digital scanning systems on prepared teeth digitally isolated from a complete dental arch. J. Prosthet. Dent. 2019, 121, 811–820. [Google Scholar] [CrossRef]
- Triduo, M.; Zubizarreta-Macho, Á.; Pérez-Barquero, J.A.; Guinot Barona, C.; Alvarado Lorenzo, A.; Vicente-Galindo, P.; Albaladejo Martínez, A. A Novel Digital Technique to Quantify the Area and Volume of Enamel Removal after Interproximal Enamel Reduction. Appl. Sci. 2020, 9, 1098. [Google Scholar] [CrossRef]
- Sittikornpaiboon, P.; Arunjaroensuk, S.; Kaboosaya, B.; Subbalekha, K.; Mattheos, N.; Pimkhaokham, A. Comparison of the accuracy of implant placement using different drilling systems for static computer-assisted implant surgery: A simulation-based experimental study. Clin. Implant. Dent. Relat. Res. 2021, 23, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Bencharit, S.; Staffen, A.; Yeung, M.; Whitley, D., 3rd; Laskin, D.M.; Deeb, G.R. In Vivo Tooth-Supported Implant Surgical Guides Fabricated with Desktop Stereolithographic Printers: Fully Guided Surgery Is More Accurate Than Partially Guided Surgery. J. Oral Maxillofac. Surg. 2018, 76, 1431–1439. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Ding, Q.; Yuan, F.; Zhang, L.; Sun, Y.; Xie, Q. Accuracy of a chairside, fused deposition modeling three-dimensional-printed, single tooth surgical guide for implant placement: A randomized controlled clinical trial. Clin. Oral Implants Res. 2022, 33, 1000–1009. [Google Scholar] [CrossRef]
- Derksen, W.; Wismeijer, D.; Flügge, T.; Hassan, B.; Tahmaseb, A. The accuracy of computer-guided implant surgery with tooth-supported, digitally designed drill guides based on CBCT and intraoral scanning. A prospective cohort study. Clin. Oral Implants Res. 2019, 30, 1005–1015. [Google Scholar] [CrossRef] [PubMed]
- Pessoa, R.; Siqueira, R.; Li, J.; Saleh, I.; Meneghetti, P.; Bezerra, F.; Wang, H.L.; Mendonça, G. The Impact of Surgical Guide Fixation and Implant Location on Accuracy of Static Computer-Assisted Implant Surgery. J. Prosthodont. 2022, 31, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Ngamprasertkit, C.; Aunmeungthong, W.; Khongkhunthian, P. The implant position accuracy between using only surgical drill guide and surgical drill guide with implant guide in fully digital workflow: A randomized clinical trial. Oral Maxillofac. Surg. 2022, 26, 229–237. [Google Scholar] [CrossRef]
- Li, Z.Y.; Bai, H.F.; Zhao, Y.J.; Wang, Y.; Ye, H.Q.; Sun, Y.C. 3D Evaluation of Accuracy of Tooth Preparation for Laminate Veneers Assisted by Rigid Constraint Guides Printed by Selective Laser Melting. Chin. J. Dent. Res. 2020, 23, 183–189. [Google Scholar] [CrossRef]
- Jurado, C.A.; AlResayes, S.; Sayed, M.E.; Villalobos-Tinoco, J.; Llanes-Urias, N.; Tsujimoto, A. A customized metal guide for controllable modification of anterior teeth contour prior to minimally invasive preparation. Saudi Dent. J. 2021, 33, 518–523. [Google Scholar] [CrossRef]
- Johner, A.M.; Pandis, N.; Dudic, A.; Kiliaridis, S. Quantitative comparison of 3 enamel-stripping devices in vitro: How precisely can we strip teeth? Am. J. Orthod. Dentofac. Orthop. 2013, 143 (Suppl. S4), S168–S172. [Google Scholar] [CrossRef]
- Kalemaj, Z.; Levrini, L. Quantitative evaluation of implemented interproximal enamel reduction during aligner therapy. Angle Orthod. 2021, 91, 61–66. [Google Scholar] [CrossRef] [PubMed]
- De Felice, M.E.; Nucci, L.; Fiori, A.; Flores-Mir, C.; Perillo, L.; Grassia, V. Accuracy of interproximal enamel reduction during clear aligner treatment. Prog. Orthod. 2020, 21, 28. [Google Scholar] [CrossRef] [PubMed]
- Laganà, G.; Malara, A.; Lione, R.; Danesi, C.; Meuli, S.; Cozza, P. Enamel interproximal reduction during treatment with clear aligners: Digital planning versus OrthoCAD analysis. BMC Oral Health 2021, 21, 199. [Google Scholar] [CrossRef] [PubMed]
- Sarig, R.; Vardimon, A.D.; Sussan, C.; Benny, L.; Sarne, O.; Hershkovitz, I.; Shpack, N. Pattern of maxillary and mandibular proximal enamel thickness at the contact area of the permanent dentition from first molar to first molar. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 435–444. [Google Scholar] [CrossRef]
- Güth, J.F.; Runkel, C.; Beuer, F.; Stimmelmayr, M.; Edelhoff, D.; Keul, C. Accuracy of five intraoral scanners compared to indirect digitalization. Clin. Oral Investig. 2017, 21, 1445–1455. [Google Scholar] [CrossRef]
- Jivanescu, A.; Rotar, P.; Hategan, S.; Pricop, C.; Rus, R.; Goguta, L. Clinical Factors Influence the Trueness of Intra-oral Scanning. Eur. J. Prosthodont. Restor. Dent. 2019, 27, 51–55. [Google Scholar] [CrossRef]
- Abduo, J.; Elseyoufi, M. Accuracy of Intraoral Scanners: A Systematic Review of Influencing Factors. Eur. J. Prosthodont. Restor. Dent. 2018, 26, 101–121. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Gohil, A.; Barmak, A.B.; Gómez-Polo, M.; Pérez-Barquero, J.A.; Att, W.; Kois, J.C. Influence of ambient temperature changes on intraoral scanning accuracy. J. Prosthet. Dent. 2023, 130, 755–760. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Alonso Pérez-Barquero, J.; Zubizarreta-Macho, Á.; Barmak, A.B.; Att, W.; Kois, J.C. Influence of the Number of Teeth and Location of the Virtual Occlusal Record on the Accuracy of the Maxillo-Mandibular Relationship Obtained by Using An Intraoral Scanner. J. Prosthodont. 2023, 32, 253–258. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
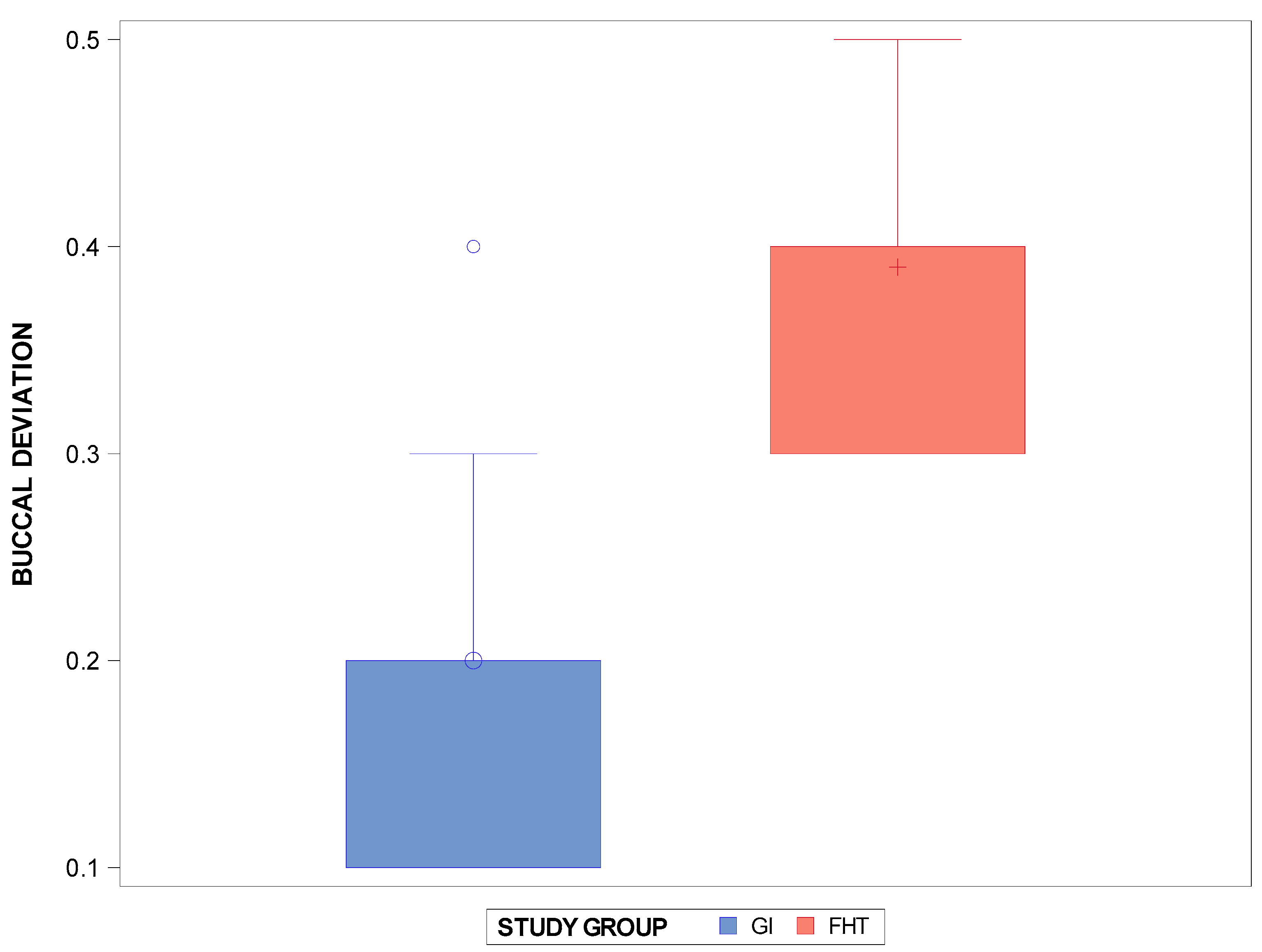
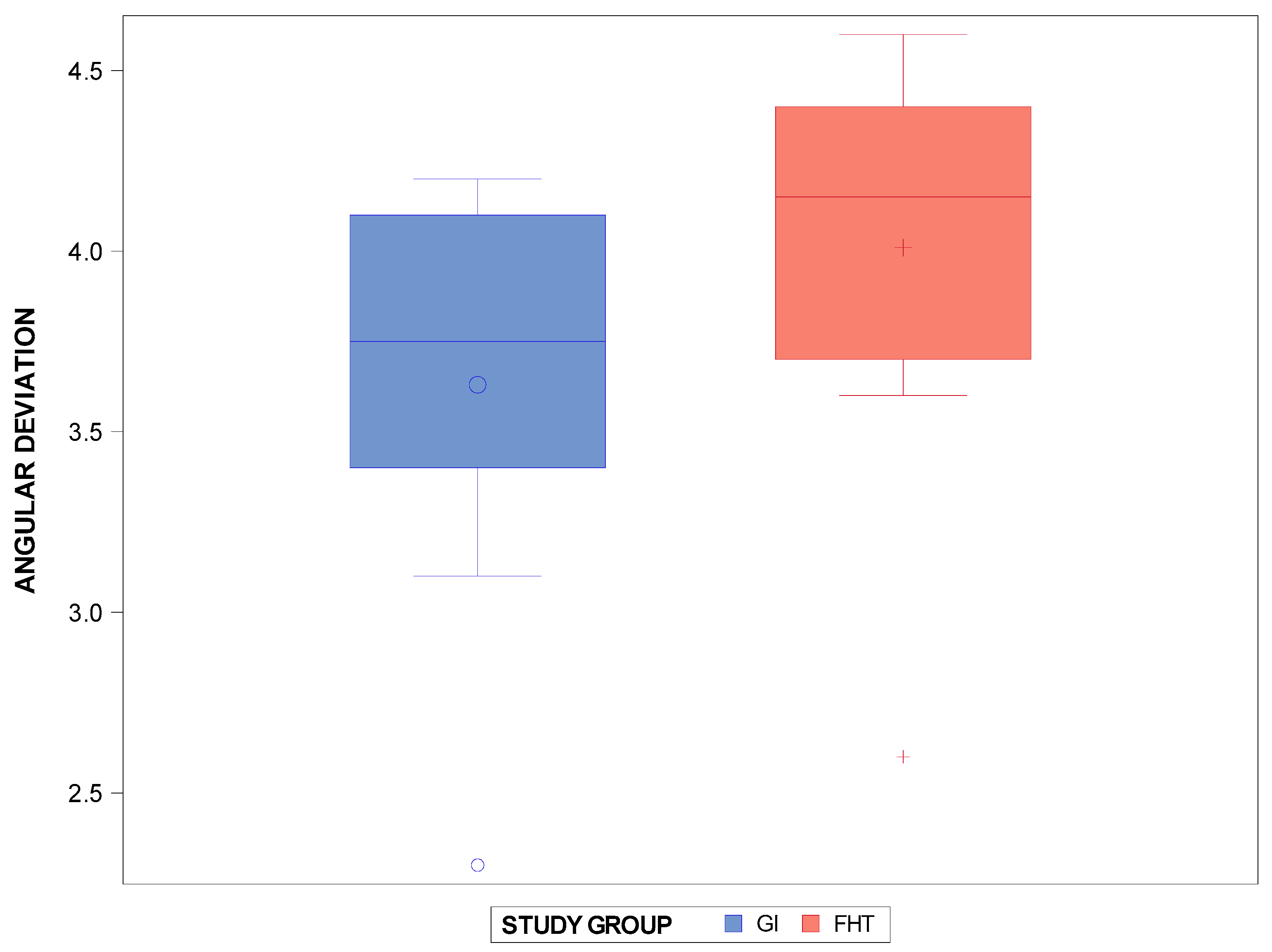
| Measure | Technique | n | Mean (mm) | SD (mm) | Minimum (mm) | Maximum (mm) |
|---|---|---|---|---|---|---|
| Buccal | GI | 100 | 0.20 | 0.09 | 0.10 | 0.40 |
| FHT | 100 | 0.39 | 0.07 | 0.30 | 0.50 | |
| Lingual/Palatal | GI | 100 | 0.24 | 0.11 | 0.10 | 0.40 |
| FHT | 100 | 0.58 | 0.9 | 0.40 | 0.70 | |
| Angular | GI | 100 | 3.63 | 0.58 | 2.30 | 4.20 |
| FHT | 100 | 4.01 | 0.60 | 2.60 | 4.60 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cotrina-Peregrín, M.D.; Arrieta-Blanco, P.; Aragoneses-Lamas, J.M.; Albaladejo Martínez, A.; Lobo Galindo, A.B.; Zubizarreta-Macho, Á. Novel Technique of Interproximal Enamel Reduction Based on Computer-Aided Navigation Technique—An In Vitro Study. J. Pers. Med. 2024, 14, 138. https://doi.org/10.3390/jpm14020138
Cotrina-Peregrín MD, Arrieta-Blanco P, Aragoneses-Lamas JM, Albaladejo Martínez A, Lobo Galindo AB, Zubizarreta-Macho Á. Novel Technique of Interproximal Enamel Reduction Based on Computer-Aided Navigation Technique—An In Vitro Study. Journal of Personalized Medicine. 2024; 14(2):138. https://doi.org/10.3390/jpm14020138
Chicago/Turabian StyleCotrina-Peregrín, María Dolores, Patricia Arrieta-Blanco, Juan Manuel Aragoneses-Lamas, Alberto Albaladejo Martínez, Ana Belén Lobo Galindo, and Álvaro Zubizarreta-Macho. 2024. "Novel Technique of Interproximal Enamel Reduction Based on Computer-Aided Navigation Technique—An In Vitro Study" Journal of Personalized Medicine 14, no. 2: 138. https://doi.org/10.3390/jpm14020138