
A Prospective Observational Study on the Role of Immunohistochemical Expression of Orphanin in Laryngeal Squamous Cell Carcinoma Recurrence
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
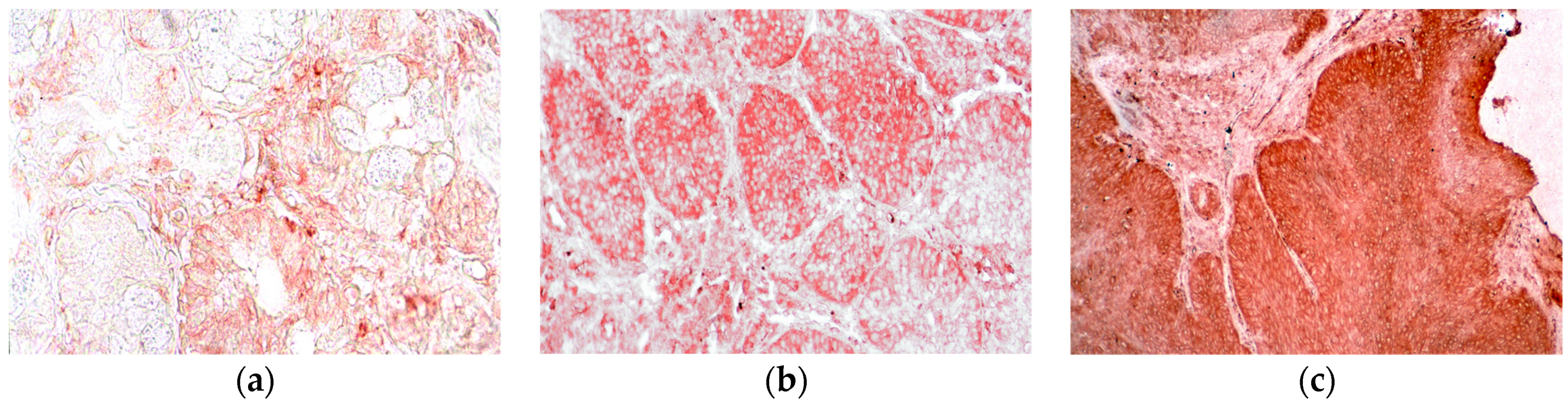
2.1. Histological Examination
2.2. Statistical Analysis
3. Results
3.1. Clinical-Pathological and Histological Characteristics of the Patients
3.2. N/OFQ and TNM Staging
3.3. N/OFQ and Grading
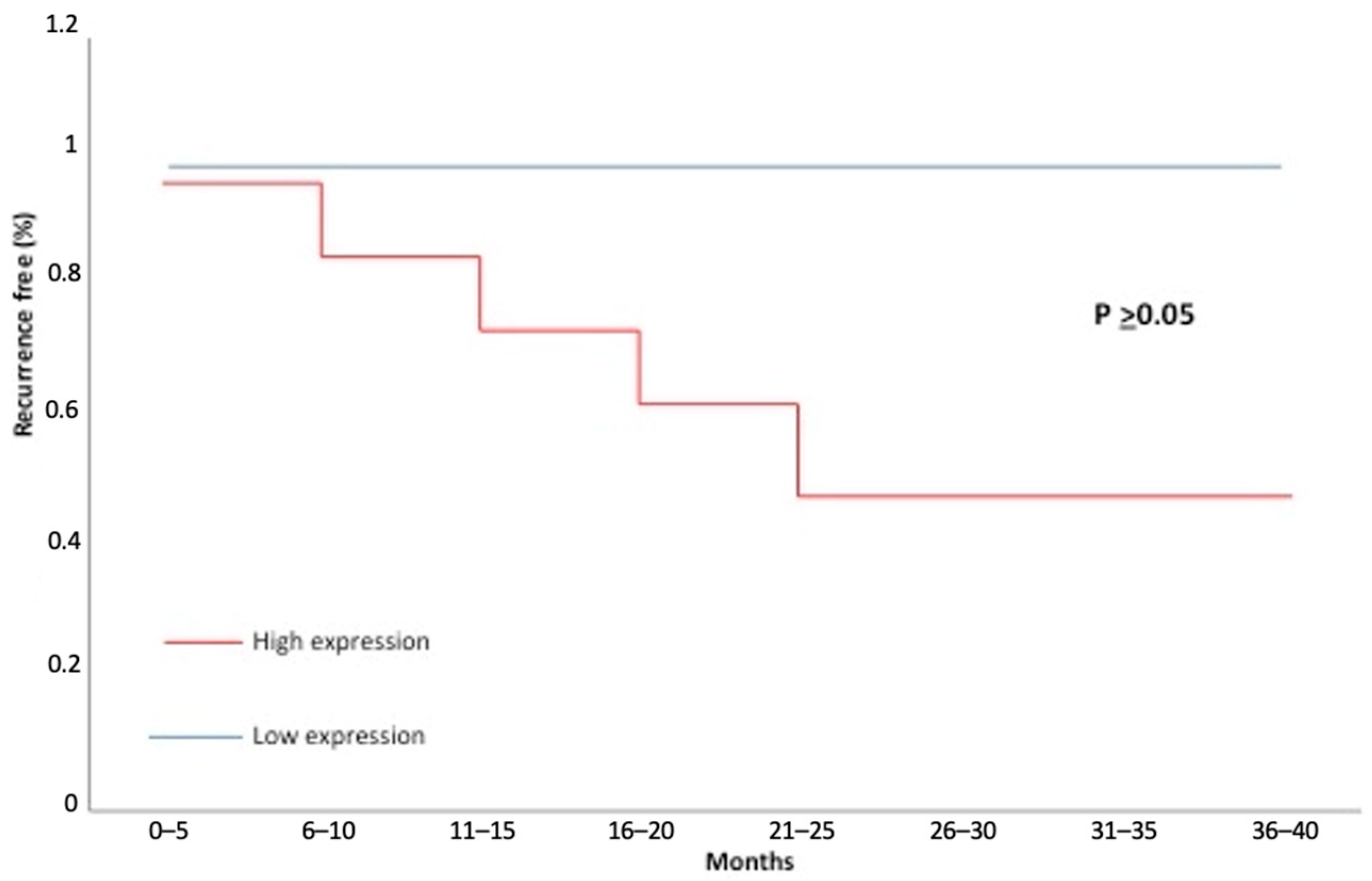
3.4. N/OFQ and Recurrences
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barnes, L.; Tse, L.L.Y.; Hunt, J.L.; Brandwein-Gensler, M.; Urken, M.; Slootweg, P.; Gale, N.; Cardesa, A.; Zidar, N.; Boffetta, P. Tumours of the hypopharynx, larynx and trachea: Introduction. In World Health Organization Classification of Tumours. Pathology and Genetics of Head and Neck Tumours; Barnes, L., Eveson, J., Reichart, P., Sidransky, D., Eds.; IARC Press: Lyon, France, 2005; pp. 111–117. [Google Scholar]
- Forastiere, A.; Koch, W.; Trotti, A.; Sidransky, D. Head-and-neck cancer. N. Engl. J. Med. 2001, 345, 1890–1900. [Google Scholar] [CrossRef]
- Shalev, U.; Erb, S.; Shaham, Y. Role of CRF and other neuropeptides in stress-induced reinstatement of drug seeking. Brain Res. 2010, 1314, 15–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinscheid, R.K.; Nothacker, H.P.; Bourson, A.; Ardati, A.; Henningsen, R.A.; Bunzow, J.R.; Grandy, D.K.; Langen, H.; Monsma, F.J., Jr.; Civelli, O. Orphanin FQ: A neuropeptide that activates an opioidlike G protein-coupled receptor. Science 1995, 270, 792–794. [Google Scholar] [CrossRef]
- Meunier, J.C.; Mollereau, C.; Toll, L.; Suaudeau, C.; Moisand, C.; Alvinerie, P.; Butour, J.L.; Guillemot, J.C.; Ferrara, P.; Monsarrat, B.; et al. Isolation and structure of the endogenous agonist of opioid receptor-like ORL1 receptor. Nature 1995, 377, 532–535. [Google Scholar] [CrossRef] [PubMed]
- Pearse, A.G. Common cytochemical properties of cells producing polypeptide hormones, with particular reference to calcitonin and the thyroid C cells. Vet. Rec. 1966, 79, 587–590. [Google Scholar] [CrossRef] [PubMed]
- Bloom, S.R.; Polak, J.M. Gut hormone overview. In Gut Hormones; Bloom, S.R., Ed.; Churchill and Livingstone: London, UK, 1978; pp. 3–18. [Google Scholar]
- Le Douarin, N.M. The embryological origin of the endocrine cells associated with the digestive tract. In Gut Hormones; Bloom, S.R., Ed.; Churchill and Livingstone: London, UK, 1978; pp. 49–56. [Google Scholar]
- Evsiukova, E.V. APUD cells. The human pulmonary neuroendocrine system. Fiziol. Cheloveka 2006, 32, 121–130. [Google Scholar] [CrossRef]
- Lindheim, S.R.; Sauer, M.V.; Carmina, E.; Chang, P.L.; Zimmerman, R.; Lobo, R.A. Circulating leptin levels during ovulation induction: Relation to adiposity and ovarian morphology. Fertil. Steril. 2000, 73, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Pearse, A.G.E.; Polak, J.M. The diffuse neuroendocrine system and the APUD concept. In Gut Hormones; Bloom, S.R., Ed.; Churchill and Livingstone: London, UK, 1978; pp. 33–39. [Google Scholar]
- Hantos, M.B.; Szalay, F.; Lakatos, P.L.; Hegedűs, D.; Firneisz, G.; Reiczigel, J.; Török, T.; Tekes, K. Elevated plasma nociceptin level in patients with Wilson disease. Brain Res. Bull. 2002, 58, 311–313. [Google Scholar] [CrossRef]
- Bedini, A.; Baiula, M.; Vincelli, G.; Formaggio, F.; Lombardi, S.; Caprini, M.; Spampinato, S. Nociceptin/orphanin FQ antagonizes lipopolysaccharide-stimulated proliferation, migration and inflammatory signaling in human glioblastoma U87 cells. Biochem. Pharmacol. 2017, 140, 89–104. [Google Scholar] [CrossRef]
- Zhou, X.; Chen, D.; Yan, Y.; Li, Q.; Xing, W.; Liu, Y.; Chen, Y.; Wang, D.; Yuan, Y.; Xie, J.; et al. The nociceptin receptor promotes autophagy through NF-kB signaling and is transcriptionally regulated by E2F1 in HCC. Cell Death Discov. 2022, 8, 165. [Google Scholar] [CrossRef]
- Szalay, F.; Hantos, M.B.; Horvath, A.; Lakatos, P.L.; Folhoffer, A.; Dunkel, K.; Hegedus, D.; Tekes, K. Increased nociceptin/orphanin FQ plasma levels in hepatocellular carcinoma. World J. Gastroenterol. 2004, 10, 42–45. [Google Scholar] [CrossRef]
- Sireci, F.; Cappello, F.; Canevari, F.R.; Dispenza, F.; Gallina, S.; Salvago, P.; Martines, F. The Role of Leptin in Laryngeal Squamous Cell Carcinoma. In Leptin: Production, Regulation and Functions; Gilles, É., Mickaël, D., Eds.; Production, Regulation and Functions; Nova Publisher Leptin: Hauppauge, NY, USA, 2017; pp. 167–176. [Google Scholar]
- Cavaliere, M.; Bisogno, A.; Scarpa, A.; D’Urso, A.; Marra, P.; Colacurcio, V.; De Luca, P.; Ralli, M.; Cassandro, E.; Cassandro, C. Biomarkers of laryngeal squamous cell carcinoma: A review. Ann. Diagn. Pathol. 2021, 54, 151787. [Google Scholar] [CrossRef]
- Cooper, J.S.; Porter, K.; Mallin, K.; Hoffman, H.T.; Weber, R.S.; Ang, K.K.; Gay, E.G.; Langer, C.J. National Cancer Database report on cancer of the head and neck: 10-year update. Head Neck 2009, 31, 748–758. [Google Scholar] [CrossRef] [PubMed]
- Lehr, H.A.; Mankoff, D.A.; Corwin, D.; Santeusanio, G.; Gown, A.M. Application of photoshop-based image analysis to quantification of hormone receptor expression in breast cancer. J. Histochem. Cytochem. 1997, 45, 1559–1565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkeby, S.; Thomsen, C.E. Quantitative immunohistochemistry of fluorescence labelled probes using low-cost software. J. Immunol. Methods 2005, 301, 102–113. [Google Scholar] [CrossRef]
- Pham, N.A.; Morrison, A.; Schwock, J.; Aviel-Ronen, S.; Iakovlev, V.; Tsao, M.S.; Ho, J.; Hedley, D.W. Quantitative image analysis of immunohistochemical stains using a CMYK color model. Diagn. Pathol. 2007, 27, 2–8. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, M.; Zouhair, A.; Azria, D.; Ozsahin, M. The epidermal growth factor receptor (EGFR) in head and neck cancer: Its role and treatment implications. Radiat. Oncol. 2006, 1, 11. [Google Scholar] [CrossRef] [PubMed]
- Leone, A.; Spatola, G.F.; Cucco, D.; Tessitore, V.; Bonaventura, G.; Uzzo, M.L. Immunohistochemical expression and distribution of orexin, orphanin and leptin in the major salivary glands of some mammals. Folia Histochem. Cytobiol. 2012, 50, 504–512. [Google Scholar] [CrossRef]
- Gallina, S.; Sireci, F.; Lorusso, F.; Di Benedetto, D.V.; Speciale, R.; Marchese, D.; Costantino, C.; Napoli, G.; Tessitore, V.; Cucco, D.; et al. The immunohistochemical peptidergic expression of leptin is associated with recurrence of malignancy in laryngeal squamous cell carcinoma. ACTA Otorhinolaryngol. Ital. 2015, 35, 15–22. [Google Scholar]
- Easten, K.H.; Harry, R.A.; Purcell, W.M.; McLeod, J.D. Nociceptin-induced modulation of human T cell function. Peptides 2009, 30, 926–934. [Google Scholar] [CrossRef]
- Ko, M.H.; Kim, Y.H.; Woo, R.S.; Kim, K.W. Quantitative analysis of nociceptin in blood of patients with acute and chronic pain. Neuroreport 2002, 13, 1631–1633. [Google Scholar] [CrossRef] [PubMed]
- Trombella, S.; Vergura, R.; Falzarano, S.; Guerrini, R.; Calo, G.; Spisani, S. Nociceptin/orphanin FQ stimulates human monocyte chemotaxis via NOP receptor activation. Peptides 2005, 26, 1497–1502. [Google Scholar] [CrossRef]
- Waits, P.S.; Purcell, W.M.; Fulford, A.J.; McLeod, J.D. Nociceptin/ /orphanin FQ modulates human T cell function in vitro. J. Neuroimmunol. 2004, 149, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Noguchi, Y.; Yoshikawa, T.; Matsumoto, A.; Svaninger, G.; Gelin, J. Are cytokines possible mediators of cancer cachexia? Surg. Today 1996, 26, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Matthys, P.; Matthys, P.; Billiau, A. Cytokines and cachexia. Nutrition 1997, 13, 763–770. [Google Scholar] [CrossRef]
- Hinz, B.; Ramer, R. Anti-tumour actions of cannabinoids. Br. J. Pharmacol. 2019, 176, 1384–1394. [Google Scholar] [CrossRef]
- Picardi, P.; Ciaglia, E.; Proto, M.C.; Pisanti, S. Anandamide inhibits breast tumour-induced angiogenesis. Transl. Med. UniSa 2014, 10, 8–12. [Google Scholar]
- Caffarel, M.M.; Andradas, C.; Pérez-Gómez, E.; Guzmán, M.; Sánchez, C. Cannabinoids: A new hope for breast cancer therapy? Cancer Treat. Rev. 2012, 38, 911–918. [Google Scholar] [CrossRef]
- Sliepen, S.H.; Korioth, J.; Christoph, T.; Tzschentke, T.M.; Diaz-delCastillo, M.; Heegaard, A.M.; Rutten, K. The nociceptin/orphanin FQ receptor system as a target to alleviate cancer-induced bone pain in rats: Model validation and pharmacological evaluation. Br. J. Pharmacol. 2021, 178, 1995–2007. [Google Scholar] [CrossRef] [Green Version]
- Dib, P.; Zhang, Y.; Ihnat, M.A.; Gallucci, R.M.; Standifer, K.M. TNF-Alpha as an Initiator of Allodynia and Anxiety-Like Behaviors in a Preclinical Model of PTSD and Comorbid Pain. Front. Psychiatry 2021, 12, 721999. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| N (%) | N/OFQ | p Value | |||
|---|---|---|---|---|---|
| Low | High | ||||
| Cases | 48 | 10 (20.8) | 38 (79.2) | ||
| Age | ≤59 | 18 (37.5) | 2 (11.1) | 16 (88.8) | 0.19 |
| >59 | 30 (62.5) | 8 (26.6) | 22 (73.3) | ||
| T stadium (early/advanced) | T1–T2 (early) | 12 (25) | 0 | 12 (100) | 0.20 |
| T3–T4 (advanced) | 36 (75) | 10 (27.7) | 26 (72.2) | ||
| pT1 | 0 | 0 | 0 | ||
| pT2 | 12 (25) | 0 | 12 (100) | ||
| pT3 | 24 (50) | 8 (33.3) | 16 (66.6) | ||
| PT4 | 12 (25) | 2 (16.6) | 10 (83.3) | ||
| N0 and N+ category | N0 | 28 (58.3) | 8 (33.3) | 20 (66.7) | 0.11 |
| N+ | 20 (41.7) | 2 | 18 (100) | ||
| pN0 | 28 (58.3) | 8 (28.6) | 20 (71.4) | ||
| pN1 | 4 (8.3) | 2 (50) | 2 (50) | ||
| pN2 | 10 (25) | 0 | 10 (100) | ||
| pN3 | 4 (8.3) | 0 | 4 (100) | ||
| Tot | 10 (20.8) | 36 (79.2) | |||
| Stage (early/advanced) | early (I–II) | 8 (16.6) | 0 | 8 (100) | 0.36 |
| advanced (III–IV) | 40 (83.3) | 10 (25) | 30 (75) | ||
| Stage I | 0 | 0 | 0 | ||
| Stage II | 8 (16.6) | 0 | 8 (100) | ||
| Stage III | 16 (33.3) | 5 (31.2) | 11 (68.8) | ||
| Stage IV | 24 (50) | 5 (20.8) | 19 (79.2) | ||
| Grading (low and high) | Low (G1) | 8 (16.6) | 0 | 8 (100) | |
| High (G2–G3) | 40 (83.4) | 10 (25) | 30 (75) | ||
| G1 | 8 (16.6) | 0 | 8 (100) | 0.36 | |
| G2 | 20 (41.6) | 5 (25) | 15 (75) | ||
| G3 | 20 (41.6) | 5 (25) | 15 (75) | ||
| Loco-regional recurrence | No | 32 (66.6) | 2 (6.2) | 30 (93.8) | 0.66 |
| Yes | 16 (33.3) | 0 | 16 (100) | ||
| Cases | Controls | p Value | ||
|---|---|---|---|---|
| N/OFQ | Yes | 48 | 12 | 0.001 |
| No | 0 | 36 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sireci, F.; Lorusso, F.; Dispenza, F.; Immordino, A.; Gallina, S.; Salvago, P.; Martines, F.; Bonaventura, G.; Uzzo, M.L.; Spatola, G.F. A Prospective Observational Study on the Role of Immunohistochemical Expression of Orphanin in Laryngeal Squamous Cell Carcinoma Recurrence. J. Pers. Med. 2023, 13, 1211. https://doi.org/10.3390/jpm13081211
Sireci F, Lorusso F, Dispenza F, Immordino A, Gallina S, Salvago P, Martines F, Bonaventura G, Uzzo ML, Spatola GF. A Prospective Observational Study on the Role of Immunohistochemical Expression of Orphanin in Laryngeal Squamous Cell Carcinoma Recurrence. Journal of Personalized Medicine. 2023; 13(8):1211. https://doi.org/10.3390/jpm13081211
Chicago/Turabian StyleSireci, Federico, Francesco Lorusso, Francesco Dispenza, Angelo Immordino, Salvatore Gallina, Pietro Salvago, Francesco Martines, Giuseppe Bonaventura, Maria Laura Uzzo, and Giovanni Francesco Spatola. 2023. "A Prospective Observational Study on the Role of Immunohistochemical Expression of Orphanin in Laryngeal Squamous Cell Carcinoma Recurrence" Journal of Personalized Medicine 13, no. 8: 1211. https://doi.org/10.3390/jpm13081211