
Impact of Stepwise Recruitment Maneuvers on Cerebral Hemodynamics: Experimental Study in Neonatal Model
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Committee
2.2. Anesthesia
- -
- 10 mL/kg of physiological saline at 36 °C was administered when the mean arterial pressure (MAP) was under 45 mmHg.
- -
- An extra dose of morphine (0.1 mg/kg) was administered when the piglet had a heart rate greater than 180 bpm.
2.3. Monitoring
2.4. Recruitment Maneuvers
2.5. Recorded Variables
2.6. Statistical Analysis
3. Results
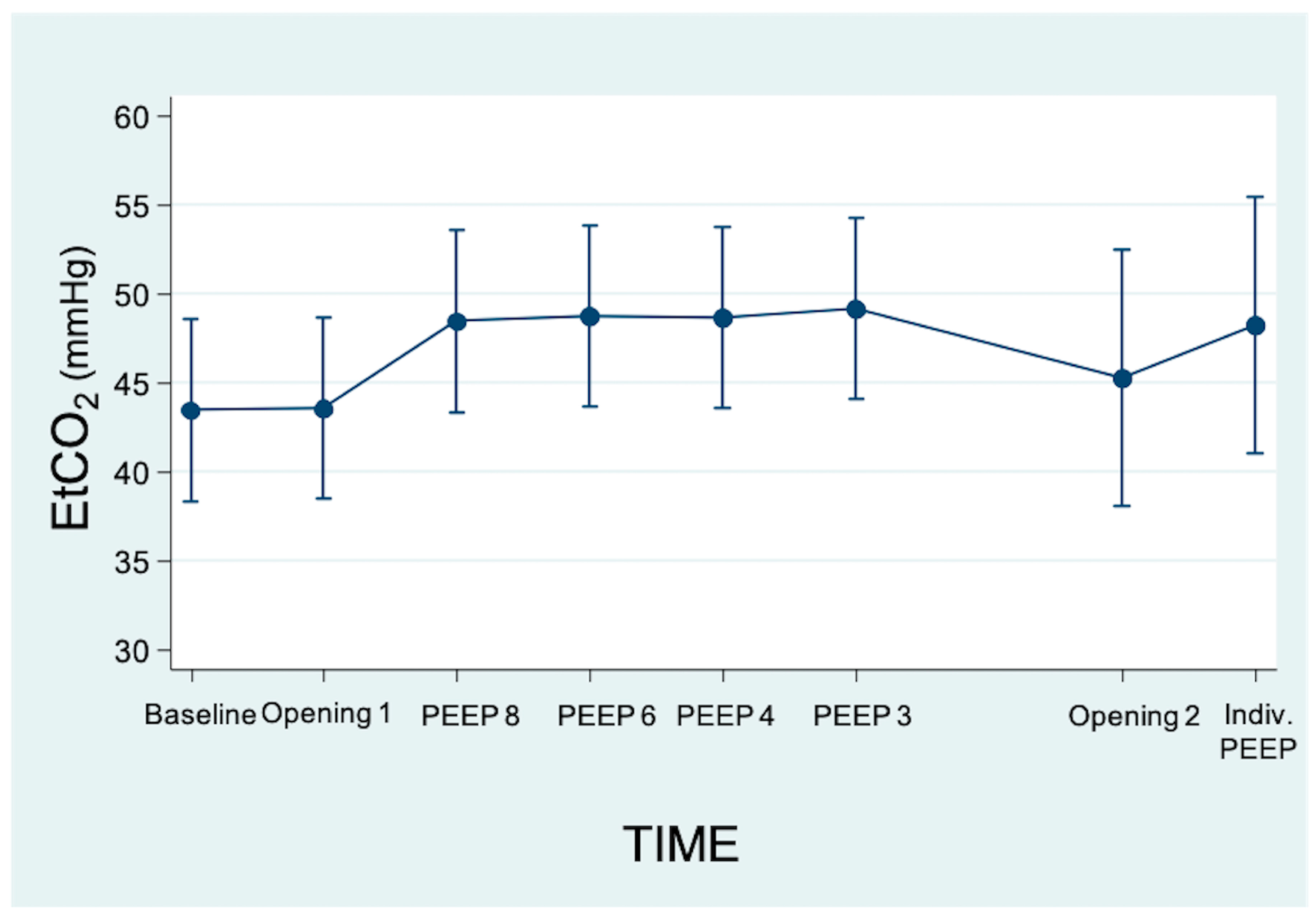
3.1. Effects on Respiratory Variables
3.2. Effects on Systemic Hemodynamics
3.3. Effects on Cerebral Hemodynamics
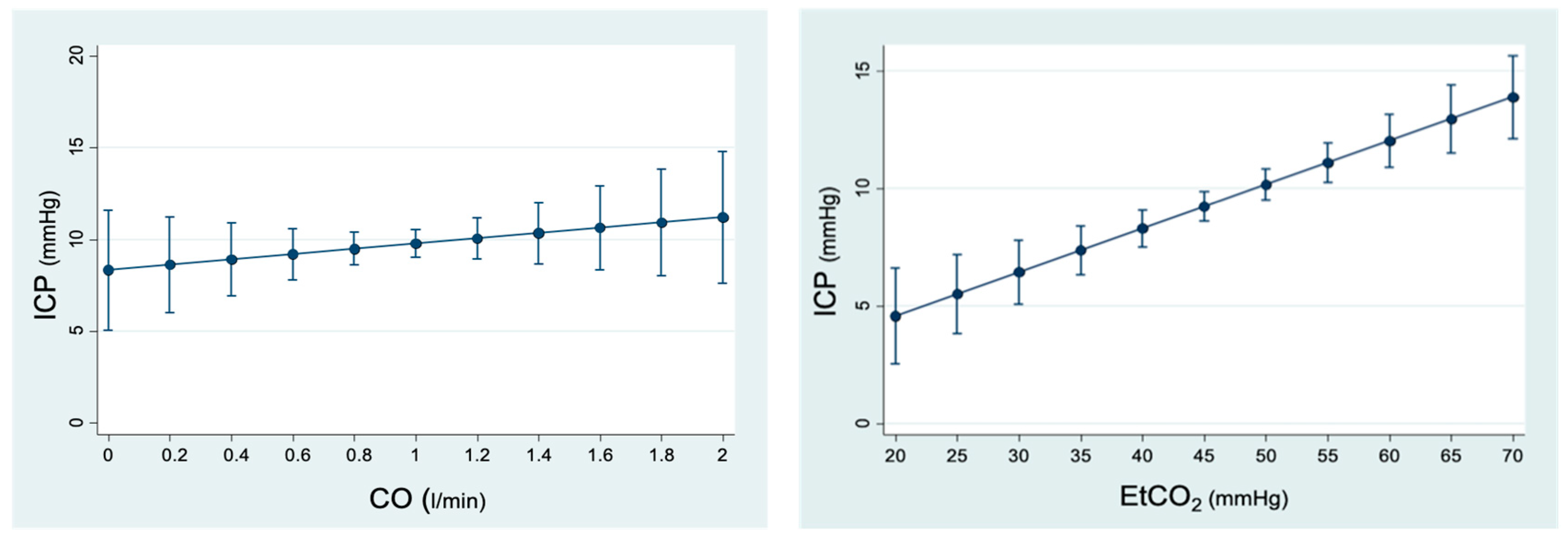
3.3.1. Analysis of the Relationship between ICP and Changes in Hemodynamic Variables
3.3.2. Analysis of the Relationship between ICP and Respiratory Parameters
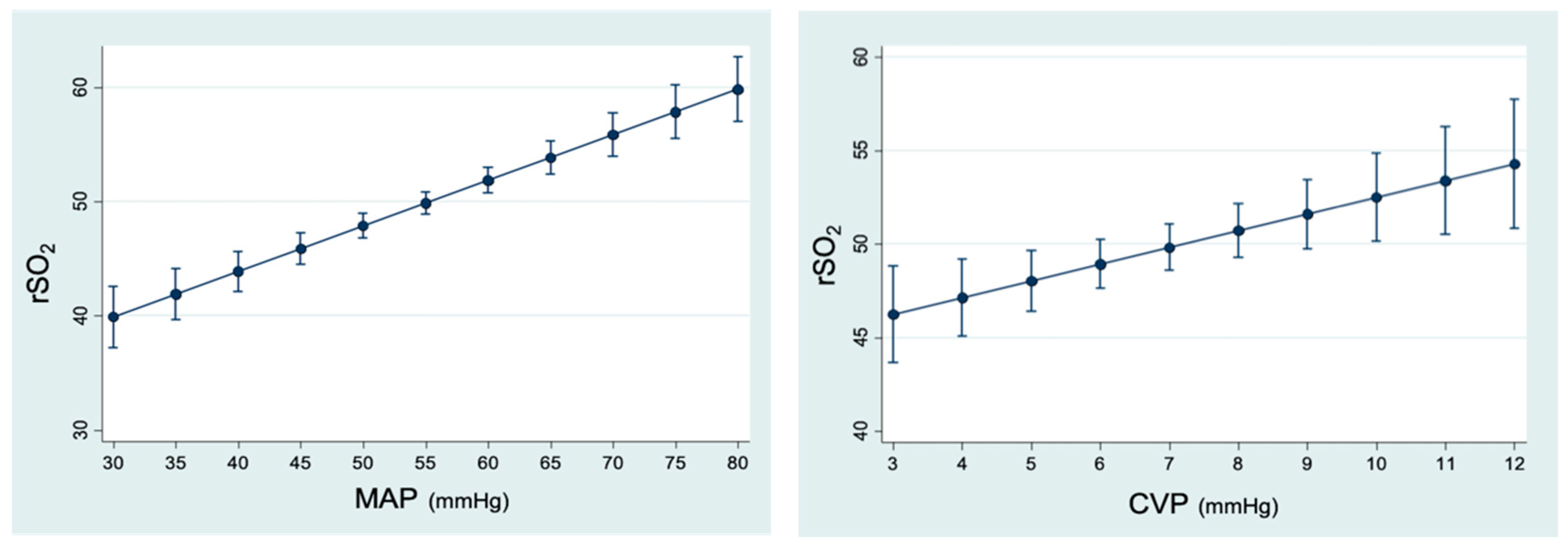
3.3.3. Analysis of the Relationship between rSO2 and Hemodynamic Parameters
3.3.4. Analysis of the Relationship between rSO2 and Respiratory Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Giordano, G.; Pugliese, F.; Bilotta, F. Neuroinflammation, Neuronal Damage or Cognitive Impairment Associated with Mechanical Ventilation: A Systematic Review of Evidence from Animal Studies. J. Crit. Care 2021, 62, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Cannavò, L.; Rulli, I.; Falsaperla, R.; Corsello, G.; Gitto, E. Ventilation, Oxidative Stress and Risk of Brain Injury in Preterm Newborn. Ital. J. Pediatr. 2020, 46, 100. [Google Scholar] [CrossRef]
- Bilotta, F.; Giordano, G.; Sergi, P.G.; Pugliese, F. Harmful Effects of Mechanical Ventilation on Neurocognitive Functions. Crit. Care 2019, 23, 273. [Google Scholar] [CrossRef] [Green Version]
- Tusman, G.; Böhm, S.H.; Tempra, A.; Melkun, F.; García, E.; Turchetto, E.; Mulder, P.G.H.; Lachmann, B. Effects of Recruitment Maneuver on Atelectasis in Anesthetized Children. Anesthesiology 2003, 98, 14–22. [Google Scholar] [CrossRef]
- Garcia-Fernandez, J.; Castro, L.; Belda, F.J. Ventilating the Newborn and Child. Curr. Anaesth. Crit. Care 2010, 21, 262–268. [Google Scholar] [CrossRef]
- García-Fernández, J.; Romero, A.; Blanco, A.; Gonzalez, P.; Abad-Gurumeta, A.; Bergese, S.D. Maniobras de reclutamiento en anestesia: ¿qué más excusas para no usarlas? Rev. Esp. Anestesiol. Reanim. 2018, 65, 209–217. [Google Scholar] [CrossRef]
- Bein, T.; Kuhr, L.-P.; Bele, S.; Ploner, F.; Keyl, C.; Taeger, K. Lung Recruitment Maneuver in Patients with Cerebral Injury: Effects on Intracranial Pressure and Cerebral Metabolism. Intensive Care Med. 2002, 28, 554–558. [Google Scholar] [CrossRef] [PubMed]
- Aydin, P.; Kizilkaya, M. Effects of Recruitment Maneuvers on Oxygenation and Intracranial Pressure in the Experimental ARDS Model. Eurasian J. Med. 2022, 54, 274–280. [Google Scholar] [CrossRef]
- Zhang, X.; Yang, Z.; Wang, Q.; Fan, H. Impact of Positive End-Expiratory Pressure on Cerebral Injury Patients with Hypoxemia. Am. J. Emerg. Med. 2011, 29, 699–703. [Google Scholar] [CrossRef]
- Frost, E.M. Effects of Positive End-Expiratory Pressure on Intracranial Pressure and Compliance in Brain-Injured Patients. J. Neurosurg. 1977, 47, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boone, M.D.; Jinadasa, S.P.; Mueller, A.; Shaefi, S.; Kasper, E.M.; Hanafy, K.A.; O’Gara, B.P.; Talmor, D.S. The Effect of Positive End-Expiratory Pressure on Intracranial Pressure and Cerebral Hemodynamics. Neurocrit. Care 2017, 26, 174–181. [Google Scholar] [CrossRef]
- Ruggieri, F.; Beretta, L.; Corno, L.; Testa, V.; Martino, E.A.; Gemma, M. Feasibility of Protective Ventilation During Elective Supratentorial Neurosurgery: A Randomized, Crossover, Clinical Trial. J. Neurosurg. Anesthesiol. 2017, 30, 246–250. [Google Scholar] [CrossRef]
- De Rosa, S.; Villa, G.; Franchi, P.; Mancino, A.; Tosi, F.; Martin, M.A.; Bazzano, S.; Conti, G.; Pulitanò, S.M. Impact of Positive End Expiratory Pressure on Cerebral Hemodynamic in Paediatric Patients with Post-Traumatic Brain Swelling Treated by Surgical Decompression. PLoS ONE 2018, 13, e0196980. [Google Scholar] [CrossRef] [Green Version]
- Pulitanò, S.; Mancino, A.; Pietrini, D.; Piastra, M.; De Rosa, S.; Tosi, F.; De Luca, D.; Conti, G. Effects of Positive End Expiratory Pressure (PEEP) on Intracranial and Cerebral Perfusion Pressure in Pediatric Neurosurgical Patients. J. Neurosurg. Anesthesiol. 2013, 25, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Serrano Zueras, C.; Guilló Moreno, V.; Santos González, M.; Gómez Nieto, F.J.; Hedenstierna, G.; García Fernández, J. Safety and Efficacy Evaluation of the Automatic Stepwise Recruitment Maneuver in the Neonatal Population: An in Vivo Interventional Study. Can Anesthesiologists Safely Perform Automatic Lung Recruitment Maneuvers in Neonates? Pediatr. Anesth. 2021, 31, 1003–1010. [Google Scholar] [CrossRef]
- González-Pizarro, P.; García-Fernández, J.; Canfrán, S.; Gilsanz, F. Neonatal Pneumothorax Pressures Surpass Higher Threshold in Lung Recruitment Maneuvers: An In Vivo Interventional Study. Respir. Care 2016, 61, 142–148. [Google Scholar] [CrossRef]
- Gutiérrez Martínez, A.; Guilló Moreno, V.; Santos, M.; Mingote Lladó, Á.; González-Pizarro, P.; García-Fernández, J. Safe Inspiratory Pressures Threshold in Lung Recruitment Maneuvers: An In Vivo Neonatal ARDS Model. Respir. Care 2022, 67, 1300–1309. [Google Scholar] [CrossRef]
- Lerman, J.; Oyston, J.P.; Gallagher, T.M.; Miyasaka, K.; Volgyesi, G.A.; Burrows, F.A. The Minimum Alveolar Concentration (MAC) and Hemodynamic Effects of Halothane, Isoflurane, and Sevoflurane in Newborn Swine. Anesthesiology 1990, 73, 717–721. [Google Scholar] [CrossRef]
- Wilson, M.H. Monro-Kellie 2.0: The Dynamic Vascular and Venous Pathophysiological Components of Intracranial Pressure. J. Cereb. Blood Flow Metab. 2016, 36, 1338–1350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burchiel, K.J.; Steege, T.D.; Wyler, A.R. Intracranial Pressure Changes in Brain-Injured Patients Requiring Positive End-Expiratory Pressure Ventilation. Neurosurgery 1981, 8, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Feldman, Z.; Robertson, C.S.; Contant, C.F.; Gopinath, S.P.; Grossman, R.G. Positive End Expiratory Pressure Reduces Intracranial Compliance in the Rabbit. J. Neurosurg. Anesthesiol. 1997, 9, 175–179. [Google Scholar] [CrossRef]
- Juhász, M.; Molnár, L.; Fülesdi, B.; Végh, T.; Páll, D.; Molnár, C. Effect of Sevoflurane on Systemic and Cerebral Circulation, Cerebral Autoregulation and CO2 Reactivity. BMC Anesthesiol. 2019, 19, 109. [Google Scholar] [CrossRef] [Green Version]
- Valencia, L.; Rodríguez-Pérez, A.; Kühlmorgen, B.; Santana, R.Y. Does Sevoflurane Preserve Regional Cerebral Oxygen Saturation Measured by Near-Infrared Spectroscopy Better than Propofol? Ann. Fr. Anesth. Réanim. 2014, 33, e59–e65. [Google Scholar] [CrossRef] [PubMed]
- Caricato, A.; Conti, G.; Corte, F.D.; Mancino, A.; Santilli, F.; Sandroni, C.; Proietti, R.; Antonelli, M. Effects of PEEP on the Intracranial System of Patients With Head Injury and Subarachnoid Hemorrhage: The Role of Respiratory System Compliance. J. Trauma Inj. Infect. Crit. Care 2005, 58, 571–576. [Google Scholar] [CrossRef] [PubMed]
- McGuire, G.; Crossley, D.; Richards, J.; Wong, D. Effects of Varying Levels of Positive End-Expiratory Pressure on Intracranial Pressure and Cerebral Perfusion Pressure. Crit. Care Med. 1997, 25, 1059–1062. [Google Scholar] [CrossRef] [PubMed]
- Videtta, W.; Villarejo, F.; Cohen, M.; Domeniconi, G.; Santa Cruz, R.; Pinillos, O.; Rios, F.; Maskin, B. Effects of Positive End-Expiratory Pressure on Intracranial Pressure and Cerebral Perfusion Pressure. In Intracranial Pressure and Brain Biochemical Monitoring; Acta Neurochirurgica Supplements; Springer: Vienna, Austria, 2002; Volume 81, pp. 93–97. [Google Scholar] [CrossRef]
- Chen, H.; Zhou, J.; Lin, Y.-Q.; Zhou, J.-X.; Yu, R.-G. Intracranial Pressure Responsiveness to Positive End-Expiratory Pressure in Different Respiratory Mechanics: A Preliminary Experimental Study in Pigs. BMC Neurol. 2018, 18, 183. [Google Scholar] [CrossRef]
- Kongstad, L.; Grände, P.O. The Role of Arterial and Venous Pressure for Volume Regulation of an Organ Enclosed in a Rigid Compartment with Application to the Injured Brain: Blood Pressure and Tissue Volume. Acta Anaesthesiol. Scand. 1999, 43, 501–508. [Google Scholar] [CrossRef]
- Chen, H.; Zhou, X.-F.; Zhou, D.-W.; Zhou, J.-X.; Yu, R.-G. Effect of Increased Positive End-Expiratory Pressure on Intracranial Pressure and Cerebral Oxygenation: Impact of Respiratory Mechanics and Hypovolemia. BMC Neurosci. 2021, 22, 72. [Google Scholar] [CrossRef]
- Mascia, L.; Grasso, S.; Fiore, T.; Bruno, F.; Berardino, M.; Ducati, A. Cerebro-Pulmonary Interactions during the Application of Low Levels of Positive End-Expiratory Pressure. Intensive Care Med. 2005, 31, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Balakrishnan, S.; Naik, S.; Chakrabarti, D.; Konar, S.; Sriganesh, K. Effect of Respiratory Physiological Changes on Optic Nerve Sheath Diameter and Cerebral Oxygen Saturation in Patients With Acute Traumatic Brain Injury. J. Neurosurg. Anesthesiol. 2022, 34, e52–e56. [Google Scholar] [CrossRef]
- Robba, C.; Ball, L.; Nogas, S.; Battaglini, D.; Messina, A.; Brunetti, I.; Minetti, G.; Castellan, L.; Rocco, P.R.M.; Pelosi, P. Effects of Positive End-Expiratory Pressure on Lung Recruitment, Respiratory Mechanics, and Intracranial Pressure in Mechanically Ventilated Brain-Injured Patients. Front. Physiol. 2021, 12, 711273. [Google Scholar] [CrossRef] [PubMed]
- Robba, C.; Ball, L.; Battaglini, D.; Iannuzzi, F.; Brunetti, I.; Fiaschi, P.; Zona, G.; Taccone, F.S.; Messina, A.; Mongodi, S.; et al. Effects of Positive End-Expiratory Pressure on Lung Ultrasound Patterns and Their Correlation with Intracranial Pressure in Mechanically Ventilated Brain Injured Patients. Crit. Care 2022, 26, 31. [Google Scholar] [CrossRef]
- Nemer, S.N.; Caldeira, J.B.; Santos, R.G.; Guimarães, B.L.; Garcia, J.M.; Prado, D.; Silva, R.T.; Azeredo, L.M.; Faria, E.R.; Souza, P.C.P. Effects of Positive End-Expiratory Pressure on Brain Tissue Oxygen Pressure of Severe Traumatic Brain Injury Patients with Acute Respiratory Distress Syndrome: A Pilot Study. J. Crit. Care 2015, 30, 1263–1266. [Google Scholar] [CrossRef] [PubMed]
- Maissan, I.M.; Dirven, P.J.A.C.; Haitsma, I.K.; Hoeks, S.E.; Gommers, D.; Stolker, R.J. Ultrasonographic Measured Optic Nerve Sheath Diameter as an Accurate and Quick Monitor for Changes in Intracranial Pressure. J. Neurosurg. 2015, 123, 743–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Situation | Individualized PEEP | p Value | |
|---|---|---|---|
| PaO2 | 115 (94.7–128) | 122 (119–149) | 0.34 |
| Cdyn | 3 (2–3) | 4 (4–4) | 0.09 |
| Cstat | 4 (2.9–4.1) | 4.3 (3.9–4.7) | 0.04 |
| Pmean | 7.5 (7.5–8) | 8.5 (8–9) | 0.17 |
| PEEP | 3 (3–3) | 6 (5–6) | 0.04 |
| Opening 1 | p Value | Opening 2 | p Value | Individualized PEEP | p Value | |
|---|---|---|---|---|---|---|
| MAP | −6 (95% CI −13.39–1.39) | 0.11 | −2.2 (95% CI −11.25–6.85) | 0.63 | +2.2 (95% CI −6.85–11.25) | 0.63 |
| CVP | +1.6 (95% CI −0.06–3.26) | 0.06 | +1.6 (95% CI −0.43–3.63) | 0.12 | +0.2 (95% CI −1.83–2.22) | 0.85 |
| CO | −0.09 (95% CI −0.28–0.96) | 0.33 | −0.04 (95% CI −0.27–0.19) | 0.72 | −0.06 (95% CI −0.29–0.17) | 0.62 |
| CPP | −6.8 (95% CI −14.51–0.91) | 0.08 | −4.2 (95% CI −13.64–5.24) | 0.38 | +1.6 (95% CI −7.84–11.04) | 0.74 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torre Oñate, T.; Romero Berrocal, A.; Bilotta, F.; Badenes, R.; Santos Gonzalez, M.; de Reina Perez, L.; Garcia Fernandez, J. Impact of Stepwise Recruitment Maneuvers on Cerebral Hemodynamics: Experimental Study in Neonatal Model. J. Pers. Med. 2023, 13, 1184. https://doi.org/10.3390/jpm13081184
Torre Oñate T, Romero Berrocal A, Bilotta F, Badenes R, Santos Gonzalez M, de Reina Perez L, Garcia Fernandez J. Impact of Stepwise Recruitment Maneuvers on Cerebral Hemodynamics: Experimental Study in Neonatal Model. Journal of Personalized Medicine. 2023; 13(8):1184. https://doi.org/10.3390/jpm13081184
Chicago/Turabian StyleTorre Oñate, Teresa, Antonio Romero Berrocal, Federico Bilotta, Rafael Badenes, Martin Santos Gonzalez, Laura de Reina Perez, and Javier Garcia Fernandez. 2023. "Impact of Stepwise Recruitment Maneuvers on Cerebral Hemodynamics: Experimental Study in Neonatal Model" Journal of Personalized Medicine 13, no. 8: 1184. https://doi.org/10.3390/jpm13081184