
Sedation with Sevoflurane versus Propofol in COVID-19 Patients with Acute Respiratory Distress Syndrome: Results from a Randomized Clinical Trial
 , , , ,
, , , ,
Abstract
:1. Introduction
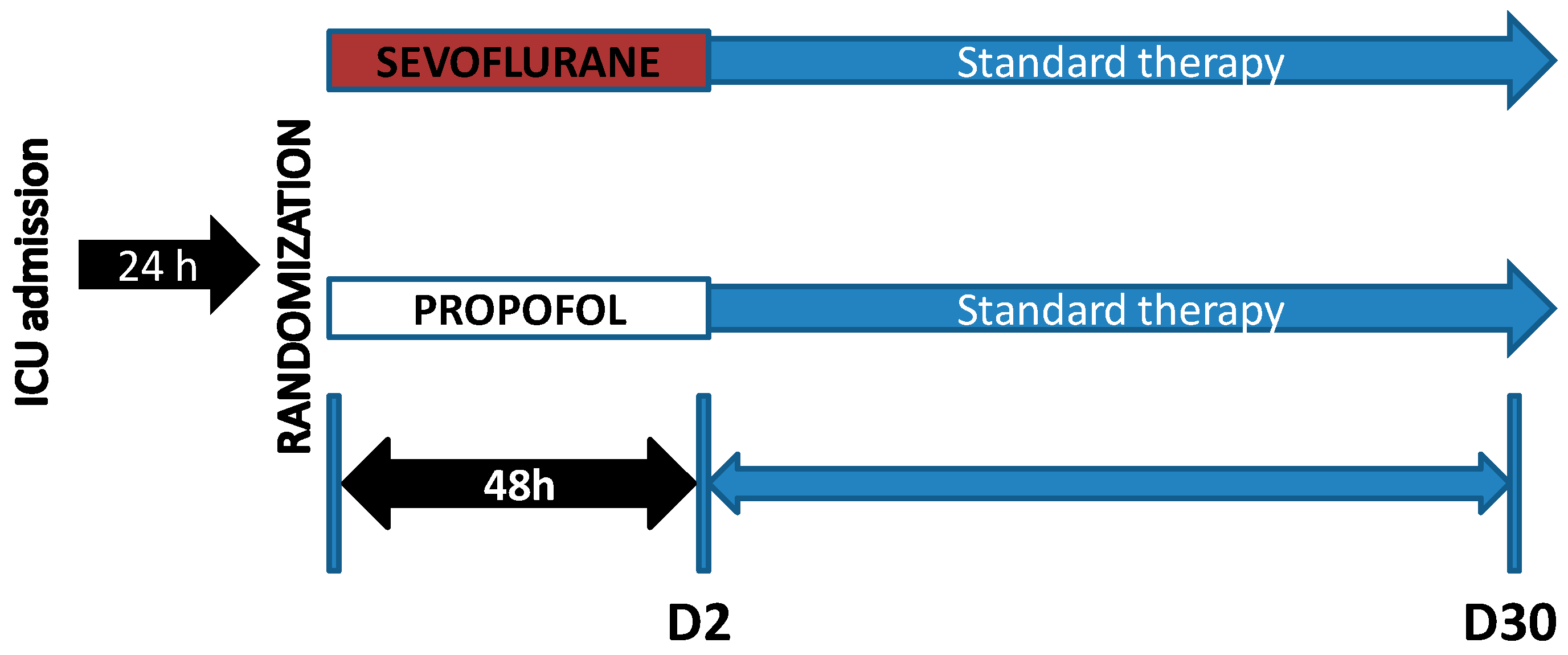
2. Materials and Methods
2.1. Study Population, Setting and Data Collection
2.2. Hypothesis and Objectives
2.3. Statistical Analysis
3. Results
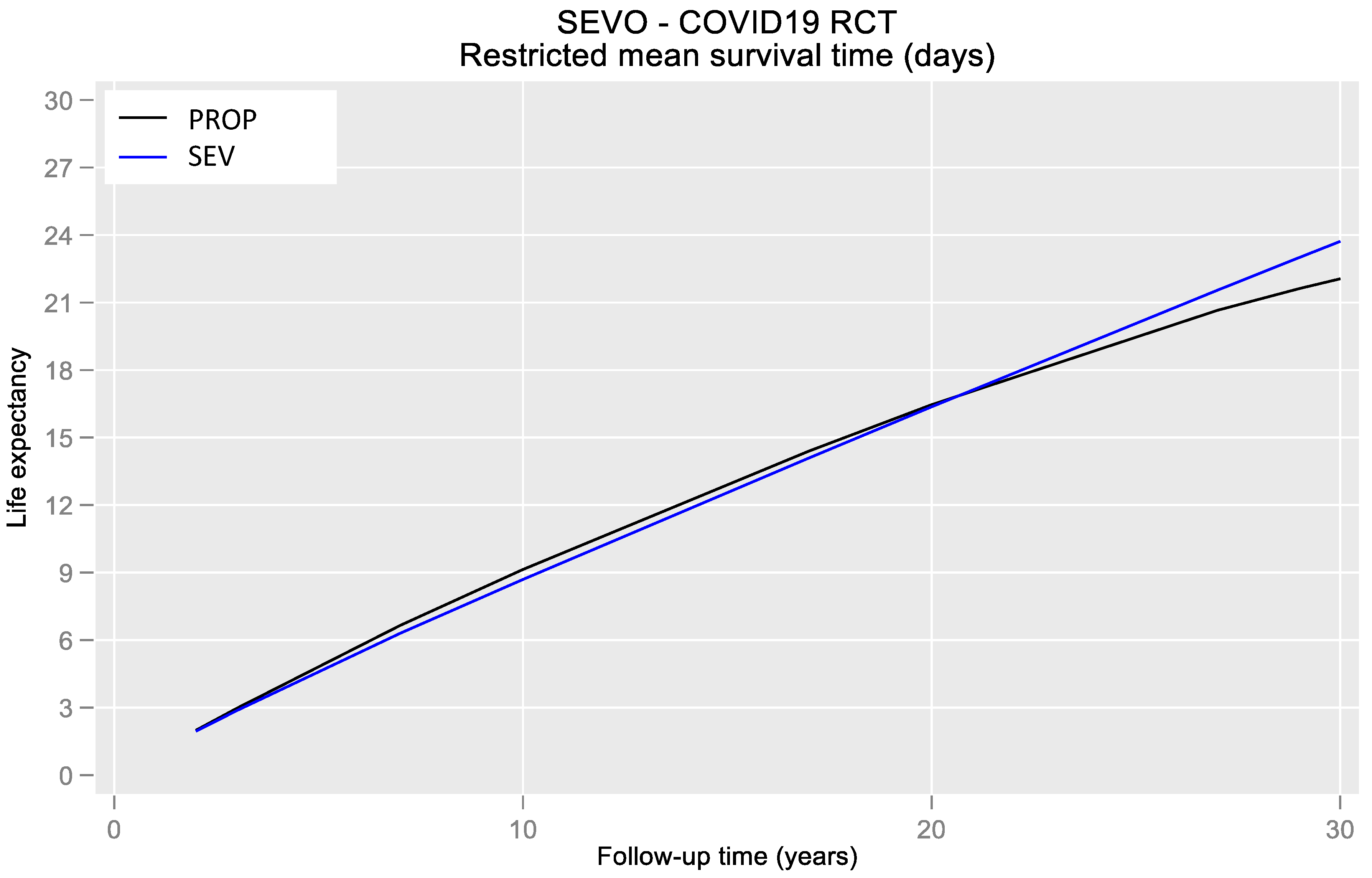
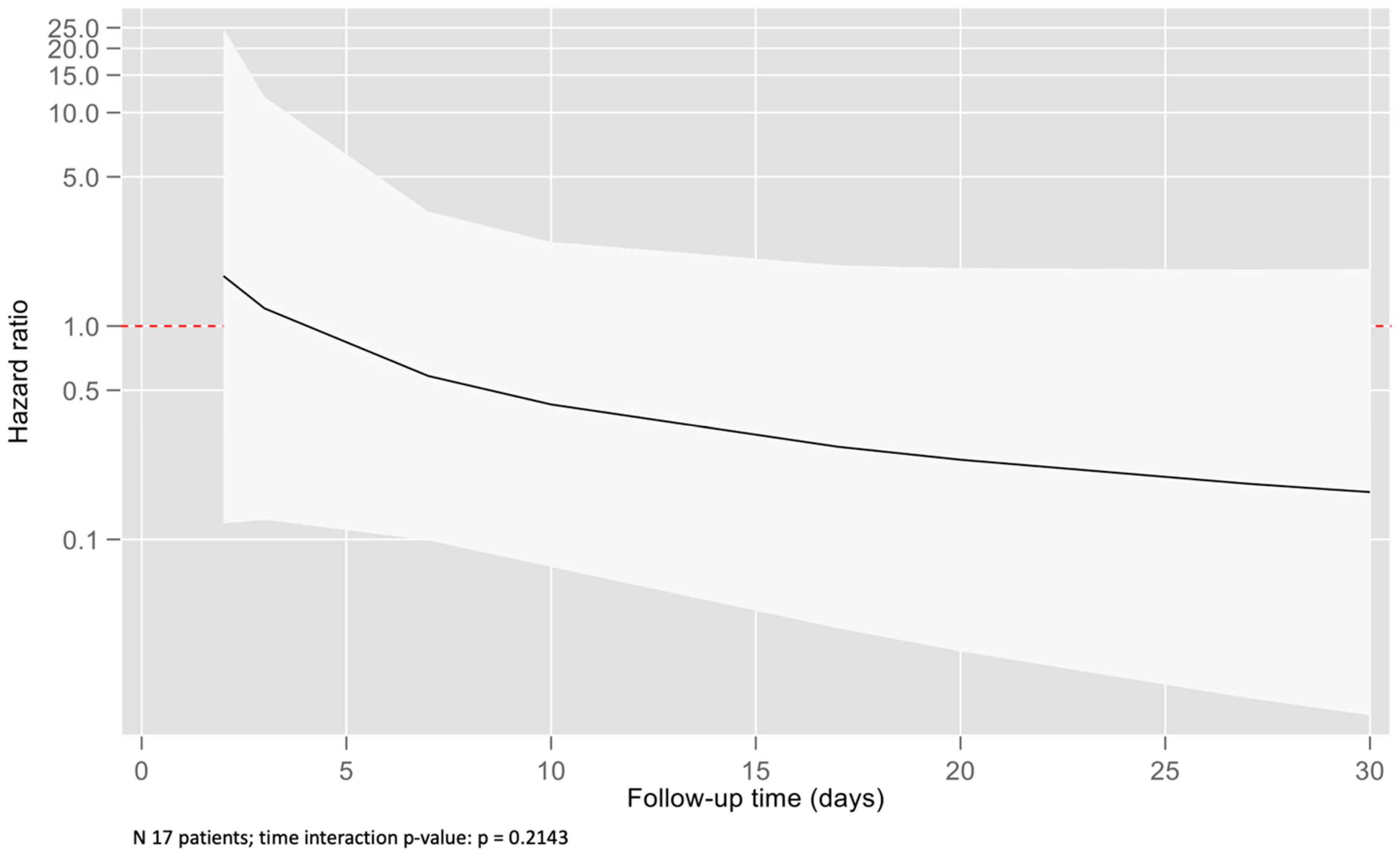
3.1. Primary Results
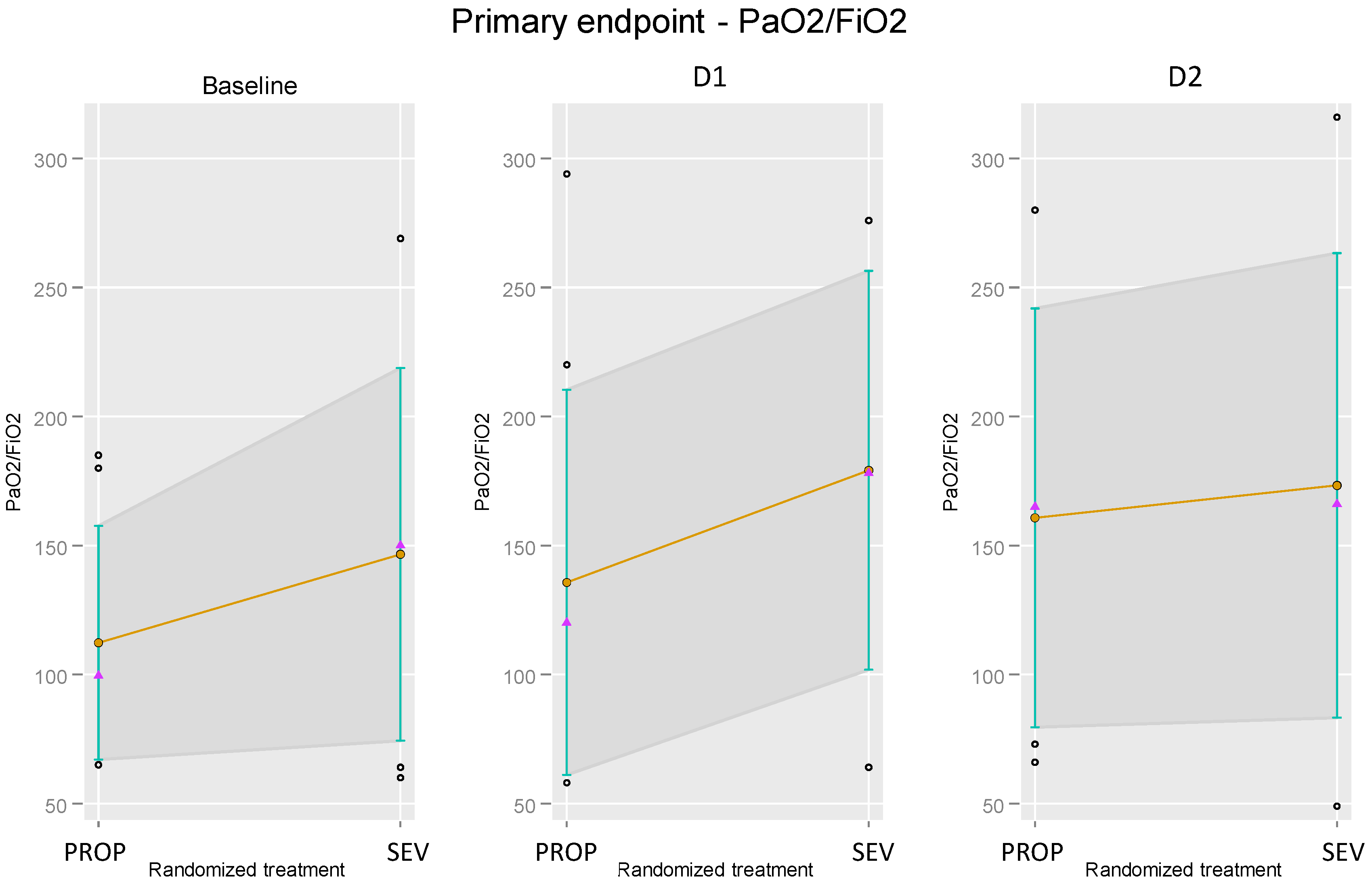
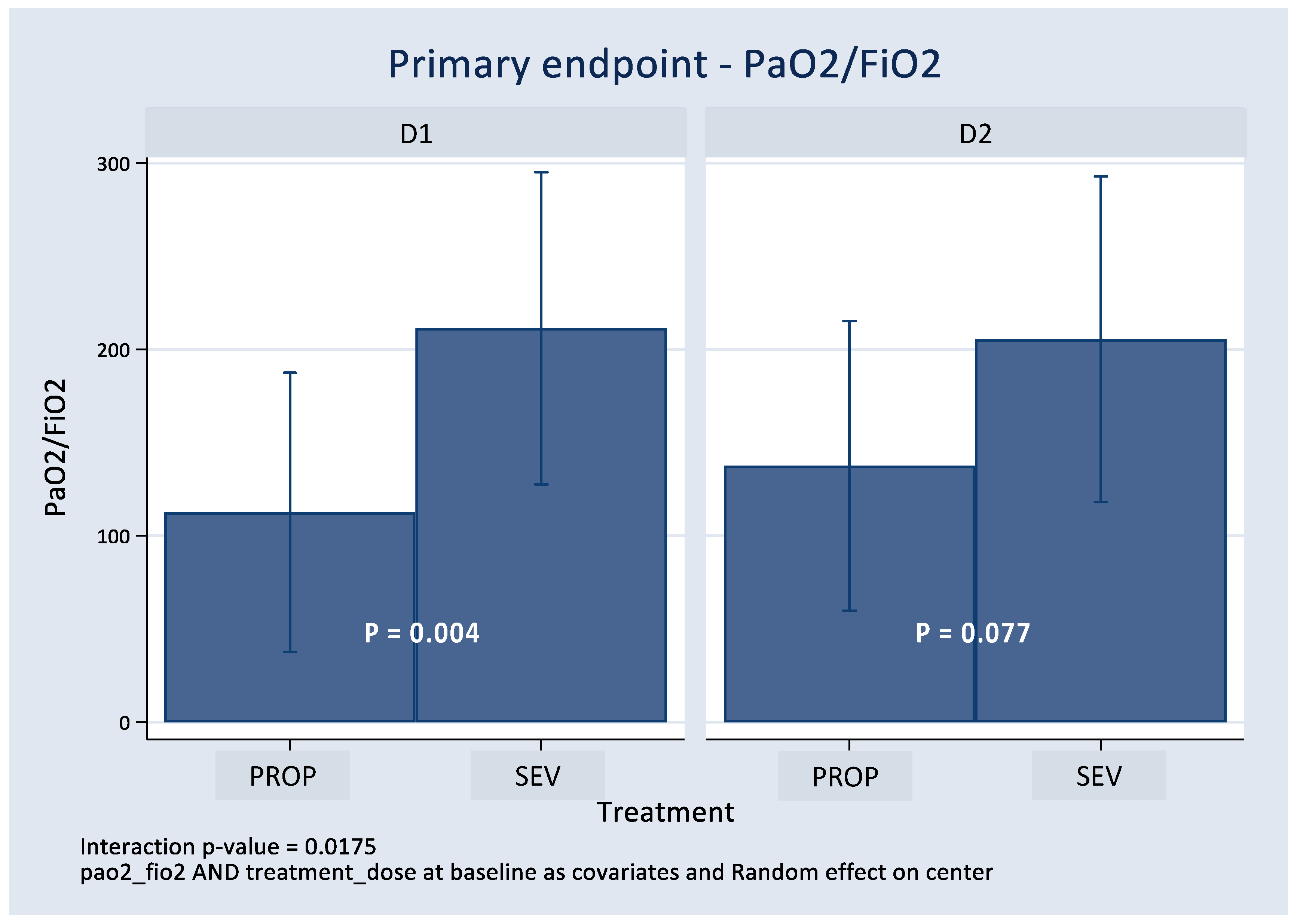
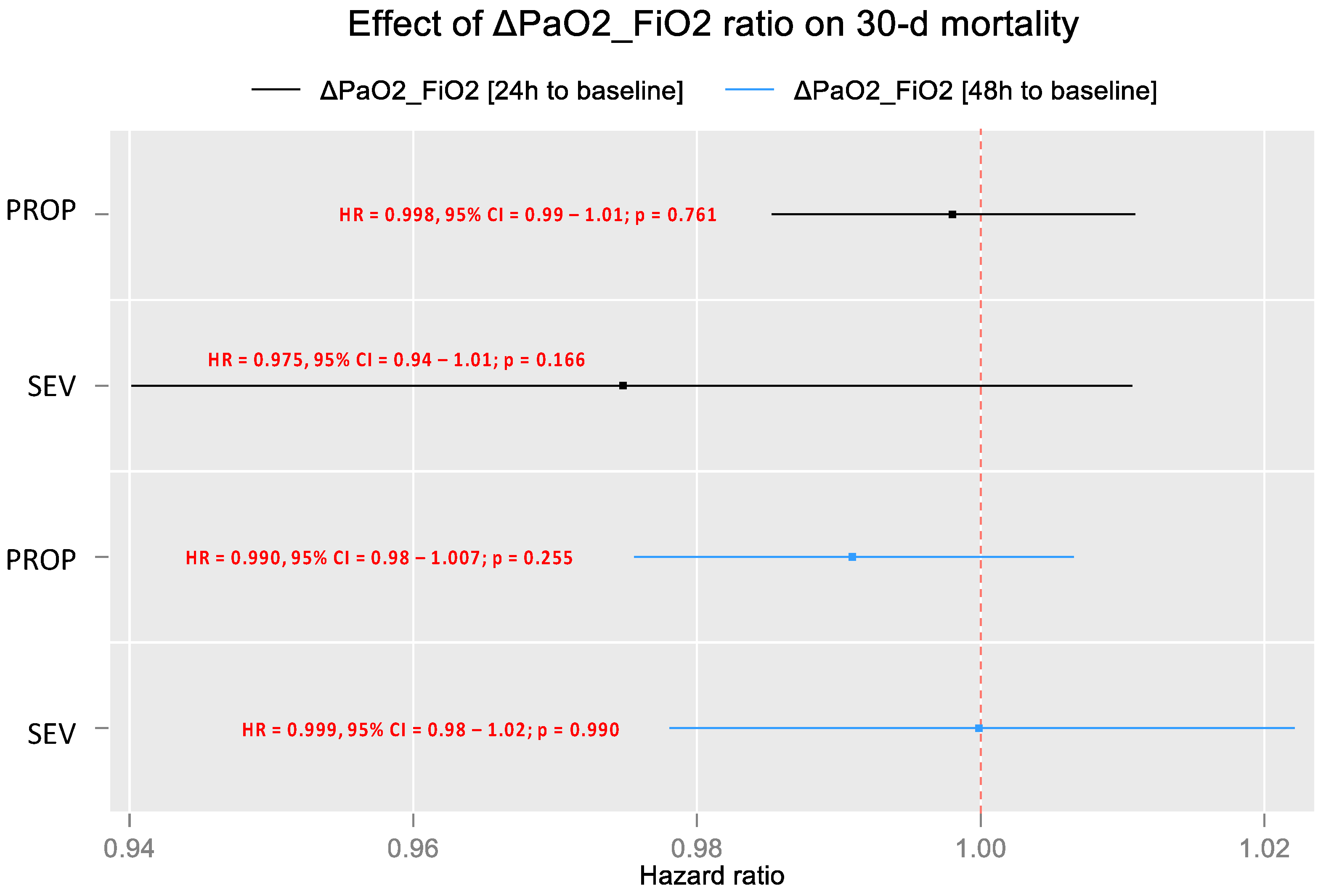
3.2. Effect on PaO2/FiO2
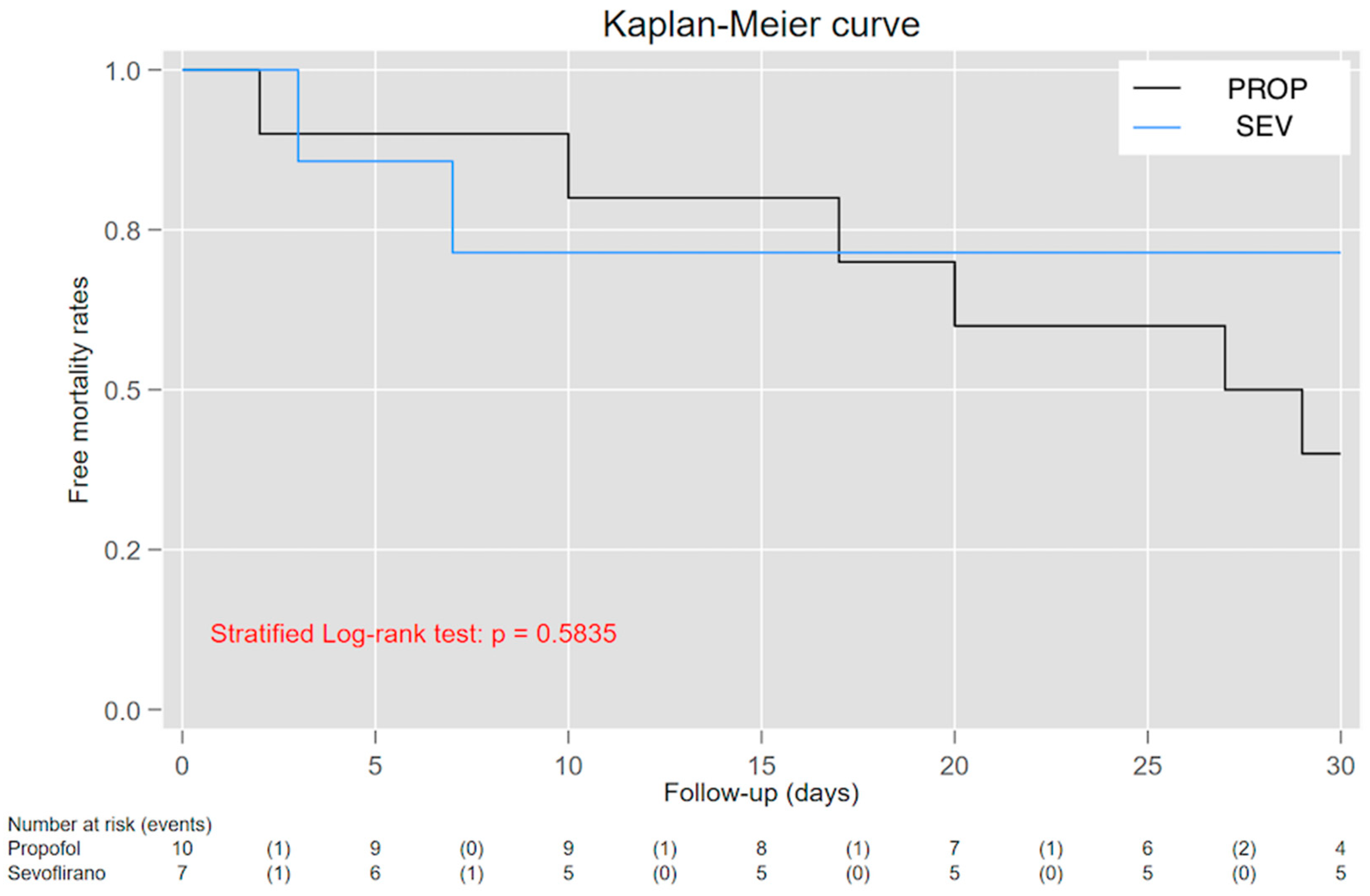
3.3. Effect over 30-Day Mortality
4. Discussion
4.1. Limitations
4.2. Generalizability and Interpretation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hopkins, J. Coronavirus Resource Center. 2021. Available online: https://coronavirus.jhu.edu/ (accessed on 25 April 2022).
- Welker, C.; Huang, J.; Gil, I.; Ramakrishna, H. 2021 Acute Respiratory Distress Syndrome Update, with Coronavirus Disease 2019 Focus. J. Cardiothorac. Vasc. Anesth. 2022, 36, 1188–1195. [Google Scholar] [CrossRef] [PubMed]
- Luz, M.; Barreto, B.B.; de Castro, R.E.V.; Salluh, J.; Dal-Pizzol, F.; Araujo, C.; De Jong, A.; Chanques, G.; Myatra, S.N.; Tobar, E.; et al. Practices in sedation, analgesia, mobilization, delirium, and sleep deprivation in adult intensive care units (SAMDS-ICU): An international survey before and during the COVID-19 pandemic. Ann. Intensive Care 2022, 12, 9. [Google Scholar] [CrossRef] [PubMed]
- Tapaskar, N.; Colon Hidalgo, D.; Koo, G.; Shingada, K.; Rao, S.; Rodriguez, R.; Alcantar, D.; Barrera, D.E.; Lee, R.; Rameshkumar, N.; et al. Sedation Usage in COVID-19 Acute Respiratory Distress Syndrome: A Multicenter Study. Ann. Pharmacother. 2022, 56, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Jabaudon, M.; Boucher, P.; Imhoff, E.; Chabanne, R.; Faure, J.S.; Roszyk, L.; Thibault, S.; Blondonnet, R.; Clairefond, G.; Guérin, R.; et al. Sevoflurane for Sedation in Acute Respiratory Distress Syndrome. A Randomized Controlled Pilot Study. Am. J. Respir. Crit. Care Med. 2017, 195, 792–800. [Google Scholar] [CrossRef]
- Jerath, A.; Ferguson, N.D.; Cuthbertson, B. Inhalational volatile-based sedation for COVID-19 pneumonia and ARDS. Intensive Care Med. 2020, 46, 1563–1566. [Google Scholar] [CrossRef]
- Ferrando, C.; Aguilar, G.; Piqueras, L.; Soro, M.; Moreno, J.; Belda, F.J. Sevoflurane, but not propofol, reduces the lung inflammatory response and improves oxygenation in an acute respiratory distress syndrome model: A randomised laboratory study. Eur. J. Anaesthesiol. 2013, 30, 455–463. [Google Scholar] [CrossRef]
- Meiser, A.; Volk, T.; Wallenborn, J.; Guenther, U.; Becher, T.; Bracht, H.; Schwarzkopf, K.; Knafelj, R.; Faltlhauser, A.; Thal, S.C.; et al. Inhaled isoflurane via the anaesthetic conserving device versus propofol for sedation of invasively ventilated patients in intensive care units in Germany and Slovenia: An open-label, phase 3, randomised controlled, non-inferiority trial. Lancet Respir. Med. 2021, 9, 1231–1240. [Google Scholar] [CrossRef]
- Jerath, A.; Beattie, S.W.; Chandy, T.; Karski, J.; Djaiani, G.; Rao, V.; Yau, T.; Wasowicz, M. Volatile-Based Short-Term Sedation in Cardiac Surgical Patients. Crit. Care Med. 2015, 43, 1062–1069. [Google Scholar] [CrossRef]
- Kong, K.L.; Willatts, S.M.; Prys-Roberts, C. Isoflurane compared with midazolam for sedation in the intensive care unit. BMJ 1989, 298, 1277–1280. [Google Scholar] [CrossRef]
- Kulkarni, A.P.; Bhosale, S.J.; Kalvit, K.R.; Sahu, T.K.; Mohanty, R.; Dhas, M.M. Safety and feasibility of AnaConDaTM to deliver inhaled isoflurane for sedation in patients undergoing elective postoperative mechanical ventilation: A prospective, open-label, interventional trial (INSTINCT I Study). Indian. J. Crit. Care Med. 2022, 26, 906–912. [Google Scholar]
- Steurer, M.; Schläpfer, M.; Steurer, M.; Roth Z’graggen, B.; Booy, C.; Reyes, L.; Spahn, D.R.; Beck-Schimmer, B. The volatile anaesthetic sevoflurane attenuates lipopolysaccharide-induced injury in alveolar macrophages. Clin. Exp. Immunol. 2009, 155, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Suter, D.; Spahn, D.R.; Blumenthal, S.; Reyes, L.; Booy, C.; Z’graggen, B.R.; Beck-Schimmer, B. The immunomodulatory effect of sevoflurane in endotoxin-injured alveolar epithelial cells. Anesth. Analg. 2007, 104, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Voigtsberger, S.; Lachmann, R.A.; Leutert, A.C.; Schläpfer, M.; Booy, C.; Reyes, L.; Urner, M.; Schild, J.; Schimmer, R.C.; Beck-Schimmer, B. Sevoflurane ameliorates gas exchange and attenuates lung damage in experimental lipopolysaccharide-induced lung injury. Anesthesiology. 2009, 111, 1238–1248. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuijs-Moeke, G.J.; Jainandunsing, J.S.; Struys, M.M.R.F. Sevoflurane, a sigh of relief in COVID-19? Br. J. Anaesth. 2020, 125, 118–121. [Google Scholar] [CrossRef] [PubMed]
- Orser, B.A.; Wang, D.S.; Lu, W.Y. Sedating ventilated COVID-19 patients with inhalational anesthetic drugs. EBioMedicine 2020, 55, 102770. [Google Scholar] [CrossRef]
- Suleiman, A.; Qaswal, A.B.; Alnouti, M.; Yousef, M.; Suleiman, B.; El Jarbeh, M.; Alshawabkeh, G.; Bsisu, I.; Santarisi, A.; Ababneh, M. Sedating mechanically ventilated COVID-19 patients with volatile anesthetics: Insights on the last-minute potential weapons. Sci. Pharm. 2021, 89, 6. [Google Scholar] [CrossRef]
- Ammar, M.A.; Sacha, G.L.; Welch, S.C.; Bass, S.N.; Kane-Gill, S.L.; Duggal, A.; Ammar, A.A. Sedation, Analgesia, and Paralysis in COVID-19 Patients in the Setting of Drug Shortages. J. Intensive Care Med. 2021, 36, 157–174. [Google Scholar] [CrossRef]
- Montmeat, D.; Gard, C.; Raux, M.; Constantin, J.M.; Tilleul, P. Shortage of sedatives and neuromuscular blockers during COVID-19 pandemic: The result of an overstocking procedure in French hospitals? Anaesth. Crit. Care Pain Med. 2020, 39, 585–586. [Google Scholar] [CrossRef]
- Shuman, A.G.; Fox, E.; Unguru, Y. Preparing for COVID-19-related Drug Shortages. Ann. Am. Thorac. Soc. 2020, 17, 928–931. [Google Scholar] [CrossRef]
- Payen, J.F.; Chanques, G.; Futier, E.; Velly, L.; Jaber, S.; Constantin, J.M. Sedation for critically ill patients with COVID-19: Which specificities? One size does not fit all. Anaesth. Crit. Care Pain Med. 2020, 39, 341–343. [Google Scholar] [CrossRef]
- Dreucean, D.; Harris, J.E.; Voore, P.; Donahue, K.R. Approach to Sedation and Analgesia in COVID-19 Patients on Venovenous Extracorporeal Membrane Oxygenation. Ann. Pharmacother. 2022, 56, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, Y.; Shiga, T.; Hoshi, N.; Irimada, D.; Saito, H.; Konno, D.; Saito, K.; Yamauchi, M. Sevoflurane administration from extracorporeal membrane oxygenation via the AnaConDa device for a patient with COVID-19: A breakthrough solution for the shortage of intravenous anesthetics. Heart Lung 2022, 56, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Wiedemann, H.P.; Wheeler, A.P.; Bernard, G.R.; Thompson, B.T.; Hayden, D.; deBoisblanc, B.; Connors, A.F., Jr.; Hite, R.D.; Harabin, A.L. Comparison of Two Fluid-Management Strategies in Acute Lung Injury. N. Engl. J. Med. 2006, 354, 2564–2575. [Google Scholar] [CrossRef]
- Badenes Quiles, R. Sedación Con Sevoflurano versus Propofol en Pacientes Con Síndrome de Distrés Respiratorio Agudo Causado por la Infección COVID-19; Instituto de Investigación Sanitaria INCLIVA: Valencia, Spain, 2020. [Google Scholar]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A new simplified acute physiologic score (SAPS-II) based on a European/North-American multicenter study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.F.; Matthay, M.A.; Luce, J.M.; Flick, M.R. An expanded definition of the adult respiratory distress syndrome. Am. Rev. Respir. Dis. 1988, 138, 720–723. [Google Scholar] [CrossRef] [PubMed]
- Chanques, G.; Constantin, J.M.; Devlin, J.W.; Ely, E.W.; Fraser, G.L.; Gélinas, C.; Girard, T.D.; Guérin, C.; Jabaudon, M.; Jaber, S.; et al. Analgesia and sedation in patients with ARDS. Intensive Care Med. 2020, 46, 2342–2356. [Google Scholar] [CrossRef] [PubMed]
- Devlin, J.W.; Skrobik, Y.; Gélinas, C.; Needham, D.M.; Slooter, A.J.C.; Pandharipande, P.P.; Watson, P.L.; Weinhouse, G.L.; Nunnally, M.E.; Rochwerg, B.; et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit. Care Med. 2018, 46, e825–e873. [Google Scholar] [CrossRef]
- Jerath, A.; Panckhurst, J.; Parotto, M.; Lightfoot, N.; Wasowicz, M.; Ferguson, N.D.; Steel, A.; Beattie, W.S. Safety and Efficacy of Volatile Anesthetic Agents Compared With Standard Intravenous Midazolam/Propofol Sedation in Ventilated Critical Care Patients: A Meta-analysis and Systematic Review of Prospective Trials. Anesth. Analg. 2017, 124, 1190–1199. [Google Scholar] [CrossRef]
- Flinspach, A.N.; Zacharowski, K.; Ioanna, D.; Adam, E.H. Volatile Isoflurane in Critically Ill Coronavirus Disease 2019 Patients—A Case Series and Systematic Review. Crit. Care Explor. 2020, 2, e0256. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.; Na, S.; Bin Kim, H.; Joo, H.J.; Kim, J. Inhalation sedation for postoperative patients in the intensive care unit: Initial sevoflurane concentration and comparison of opioid use with propofol sedation. Acute Crit. Care 2020, 35, 197–204. [Google Scholar] [CrossRef]
- Meiser, A.; Laubenthal, H. Inhalational anaesthetics in the ICU: Theory and practice of inhalational sedation in the ICU, economics, risk-benefit. Best Pr. Res. Clin. Anaesthesiol. 2005, 19, 523–538. [Google Scholar] [CrossRef]
- Mesnil, M.; Capdevila, X.; Bringuier, S.; Trine, P.O.; Falquet, Y.; Charbit, J.; Roustan, J.-P.; Chanques, G.; Jaber, S. Long-term sedation in intensive care unit: A randomized comparison between inhaled sevoflurane and intravenous propofol or midazolam. Intensive Care Med. 2011, 37, 933–941. [Google Scholar] [CrossRef]
- Schläpfer, M.; Leutert, A.C.; Voigtsberger, S.; Lachmann, R.A.; Booy, C.; Beck-Schimmer, B. Sevoflurane reduces severity of acute lung injury possibly by impairing formation of alveolar oedema. Clin. Exp. Immunol. 2012, 168, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Bellgardt, M.; Bomberg, H.; Herzog-Niescery, J.; Dasch, B.; Vogelsang, H.; Weber, T.P.; Steinfort, C.; Uhl, W.; Wagenpfeil, S.; Volk, T.; et al. Survival after long-term isoflurane sedation as opposed to intravenous sedation in critically ill surgical patients: Retrospective analysis. Eur. J. Anaesthesiol. 2016, 33, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Belda, J.F.; Soro, M.; Badenes, R.; Meiser, A.; García, M.L.; Aguilar, G.; Martí, F.J. The predictive performance of a pharmacokinetic model for manually adjusted infusion of liquid sevofluorane for use with the Anesthetic-Conserving Device (AnaConDa): A clinical study. Anesth. Analg. 2008, 106, 1207–1214. [Google Scholar] [CrossRef] [PubMed]
- Wolf, A.; Mörgeli, R.; Müller, A.; Weiss, B.; Spies, C. Delirium, analgesia, and sedation in intensive care medicine: Development of a protocol-based management approach. Med. Klin. Intensiv. Notfmed. 2017, 112, 65–74. [Google Scholar] [CrossRef]
- Peyró, R.; Soro, M.; Aldecoa, C.; Valía, J.C.; Ramos, F.; Acosta, F.; Álvarez, F.; Navarro, J.; Soria, C.; Belda, J. Protocolo Terapéutico Asistencial Para la Sedación Inhalatoria Con Sevoflurano a Través Del Dispositivo AnaConDa® en Pacientes Ingresados en la Unidad de Cuidados Críticos; Sección de Cuidados Críticos de la SEDAR: Madrid, Spain, 2010; pp. 1–12. [Google Scholar]
- Landoni, G.; Belloni, O.; Russo, G.; Bonaccorso, A.; Carà, G.; Jabaudon, M. Inhaled Sedation for Invasively Ventilated COVID-19 Patients: A Systematic Review. J. Clin. Med. 2022, 11, 2500. [Google Scholar] [CrossRef]
- Kermad, A.; Speltz, J.; Danziger, G.; Mertke, T.; Bals, R.; Volk, T.; Lepper, P.M.; Meiser, A. Comparison of isoflurane and propofol sedation in critically ill COVID-19 patients—A retrospective chart review. J. Anesth. 2021, 35, 625–632. [Google Scholar] [CrossRef]
- Sackey, P.V.; Martling, C.R.; Granath, F.; Radell, P.J. Prolonged isoflurane sedation of intensive care unit patients with the Anesthetic Conserving Device. Crit. Care Med. 2004, 32, 2241–2246. [Google Scholar] [CrossRef]
- Sackey, P.V.; Martling, C.R.; Carlswärd, C.; Sundin, Ö.; Radell, P.J. Short- and long-term follow-up of intensive care unit patients after sedation with isoflurane and midazolam—A pilot study*. Crit. Care Med. 2008, 36, 801–806. [Google Scholar] [CrossRef]
- Meiser, A.; Sirtl, C.; Bellgardt, M.; Lohmann, S.; Garthoff, A.; Kaiser, J.; Hügler, P.; Laubenthal, H.J. Desflurane compared with propofol for postoperative sedation in the intensive care unit. Br. J. Anaesth. 2003, 90, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Lee, J.E.; Kim, H.Y.; Kim, J. Volatile sedation in the intensive care unit. Medicine 2017, 96, e8976. [Google Scholar] [CrossRef]
- Coupet, R.; Schläpfer, M.; Neff, T.A.; Boucher, P.; Bailly, P.; Bellgardt, M.; Badenes, R.; Carbonell, J.; Becher, T.; Varillon, C.; et al. Inhaled Sedation in Patients with COVID-19-Related Acute Respiratory Distress Syndrome: An International Retrospective Study †. J. Clin. Med. 2023, 12, 12. [Google Scholar] [CrossRef] [PubMed]
- Du, X.; Jiang, C.; Lv, Y.; Dull, R.O.; Zhao, Y.Y.; Schwartz, D.E.; Hu, G. Isoflurane promotes phagocytosis of apoptotic neutrophils through AMPK-mediated ADAM17/Mer signaling. PLoS ONE. 2017, 12, e0180213. [Google Scholar] [CrossRef] [PubMed]
- Ohsumi, A.; Marseu, K.; Slinger, P.; McRae, K.; Kim, H.; Guan, Z.; Hwang, D.M.; Liu, M.; Keshavjee, S.; Cypel, M. Sevoflurane Attenuates Ischemia-Reperfusion Injury in a Rat Lung Transplantation Model. Ann. Thorac. Surg. 2017, 103, 1578–1586. [Google Scholar] [CrossRef]
- Fortis, S.; Spieth, P.M.; Lu, W.Y.; Parotto, M.; Haitsma, J.J.; Slutsky, A.S.; Zhong, N.; Mazer, C.D.; Zhang, H. Effects of anesthetic regimes on inflammatory responses in a rat model of acute lung injury. Intensive Care Med. 2012, 38, 1548–1555. [Google Scholar] [CrossRef]
- Kellner, P.; Müller, M.; Piegeler, T.; Eugster, P.; Booy, C.; Schläpfer, M.; Beck-Schimmer, B. Sevoflurane Abolishes Oxygenation Impairment in a Long-Term Rat Model of Acute Lung Injury. Anesth. Analg. 2017, 124, 194–203. [Google Scholar] [CrossRef]
- Blondonnet, R.; Balde, A.; Zhai, R.; Pereira, B.; Futier, E.; Bazin, J.E.; Godet, T.; Constantin, J.-M.; Lambert, C.; Jabaudon, M. Use of volatile anesthetics for sedation in the ICU during the COVID-19 pandemic: A national survey in France (VOL’ICU 2 study). PLoS ONE 2022, 17, e0278090. [Google Scholar] [CrossRef]
- Bansbach, J.; Wenz, J.; Kaufmann, K.; Heinrich, S.; Kalbhenn, J. Sevoflurane in combination with esketamine is an effective sedation regimen in COVID-19 patients enabling assisted spontaneous breathing even during prone positioning. Anaesthesiol. Intensive Ther. 2022, 54, 23–29. [Google Scholar] [CrossRef]
- Kaura, V.; Hopkins, P.M. Sevoflurane may not be a complete sigh of relief in COVID-19. Br. J. Anaesth. 2020, 125, e487–e488. [Google Scholar] [CrossRef]
- Bourdeaux, D.; Sautou-Miranda, V.; Montagner, A.; Perbet, S.; Constantin, J.M.; Bazin, J.E.; Chopineau, J. Simple assay of plasma sevoflurane and its metabolite hexafluoroisopropanol by headspace GC–MS. J. Chromatogr. B 2010, 878, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Perbet, S.; Bourdeaux, D.; Lenoire, A.; Biboulet, C.; Pereira, B.; Sadoune, M.; Plaud, B.; Launay, J.-M.; Bazin, J.-E.; Sautou, V.; et al. Sevoflurane for procedural sedation in critically ill patients: A pharmacokinetic comparative study between burn and non-burn patients. Anaesth. Crit. Care Pain. Med. 2018, 37, 551–556. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Visits | Selection | Randomization | Visit 1 | Visit 2 | Final Visit |
|---|---|---|---|---|---|
| Time | −24 h | D0 | D1 | D2 | D30 |
| Procedures and testing | |||||
| Informed consent | X | ||||
| Inclusion/exclusion criteria | X | ||||
| Medical records | X | ||||
| Anthropometric data | X | ||||
| Clinical data | X | ||||
| Respiratory values | X | ||||
| Hemodynamic values | X | ||||
| Blood sample | X | ||||
| Respiratory sample | X | ||||
| Treatment | |||||
| Randomization | X | ||||
| Sedative agent administration | X | X | X | ||
| Other treatments | X | X | X | X | |
| Adverse events | X | X | X |
| Patient Characteristics | PROP | SEV | Total | p Value | Missings |
|---|---|---|---|---|---|
| Age, years, mean (sd) | 62.9 (12.1) | 64.4 (14.6) | 63.5 (12.7) | 0.816 | 0/17 (0.00) |
| Gender (female), n (%) | 4 (40.0) | 4 (57.1) | 8 (47.1) | 0.486 | 0/17 (0.00) |
| Height, m, mean (sd) | 1.66 (0.09) | 1.68 (0.06) | 1.67 (0.08) | 0.613 | 1/17 (5.88) |
| Weight, kg, mean (sd) | 87.8 (31.4) | 85.1 (22.3) | 86.6 (27.0) | 0.854 | 1/17 (5.88) |
| BMI, (kg/m2), mean (sd) | 31.1 (7.4) | 29.8 (6.0) | 30.5 (6.6) | 0.709 | 1/17 (5.88) |
| Baseline Ventilatory Settings, Mean (SD) | PROP | SEV | Total | p Value | Missings |
|---|---|---|---|---|---|
| End-expiratory lung volume, mL/kg | 6.2 (1.0) | 7.0 (1.8) | 6.5 (1.4) | 0.293 | 2/17 (11.76) |
| PEEP, cmH2O | 8.6 (2.9) | 9.7 (1.5) | 9.1 (2.4) | 0.365 | 0/17 (0.00) |
| Inspiratory pressure, cmH2O | 15.6 (10.4) | 22.0 (2.2) | 18.4 (8.4) | 0.170 | 3/17 (17.65) |
| Lung compliance, L/cmH2O | 41.5 (24.4) | 41.2 (8.5) | 41.4 (18.6) | 0.975 | 3/17 (17.65) |
| Airway resistance, cmH2O/L/s | 19.5 (20.3) | 15.0 (3.8) | 17.6 (15.3) | 0.605 | 3/17 (17.65) |
| FiO2 (%) | 83.0 (17.0) | 79.3 (19.7) | 81.5 (17.7) | 0.684 | 0/17 (0.00) |
| Arterial pH | 7.35 (0.10) | 7.37 (0.14) | 7.36 (0.12) | 0.759 | 0/17 (0.00) |
| Respiratory rate, breaths per minute | 21.9 (4.1) | 18.2 (3.9) | 20.4 (4.3) | 0.104 | 2/17 (11.76) |
| PaCO2, mmHg | 48.5 (15.2) | 45.4 (14.2) | 47.2 (14.4) | 0.680 | 0/17 (0.00) |
| PaO2/FiO2 | 112.3 (45.3) | 146.6 (72.2) | 126.4 (58.4) | 0.246 | 0/17 (0.00) |
| Heart rate, beats per minute | 64.1 (33.8) | 81.9 (15.7) | 71.4 (28.6) | 0.217 | 0/17 (0.00) |
| Mean arterial pressure, mmHg | 82.0 (12.6) | 79.0 (13.5) | 80.8 (12.7) | 0.646 | 0/17 (0.00) |
| BIS | 44.0 (9.3) | 41.0 (5.2) | 42.5 (7.4) | 0.470 | 3/17 (17.65) |
| Ventilatory Settings on D1, Mean (SD) | PROP | SEV | Total | p Value | Missings |
|---|---|---|---|---|---|
| End-expiratory lung volume, mL/kg | 11.9 (18.7) | 6.1 (0.4) | 9.5 (14.3) | 0.432 | 0/17 (0.00) |
| PEEP, cmH2O | 9.9 (3.4) | 10.1 (1.7) | 10.0 (2.7) | 0.864 | 0/17 (0.00) |
| Inspiratory pressure, cmH2O | 22.9 (5.5) | 21.0 (4.1) | 22.1 (4.9) | 0.501 | 3/17 (17.65) |
| Lung compliance, L/cmH2O | 33.8 (14.8) | 44.3 (14.7) | 38.7 (15.2) | 0.191 | 2/17 (11.76) |
| Airway resistance, cmH2O/L/s | 10.4 (8.4) | 14.3 (5.5) | 12.1 (7.3) | 0.338 | 3/17 (17.65) |
| FiO2 (%) | 81.5 (21.1) | 69.9 (16.3) | 76.7 (19.6) | 0.240 | 0/17 (0.00) |
| Arterial pH | 7.39 (0.07) | 7.35 (0.14) | 7.37 (0.10) | 0.381 | 0/17 (0.00) |
| Respiratory rate, breaths per minute | 20.5 (5.2) | 17.0 (3.8) | 19.1 (4.9) | 0.151 | 0/17 (0.00) |
| PaCO2, mmHg | 48.1 (12.5) | 52.0 (15.2) | 49.7 (13.4) | 0.570 | 0/17 (0.00) |
| PaO2/FiO2 | 135.7 (74.6) | 179.1 (77.3) | 153.6 (76.5) | 0.262 | 0/17 (0.00) |
| Heart rate, beats per minute | 76.4 (18.9) | 66.0 (30.1) | 72.1 (23.8) | 0.393 | 0/17 (0.00) |
| Mean arterial pressure, mmHg | 73.2 (9.2) | 78.3 (10.8) | 75.3 (9.9) | 0.311 | 0/17 (0.00) |
| BIS | 44.0 (9.3) | 41.0 (5.2) | 42.5 (7.4) | 0.470 | 3/17 (17.65) |
| Ventilatory Settings on D2, Mean (SD) | PROP | SEV | Total | p Value | Missings |
|---|---|---|---|---|---|
| End-expiratory lung volume, mL/kg | 11.8 (18.7) | 7.3 (2.6) | 9.9 (14.3) | 0.540 | 0/17 (0.00) |
| PEEP, cmH2O | 10.1 (2.6) | 9.9 (1.7) | 10.0 (2.2) | 0.832 | 0/17 (0.00) |
| Inspiratory pressure, cmH2O | 21.1 (5.1) | 24.2 (4.4) | 22.4 (4.9) | 0.268 | 3/17 (17.65) |
| Lung compliance, L/cmH2O | 34.0 (15.8) | 37.4 (13.9) | 35.7 (14.4) | 0.674 | 3/17 (17.65) |
| Airway resistance, cmH2O/L/s | 12.9 (11.2) | 14.2 (3.4) | 13.4 (8.5) | 0.792 | 3/17 (17.65) |
| FiO2 (%) | 71.5 (15.3) | 67.1 (16.8) | 69.7 (15.6) | 0.587 | 0/17 (0.00) |
| Arterial pH | 7.42 (0.04) | 7.31 (0.11) | 7.38 (0.09) | 0.010 ** | 0/17 (0.00) |
| Respiratory rate, breaths per minute | 19.7 (3.6) | 18.7 (4.9) | 19.3 (4.0) | 0.635 | 0/17 (0.00) |
| PaCO2, mmHg | 44.5 (7.8) | 59.1 (15.5) | 50.5 (13.4) | 0.021 ** | 0/17 (0.00) |
| PaO2/FiO2 | 160.7 (81.2) | 173.3 (90.0) | 165.9 (82.4) | 0.767 | 0/17 (0.00) |
| Heart rate, beats per minute | 73.6 (20.5) | 80.7 (15.4) | 76.5 (18.4) | 0.451 | 0/17 (0.00) |
| Mean arterial pressure, mmHg | 78.2 (13.6) | 71.3 (7.9) | 75.4 (11.8) | 0.247 | 0/17 (0.00) |
| BIS | 40.1 (10.0) | 44.0 (19.1) | 41.9 (14.5) | 0.624 | 2/17 (11.76) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Castro, S.; Monleón, B.; Puig, J.; Ferrer Gomez, C.; Quesada, M.; Pestaña, D.; Balvis, A.; Maseda, E.; de la Rica, A.S.; Feijoo, A.M.; et al. Sedation with Sevoflurane versus Propofol in COVID-19 Patients with Acute Respiratory Distress Syndrome: Results from a Randomized Clinical Trial. J. Pers. Med. 2023, 13, 925. https://doi.org/10.3390/jpm13060925
Martínez-Castro S, Monleón B, Puig J, Ferrer Gomez C, Quesada M, Pestaña D, Balvis A, Maseda E, de la Rica AS, Feijoo AM, et al. Sedation with Sevoflurane versus Propofol in COVID-19 Patients with Acute Respiratory Distress Syndrome: Results from a Randomized Clinical Trial. Journal of Personalized Medicine. 2023; 13(6):925. https://doi.org/10.3390/jpm13060925
Chicago/Turabian StyleMartínez-Castro, Sara, Berta Monleón, Jaume Puig, Carolina Ferrer Gomez, Marta Quesada, David Pestaña, Alberto Balvis, Emilio Maseda, Alejandro Suárez de la Rica, Ana Monero Feijoo, and et al. 2023. "Sedation with Sevoflurane versus Propofol in COVID-19 Patients with Acute Respiratory Distress Syndrome: Results from a Randomized Clinical Trial" Journal of Personalized Medicine 13, no. 6: 925. https://doi.org/10.3390/jpm13060925