
Physiological Modeling of Hemodynamic Responses to Sodium Nitroprusside
Abstract
:1. Introduction
2. Methods
2.1. Base Computational Model
2.2. Addition of SNP to the Model
2.3. Animal Data
2.4. Individual Model Fitting
- First, using the initial starting parameters shown in Table 1, a plasma SNP concentration was calculated from the administration rates, φ1 (half-life), and φ2 (infusion-to-onset delay).
- Cardiac stroke volume was calculated using Equation (12b) above and the initial θ1–4 and φ5 parameters in Table 1.
- The root-mean-squared error (RMSE) was then calculated between the measured SV and the simulated SV. RMSE was used as the minimization criterion as this is the parameter reported by the authors in the original Bighamian model, so it made a useful direct comparator.
- Each of the parameters θ1, θ2, θ3, θ4, and φ5 was individually increased and decreased by 10%, and the cardiac stroke volume and resulting RMSE from the new set was recalculated. The modification that resulted in the largest decrease in RMSE was implemented.
- Step 4 was repeated until no modification of a parameter resulted in at least a 1% reduction in RMSE.
- φ1 and φ2 were then individually increased and decreased by 10% and the stroke volume and RMSE recalculated, and the process returned to step 1, calculating new plasma concentrations using the new values and then repeating the fitting process in steps 2–5. The change resulting in the largest reduction of RMSE for φ1 and φ2 was implemented.
- Step 6 was continued until no change in φ1 and φ2 parameters resulted in at least a 1% reduction in RMSE.
- Finally, once the process above was completed, since φ3 and φ4 affect only MAP, they were calculated last using a grid search process identical to steps 4 and 5 above but using a simulated MAP instead of a simulated SV (with said MAP calculated using the previously calculated simulated SV and the model parameters in Equation (14b)) against recorded MAP to calculate RMSE scores.
2.5. Statistical Analysis and Reporting
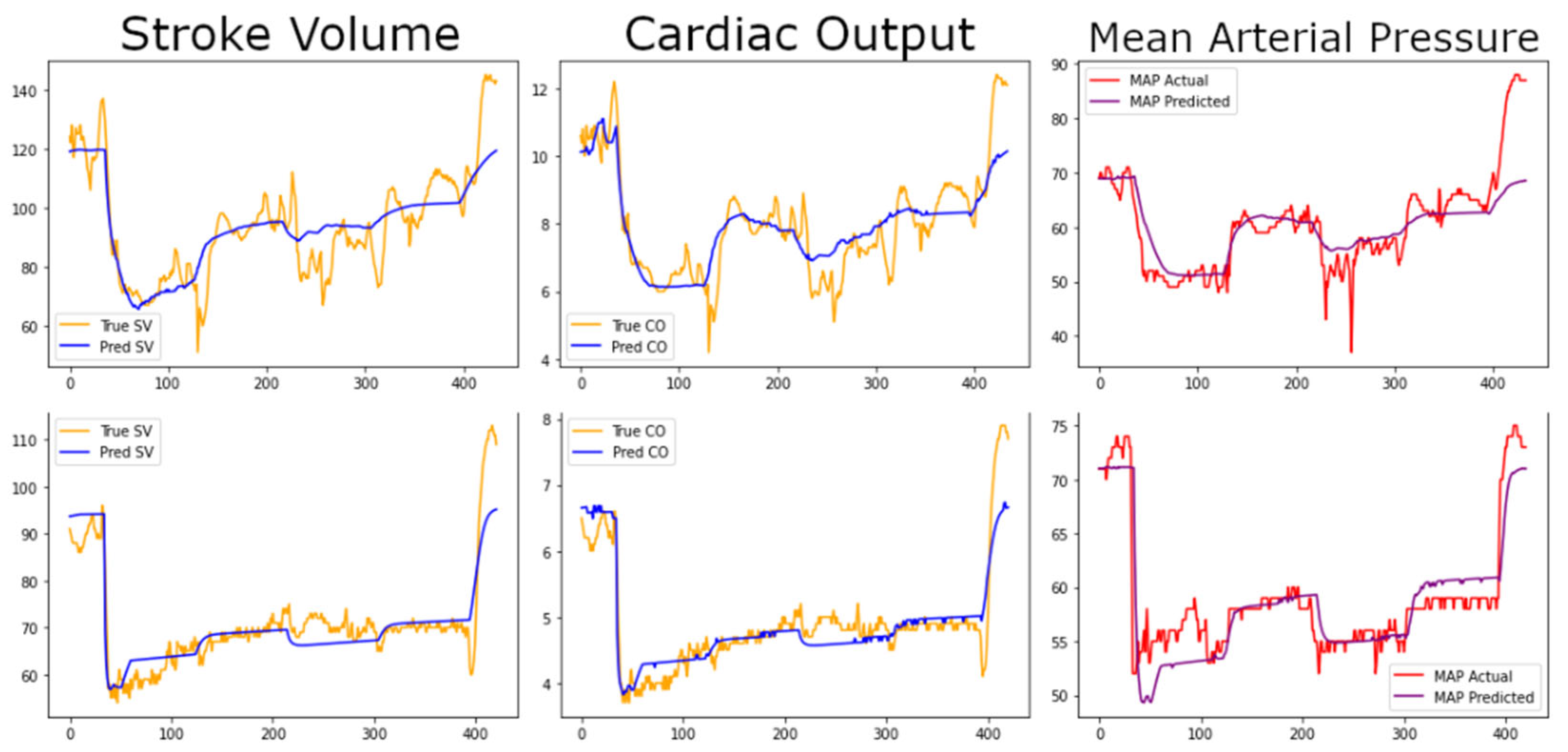
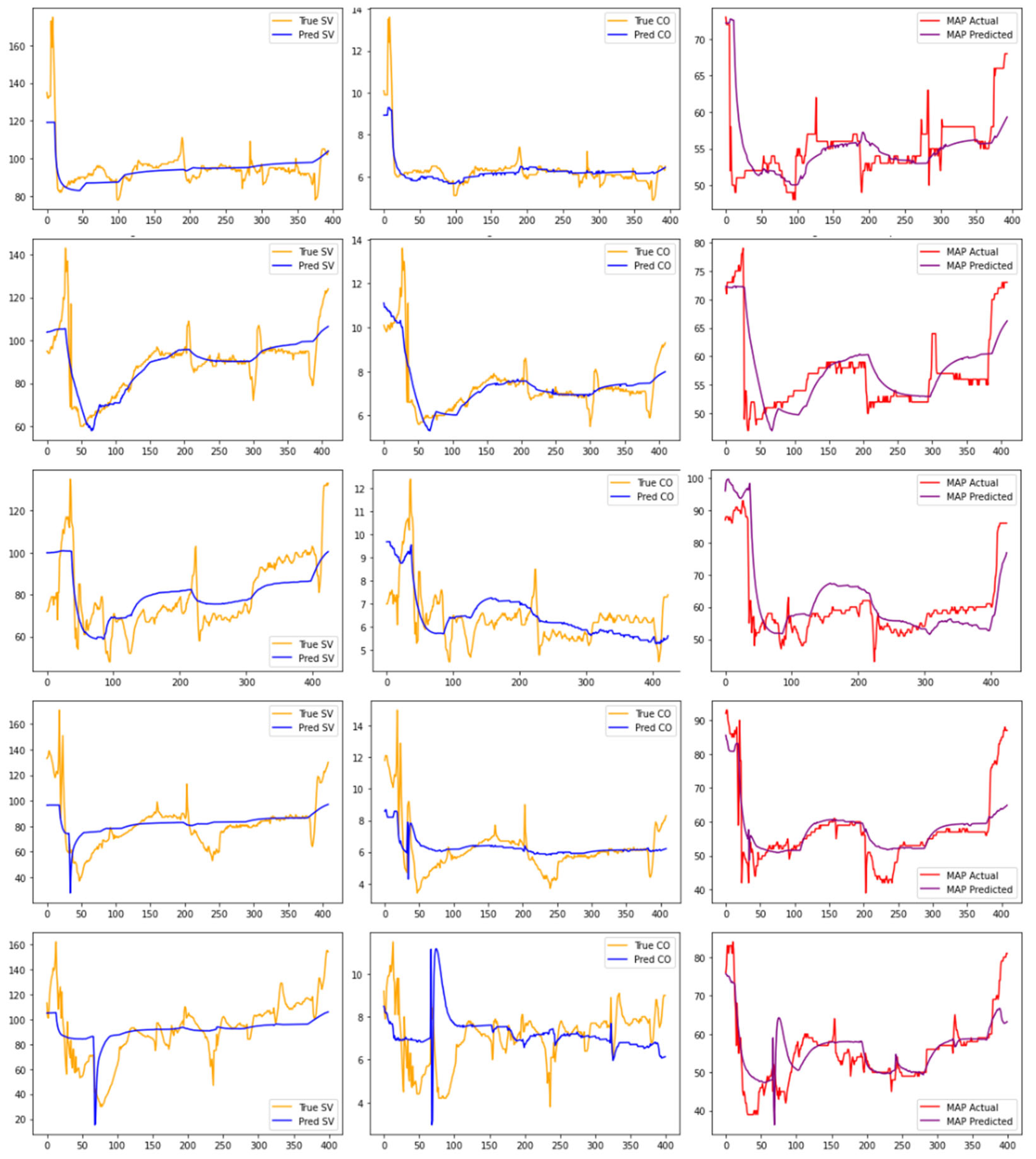
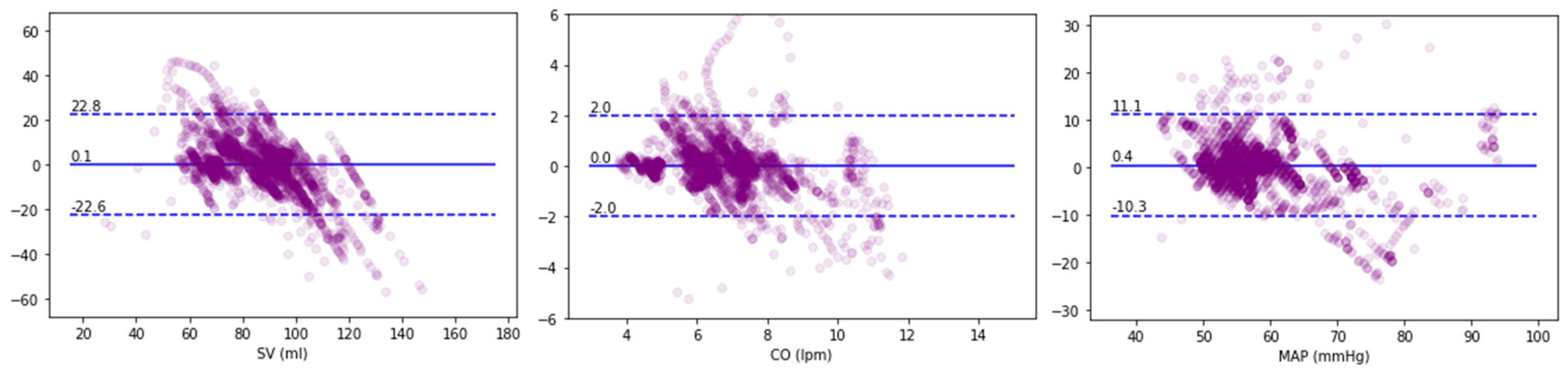
3. Results
4. Discussion
4.1. Limitations
4.2. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhao, Q.; Yu, H.; Ji, M.; Zhao, Y.; Chen, X. Computational Model Development of Drug-Target Interaction Prediction: A Review. Curr. Protein Pept. Sci. 2019, 20, 492–494. [Google Scholar] [CrossRef]
- Collin, C.B.; Gebhardt, T.; Golebiewski, M.; Karaderi, T.; Hillemanns, M.; Khan, F.M.; Salehzadeh-Yazdi, A.; Kirschner, M.; Krobitsch, S.; EU-STANDS4PM consortium; et al. Computational Models for Clinical Applications in Personalized Medicine—Guidelines and Recommendations for Data Integration and Model Validation. J. Pers. Med. 2022, 12, 166. [Google Scholar] [CrossRef] [PubMed]
- Chase, J.G.; Preiser, J.-C.; Dickson, J.L.; Pironet, A.; Chiew, Y.S.; Pretty, C.G.; Shaw, G.M.; Benyo, B.; Moeller, K.; Safaei, S.; et al. Next-generation, personalised, model-based critical care medicine: A state-of-the art review of in silico virtual patient models, methods, and cohorts, and how to validation them. BioMedi. Eng. Online 2018, 17, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leiderman, K.; Sindi, S.S.; Monroe, D.M.; Fogelson, A.L.; Neeves, K.B. The Art and Science of Building a Computational Model to Understand Hemostasis. Semin. Thromb. Hemost. 2021, 47, 129–138. [Google Scholar] [CrossRef]
- Parvinian, B.; Scully, C.; Wiyor, H.; Kumar, A.; Weininger, S. Regulatory Considerations for Physiological Closed-Loop Controlled Medical Devices Used for Automated Critical Care: Food and Drug Administration Workshop Discussion Topics. Anesth. Analg. 2018, 126, 1916–1925. [Google Scholar] [CrossRef]
- Zhang, Q.; Li, J.; Middleton, A.; Bhattacharya, S.; Conolly, R.B. Bridging the Data Gap From in vitro Toxicity Testing to Chemical Safety Assessment Through Computational Modeling. Front. Public Health 2018, 6, 261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cappon, F.; Wu, T.; Papaioannou, T.; Du, X.; Hsu, P.-L.; Khir, A.W. Mock circulatory loops used for testing cardiac assist devices: A review of computational and experimental models. Int. J. Artif. Organs 2021, 44, 793–806. [Google Scholar] [CrossRef]
- Parvinian, B.; Pathmanathan, P.; Daluwatte, C.; Yaghouby, F.; Gray, R.A.; Weininger, S.; Morrison, T.M.; Scully, C.G. Credibility Evidence for Computational Patient Models Used in the Development of Physiological Closed-Loop Controlled Devices for Critical Care Medicine. Front. Physiol. 2019, 10, 220. [Google Scholar] [CrossRef]
- Scully, C.G.; Pathmanathan, P.; Daluwatte, C.; Yaghouby, F.; Gray, R.A.; Weininger, S.; Morrison, T.M.; Parvinian, B. Applying a Computational Model Credibility Framework to Physiological Closed-Loop Controlled Medical Device Testing. In Proceedings of the 2018 IEEE Life Sciences Conference (LSC), Montreal, QC, Canada, 28–30 October 2018; pp. 130–133. [Google Scholar] [CrossRef]
- Parvinian, B.; Bighamian, R.; Scully, C.G.; Hahn, J.-O.; Pathmanathan, P. Credibility Assessment of a Subject-Specific Mathematical Model of Blood Volume Kinetics for Prediction of Physiological Response to Hemorrhagic Shock and Fluid Resuscitation. Front. Physiol. 2021, 12, 705222. [Google Scholar] [CrossRef]
- Bighamian, R.; Parvinian, B.; Scully, C.G.; Kramer, G.; Hahn, J.-O. Control-oriented physiological modeling of hemodynamic responses to blood volume perturbation. Control Eng. Pract. 2018, 73, 149–160. [Google Scholar] [CrossRef]
- Bighamian, R.; Reisner, A.T.; Hahn, J.-O. A Lumped-Parameter Subject-Specific Model of Blood Volume Response to Fluid Infusion. Front. Physiol. 2016, 7, 390. [Google Scholar] [CrossRef] [Green Version]
- Joosten, A.; Delaporte, A.; Alexander, B.; Su, F.; Creteur, J.; Vincent, J.-L.; Cannesson, M.; Rinehart, J. Automated Titration of Vasopressor Infusion Using a Closed-loop Controller: In Vivo Feasibility Study Using a Swine Model. Anesthesiology 2019, 130, 394–403. [Google Scholar] [CrossRef]
- Desebbe, O.; Rinehart, J.; van der Linden, P.; Cannesson, M.; Delannoy, B.; Vigneron, M.; Curtil, A.; Hautin, E.; Vincent, J.-L.; Duranteau, J.; et al. Control of Postoperative Hypotension Using a Closed-Loop System for Norepinephrine Infusion in Patients After Cardiac Surgery: A Randomized Trial. Anesth. Analg. 2022, 134, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Joosten, A.; Rinehart, J.; van der Linden, P.; Alexander, B.; Penna, C.; De Montblanc, J.; Cannesson, M.; Vincent, J.-L.; Vicaut, E.; Duranteau, J. Computer-assisted Individualized Hemodynamic Management Reduces Intraoperative Hypotension in Intermediate- and High-risk Surgery: A Randomized Controlled Trial. Anesthesiology 2021, 135, 258–272. [Google Scholar] [CrossRef] [PubMed]
- Joosten, A.; Chirnoaga, D.; van der Linden, P.; Barvais, L.; Alexander, B.; Duranteau, J.; Vincent, J.-L.; Cannesson, M.; Rinehart, J. Automated closed-loop versus manually controlled norepinephrine infusion in patients undergoing intermediate- to high-risk abdominal surgery: A randomised controlled trial. Br. J. Anaesth. 2021, 126, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Zaouter, C.; Joosten, A.; Rinehart, J.; Struys, M.M.R.F.; Hemmerling, T.M. Autonomous Systems in Anesthesia: Where Do We Stand in 2020? A Narrative Review. Anesth. Analg. 2020, 130, 1120–1132. [Google Scholar] [CrossRef]
- Rinehart, J.; Lee, S.; Saugel, B.; Joosten, A. Automated Blood Pressure Control. Semin. Respir. Crit. Care Med. 2020, 42, 047–058. [Google Scholar] [CrossRef]
- Coeckelenbergh, S.; Zaouter, C.; Alexander, B.; Cannesson, M.; Rinehart, J.; Duranteau, J.; van der Linden, P.; Joosten, A. Automated systems for perioperative goal-directed hemodynamic therapy. J. Anesth. 2019, 34, 104–114. [Google Scholar] [CrossRef]
- Rinehart, J.; Cannesson, M. Automation and the Safer Future of Anesthesia. In Anesthesiology News; McMahon Publishing: New York, NY, USA, 2012; pp. 53–56. [Google Scholar]
- Hottinger, D.G.; Beebe, D.S.; Kozhimannil, T.; Prielipp, R.C.; Belani, K.G. Sodium nitroprusside in 2014: A clinical concepts review. J. Anaesthesiol. Clin. Pharmacol. 2014, 30, 462–471. [Google Scholar] [CrossRef]
- Chou, J.; Rinehart, J.B. Computer simulated modeling of healthy and diseased right ventricular and pulmonary circulation. J. Clin. Monit. Comput. 2018, 32, 1015–1024. [Google Scholar] [CrossRef]
- Rinehart, J.; Lee, C.; Cannesson, M.; Dumont, G. Closed-Loop Fluid Resuscitation: Robustness Against Weight and Cardiac Contractility Variations. Anesth. Analg. 2013, 117, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Rinehart, J.; Alexander, B.; Manach, Y.L.; Hofer, C.K.; Tavernier, B.; Kain, Z.N.; Cannesson, M. Evaluation of a novel closed-loop fluid-administration system based on dynamic predictors of fluid responsiveness: An in silico simulation study. Crit. Care 2011, 15, R278. [Google Scholar] [CrossRef] [Green Version]
- Rinehart, J.; Lilot, M.; Lee, C.; Joosten, A.; Huynh, T.; Canales, C.; Imagawa, D.; Demirjian, A.; Cannesson, M. Closed-loop assisted versus manual goal-directed fluid therapy during high-risk abdominal surgery: A case–control study with propensity matching. Crit. Care 2015, 19, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joosten, A.; Huynh, T.; Suehiro, K.; Canales, C.; Cannesson, M.; Rinehart, J. Goal-Directed fluid therapy with closed-loop assistance during moderate risk surgery using noninvasive cardiac output monitoring: A pilot study. Br. J. Anaesth. 2015, 114, 886–892. [Google Scholar] [CrossRef] [Green Version]
- Joosten, A.; Alexander, B.; Delaporte, A.; Lilot, M.; Rinehart, J.; Cannesson, M. Perioperative goal directed therapy using automated closed-loop fluid management: The future? Anaesthesiol. Intensive Ther. 2015, 47, 517–523. [Google Scholar] [CrossRef]
- Rinehart, J.; Lee, C.; Canales, C.; Kong, A.; Kain, Z.; Cannesson, M. Closed-Loop Fluid Administration Compared to Anesthesiologist Management for Hemodynamic Optimization and Resuscitation During Surgery: An In Vivo Study. Anesth. Analg. 2013, 117, 1119–1129. [Google Scholar] [CrossRef]
- Rinehart, J.; Le Manach, Y.; Douiri, H.; Lee, C.; Lilot, M.; Le, K.; Canales, C.; Cannesson, M. First closed-loop goal directed fluid therapy during surgery: A pilot study. Ann. Fr. D’anesthesie Reanim. 2014, 33, e35–e41. [Google Scholar] [CrossRef] [PubMed]
- Rinehart, J.; Chung, E.; Canales, C.; Cannesson, M. Intraoperative Stroke Volume Optimization Using Stroke Volume, Arterial Pressure, and Heart Rate: Closed-Loop (Learning Intravenous Resuscitator) Versus Anesthesiologists. J. Cardiothorac. Vasc. Anesth. 2012, 26, 933–939. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Model Parameter | Initial Value | 1 | 2 | 3 | 4 | 5 | 6 | 7 | Mean | SD | % Var |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Au (crystalloid) | 1.9 | (fixed) | 1.9 | 0 | 0 | ||||||
| Au (colloid) | 0.0 | (fixed) | 0.0 | 0 | 0 | ||||||
| Av | 0.13 | (fixed) | 0.13 | 0 | 0 | ||||||
| Kp | 0.0031 | (fixed) | 0.0031 | 0 | 0 | ||||||
| Ki | 1.09 | (fixed) | 1.09 | 0 | 0 | ||||||
| θ1 | 13 | 16 | 12 | 16 | 14 | 13 | 13 | 14 | 14 | 1.4 | 10 |
| θ2 | −1.0 | −4.3 | 0.0 | 0.0 | −6.9 | −5.0 | −4.6 | −4.9 | −3.7 | 2.6 | −72 |
| θ3 | 0.29 | 0.58 | 0.60 | 0.59 | 0.58 | 0.59 | 0.65 | 0.68 | 0.61 | 0.04 | 6 |
| θ4 | −420 | 46 | 0 | 0 | 0 | 101 | 130 | 175 | 65 | 71 | 111 |
| φ1 | 120 | 144 | 46 | 187 | 207 | 108 | 120 | 120 | 133.2 | 53.2 | 40 |
| φ2 | 60 | 104 | 72 | 179 | 149 | 60 | 60 | 60 | 98 | 49 | 50 |
| φ3 | 200 | 1013 | 300 | 675 | 675 | 102 | 200 | 300 | 466.4 | 327.6 | 70 |
| φ4 | 1.0 | 0.73 | 1.00 | 0.73 | 0.81 | 1.56 | 1.00 | 1.00 | 0.98 | 0.29 | 29 |
| φ5 | 2000 | 2000 | 2208 | 1951 | 1951 | 1951 | 2000 | 2000 | 2009 | 91 | 5 |
| φ6 | 5.0 | 21.1 | 1.9 | 7.0 | 63.5 | 19.2 | 14.7 | 17.3 | 20.7 | 20.1 | 97 |
| Individually Fit Models | Population Models | Partially Fit Models | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Subject | SV | CO | MAP | SV | CO | MAP | SV | CO | MAP |
| 1 | 9.6 | 0.8 | 5.5 | 13.2 | 1.1 | 9.5 | 10.7 | 0.9 | 5.4 |
| 2 | 4.7 | 0.4 | 3.7 | 26.9 | 1.9 | 7.8 | 9.3 | 0.7 | 4.4 |
| 3 | 7.5 | 0.6 | 5.2 | 13.3 | 0.9 | 9.3 | 7.9 | 0.6 | 4.3 |
| 4 | 7.4 | 0.6 | 4.5 | 8.6 | 0.7 | 8.4 | 7.4 | 0.6 | 4.6 |
| 5 | 12.1 | 1.0 | 8.6 | 15.0 | 1.3 | 20.4 | 13.7 | 1.2 | 9.4 |
| 6 | 15.1 | 1.3 | 6.5 | 16.3 | 1.3 | 11.9 | 16.8 | 1.3 | 6.5 |
| 7 | 18.6 | 1.6 | 4.4 | 17.5 | 1.7 | 9.3 | 16.5 | 1.5 | 4.9 |
| Mean | 10.7 | 0.9 | 5.5 | 15.8 | 1.3 | 11.0 | 11.8 | 1.0 | 5.7 |
| SD | 4.9 | 0.4 | 1.6 | 5.7 | 0.4 | 4.4 | 3.9 | 0.4 | 1.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rinehart, J.; Coeckelenbergh, S.; Srivastava, I.; Cannesson, M.; Joosten, A. Physiological Modeling of Hemodynamic Responses to Sodium Nitroprusside. J. Pers. Med. 2023, 13, 1101. https://doi.org/10.3390/jpm13071101
Rinehart J, Coeckelenbergh S, Srivastava I, Cannesson M, Joosten A. Physiological Modeling of Hemodynamic Responses to Sodium Nitroprusside. Journal of Personalized Medicine. 2023; 13(7):1101. https://doi.org/10.3390/jpm13071101
Chicago/Turabian StyleRinehart, Joseph, Sean Coeckelenbergh, Ishita Srivastava, Maxime Cannesson, and Alexandre Joosten. 2023. "Physiological Modeling of Hemodynamic Responses to Sodium Nitroprusside" Journal of Personalized Medicine 13, no. 7: 1101. https://doi.org/10.3390/jpm13071101