
Biochemical Changes in Cardiopulmonary Bypass in Cardiac Surgery: New Insights
 ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Search Strategy
3. Pathophysiology of a Cardiopulmonary Bypass
3.1. Systemic Response to CPB
3.2. Metabolic Response
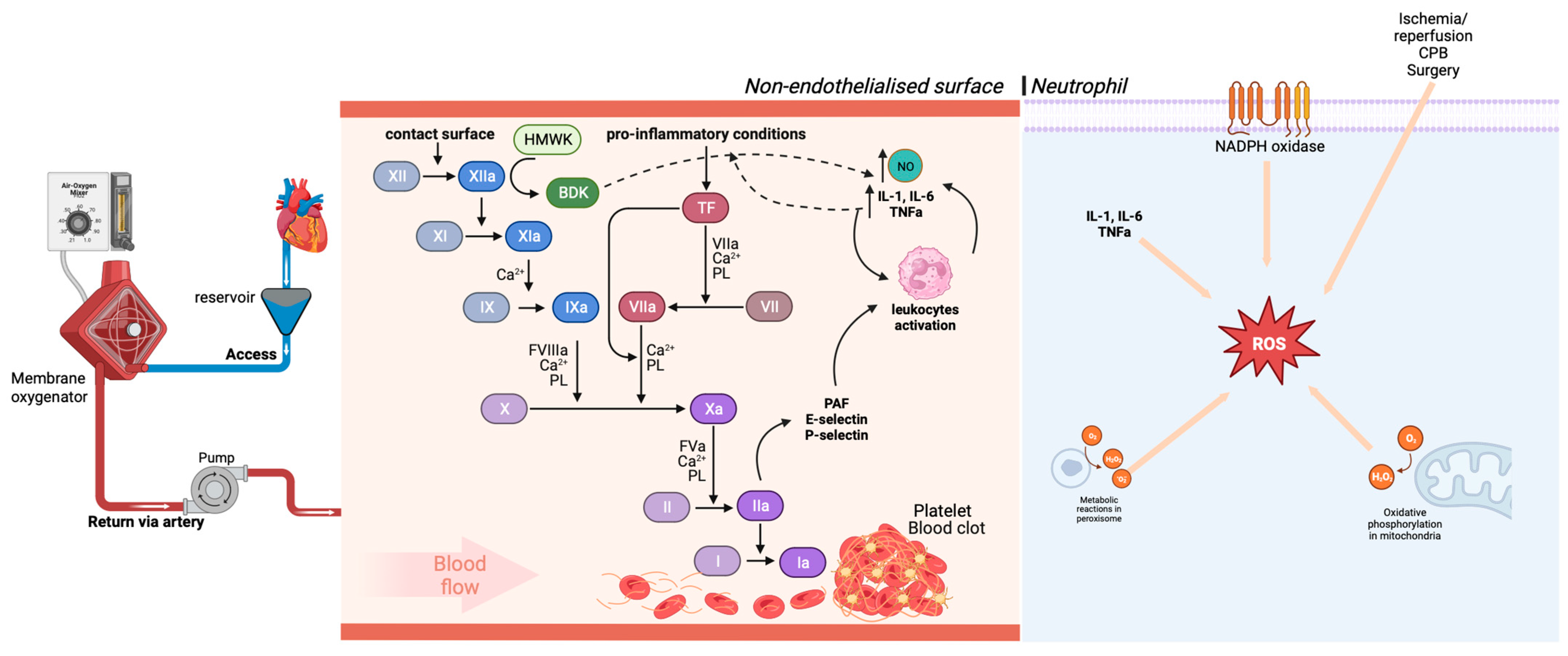
3.3. Systemic Inflammatory Reaction
3.4. Endothelial Injury
3.5. Alteration of the Coagulation Cascade
3.6. Oxidative Stress
4. Vasoplegic Syndrome Associate to CPB
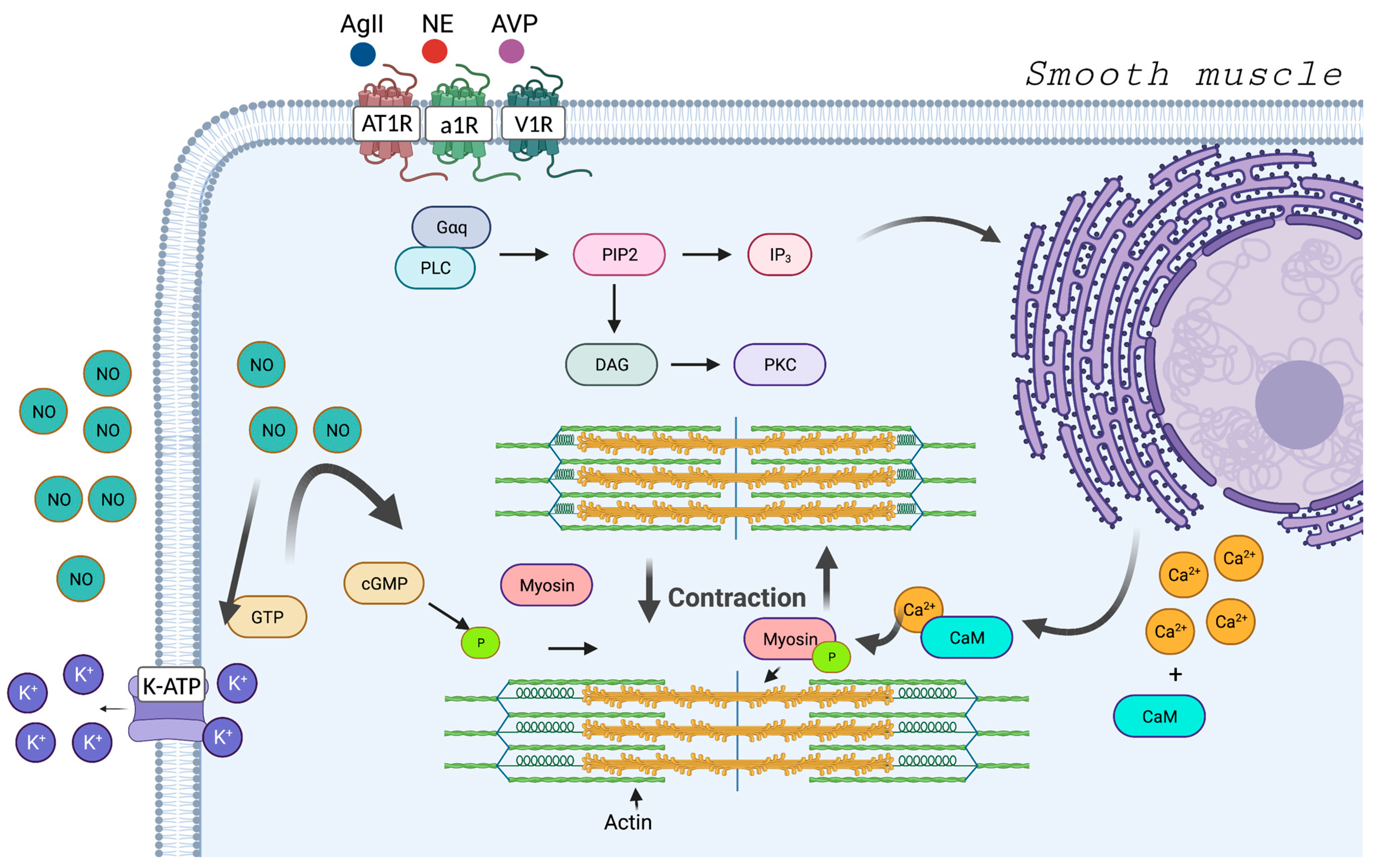
4.1. Regulatory Mechanisms: Vasoconstriction and Vasodilation
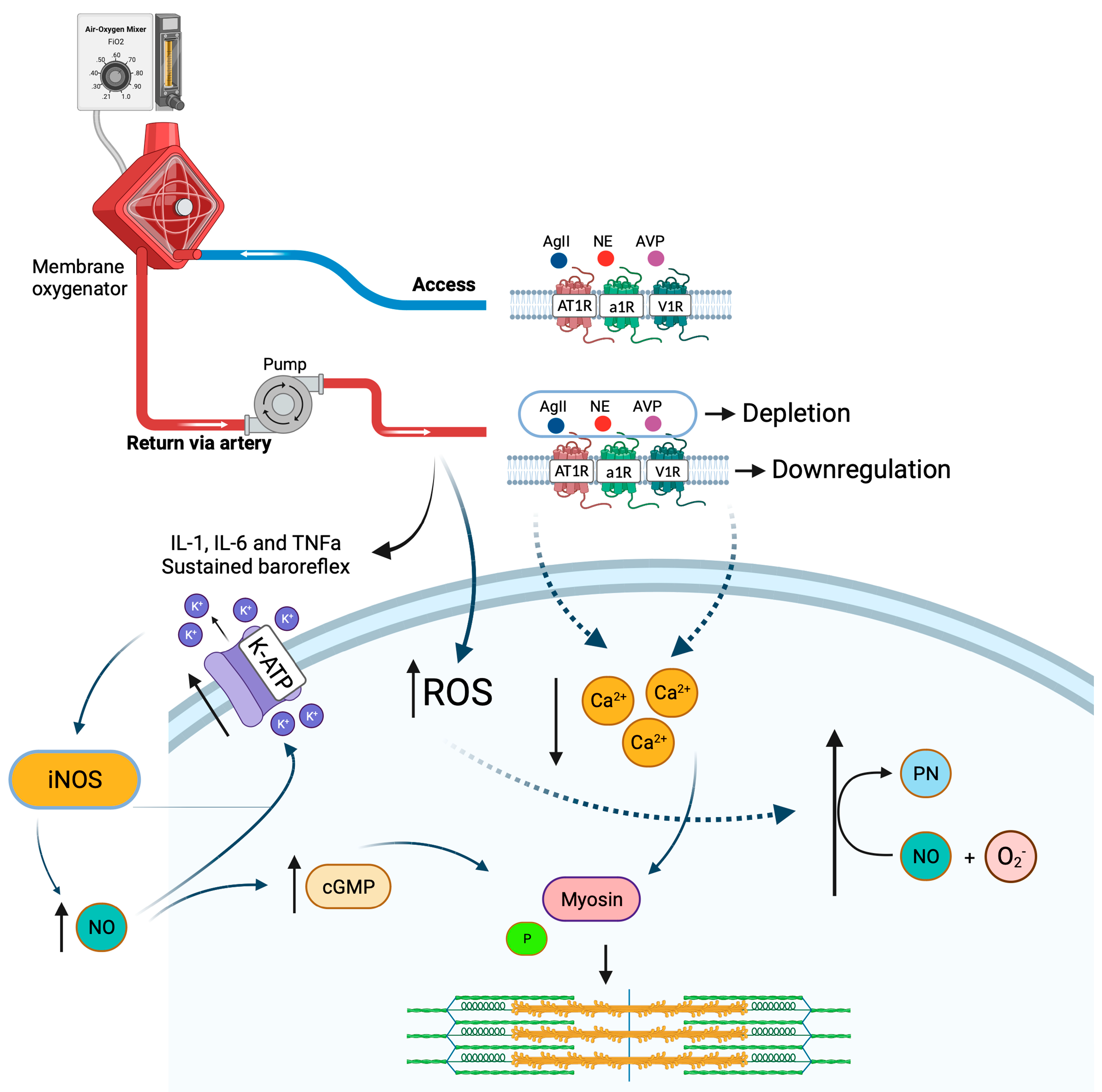
4.2. Vasoplegia
5. Future Perspective and Antioxidant Agents
5.1. Miniaturized Cardiopulmonary Bypass
5.2. Low-Level Light Therapy
5.3. Dexmedetomidine
5.4. N-Acetylcysteine
5.5. Nitric Oxide (NO)
5.6. Vitamin C
5.7. Vitamin E
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hessel, E.A. What’s New in Cardiopulmonary Bypass. J. Cardiothorac. Vasc. Anesth. 2019, 33, 2296–2326. [Google Scholar] [CrossRef] [PubMed]
- Evora, P.R.B.; Bottura, C.; Arcêncio, L.; Albuquerque, A.A.S.; Évora, P.M.; Rodrigues, A.J. Key Points for Curbing Cardiopulmonary Bypass Inflammation. Acta Cir. Bras. 2016, 31, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Borst, C.; Grundeman, P.F. Minimally Invasive Coronary Artery Bypass Grafting. Circulation 1999, 99, 1400–1403. [Google Scholar] [CrossRef]
- Kowalik, M.M.; Lango, R.; Siondalski, P.; Chmara, M.; Brzeziński, M.; Lewandowski, K.; Jagielak, D.; Klapkowski, A.; Rogowski, J. Clinical, Biochemical and Genetic Risk Factors for 30-Day and 5-Year Mortality in 518 Adult Patients Subjected to Cardiopulmonary Bypass during Cardiac Surgery—The INFLACOR Study. Acta Biochim. Pol. 2018, 65, 241–250. [Google Scholar] [CrossRef]
- Long, D.; Jenkins, E.; Griffith, K. Perfusionist Techniques of Reducing Acute Kidney Injury Following Cardiopulmonary Bypass: An Evidence-Based Review. Perfusion 2015, 30, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Goodyear-Bruch, C.; Pierce, J.D. Oxidative Stress in Critically Ill Patients. Am. J. Crit. Care 2002, 11, 543–551, quiz 552–553. [Google Scholar] [CrossRef] [PubMed]
- Karu, I.; Taal, G.; Zilmer, K.; Pruunsild, C.; Starkopf, J.; Zilmer, M. Inflammatory/Oxidative Stress during the First Week after Different Types of Cardiac Surgery. Scand. Cardiovasc. J. 2010, 44, 119–124. [Google Scholar] [CrossRef]
- Descamps-Latscha, B.; Drüeke, T.; Witko-Sarsat, V. Dialysis-Induced Oxidative Stress: Biological Aspects, Clinical Consequences, and Therapy. Semin. Dial. 2001, 14, 193–199. [Google Scholar] [CrossRef]
- Baehner, T.; Boehm, O.; Probst, C.; Poetzsch, B.; Hoeft, A.; Baumgarten, G.; Knuefermann, P. Kardiopulmonaler Bypass in Der Herzchirurgie. Anaesthesist 2012, 61, 846–856. [Google Scholar] [CrossRef]
- Murphy, G.J.; Angelini, G.D. Side Effects of Cardiopulmonary Bypass:. What Is the Reality? J. Card. Surg. 2004, 19, 481–488. [Google Scholar] [CrossRef]
- Busse, L.W.; Barker, N.; Petersen, C. Vasoplegic Syndrome Following Cardiothoracic Surgery—Review of Pathophysiology and Update of Treatment Options. Crit. Care 2020, 24, 36. [Google Scholar] [CrossRef] [PubMed]
- Zakkar, M.; Guida, G.; Suleiman, M.-S.; Angelini, G.D. Cardiopulmonary Bypass and Oxidative Stress. Oxidative Med. Cell. Longev. 2015, 2015, 189863. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, M.; Lema, G. Vasoplegic Syndrome and Its Treatment with Vasopressin during Cardiac Surgery with Cardiopulmonary Bypass. Rev. Med. Chil. 2011, 139, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.C.T.D.R. Systemic changes associated with cardiopulmonary bypass (CPB). Multidiscip. Core Sci. J. Knowl. 2018, 2, 36–54. [Google Scholar]
- Lima, G.; Cuervo, M. Mecanismo Da Circulação Extracorpórea e Eventos Neurológicos Em Cirurgia Cardíaca. Rev. Soc. Port. Anestesiol. 2019, 28, 35–42. [Google Scholar]
- Martinez, G.; Whitbread, J. Cardiopulmonary Bypass. Anaesth. Intensive Care Med. 2012, 13, 482–487. [Google Scholar] [CrossRef]
- Çelik, M.; A Max, S.; Durko, A.P.; Mahtab, E.A.F. Surgical Setup for Cardiopulmonary Bypass through Central Cannulation. Multimed. Man. Cardiothorac. Surg. 2021, 2021. [Google Scholar] [CrossRef]
- Mota, A.L.; Rodrigues, A.J.; Évora, P.R.B. Circulação Extracorpórea Em Adultos No Século XXI: Ciência, Arte Ou Empirismo? Rev. Bras. Cir. Cardiovasc. 2008, 23, 78–92. [Google Scholar] [CrossRef]
- Dekker, N.A.M.; van Leeuwen, A.L.I.; van de Ven, P.M.; de Vries, R.; Hordijk, P.L.; Boer, C.; van den Brom, C.E. Pharmacological Interventions to Reduce Edema Following Cardiopulmonary Bypass: A Systematic Review and Meta-Analysis. J. Crit. Care 2020, 56, 63–72. [Google Scholar] [CrossRef]
- Barak, M.; Katz, Y. Microbubbles. Chest 2005, 128, 2918–2932. [Google Scholar] [CrossRef]
- Biazzotto, C.B.; Brudniewski, M.; Schmidt, A.P.; Auler Júnior, J.O.C. Hipotermia No Período Peri-Operatório. Rev. Bras. Anestesiol. 2006, 56, 89–106. [Google Scholar] [CrossRef] [PubMed]
- Carneiro, T.d.C. Hipotermia Na Circulação Extracorpórea Em Cirurgia Cardíaca. Res. Soc. Dev. 2021, 10, e33510310987. [Google Scholar] [CrossRef]
- da Costa Soares, L.C.; Ribas, D.; Spring, R.; Silva, J.M.F.d.; Miyague, N.I. Perfil Clínico Da Resposta Inflamatória Sistêmica Após Cirurgia Cardíaca Pediátrica Com Circulação Extracorpórea. Arq. Bras. Cardiol. 2010, 94, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Pontes, J.C.D.V.; da Silva, G.V.R.; Benfatti, R.A.; Machado, N.P.; Pontelli, R.; Pontes, E.R.J.C. Fatores de Risco No Desenvolvimento de Insuficiência Renal Aguda Após Cirurgia de Revascularização Miocárdica Com CEC. Rev. Bras. Cir. Cardiovasc. 2007, 22, 484–490. [Google Scholar] [CrossRef]
- Santos, F.O.; Silveira, M.A.; Maia, R.B.; Monteiro, M.D.C.; Martinelli, R. Insuficiência Renal Aguda Após Cirurgia de Revascularização Miocárdica Com Circulação Extracorpórea: Incidência, Fatores de Risco e Mortalidade. Arq. Bras. Cardiol. 2004, 83, 145–149. [Google Scholar] [CrossRef]
- Andrade, A.Y.T.; de Lima Tanaka, P.S.; Poveda, V.D.B.; Turrini, R.N.T. Complicações No Pós-Operatório Imediato de Revascularização Do Miocárdio. Rev. Sobecc 2019, 24, 224–230. [Google Scholar] [CrossRef]
- Torrati, F.G.; Dantas, R.A.S. Circulação Extracorpórea e Complicações No Período Pós-Operatório Imediato de Cirurgias Cardíacas. Acta Paul. Enferm. 2012, 25, 340–345. [Google Scholar] [CrossRef]
- Padovani, C.; Cavenaghi, O.M. Recrutamento Alveolar Em Pacientes No Pós-Operatório Imediato de Cirurgia Cardíaca. Rev. Bras. Cir. Cardiovasc. 2011, 26, 116–121. [Google Scholar] [CrossRef]
- Machado, L.B.; Negri, E.M.; Bonafé, W.W.; Santos, L.M.; Malbouisson, L.M.S.; Carmona, M.J.C. Avaliação Dos Níveis de Citocinas e Da Função Pulmonar de Pacientes Submetidos à Cirurgia Cardíaca Com Circulação Extracorpórea. Rev. Bras. Anestesiol. 2011, 61, 280–285. [Google Scholar] [CrossRef]
- Godinho, A.S.; Alves, A.S.; Pereira, A.J.; Pereira, T.S. Cirurgia de Revascularização Miocárdica Com Circulação Extracorpórea versus Sem Circulação Extracorpórea: Uma Metanálise. Arq. Bras. Cardiol. 2012, 98, 87–94. [Google Scholar] [CrossRef]
- Buggeskov, K.; Maltesen, R.; Rasmussen, B.; Hanifa, M.; Lund, M.; Wimmer, R.; Ravn, H. Lung Protection Strategies during Cardiopulmonary Bypass Affect the Composition of Blood Electrolytes and Metabolites—A Randomized Controlled Trial. J. Clin. Med. 2018, 7, 462. [Google Scholar] [CrossRef] [PubMed]
- Bilal, M.; Haseeb, A.; Khan, M.H.; Khetpal, A.; Saad, M.; Arshad, M.H.; Dar, M.I.; Hasan, N.; Rafiq, R.; Sherwani, M.; et al. Assessment of Blood Glucose and Electrolytes during Cardiopulmonary Bypass in Diabetic and Non-Diabetic Patients of Pakistan. Glob. J. Health Sci. 2016, 8, 159. [Google Scholar] [CrossRef] [PubMed]
- Shahidi, M.; Bakhshandeh, H.; Rahmani, K.; Afkhamzadeh, A. Hypomagnesaemia and Other Electrolytes Imbalances in Open and Closed Pediatrics Cardiac Surgery. Pak. J. Med. Sci. 2019, 35, 353. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, I.; Roth, H.; Hanafiah, A.; Hakim, T.; Anwar, M.; Siregar, E.; Leverve, X.M. Effect of Cardiopulmonary Bypass on Lactate Metabolism. Intensive Care Med. 2003, 29, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Stephens, E.H.; Epting, C.L.; Backer, C.L.; Wald, E.L. Hyperlactatemia: An Update on Postoperative Lactate. World J. Pediatr. Congenit. Heart Surg. 2020, 11, 316–324. [Google Scholar] [CrossRef]
- Demers, P.; Elkouri, S.; Martineau, R.; Couturier, A.; Cartier, R. Outcome with High Blood Lactate Levels during Cardiopulmonary Bypass in Adult Cardiac Operation. Ann. Thorac. Surg. 2000, 70, 2082–2086. [Google Scholar] [CrossRef]
- Clingan, S.; Reagor, J.; Lombardi, J. Retrospective Analysis of Cardiac Index and Lactate Production on Cardiopulmonary Bypass for a Congenital Cardiac Patient Population. Perfusion 2019, 34, 231–235. [Google Scholar] [CrossRef]
- Adeva-Andany, M.; López-Ojén, M.; Funcasta-Calderón, R.; Ameneiros-Rodríguez, E.; Donapetry-García, C.; Vila-Altesor, M.; Rodríguez-Seijas, J. Comprehensive Review on Lactate Metabolism in Human Health. Mitochondrion 2014, 17, 76–100. [Google Scholar] [CrossRef]
- Greco, G.; Kirkwood, K.A.; Gelijns, A.C.; Moskowitz, A.J.; Lam, D.W. Diabetes Is Associated With Reduced Stress Hyperlactatemia in Cardiac Surgery. Diabetes Care 2018, 41, 469–477. [Google Scholar] [CrossRef]
- Giacinto, O.; Satriano, U.; Nenna, A.; Spadaccio, C.; Lusini, M.; Mastroianni, C.; Nappi, F.; Chello, M. Inflammatory Response and Endothelial Dysfunction Following Cardiopulmonary Bypass: Pathophysiology and Pharmacological Targets. Recent Pat. Inflamm. Allergy Drug Discov. 2019, 13, 158–173. [Google Scholar] [CrossRef]
- Becker, A.C.; Lantz, C.W.; Forbess, J.M.; Epting, C.L.; Thorp, E.B. Cardiopulmonary Bypass–Induced Inflammation and Myocardial Ischemia and Reperfusion Injury Stimulates Accumulation of Soluble MER. Pediatr. Crit. Care Med. 2021, 22, 822–831. [Google Scholar] [CrossRef]
- Millar, J.E.; Fanning, J.P.; McDonald, C.I.; McAuley, D.F.; Fraser, J.F. The Inflammatory Response to Extracorporeal Membrane Oxygenation (ECMO): A Review of the Pathophysiology. Crit. Care 2016, 20, 387. [Google Scholar] [CrossRef] [PubMed]
- Phan, S.H.; Gannon, D.E.; Ward, P.A.; Karmiol, S. Mechanism of Neutrophil-Induced Xanthine Dehydrogenase to Xanthine Oxidase Conversion in Endothelial Cells: Evidence of a Role for Elastase. Am. J. Respir. Cell Mol. Biol. 1992, 6, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Cyr, A.R.; Huckaby, L.V.; Shiva, S.S.; Zuckerbraun, B.S. Nitric Oxide and Endothelial Dysfunction. Crit. Care Clin. 2020, 36, 307–321. [Google Scholar] [CrossRef] [PubMed]
- Ayıkgöz, Y.; Salih Aydın, M.; Kankılıç, N.; Temiz, E. Nuclear Factor Erythroid 2-Related Factor 2 (Nrf2), Tumor Necrosis Factor Alpha Protein (TNF-α), Heme Oxygenase-1 (HO-1) Gene Expressions during Cardiopulmonary Bypass. Gene 2021, 790, 145690. [Google Scholar] [CrossRef] [PubMed]
- Doyle, A.J.; Hunt, B.J. Current Understanding of How Extracorporeal Membrane Oxygenators Activate Haemostasis and Other Blood Components. Front. Med. 2018, 5, 352. [Google Scholar] [CrossRef]
- Zimmerman, G.A.; McIntyre, T.M.; Prescott, S.M. Thrombin Stimulates the Adherence of Neutrophils to Human Endothelial Cells in Vitro. J. Clin. Investig 1985, 76, 2235–2246. [Google Scholar] [CrossRef] [PubMed]
- Kaplanski, G.; Fabrigoule, M.; Boulay, V.; Dinarello, C.A.; Bongrand, P.; Kaplanski, S.; Farnarier, C. Thrombin Induces Endothelial Type II Activation in Vitro: IL-1 and TNF-Alpha-Independent IL-8 Secretion and E-Selectin Expression. J. Immunol. 1997, 158, 5435–5441. [Google Scholar] [CrossRef]
- Prescott, S.M.; Zimmerman, G.A.; McIntyre, T.M. Human Endothelial Cells in Culture Produce Platelet-Activating Factor (1-Alkyl-2-Acetyl-Sn-Glycero-3-Phosphocholine) When Stimulated with Thrombin. Proc. Natl. Acad. Sci. USA 1984, 81, 3534–3538. [Google Scholar] [CrossRef]
- Esper, S.A.; Subramaniam, K.; Tanaka, K.A. Pathophysiology of Cardiopulmonary Bypass. Semin. Cardiothorac. Vasc. Anesth. 2014, 18, 161–176. [Google Scholar] [CrossRef]
- Hatami, S.; Hefler, J.; Freed, D.H. Inflammation and Oxidative Stress in the Context of Extracorporeal Cardiac and Pulmonary Support. Front. Immunol. 2022, 13, 831930. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.S.; Wan, S. Limiting Inflammatory Response to Cardiopulmonary Bypass: Pharmaceutical Strategies. Curr. Opin. Pharmacol. 2012, 12, 155–159. [Google Scholar] [CrossRef]
- Kawahito, K.; Kobayashi, E.; Ohmori, M.; Harada, K.; Kitoh, Y.; Fujimura, A.; Fuse, K. Enhanced Responsiveness of Circulatory Neutrophils After Cardiopulmonary Bypass: Increased Aggregability and Superoxide Producing Capacity. Artif. Organs 2000, 24, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Li, J.-M.; Mullen, A.M.; Yun, S.; Wientjes, F.; Brouns, G.Y.; Thrasher, A.J.; Shah, A.M. Essential Role of the NADPH Oxidase Subunit P47 Phox in Endothelial Cell Superoxide Production in Response to Phorbol Ester and Tumor Necrosis Factor-α. Circ. Res. 2002, 90, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Suleiman, M.-S.; Zacharowski, K.; Angelini, G.D. Inflammatory Response and Cardioprotection during Open-Heart Surgery: The Importance of Anaesthetics. Br. J. Pharmacol. 2008, 153, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Baskurt, O.K.; Meiselman, H.J. Blood Rheology and Hemodynamics. Semin. Thromb. Hemost. 2003, 29, 435–450. [Google Scholar] [CrossRef] [PubMed]
- Morariu, A.; Gu, Y.; Huet, R.; Siemons, W.; Rakhorst, G.; Oeveren, W. Red Blood Cell Aggregation during Cardiopulmonary Bypass: A Pathogenic Cofactor in Endothelial Cell Activation? Eur. J. Cardio-Thorac. Surg. 2004, 26, 939–946. [Google Scholar] [CrossRef]
- Byrne, J. Risk Factors and Outcomes for “vasoplegia Syndrome” Following Cardiac Transplantation. Eur. J. Cardio-Thorac. Surg. 2004, 25, 327–332. [Google Scholar] [CrossRef]
- Levin, M.A.; Lin, H.-M.; Castillo, J.G.; Adams, D.H.; Reich, D.L.; Fischer, G.W. Early On–Cardiopulmonary Bypass Hypotension and Other Factors Associated With Vasoplegic Syndrome. Circulation 2009, 120, 1664–1671. [Google Scholar] [CrossRef]
- Omar, S.; Zedan, A.; Nugent, K. Cardiac Vasoplegia Syndrome: Pathophysiology, Risk Factors and Treatment. Am. J. Med. Sci. 2015, 349, 80–88. [Google Scholar] [CrossRef]
- Shaefi, S.; Mittel, A.; Klick, J.; Evans, A.; Ivascu, N.S.; Gutsche, J.; Augoustides, J.G.T. Vasoplegia After Cardiovascular Procedures—Pathophysiology and Targeted Therapy. J. Cardiothorac. Vasc. Anesth. 2018, 32, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Landry, D.W.; Oliver, J.A. The Pathogenesis of Vasodilatory Shock. N. Engl. J. Med. 2001, 345, 588–595. [Google Scholar] [CrossRef]
- Vincent, J.-L.; De Backer, D. Circulatory Shock. N. Engl. J. Med. 2013, 369, 1726–1734. [Google Scholar] [CrossRef] [PubMed]
- Weis, F.; Kilger, E.; Beiras-Fernandez, A.; Nassau, K.; Reuter, D.; Goetz, A.; Lamm, P.; Reindl, L.; Briegel, J. Association between Vasopressor Dependence and Early Outcome in Patients after Cardiac Surgery. Anaesthesia 2006, 61, 938–942. [Google Scholar] [CrossRef]
- Leyh, R.G.; Kofidis, T.; Strüber, M.; Fischer, S.; Knobloch, K.; Wachsmann, B.; Hagl, C.; Simon, A.R.; Haverich, A. Methylene Blue: The Drug of Choice for Catecholamine-Refractory Vasoplegia after Cardiopulmonary Bypass. J. Thorac. Cardiovasc. Surg. 2003, 125, 1426–1431. [Google Scholar] [CrossRef] [PubMed]
- Levy, B.; Fritz, C.; Tahon, E.; Jacquot, A.; Auchet, T.; Kimmoun, A. Vasoplegia Treatments: The Past, the Present, and the Future. Crit. Care 2018, 22, 52. [Google Scholar] [CrossRef] [PubMed]
- Elenkov, I.J.; Wilder, R.L.; Chrousos, G.P.; Vizi, E.S. The Sympathetic Nerve--an Integrative Interface between Two Supersystems: The Brain and the Immune System. Pharmacol. Rev. 2000, 52, 595–638. [Google Scholar]
- Liu, J.; Hughes, T.E.; Sessa, W.C. The First 35 Amino Acids and Fatty Acylation Sites Determine the Molecular Targeting of Endothelial Nitric Oxide Synthase into the Golgi Region of Cells: A Green Fluorescent Protein Study. J. Cell Biol. 1997, 137, 1525–1535. [Google Scholar] [CrossRef]
- Spink, J.; Cohen, J.; Evans, T.J. The Cytokine Responsive Vascular Smooth Muscle Cell Enhancer of Inducible Nitric Oxide Synthase. J. Biol. Chem. 1995, 270, 29541–29547. [Google Scholar] [CrossRef]
- Datt, V.; Wadhhwa, R.; Sharma, V.; Virmani, S.; Minhas, H.S.; Malik, S. Vasoplegic Syndrome after Cardiovascular Surgery: A Review of Pathophysiology and Outcome-oriented Therapeutic Management. J. Card. Surg. 2021, 36, 3749–3760. [Google Scholar] [CrossRef]
- Anavi, S.; Tirosh, O. INOS as a Metabolic Enzyme under Stress Conditions. Free Radic. Biol. Med. 2020, 146, 16–35. [Google Scholar] [CrossRef] [PubMed]
- Green, S.J.; Scheller, L.F.; Marletta, M.A.; Seguin, M.C.; Klotz, F.W.; Slayter, M.; Nelson, B.J.; Nacy, C.A. Nitric Oxide: Cytokine-Regulation of Nitric Oxide in Host Resistance to Intracellular Pathogens. Immunol. Lett. 1994, 43, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Forstermann, U.; Sessa, W.C. Nitric Oxide Synthases: Regulation and Function. Eur. Heart J. 2012, 33, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Ko, E.A.; Han, J.; Jung, I.D.; Park, W.S. Physiological Roles of K+ Channels in Vascular Smooth Muscle Cells. J. Smooth Muscle Res. 2008, 44, 65–81. [Google Scholar] [CrossRef] [PubMed]
- GAO, M.; XIE, B.; GU, C.; LI, H.; ZHANG, F.; YU, Y. Targeting the Proinflammatory Cytokine Tumor Necrosis Factor-α to Alleviate Cardiopulmonary Bypass-Induced Lung Injury (Review). Mol. Med. Rep. 2015, 11, 2373–2378. [Google Scholar] [CrossRef]
- Haeffner-Cavaillon, N.; Roussellier, N.; Ponzio, O.; Carreno, M.P.; Laude, M.; Carpentier, A.; Kazatchkine, M.D. Induction of Interleukin-1 Production in Patients Undergoing Cardiopulmonary Bypass. J. Thorac. Cardiovasc. Surg. 1989, 98, 1100–1106. [Google Scholar] [CrossRef]
- Hill, G.E.; Whitten, C.W.; Landers, D.F. The Influence of Cardiopulmonary Bypass on Cytokines and Cell-Cell Communication. J. Cardiothorac. Vasc. Anesth. 1997, 11, 367–375. [Google Scholar] [CrossRef]
- Liu, X.; Yang, L.; Wang, L.; Guo, Q. RETRACTED: Oleocanthal Protects against Neuronal Inflammation and Cardiopulmonary Bypass Surgery-Induced Brain Injury in Rats by Regulating the NLRP3 Pathway. Restor. Neurol. Neurosci. 2021, 39, 39–44. [Google Scholar] [CrossRef]
- Pacher, P.; Beckman, J.S.; Liaudet, L. Nitric Oxide and Peroxynitrite in Health and Disease. Physiol. Rev. 2007, 87, 315–424. [Google Scholar] [CrossRef]
- Kerbaul, F.; Guidon, C.; Lejeune, P.J.; Mollo, M.; Mesana, T.; Gouin, F. Hyperprocalcitonemia Is Related to Noninfectious Postoperative Severe Systemic Inflammatory Response Syndrome Associated with Cardiovascular Dysfunction after Coronary Artery Bypass Graft Surgery. J. Cardiothorac. Vasc. Anesth. 2002, 16, 47–53. [Google Scholar] [CrossRef]
- Ma, H.; Dong, Y.; Sun, K.; Wang, S.; Zhang, Z. Protective Effect of MiR-146 on Renal Injury Following Cardiopulmonary Bypass in Rats through Mediating NF-ΚB Signaling Pathway. Bioengineered 2022, 13, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Ammar, M.A.; Ammar, A.A.; Wieruszewski, P.M.; Bissell, B.D.; Long, M.T.; Albert, L.; Khanna, A.K.; Sacha, G.L. Timing of Vasoactive Agents and Corticosteroid Initiation in Septic Shock. Ann. Intensive Care 2022, 12, 47. [Google Scholar] [CrossRef] [PubMed]
- Papazisi, O.; Palmen, M.; Danser, A.H.J. The Use of Angiotensin II for the Treatment of Post-Cardiopulmonary Bypass Vasoplegia. Cardiovasc. Drugs Ther. 2022, 36, 739–748. [Google Scholar] [CrossRef] [PubMed]
- Jochberger, S.; Velik-Salchner, C.; Mayr, V.D.; Luckner, G.; Wenzel, V.; Falkensammer, G.; Ulmer, H.; Morgenthaler, N.; Hasibeder, W.; Dünser, M.W. The Vasopressin and Copeptin Response in Patients with Vasodilatory Shock after Cardiac Surgery: A Prospective, Controlled Study. Intensive Care Med. 2009, 35, 489–497. [Google Scholar] [CrossRef]
- Colson, P.H.; Bernard, C.; Struck, J.; Morgenthaler, N.G.; Albat, B.; Guillon, G. Post Cardiac Surgery Vasoplegia Is Associated with High Preoperative Copeptin Plasma Concentration. Crit. Care 2011, 15, R255. [Google Scholar] [CrossRef]
- Landry, D.W.; Levin, H.R.; Gallant, E.M.; Ashton, R.C.; Seo, S.; D’Alessandro, D.; Oz, M.C.; Oliver, J.A. Vasopressin Deficiency Contributes to the Vasodilation of Septic Shock. Circulation 1997, 95, 1122–1125. [Google Scholar] [CrossRef]
- Davies, N.W. Modulation of ATP-Sensitive K+ Channels in Skeletal Muscle by Intracellular Protons. Nature 1990, 343, 375–377. [Google Scholar] [CrossRef]
- Ohkawa, F.; Ikeda, U.; Kanbe, T.; Kawasaki, K.; Shimada, K. Effects of Inflammatory Cytokines on Vascular Tone. Cardiovasc. Res. 1995, 30, 711–715. [Google Scholar] [CrossRef]
- Kilger, E.; Weis, F.; Briegel, J.; Frey, L.; Goetz, A.E.; Reuter, D.; Nagy, A.; Schuetz, A.; Lamm, P.; Knoll, A.; et al. Stress Doses of Hydrocortisone Reduce Severe Systemic Inflammatory Response Syndrome and Improve Early Outcome in a Risk Group of Patients after Cardiac Surgery. Crit. Care Med. 2003, 31, 1068–1074. [Google Scholar] [CrossRef]
- Träger, K.; Fritzler, D.; Fischer, G.; Schröder, J.; Skrabal, C.; Liebold, A.; Reinelt, H. Treatment of Post-Cardiopulmonary Bypass SIRS by Hemoadsorption: A Case Series. Int. J. Artif. Organs 2016, 39, 141–146. [Google Scholar] [CrossRef]
- Manzanares, W.; Dhaliwal, R.; Jiang, X.; Murch, L.; Heyland, D.K. Antioxidant Micronutrients in the Critically Ill: A Systematic Review and Meta-Analysis. Crit. Care 2012, 16, R66. [Google Scholar] [CrossRef] [PubMed]
- Visser, J.; Labadarios, D.; Blaauw, R. Micronutrient Supplementation for Critically Ill Adults: A Systematic Review and Meta-Analysis. Nutrition 2011, 27, 745–758. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Bansal, M.; Nath, S.S.; Kumar, V.; Malviya, D.; Srivastava, D. N-Acetylcysteine Supplementation for the Prevention of Postoperative Liver Dysfunction after On-Pump Cardiac Surgery. Turk. J. Anaesthesiol. Reanim. 2021, 49, 460–469. [Google Scholar] [CrossRef] [PubMed]
- McDonald, C.I.; Fraser, J.F.; Coombes, J.S.; Fung, Y.L. Oxidative Stress during Extracorporeal Circulation. Eur. J. Cardio-Thorac. Surg. 2014, 46, 937–943. [Google Scholar] [CrossRef]
- Türker, F.S.; Doğan, A.; Ozan, G.; Kıbar, K.; Erışır, M. Change in Free Radical and Antioxidant Enzyme Levels in the Patients Undergoing Open Heart Surgery with Cardiopulmonary Bypass. Oxidative Med. Cell. Longev. 2016, 2016, 1783728. [Google Scholar] [CrossRef]
- Alsatli, R. Mini Cardiopulmonary Bypass: Anesthetic Considerations. Anesth. Essays Res. 2012, 6, 10. [Google Scholar] [CrossRef]
- Mueller, X. A New Concept of Integrated Cardiopulmonary Bypass Circuit. Eur. J. Cardio-Thorac. Surg. 2002, 21, 840–846. [Google Scholar] [CrossRef]
- Anastasiadis, K.; Murkin, J.; Antonitsis, P.; Bauer, A.; Ranucci, M.; Gygax, E.; Schaarschmidt, J.; Fromes, Y.; Philipp, A.; Eberle, B.; et al. Use of Minimal Invasive Extracorporeal Circulation in Cardiac Surgery: Principles, Definitions and Potential Benefits. A Position Paper from the Minimal Invasive Extra-Corporeal Technologies International Society (MiECTiS). Interact. Cardiovasc. Thorac. Surg. 2016, 22, 647–662. [Google Scholar] [CrossRef]
- Cheng, T.; Barve, R.; Cheng, Y.W.M.; Ravendren, A.; Ahmed, A.; Toh, S.; Goulden, C.J.; Harky, A. Conventional versus Miniaturized Cardiopulmonary Bypass: A Systematic Review and Meta-Analysis. JTCVS Open 2021, 8, 418–441. [Google Scholar] [CrossRef]
- Walski, T.; Drohomirecka, A.; Bujok, J.; Czerski, A.; Wąż, G.; Trochanowska-Pauk, N.; Gorczykowski, M.; Cichoń, R.; Komorowska, M. Low-Level Light Therapy Protects Red Blood Cells Against Oxidative Stress and Hemolysis During Extracorporeal Circulation. Front. Physiol. 2018, 9, 647. [Google Scholar] [CrossRef]
- Drohomirecka, A.; Iwaszko, A.; Walski, T.; Pliszczak-Król, A.; Wąż, G.; Graczyk, S.; Gałecka, K.; Czerski, A.; Bujok, J.; Komorowska, M. Low-Level Light Therapy Reduces Platelet Destruction during Extracorporeal Circulation. Sci. Rep. 2018, 8, 16963. [Google Scholar] [CrossRef] [PubMed]
- Chludzińska, L.; Ananicz, E.; Jarosawska, A.; Komorowska, M. Near-Infrared Radiation Protects the Red Cell Membrane against Oxidation. Blood Cells Mol. Dis. 2005, 35, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Walski, T.; Dyrda, A.; Dzik, M.; Chludzińska, L.; Tomków, T.; Mehl, J.; Detyna, J.; Gałecka, K.; Witkiewicz, W.; Komorowska, M. Near Infrared Light Induces Post-Translational Modifications of Human Red Blood Cell Proteins. Photochem. Photobiol. Sci. 2015, 14, 2035–2045. [Google Scholar] [CrossRef] [PubMed]
- Hall, R. Identification of Inflammatory Mediators and Their Modulation by Strategies for the Management of the Systemic Inflammatory Response During Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2013, 27, 983–1033. [Google Scholar] [CrossRef]
- Li, P.; Han, J.; Zhang, D.; Cao, S.; Su, C. Effects of Dexmedetomidine on Oxidative Stress and Inflammatory Response in Lungs during Mechanical Ventilation in COPD Rats. Exp. Ther. Med. 2019, 19, 1219–1224. [Google Scholar] [CrossRef]
- CAN, M.; GUL, S.; BEKTAS, S.; HANCI, V.; ACIKGOZ, S. Effects of Dexmedetomidine or Methylprednisolone on Inflammatory Responses in Spinal Cord Injury. Acta Anaesthesiol. Scand. 2009, 53, 1068–1072. [Google Scholar] [CrossRef]
- Bulow, N.M.H.; Colpo, E.; Pereira, R.P.; Correa, E.F.M.; Waczuk, E.P.; Duarte, M.F.; Rocha, J.B.T. Dexmedetomidine Decreases the Inflammatory Response to Myocardial Surgery under Mini-Cardiopulmonary Bypass. Braz. J. Med. Biol. Res. 2016, 49, e4646. [Google Scholar] [CrossRef]
- Ueki, M.; Kawasaki, T.; Habe, K.; Hamada, K.; Kawasaki, C.; Sata, T. The Effects of Dexmedetomidine on Inflammatory Mediators after Cardiopulmonary Bypass. Anaesthesia 2014, 69, 693–700. [Google Scholar] [CrossRef]
- Kim, S.; Park, S.J.; Nam, S.B.; Song, S.-W.; Han, Y.; Ko, S.; Song, Y. Pulmonary Effects of Dexmedetomidine Infusion in Thoracic Aortic Surgery under Hypothermic Circulatory Arrest: A Randomized Placebo-Controlled Trial. Sci. Rep. 2021, 11, 10975. [Google Scholar] [CrossRef]
- Zhai, M.; Kang, F.; Han, M.; Huang, X.; Li, J. The Effect of Dexmedetomidine on Renal Function in Patients Undergoing Cardiac Valve Replacement under Cardiopulmonary Bypass: A Double-Blind Randomized Controlled Trial. J. Clin. Anesth. 2017, 40, 33–38. [Google Scholar] [CrossRef]
- Turan, A.; Duncan, A.; Leung, S.; Karimi, N.; Fang, J.; Mao, G.; Hargrave, J.; Gillinov, M.; Trombetta, C.; Ayad, S.; et al. Dexmedetomidine for Reduction of Atrial Fibrillation and Delirium after Cardiac Surgery (DECADE): A Randomised Placebo-Controlled Trial. Lancet 2020, 396, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Peng, K.; Shen, Y.; Ying, Y.; Kiaii, B.; Rodriguez, V.; Boyd, D.; Applegate, R.L.; Lubarsky, D.A.; Zhang, Z.; Xia, Z.; et al. Perioperative Dexmedetomidine and 5-Year Survival in Patients Undergoing Cardiac Surgery. Br. J. Anaesth. 2021, 127, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Moura, E.; Afonso, J.; Hein, L.; Vieira-Coelho, M.A. α 2 -Adrenoceptor Subtypes Involved in the Regulation of Catecholamine Release from the Adrenal Medulla of Mice. Br. J. Pharmacol. 2006, 149, 1049–1058. [Google Scholar] [CrossRef]
- Xiang, H.; Hu, B.; Li, Z.; Li, J. Dexmedetomidine Controls Systemic Cytokine Levels through the Cholinergic Anti-Inflammatory Pathway. Inflammation 2014, 37, 1763–1770. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.; Shi, T.; Zhuang, R.; Fang, H.; Jiang, X.; Shao, Y.; Zhou, H. Protective Effect of N-Acetylcysteine Activated Carbon Release Microcapsule on Myocardial Ischemia-Reperfusion Injury in Rats. Exp. Ther. Med. 2018, 15, 1809–1818. [Google Scholar] [CrossRef] [PubMed]
- Blasi, F.; Page, C.; Rossolini, G.M.; Pallecchi, L.; Matera, M.G.; Rogliani, P.; Cazzola, M. The Effect of N -Acetylcysteine on Biofilms: Implications for the Treatment of Respiratory Tract Infections. Respir. Med. 2016, 117, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Paintlia, M.K.; Paintlia, A.S.; Contreras, M.A.; Singh, I.; Singh, A.K. Lipopolysaccharide-Induced Peroxisomal Dysfunction Exacerbates Cerebral White Matter Injury: Attenuation by N-Acetyl Cysteine. Exp. Neurol. 2008, 210, 560–576. [Google Scholar] [CrossRef]
- Samuni, Y.; Goldstein, S.; Dean, O.M.; Berk, M. The Chemistry and Biological Activities of N-Acetylcysteine. Biochim. Et Biophys. Acta (BBA)-Gen. Subj. 2013, 1830, 4117–4129. [Google Scholar] [CrossRef]
- Yi, X.; Cui, X.; Wu, P.; Wang, S.; Wang, G.; Yang, X.; Yang, F.; Zheng, S.; Li, Z. Effects of N-Acetylcysteine on Apoptosis Induced by Myocardial Ischemia Reperfusion Injury in Rats’ Heart Transplantation. Chin. J. Reparative Reconstr. Surg. 2013, 27, 1234–1239. [Google Scholar] [PubMed]
- WU, X.-Y.; LUO, A.-Y.; ZHOU, Y.-R.; REN, J.-H. N-Acetylcysteine Reduces Oxidative Stress, Nuclear Factor-ΚB Activity and Cardiomyocyte Apoptosis in Heart Failure. Mol. Med. Rep. 2014, 10, 615–624. [Google Scholar] [CrossRef]
- Orhan, G.; Yapici, N.; Yuksel, M.; Sargin, M.; Şenay, Ş.; Yalçin, A.S.; Aykaç, Z.; Aka, S.A. Effects of N-Acetylcysteine on Myocardial Ischemia–Reperfusion Injury in Bypass Surgery. Heart Vessels 2006, 21, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Giam, B.; Chu, P.-Y.; Kuruppu, S.; Smith, A.I.; Horlock, D.; Kiriazis, H.; Du, X.-J.; Kaye, D.M.; Rajapakse, N.W. N- Acetylcysteine Attenuates the Development of Cardiac Fibrosis and Remodeling in a Mouse Model of Heart Failure. Physiol. Rep. 2016, 4, e12757. [Google Scholar] [CrossRef] [PubMed]
- Onk, D.; Özçelik, F.; Onk, O.A.; Günay, M.; Akarsu Ayazoğlu, T.; Ünver, E. Assessment of Renal and Hepatic Tissue-Protective Effects of N-Acetylcysteine via Ammonia Metabolism: A Prospective Randomized Study. Med. Sci. Monit. 2018, 24, 1540–1546. [Google Scholar] [CrossRef]
- Permeisari, D. Future Insights of Pharmacological Prevention for AKI Post Cardiopulmonary Bypass Surgery (Based on PK/PD Approach). Front. Pharmacol. 2022, 13, 975641. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.I.; Brewster, D.J.; Horrigan, D.; Sarode, V. Pharmacological and Non-surgical Renal Protective Strategies for Cardiac Surgery Patients Undergoing Cardiopulmonary Bypass: A Systematic Review. ANZ J. Surg. 2019, 89, 296–302. [Google Scholar] [CrossRef]
- Savluk, O.F.; Guzelmeric, F.; Yavuz, Y.; Cevirme, D.; Gurcu, E.; Ogus, H.; Orki, T.; Kocak, T. N-Acetylcysteine versus Dopamine to Prevent Acute Kidney Injury after Cardiac Surgery in Patients with Preexisting Moderate Renal Insufficiency. Braz. J. Cardiovasc. Surg. 2017, 32, 8–14. [Google Scholar] [CrossRef]
- Redaelli, S.; Magliocca, A.; Malhotra, R.; Ristagno, G.; Citerio, G.; Bellani, G.; Berra, L.; Rezoagli, E. Nitric Oxide: Clinical Applications in Critically Ill Patients. Nitric Oxide 2022, 121, 20–33. [Google Scholar] [CrossRef]
- Kamenshchikov, N.O.; Duong, N.; Berra, L. Nitric Oxide in Cardiac Surgery: A Review Article. Biomedicines 2023, 11, 1085. [Google Scholar] [CrossRef]
- Bolli, R. The Late Phase of Preconditioning. Circ. Res. 2000, 87, 972–983. [Google Scholar] [CrossRef]
- Kamenshchikov, N.O.; Anfinogenova, Y.J.; Kozlov, B.N.; Svirko, Y.S.; Pekarskiy, S.E.; Evtushenko, V.V.; Lugovsky, V.A.; Shipulin, V.M.; Lomivorotov, V.V.; Podoksenov, Y.K. Nitric Oxide Delivery during Cardiopulmonary Bypass Reduces Acute Kidney Injury: A Randomized Trial. J. Thorac. Cardiovasc. Surg. 2022, 163, 1393–1403.e9. [Google Scholar] [CrossRef]
- Loughlin, J.M.; Browne, L.; Hinchion, J. The Impact of Exogenous Nitric Oxide during Cardiopulmonary Bypass for Cardiac Surgery. Perfusion 2022, 37, 656–667. [Google Scholar] [CrossRef] [PubMed]
- Hornik, C.P. Invited Commentary: Efficacy of Nitric Oxide Administration During Neonatal Cardiopulmonary Bypass. World J. Pediatr. Congenit. Heart Surg. 2020, 11, 424–425. [Google Scholar] [CrossRef] [PubMed]
- Checchia, P.A.; Bronicki, R.A.; Muenzer, J.T.; Dixon, D.; Raithel, S.; Gandhi, S.K.; Huddleston, C.B. Nitric Oxide Delivery during Cardiopulmonary Bypass Reduces Postoperative Morbidity in Children—A Randomized Trial. J. Thorac. Cardiovasc. Surg. 2013, 146, 530–536. [Google Scholar] [CrossRef] [PubMed]
- James, C.; Millar, J.; Horton, S.; Brizard, C.; Molesworth, C.; Butt, W. Nitric Oxide Administration during Paediatric Cardiopulmonary Bypass: A Randomised Controlled Trial. Intensive Care Med. 2016, 42, 1744–1752. [Google Scholar] [CrossRef] [PubMed]
- Kamenshchikov, N.O.; Mandel, I.A.; Podoksenov, Y.K.; Svirko, Y.S.; Lomivorotov, V.V.; Mikheev, S.L.; Kozlov, B.N.; Shipulin, V.M.; Nenakhova, A.A.; Anfinogenova, Y.J. Nitric Oxide Provides Myocardial Protection When Added to the Cardiopulmonary Bypass Circuit during Cardiac Surgery: Randomized Trial. J. Thorac. Cardiovasc. Surg. 2019, 157, 2328–2336.e1. [Google Scholar] [CrossRef]
- Carr, A.; Maggini, S. Vitamin C and Immune Function. Nutrients 2017, 9, 1211. [Google Scholar] [CrossRef]
- Doseděl, M.; Jirkovský, E.; Macáková, K.; Krčmová, L.; Javorská, L.; Pourová, J.; Mercolini, L.; Remião, F.; Nováková, L.; Mladěnka, P. Vitamin C—Sources, Physiological Role, Kinetics, Deficiency, Use, Toxicity, and Determination. Nutrients 2021, 13, 615. [Google Scholar] [CrossRef]
- Tai, Y.-H.; Wu, H.-L.; Chu, Y.-H.; Huang, C.-H.; Ho, S.-T.; Lin, T.-C.; Lu, C.-C. Vitamin C Supplementation Attenuates Oxidative Stress and Improves Erythrocyte Deformability in Cardiac Surgery with Cardiopulmonary Bypass. Chin. J. Physiol. 2022, 65, 241. [Google Scholar] [CrossRef]
- Wieruszewski, P.M.; Nei, S.D.; Maltais, S.; Schaff, H.V.; Wittwer, E.D. Vitamin C for Vasoplegia After Cardiopulmonary Bypass: A Case Series. A A Pract. 2018, 11, 96–99. [Google Scholar] [CrossRef]
- Ghorbaninezhad, K.; Bakhsha, F.; Yousefi, Z.; Halakou, S.; Mehrbakhsh, Z. Comparison Effect of Tranexamic Acid (TA) and Tranexamic Acid Combined with Vitamin C (TXC) on Drainage Volume and Atrial Fibrillation Arrhythmia in Patients Undergoing Cardiac Bypass Surgery: Randomized Clinical Trial. Anesthesiol. Pain Med. 2019, 9, e96096. [Google Scholar] [CrossRef]
- Yanase, F.; Bitker, L.; Hessels, L.; Osawa, E.; Naorungroj, T.; Cutuli, S.L.; Young, P.J.; Ritzema, J.; Hill, G.; Latimer-Bell, C.; et al. A Pilot, Double-Blind, Randomized, Controlled Trial of High-Dose Intravenous Vitamin C for Vasoplegia After Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2020, 34, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Das, D.; Sen, C.; Goswami, A. Effect of Vitamin C on Adrenal Suppression by Etomidate Induction in Patients Undergoing Cardiac Surgery: A Randomized Controlled Trial. Ann. Card. Anaesth. 2016, 19, 410. [Google Scholar] [CrossRef]
- Miyazawa, T.; Burdeos, G.C.; Itaya, M.; Nakagawa, K.; Miyazawa, T. Vitamin E: Regulatory Redox Interactions. IUBMB Life 2019, 71, 430–441. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.; Borgs, C.; Fitzner, C.; Stoppe, C. Perioperative Vitamin C and E Levels in Cardiac Surgery Patients and Their Clinical Significance. Nutrients 2019, 11, 2157. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.-X.; Fu, L.; Li, Y.; Lin, Z.-B.; Liu, X.; Wang, J.-F.; Chen, Y.-X.; Wang, Z.-P.; Zhang, X.; Ou, Z.-J.; et al. The Cardioprotective Effect of Vitamin E (Alpha-Tocopherol) Is Strongly Related to Age and Gender in Mice. PLoS ONE 2015, 10, e0137405. [Google Scholar] [CrossRef]
- Zakkar, M.; Ascione, R.; James, A.F.; Angelini, G.D.; Suleiman, M.S. Inflammation, Oxidative Stress and Postoperative Atrial Fibrillation in Cardiac Surgery. Pharmacol. Ther. 2015, 154, 13–20. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreira, L.O.; Vasconcelos, V.W.; Lima, J.d.S.; Vieira Neto, J.R.; da Costa, G.E.; Esteves, J.d.C.; de Sousa, S.C.; Moura, J.A.; Santos, F.R.S.; Leitão Filho, J.M.; et al. Biochemical Changes in Cardiopulmonary Bypass in Cardiac Surgery: New Insights. J. Pers. Med. 2023, 13, 1506. https://doi.org/10.3390/jpm13101506
Ferreira LO, Vasconcelos VW, Lima JdS, Vieira Neto JR, da Costa GE, Esteves JdC, de Sousa SC, Moura JA, Santos FRS, Leitão Filho JM, et al. Biochemical Changes in Cardiopulmonary Bypass in Cardiac Surgery: New Insights. Journal of Personalized Medicine. 2023; 13(10):1506. https://doi.org/10.3390/jpm13101506
Chicago/Turabian StyleFerreira, Luan Oliveira, Victoria Winkler Vasconcelos, Janielle de Sousa Lima, Jaime Rodrigues Vieira Neto, Giovana Escribano da Costa, Jordana de Castro Esteves, Sallatiel Cabral de Sousa, Jonathan Almeida Moura, Felipe Ruda Silva Santos, João Monteiro Leitão Filho, and et al. 2023. "Biochemical Changes in Cardiopulmonary Bypass in Cardiac Surgery: New Insights" Journal of Personalized Medicine 13, no. 10: 1506. https://doi.org/10.3390/jpm13101506