
Multi-Modal Stacking Ensemble for the Diagnosis of Cardiovascular Diseases

Abstract
:1. Introduction
2. Materials and Methods
2.1. Dataset and Preprocessing
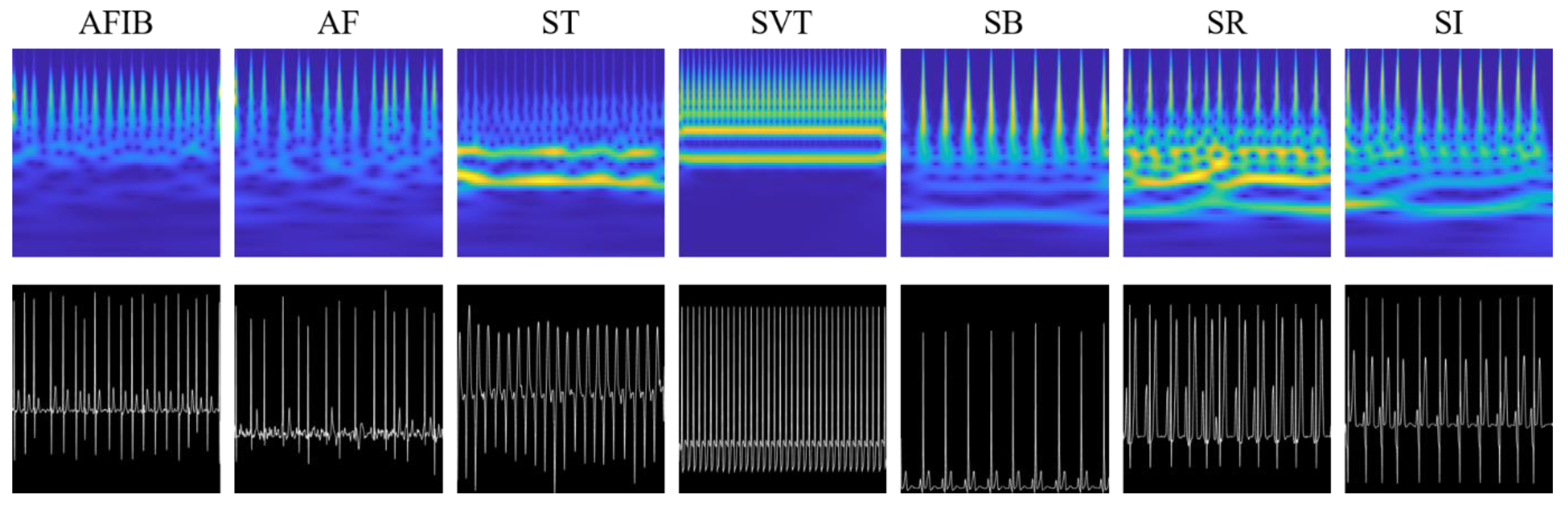
2.2. Data Transformation
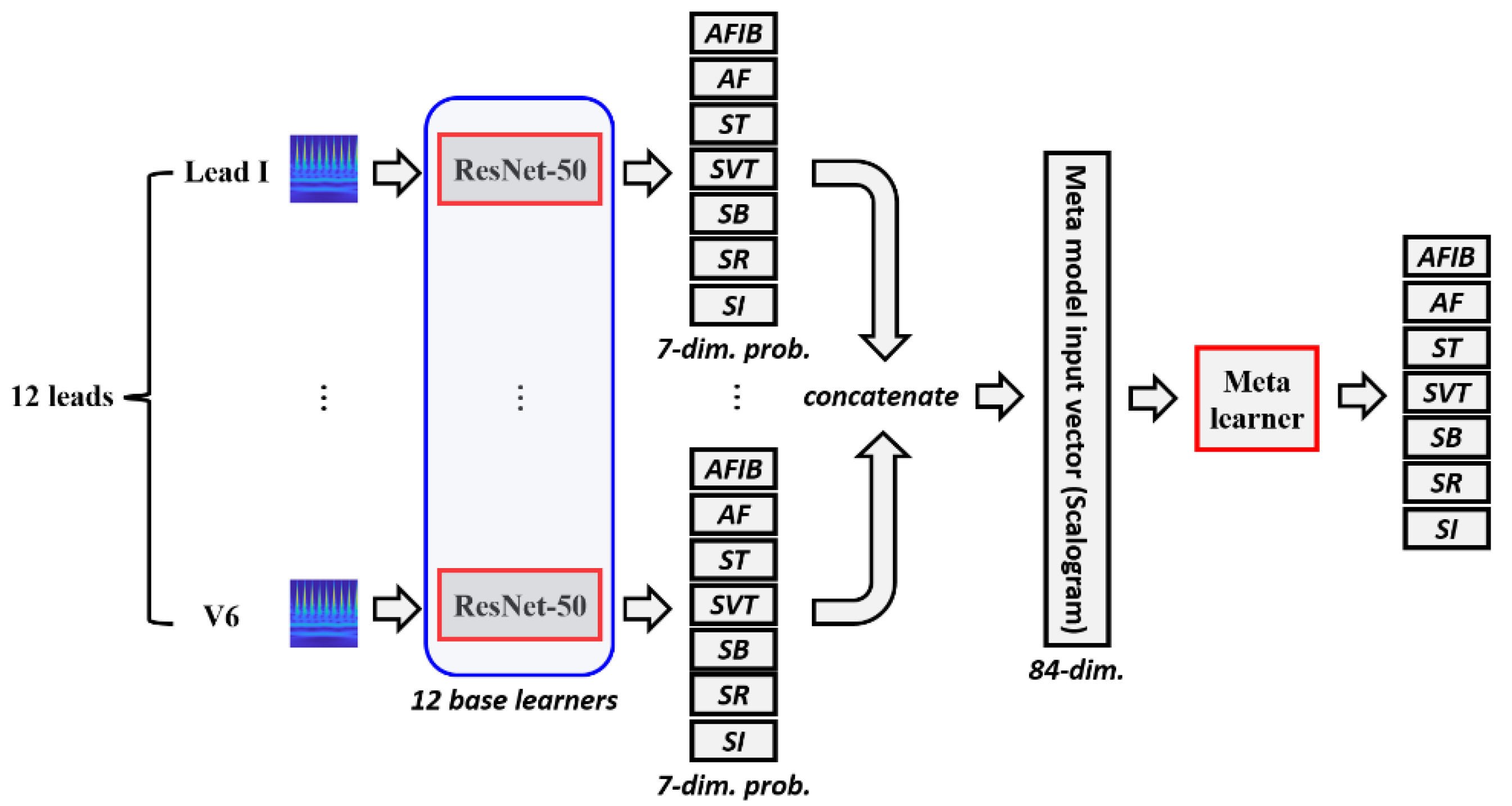
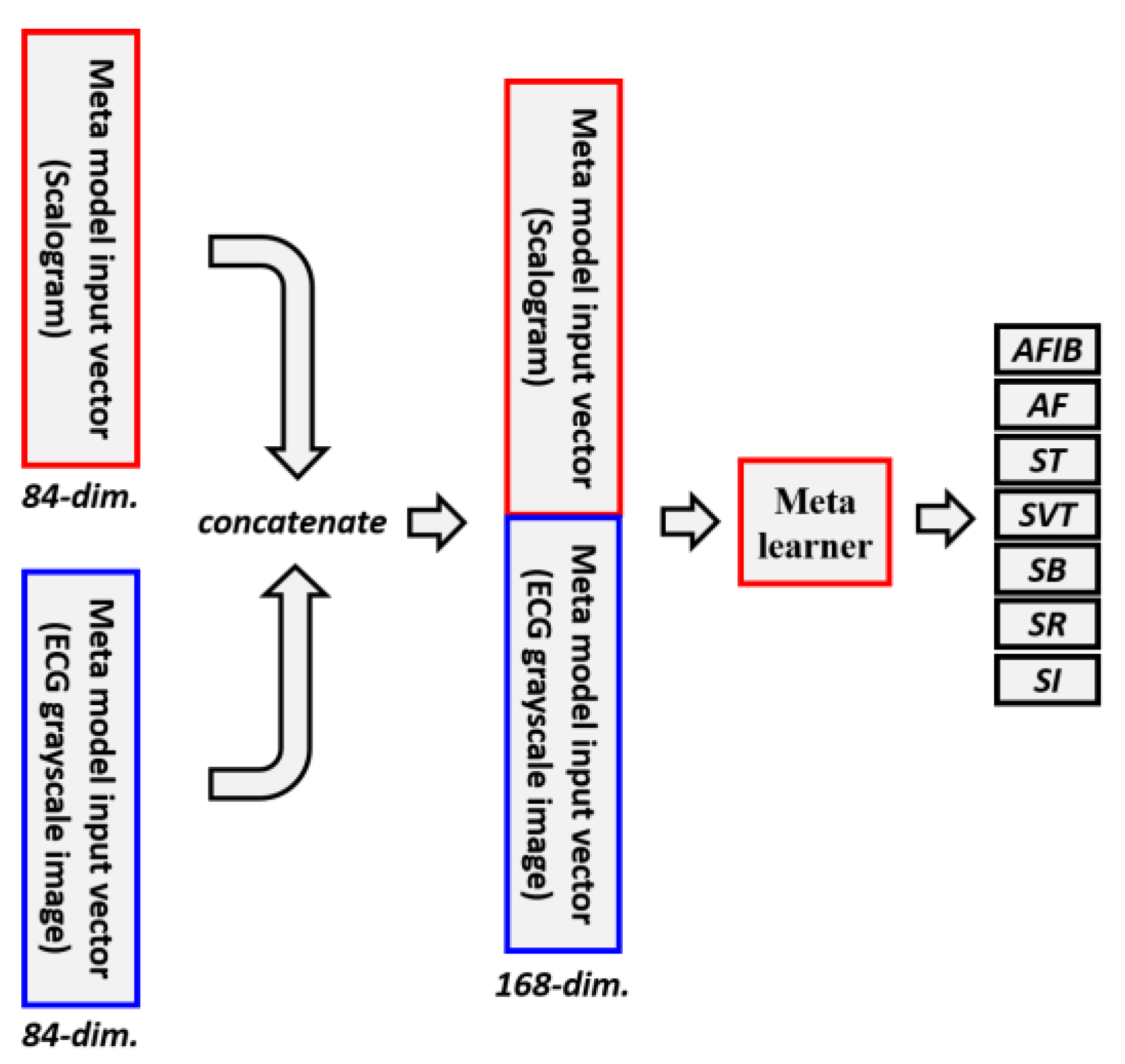
2.3. Ensemble Methods
2.4. LSTM
2.5. ResNet-50 Model and Machine Learning Algorithms
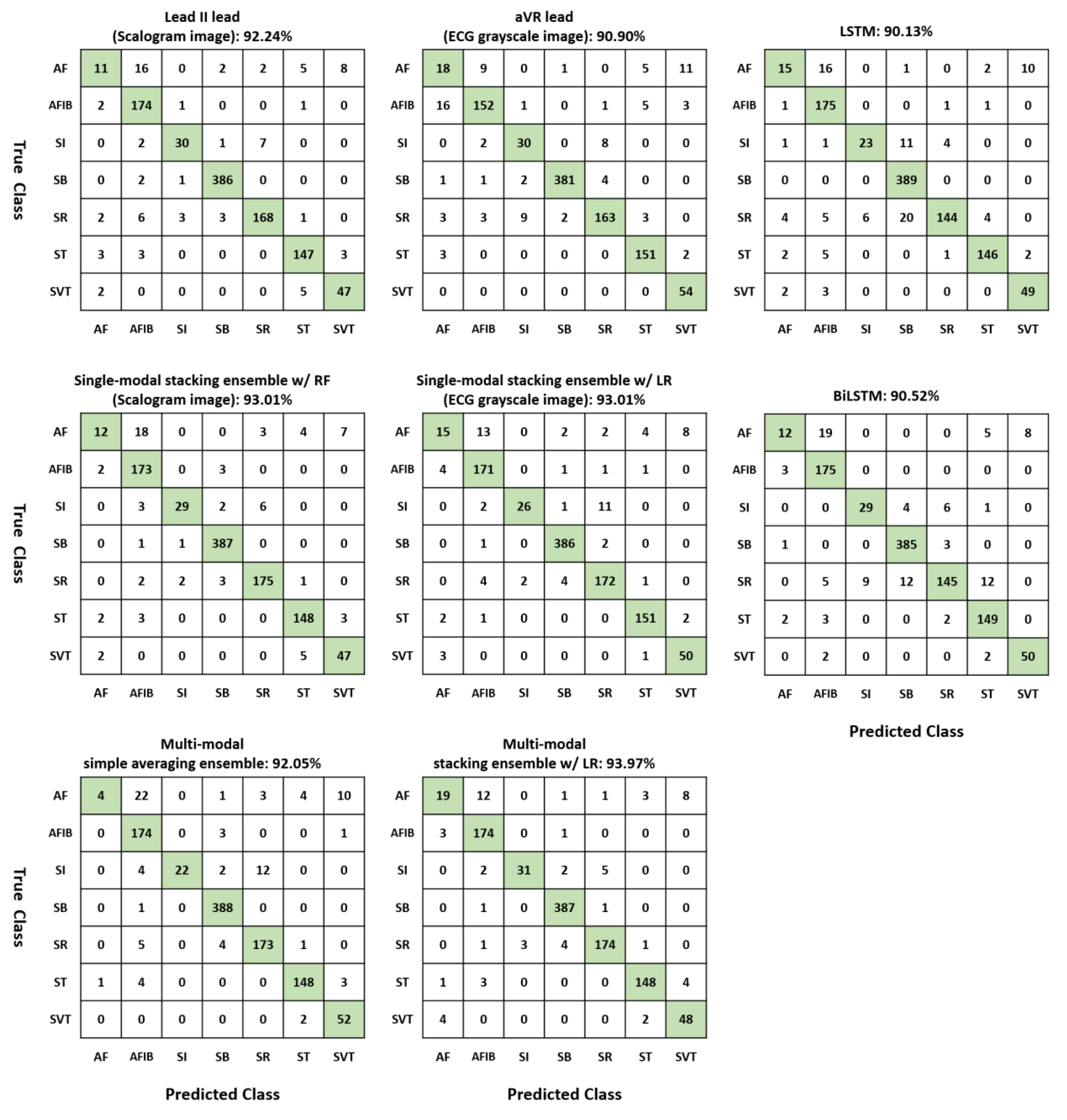
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flores, N.; Reyna, M.A.; Avitia, R.L.; Cardenas-Haro, J.A.; Garcia-Gonzalez, C. Non-Invasive Systems and Methods Patents Review Based on Electrocardiogram for Diagnosis of Cardiovascular Diseases. Algorithms 2022, 15, 82. [Google Scholar] [CrossRef]
- Husain, K.; Mohd Zahid, M.S.; Ul Hassan, S.; Hasbullah, S.; Mandala, S. Advances of ECG Sensors from Hardware, Software and Format Interoperability Perspectives. Electronics 2021, 10, 105. [Google Scholar] [CrossRef]
- Lee, H.; Yoon, T.; Yeo, C.; Oh, H.; Ji, Y.; Sim, S.; Kang, D. Cardiac Arrhythmia Classification Based on One-Dimensional Morphological Features. Appl. Sci. 2021, 11, 9460. [Google Scholar] [CrossRef]
- Ribeiro, A.H.; Ribeiro, M.H.; Paixão, G.M.M.; Oliveira, D.M.; Gomes, P.R.; Canazart, J.A.; Ferreira, M.P.S.; Andersson, C.R.; Macfarlane, P.W.; Meira Jr, W.; et al. Automatic diagnosis of the 12-lead ECG using a deep neural network. Nat. Commun. 2020, 11, 1760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.-L.; Lin, C.-S.; Cheng, C.-C.; Lin, C. A Deep Learning Algorithm for Detecting Acute Pericarditis by Electrocardiogram. J. Pers. Med. 2022, 12, 1150. [Google Scholar] [CrossRef]
- Zheng, J.; Zhang, J.; Danioko, S.; Yao, H.; Guo, H.; Rakovski, C. A 12-lead electrocardiogram database for arrhythmia research covering more than 10,000 patients. Sci. Data 2020, 7, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faust, O.; Shenfield, A.; Kareem, M.; San, T.R.; Fujita, H.; Acharya, U.R. Automated detection of atrial fibrillation using long short-term memory network with RR interval signals. Comput. Biol. Med. 2018, 102, 327–335. [Google Scholar] [CrossRef] [Green Version]
- Gao, J.; Zhang, H.; Lu, P.; Wang, Z. An Effective LSTM Recurrent Network to Detect Arrhythmia on Imbalanced ECG Dataset. J. Healthc. Eng. 2019, 2019, 6320651. [Google Scholar] [CrossRef] [Green Version]
- Guo, L.; Sim, G.; Matuszewski, B. Inter-patient ECG classification with convolutional and recurrent neural networks. Biocybern. Biomed. Eng. 2019, 39, 868–879. [Google Scholar] [CrossRef] [Green Version]
- Murat, F.; Yildirim, O.; Talo, M.; Baloglu, U.B.; Demir, Y.; Acharya, U.R. Application of deep learning techniques for heartbeats detection using ECG signals-analysis and review. Comput. Biol. Med. 2020, 120, 103726. [Google Scholar] [CrossRef]
- Yildirim, O.; Talo, M.; Ciaccio, E.J.; Tan, R.S.; Acharya, U.R. Accurate deep neural network model to detect cardiac arrhythmia on more than 10,000 individual subject ECG records. Comput. Methods Programs Biomed. 2020, 197, 105740. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, S.; Fotoohinasab, A.; Afghah, F. Single-modal and multi-modal false arrhythmia alarm reduction using attention-based convolutional and recurrent neural networks. PLoS ONE 2020, 15, e0226990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.-Y.; Lin, C.-S.; Fang, W.-H.; Lou, Y.-S.; Cheng, C.-C.; Lee, C.-C.; Lin, C. Artificial Intelligence-Enabled Electrocardiography Predicts Left Ventricular Dysfunction and Future Cardiovascular Outcomes: A Retrospective Analysis. J. Pers. Med. 2022, 12, 455. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, O.; Talo, M.; Ay, B.; Baloglu, U.B.; Aydin, G.; Acharya, U.R. Automated detection of diabetic subject using pre-trained 2D-CNN models with frequency spectrum images extracted from heart rate signals. Comput. Biol. Med. 2019, 113, 103387. [Google Scholar] [CrossRef] [PubMed]
- Yoon, T.Y.C.; Lee, H.; Kim, S.; Ji, Y.; Oh, H.; Kang, D. Comparison of 2D-CNN, LSTM, and GRU for cardiovascular disease diagnosis. In Proceedings of the 2022 IEEE International Conference on Consumer Electronics-Asia (ICCE-Asia), Yeosu, Republic of Korea, 26–28 October 2022; pp. 1–5. [Google Scholar]
- Jun, T.N.H.; Kang, D.; Kim, D.; Kim, D.; Kim, Y. ECG arrhythmia classification using a 2-D convolutional neural network. arXiv 2018, arXiv:1804.06812. [Google Scholar] [CrossRef]
- Zhai, X.; Tin, C. Automated ECG Classification Using Dual Heartbeat Coupling Based on Convolutional Neural Network. IEEE Access 2018, 6, 27465–27472. [Google Scholar] [CrossRef]
- Chang, T.-Y.; Chen, K.-W.; Liu, C.-M.; Chang, S.-L.; Lin, Y.-J.; Lo, L.-W.; Hu, Y.-F.; Chung, F.-P.; Lin, C.-Y.; Kuo, L.; et al. A High-Precision Deep Learning Algorithm to Localize Idiopathic Ventricular Arrhythmias. J. Pers. Med. 2022, 12, 764. [Google Scholar] [CrossRef]
- Shafieian, S.; Zulkernine, M. Multi-layer stacking ensemble learners for low footprint network intrusion detection. Complex Intell. Syst. 2022. [Google Scholar] [CrossRef]
- Zhou, Z.-H. Ensemble Methods: Foundations and Algorithms; CRC Press: Boca Raton, FL, USA, 2012. [Google Scholar]
- Butterworth, S. On the Theory of Filter Amplifiers. Wirel. Eng. 1930, 7, 536–541. [Google Scholar]
- Cleveland, W.S.; Devlin, S.J. Locally Weighted Regression: An Approach to Regression Analysis by Local Fitting. J. Am. Stat. Assoc. 1988, 83, 596–610. [Google Scholar] [CrossRef]
- Buades, A.; Coll, B.; Morel, J. A Review of Image Denoising Algorithms, with a New One. Multiscale Model. Simul. 2005, 4, 490–530. [Google Scholar] [CrossRef]
- Lilly, J.M.; Olhede, S.C. Generalized Morse Wavelets as a Superfamily of Analytic Wavelets. IEEE Trans. Signal Process. 2012, 60, 6036–6041. [Google Scholar] [CrossRef] [Green Version]
- Sperandei, S. Understanding logistic regression analysis. Biochem. Med. 2014, 24, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Cervantes, J.; Garcia-Lamont, F.; Rodríguez-Mazahua, L.; Lopez, A. A comprehensive survey on support vector machine classification: Applications, challenges and trends. Neurocomputing 2020, 408, 189–215. [Google Scholar] [CrossRef]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Chen, T.Q.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. In Kdd’16: Proceedings of the 22nd Acm Sigkdd International Conference on Knowledge Discovery and Data Mining; 2016; pp. 785–794. [Google Scholar] [CrossRef] [Green Version]
- He, K.Z.X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Paszke, A.; Gross, S.; Massa, F.; Lerer, A.; Bradbury, J.; Chanan, G.; Killeen, T.; Lin, Z.M.; Gimelshein, N.; Antiga, L.; et al. PyTorch: An Imperative Style, High-Performance Deep Learning Library. Adv. Neur. 2019, 32, 8026–8037. [Google Scholar]
- Kang, D.; Gweon, H.M.; Eun, N.L.; Youk, J.H.; Kim, J.-A.; Son, E.J. A convolutional deep learning model for improving mammographic breast-microcalcification diagnosis. Sci. Rep. 2021, 11, 23925. [Google Scholar] [CrossRef]
- Abdar, M.; Zomorodi-Moghadam, M.; Zhou, X.; Gururajan, R.; Tao, X.; Barua, P.D.; Gururajan, R. A new nested ensemble technique for automated diagnosis of breast cancer. Pattern Recognit. Lett. 2020, 132, 123–131. [Google Scholar] [CrossRef]
- Rao, R.S.; Shivanna, D.B.; Lakshminarayana, S.; Mahadevpur, K.S.; Alhazmi, Y.A.; Bakri, M.M.H.; Alharbi, H.S.; Alzahrani, K.J.; Alsharif, K.F.; Banjer, H.J.; et al. Ensemble Deep-Learning-Based Prognostic and Prediction for Recurrence of Sporadic Odontogenic Keratocysts on Hematoxylin and Eosin Stained Pathological Images of Incisional Biopsies. J. Pers. Med. 2022, 12, 1220. [Google Scholar] [CrossRef]
- Moody, G.B.; Mark, R.G. The impact of the MIT-BIH arrhythmia database. IEEE Eng. Med. Biol. Mag. 2001, 20, 45–50. [Google Scholar] [CrossRef]
- Clifford, G.D.; Liu, C.; Moody, B.; Lehman, L.H.; Silva, I.; Li, Q.; Johnson, A.E.; Mark, R.G. AF Classification from a Short Single Lead ECG Recording: The PhysioNet/Computing in Cardiology Challenge 2017. In Proceedings of the 2017 Computing in Cardiology (CinC), Rennes, France, 24–27 September 2017. [Google Scholar] [CrossRef]
- Eddie Yin Kwee, N.; Feifei, L.; Chengyu, L.; Lina, Z.; Xiangyu, Z.; Xiaoling, W.; Xiaoyan, X.; Yulin, L.; Caiyun, M.; Shoushui, W.; et al. An open access database for evaluating the algorithms of electrocardiogram rhythm and morphology abnormality detection. J. Med. Imaging Health Inform. 2018, 8, 1368–1373. [Google Scholar] [CrossRef]
- Wagner, P.; Strodthoff, N.; Bousseljot, R.D.; Kreiseler, D.; Lunze, F.I.; Samek, W.; Schaeffter, T. PTB-XL, a large publicly available electrocardiography dataset. Sci. Data 2020, 7, 154. [Google Scholar] [CrossRef] [PubMed]
- Merdjanovska, E.; Rashkovska, A. Benchmarking Deep Learning Methods for Arrhythmia Detection. In Proceedings of the 2022 45th Jubilee International Convention on Information, Communication and Electronic Technology (MIPRO), Opatija, Croatia, 23–27 May 2022; pp. 356–361. [Google Scholar]
- Baygin, M.; Tuncer, T.; Dogan, S.; Tan, R.-S.; Acharya, U.R. Automated arrhythmia detection with homeomorphically irreducible tree technique using more than 10,000 individual subject ECG records. Inf. Sci. 2021, 575, 323–337. [Google Scholar] [CrossRef]
- Guan, Y.; An, Y.; Xu, J.; Liu, N.; Wang, J. HA-ResNet: Residual Neural Network With Hidden Attention for ECG Arrhythmia Detection Using Two-Dimensional Signal. IEEE/ACM Trans. Comput. Biol. Bioinform. 2022, 1–10. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 11 ECG Rhythms | Number of Subjects | Number of Training Data | Number of Validation Data | Number of Test Data |
|---|---|---|---|---|
| Atrial Fibrillation (AFIB) | 1780 | 1424 | 178 | 178 |
| Atrial Flutter (AF) | 438 | 350 | 44 | 44 |
| Sinus Tachycardia (ST) | 1564 | 1251 | 157 | 156 |
| Supraventricular Tachycardia (SVT) | 544 | 435 | 55 | 54 |
| Sinus Bradycardia (SB) | 3888 | 3110 | 389 | 389 |
| Sinus Rhythm (SR) | 1825 | 1460 | 182 | 183 |
| Sinus Irregularity (SI) | 397 | 318 | 39 | 40 |
| Meta Learner Classifier | Hyperparameters in Scikit-Learn | Hyperparameter Ranges |
|---|---|---|
| LR | C | 1e-3, 1e-2, 1e-1, 1, 1e1, 1e2, 1e3 |
| SVM | C gamma | 1e-3, 1e-2, 1e-1, 1, 1e1, 1e2, 1e3 1e-3, 1e-2, 1e-1, 1, 1e1, 1e2, 1e3 |
| RF | n_estimators max_depth max_features | 100, 200, 300, 500, 1000, 2000, 3000 5, 10, 15, 20, None ‘log2′, ‘sqrt’ |
| XGBoost | n_estimators max_depth learning_rate | 100, 300, 500, 1000 3, 5, 7, 9 0.1, 0.05, 0.01 |
| Scalogram Image | ECG Grayscale Image | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Lead Names | AUC | ACC (%) | SEN | PRE | F1-Score | AUC | ACC (%) | SEN | PRE | F1-Score |
| Lead I | 0.985 | 88.89 | 0.889 | 0.871 | 0.875 | 0.981 | 88.41 | 0.884 | 0.867 | 0.872 |
| Lead II | 0.991 | 92.24 | 0.922 | 0.916 | 0.916 | 0.988 | 89.56 | 0.896 | 0.888 | 0.889 |
| Lead III | 0.988 | 90.52 | 0.905 | 0.899 | 0.899 | 0.987 | 89.27 | 0.893 | 0.886 | 0.886 |
| aVR | 0.986 | 88.79 | 0.888 | 0.889 | 0.886 | 0.985 | 90.90 | 0.909 | 0.911 | 0.909 |
| aVL | 0.984 | 88.79 | 0.888 | 0.859 | 0.870 | 0.981 | 86.97 | 0.870 | 0.868 | 0.851 |
| aVF | 0.990 | 90.52 | 0.905 | 0.904 | 0.895 | 0.983 | 88.60 | 0.886 | 0.877 | 0.873 |
| V1 | 0.987 | 88.51 | 0.885 | 0.872 | 0.874 | 0.989 | 90.71 | 0.907 | 0.903 | 0.900 |
| V2 | 0.981 | 89.75 | 0.898 | 0.892 | 0.892 | 0.979 | 88.51 | 0.885 | 0.867 | 0.867 |
| V3 | 0.982 | 89.66 | 0.897 | 0.883 | 0.885 | 0.978 | 87.26 | 0.873 | 0.866 | 0.864 |
| V4 | 0.981 | 89.08 | 0.891 | 0.872 | 0.878 | 0.977 | 89.46 | 0.895 | 0.883 | 0.887 |
| V5 | 0.974 | 88.22 | 0.882 | 0.878 | 0.877 | 0.976 | 87.07 | 0.871 | 0.859 | 0.862 |
| V6 | 0.976 | 88.03 | 0.880 | 0.872 | 0.870 | 0.980 | 87.07 | 0.871 | 0.856 | 0.859 |
| Scalogram Image | ECG Grayscale Image | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| AUC | ACC (%) | SEN | PRE | F1-Score | AUC | ACC (%) | SEN | PRE | F1-Score | |
| Single lead | 0.991 | 92.24 | 0.922 | 0.916 | 0.916 | 0.985 | 90.90 | 0.909 | 0.911 | 0.909 |
| Simple averaging ensemble | 0.993 | 91.95 | 0.920 | 0.912 | 0.907 | 0.993 | 91.95 | 0.920 | 0.927 | 0.904 |
| Stacking ensemble (LR) | 0.994 | 92.72 | 0.927 | 0.922 | 0.921 | 0.993 | 93.01 | 0.930 | 0.925 | 0.924 |
| Stacking ensemble (SVM) | 0.993 | 92.34 | 0.923 | 0.915 | 0.913 | 0.993 | 92.53 | 0.925 | 0.919 | 0.917 |
| Stacking ensemble (RF) | 0.993 | 93.01 | 0.930 | 0.925 | 0.923 | 0.993 | 92.53 | 0.925 | 0.918 | 0.918 |
| Stacking ensemble (XGBoost) | 0.995 | 92.91 | 0.929 | 0.924 | 0.925 | 0.993 | 92.34 | 0.923 | 0.918 | 0.919 |
| AUC | ACC (%) | SEN | PRE | F1-Score | |
|---|---|---|---|---|---|
| LSTM | 0.976 | 90.13 | 0.901 | 0.898 | 0.894 |
| BiLSTM | 0.974 | 90.52 | 0.905 | 0.901 | 0.897 |
| Multi-modal simple averaging ensemble | 0.995 | 92.05 | 0.920 | 0.921 | 0.905 |
| Multi-modal stacking ensemble (LR) | 0.995 | 93.97 | 0.940 | 0.937 | 0.936 |
| Multi-modal stacking ensemble (SVM) | 0.995 | 93.39 | 0.934 | 0.930 | 0.928 |
| Multi-modal stacking ensemble (RF) | 0.995 | 93.58 | 0.936 | 0.929 | 0.933 |
| Multi-modal stacking ensemble (XGBoost) | 0.996 | 93.68 | 0.937 | 0.933 | 0.933 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, T.; Kang, D. Multi-Modal Stacking Ensemble for the Diagnosis of Cardiovascular Diseases. J. Pers. Med. 2023, 13, 373. https://doi.org/10.3390/jpm13020373
Yoon T, Kang D. Multi-Modal Stacking Ensemble for the Diagnosis of Cardiovascular Diseases. Journal of Personalized Medicine. 2023; 13(2):373. https://doi.org/10.3390/jpm13020373
Chicago/Turabian StyleYoon, Taeyoung, and Daesung Kang. 2023. "Multi-Modal Stacking Ensemble for the Diagnosis of Cardiovascular Diseases" Journal of Personalized Medicine 13, no. 2: 373. https://doi.org/10.3390/jpm13020373