
The Risk Factors for New-Onset Calf Muscle Venous Thrombosis after Hip Fracture Surgery
Abstract
:1. Introduction
2. Methods
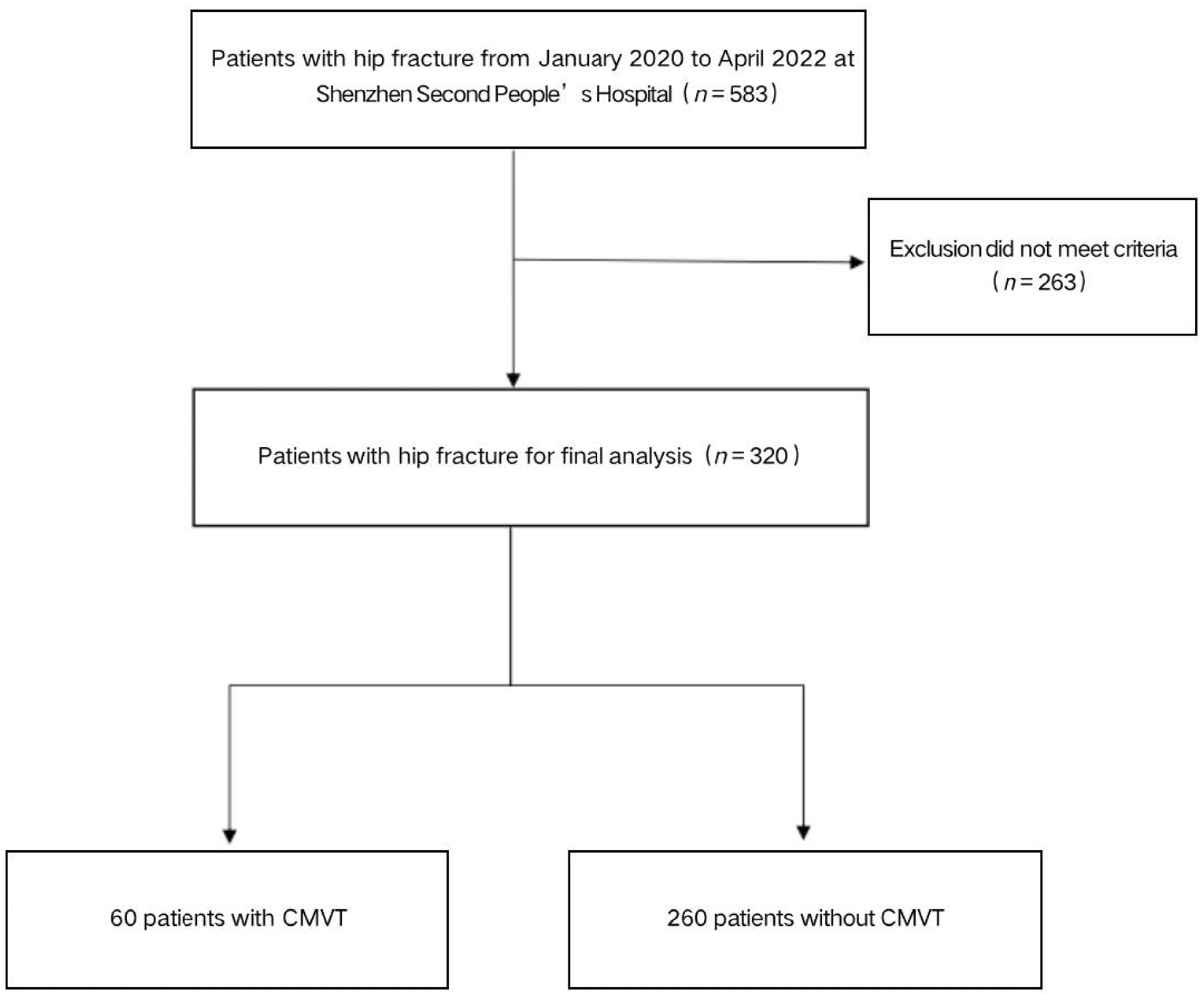
2.1. Patient Selection
2.2. Definition of CMVT
2.3. Data Collection
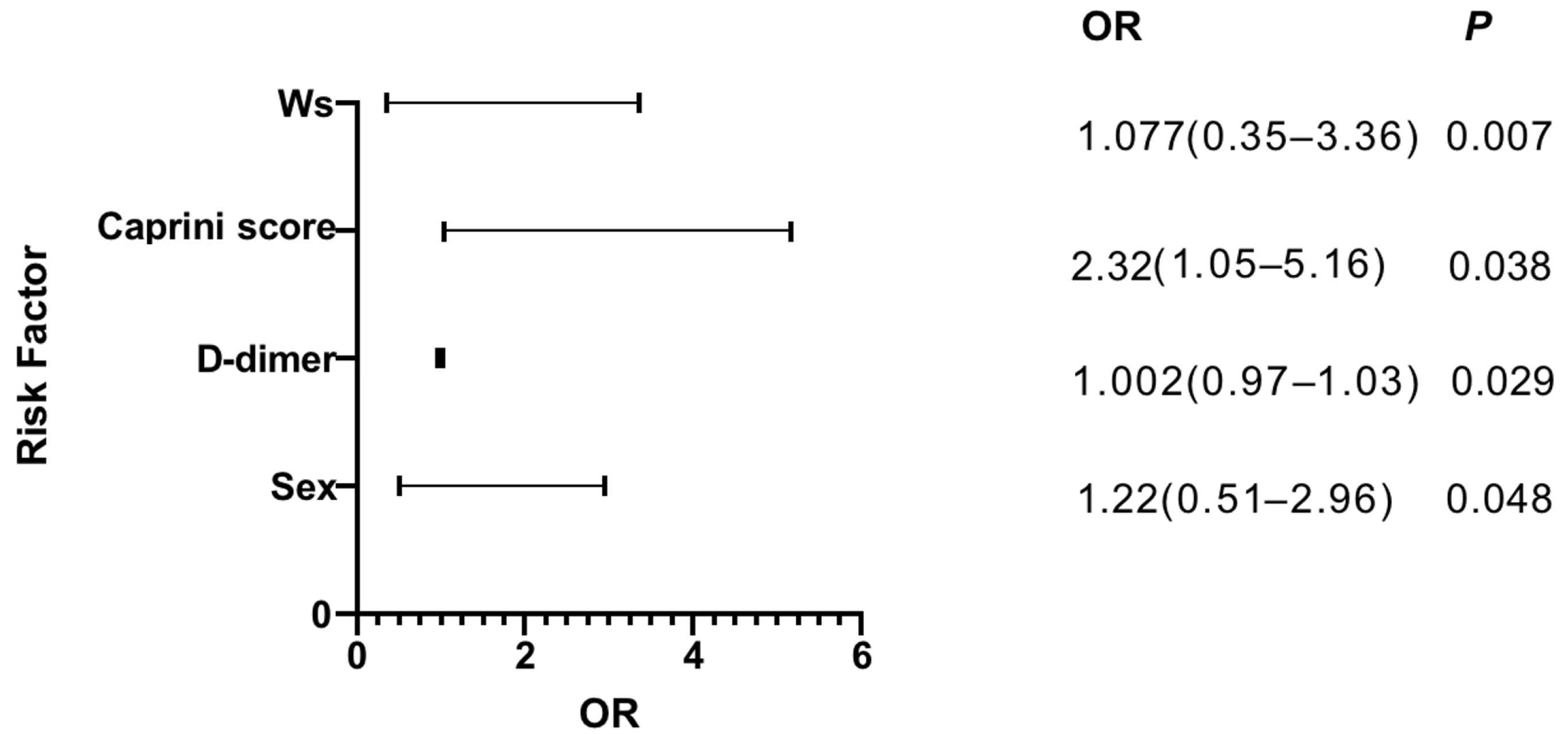
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DVT | deep venous thrombosis |
| CMVT | calf muscle venous thrombosis |
| BMI | body mass index |
| RAM | risk assessment model |
| Ws | Waterlow score |
References
- Zhang, C.; Feng, J.; Wang, S.; Gao, P.; Xu, L.; Zhu, J.; Jia, J.; Liu, L.; Liu, G.; Wang, J.; et al. Incidence of and trends in hip fracture among adults in urban China: A nationwide retrospective cohort study. PLoS Med. 2020, 17, e1003180. [Google Scholar] [CrossRef]
- Gullberg, B.; Johnell, O.; Kanis, J.A. World-wide projections for hip fracture. Osteoporos. Int. 1997, 7, 407–413. [Google Scholar] [CrossRef]
- Irwin, S.C.; Hughes, A.J.; Sheehan, E.; Merghani, K. Trends in Irish hip fracture surgery over a 7-year period and international registry comparison. Surgeon 2022, 20, 94–102. [Google Scholar] [CrossRef]
- Van Dortmont, L.M.C.; Douw, C.M.; van Breukelen, A.M.A.; Laurens, D.R.; Mulder, P.G.H.; Wereldsma, J.C.J.; Van Vugt, A.B. Outcome after hemi-arthroplasty for displaced intracapsular femoral neck fracture related to mental state. Injury 2000, 31, 327–331. [Google Scholar] [CrossRef]
- Lawrence, V.A.; Hilsenbeck, S.G.; Noveck, H.; Poses, R.M.; Carson, J.L. Medical Complications and Outcomes After Hip Fracture Repair. Arch. Intern. Med. 2002, 162, 2053–2057. [Google Scholar] [CrossRef] [Green Version]
- Carpintero, P.; Caeiro, J.R.; Carpintero, R.; Morales, A.; Silva, S.; Mesa, M. Complications of hip fractures: A review. World J. Orthop. 2014, 5, 402–411. [Google Scholar] [CrossRef]
- Geerts, W.H.; Bergqvist, D.; Pineo, G.F.; Heit, J.A.; Samama, C.M.; Lassen, M.R.; Colwell, C.W. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2008, 133, 381S–453S. [Google Scholar]
- Ruppert, A.; Steinle, T.; Lees, M. Economic burden of venous thromboembolism: A systematic review. J. Med. Econ. 2011, 14, 65–74. [Google Scholar] [CrossRef]
- Henry, J.C.; Satiani, B. Calf Muscle Venous Thrombosis: A Review of the Clinical Implications and Therapy. Vasc. Endovasc. Surg. 2014, 48, 396–401. [Google Scholar] [CrossRef]
- Guias, B.; Simoni, G.; Oger, E.; Lemire, A.; Leroyer, C.; Mottier, D.; Nonent, M.; Bressollette, L. Calf muscle venous thrombosis and pulmonary embolism. J. Mal. Vasc. 1999, 24, 132–134. [Google Scholar]
- Hyers, T.M.; Hull, R.D.; Weg, J.G. Antithrombotic therapy for venous thromboembolic disease. Chest 1986, 89, 26S–35S. [Google Scholar] [CrossRef]
- Monreal, M.; Martorell, A.; Callejas, J.M.; Valls, R.; Llamazares, J.F.; Lafoz, E.; Arias, A. Venographic assessment of deep vein thrombosis and risk of developing post-thrombotic syndrome: A prospective study. J. Intern. Med. 1993, 233, 233–238. [Google Scholar] [CrossRef]
- Su, L.-Y.; Guo, F.-J.; Xu, G.; Han, X.-J.; Sun, C.-K.; Zhang, Z.; Jing, Q.-H. Differential diagnosis of isolated calf muscle vein thrombosis and gastrocnemius hematoma by high-frequency ultrasound. Chin. Med. J. 2013, 126, 4448–4452. [Google Scholar]
- Zhuang, G.; Tang, C.; He, X.; Liang, J.; He, Z.; Ye, Y.; Deng, W.; Liu, D.; Chen, H. DANTE-SPACE: A new technical tool for DVT on 1.5T MRI. Int. J. Cardiovasc. Imaging 2019, 35, 2231–2237. [Google Scholar] [CrossRef] [Green Version]
- Schellong, S.M. Distal DVT: Worth diagnosing? Yes: Distal DVT: Worth diagnosing? J. Thromb. Haemost. 2007, 5, 51–54. [Google Scholar] [CrossRef]
- Warren, J.A.; Sundaram, K.; Anis, H.K.; Kamath, A.F.; Higuera, C.A.; Piuzzi, N.S. Have Venous Thromboembolism Rates Decreased in Total Hip and Knee Arthroplasty? J. Arthroplast. 2020, 35, 259–264. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.S. Deep Vein Thrombosis Prophylaxis after Total Hip Arthroplasty in Asian Patients. Hip Pelvis 2018, 30, 197–201. [Google Scholar] [CrossRef]
- Watson, T.; Shantsila, E.; Lip, G.Y.H. Mechanisms of thrombogenesis in atrial fibrillation: Virchow’s triad revisited. Lancet 2009, 373, 155–166. [Google Scholar] [CrossRef]
- Kyrle, P.A.; Minar, E.; Bialonczyk, C.; Hirschl, M.; Weltermann, A.; Eichinger, S. The Risk of Recurrent Venous Thromboembolism in Men and Women. New Engl. J. Med. 2004, 350, 2558–2563. [Google Scholar] [CrossRef]
- Bezemer, I.D.; Bare, L.A.; Doggen, C.J.M.; Arellano, A.R.; Tong, C.; Rowland, C.M.; Catanese, J.; Young, B.A.; Reitsma, P.H.; Devlin, J.J.; et al. Gene Variants Associated With Deep Vein Thrombosis. JAMA 2008, 299, 1306–1314. [Google Scholar] [CrossRef] [Green Version]
- Roach, R.E.J.; Cannegieter, S.C.; Lijfering, W.M. Differential risks in men and women for first and recurrent venous thrombosis: The role of genes and environment. J. Thromb. Haemost. 2014, 12, 1593–1600. [Google Scholar] [CrossRef] [PubMed]
- Bates, S.M.; Jaeschke, R.; Stevens, S.M.; Goodacre, S.; Wells, P.S.; Stevenson, M.D.; Kearon, C.; Schunemann, H.J.; Crowther, M.; Pauker, S.G.; et al. Diagnosis of DVT: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141, e351S–e418S. [Google Scholar] [CrossRef] [Green Version]
- Wolberg, A.S.; Rosendaal, F.R.; Weitz, J.I.; Jaffer, I.H.; Agnelli, G.; Baglin, T.; Mackman, N. Venous thrombosis. Nat. Rev. Dis. Prim. 2015, 1, 15006. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.; Rudd, A.; Lewis, R.R.; Hunt, B.J. Plasma D-dimers in the diagnosis of venous thromboembolism. Arch. Intern. Med. 2002, 162, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Schutgens, R.; Ackermark, P.; Haas, F.; Nieuwenhuis, H.; Peltenburg, H.; Pijlman, A.; Pruijm, M.; Oltmans, R.; Kelder, J.; Biesma, D.H. Combination of a Normal D-Dimer Concentration and a Non-High Pretest Clinical Probability Score Is a Safe Strategy to Exclude Deep Venous Thrombosis. Circulation 2003, 107, 593–597. [Google Scholar] [CrossRef] [Green Version]
- Cheng, J.; Fu, Z.; Zhu, J.; Zhou, L.; Song, W. The predictive value of plasminogen activator inhibitor-1, fibrinogen, and D-dimer for deep venous thrombosis following surgery for traumatic lower limb fracture. Ann. Palliat. Med. 2020, 9, 88. [Google Scholar] [CrossRef]
- Deng, W.; Huo, L.; Yuan, Q.; Huang, D.; Li, Q.; Tian, W. Risk factors for venous thromboembolism in patients with diabetes undergoing joint arthroplasty. BMC Musculoskelet. Disord. 2021, 22, 608. [Google Scholar] [CrossRef]
- Wu, J.X.; Qing, J.H.; Yao, Y.; Chen, D.Y.; Jiang, Q. Performance of age-adjusted D-dimer values for predicting DVT before the knee and hip arthroplasty. J. Orthop. Surg. Res. 2021, 16, 82. [Google Scholar] [CrossRef]
- Caprini, J.A. Thrombosis Risk Assessment as a Guide to Quality Patient Care. Dis. Month 2005, 51, 70–78. [Google Scholar] [CrossRef]
- Bo, H.; Li, Y.; Liu, G.; Ma, Y.; Li, Z.; Cao, J.; Liu, Y.; Jiao, J.; Li, J.; Li, F.; et al. Assessing the Risk for Development of Deep Vein Thrombosis among Chinese Patients using the 2010 Caprini Risk Assessment Model: A Prospective Multicenter Study. J. Atheroscler. Thromb. 2020, 27, 801–808. [Google Scholar] [CrossRef] [Green Version]
- Dashe, J.; Parisien, R.L.; Pina, M.; De Giacomo, A.F.; Tornetta, P. Is the Caprini Score Predictive of Venothromboembolism Events in Orthopaedic Fracture Patients? J. Orthop. Trauma 2019, 33, 269–275. [Google Scholar] [CrossRef]
- Peng, J.; Wang, H.; Zhang, L.; Lin, Z. Construction and efficiency analysis of prediction model for venous thromboembolism risk in the elderly after hip fracture. J. Central South Univ. Med. Sci. 2021, 46, 142–148. [Google Scholar]
- Wang, H.; Lv, B.; Li, W.; Wang, S.; Ding, W. Diagnostic Performance of the Caprini Risk Assessment Model Combined With D-Dimer for Preoperative Deep Vein Thrombosis in Patients With Thoracolumbar Fractures Caused by High-Energy Injuries. World Neurosurg. 2022, 157, e410–e416. [Google Scholar] [CrossRef] [PubMed]
- Waterlow, J. Pressure sores: A risk assessment card. Nurs. Times 1985, 81, 49–55. [Google Scholar] [PubMed]
- Anthony, D.; Reynolds, T.; Russell, L. A regression analysis of the Waterlow score in pressure ulcer risk assessment. Clin. Rehabil. 2003, 17, 216–223. [Google Scholar] [CrossRef]
- Thorn, C.C.; Smith, M.; Aziz, O.; Holme, T.C. The Waterlow score for risk assessment in surgical patients. Ind. Mark. Manag. 2013, 95, 52–56. [Google Scholar] [CrossRef] [Green Version]
- Nayar, S.; Li, D.; Ijaiya, B.; Lloyd, D.; Bharathan, R. Waterlow score for risk assessment in surgical patients: A systematic review. Ind. Mark. Manag. 2021, 103, 312–317. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Patients with CMVT (n = 60) | Patients without CMVT (n = 260) | p Value | |
|---|---|---|---|---|
| Age | 75.38 (12.32) | 75.00 (12.32) | 0.254 | |
| Time to surgery | 1.63 (1.60) | 1.65 (1.531) | 0.937 | |
| Duration of surgery | 86.12 (40.38) | 88.9 (36.72) | 0.604 | |
| Waterlow score | 16.67 (3.17) | 16.97 (3.45) | 0.53 | |
| Infusion volume | 1370.0 (432.28) | 1269.23 (438.84) | 0.108 | |
| SBP | 124.42 (19.32) | 122.01 (17.71) | 0.352 | |
| DBP | 66.37 (9.61) | 65.22 (8.57) | 0.353 | |
| Caprini score | 8.65 (1.40) | 7.89 (2.62) | 0.03 | |
| Preoperative D-dimer | 5.44 (9.04) | 5.16 (11.19) | 0.881 | |
| BMI | 22.03 (3.39) | 22.13 (3.99) | 0.867 | |
| Sex | 0.153 | |||
| Male | 45 (75.0%) | 170 (65.4%) | ||
| Female | 15 (25.0%) | 90 (34.6%) | ||
| Diagnosis | 0.8 | |||
| Femoral neck fractures | 42 (70.0%) | 181 (69.6%) | ||
| Intertrochanteric fractures | 17 (28.3%) | 77 (29.6%) | ||
| Subtrochanteric fractures | 1 (1.7%) | 2 (0.8%) | ||
| Hypertension | 25 (42.3%) | 107 (41.2%) | 0.942 | |
| Diabetes | 12 (20.0%) | 48 (18.5%) | 0.783 | |
| Cardiovascular | 8 (13.3%) | 26 (10.0%) | 0.45 | |
| Comorbidity | 0.395 | |||
| 0 | 26 (43.3%) | 89 (34.2%) | ||
| 1–2 | 22 (36.7%) | 128 (49.2%) | ||
| ≥3 | 12 (20.0%) | 33 (16.5%) | ||
| Previous surgical history | 23 (38.3%) | 109 (41.9%) | 0.611 | |
| Type of Anesthesia | 0.614 | |||
| General anesthesia | 9 (15.0%) | 29 (11.2%) | ||
| Epidural anesthesia | 43 (41.3%) | 231 (88.8%) | ||
| Operative procedures | 0.845 | |||
| THA | 26 (43.3%) | 112 (43.1%) | ||
| Hemiarthroplasty | 18 (30%) | 67 (25.8%) | ||
| PFNA | 15 (25.0%) | 78 (30.0%) | ||
| ORIF | 1 (1,7%) | 3 (1.2%) | ||
| NYHA | 0.177 | |||
| I–II | 54 (90.0%) | 250 (92.3%) | ||
| III–IV | 6 (10.0%) | 20 (7.7%) | ||
| ASA | 0.824 | |||
| I–II | 24 (40.0%) | 113 (43.5%) | ||
| III–IV | 36 (60.0%) | 147 (56.6%) | ||
| Mallamptis | 0.742 | |||
| I–II | 41 (68.3%) | 192 (73.8%) | ||
| III–IV | 19 (31.6%) | 68 (25.1%) |
| Variables | AUC | 95%CI Lower Bound | 95%CI Upper Bound | p Value |
|---|---|---|---|---|
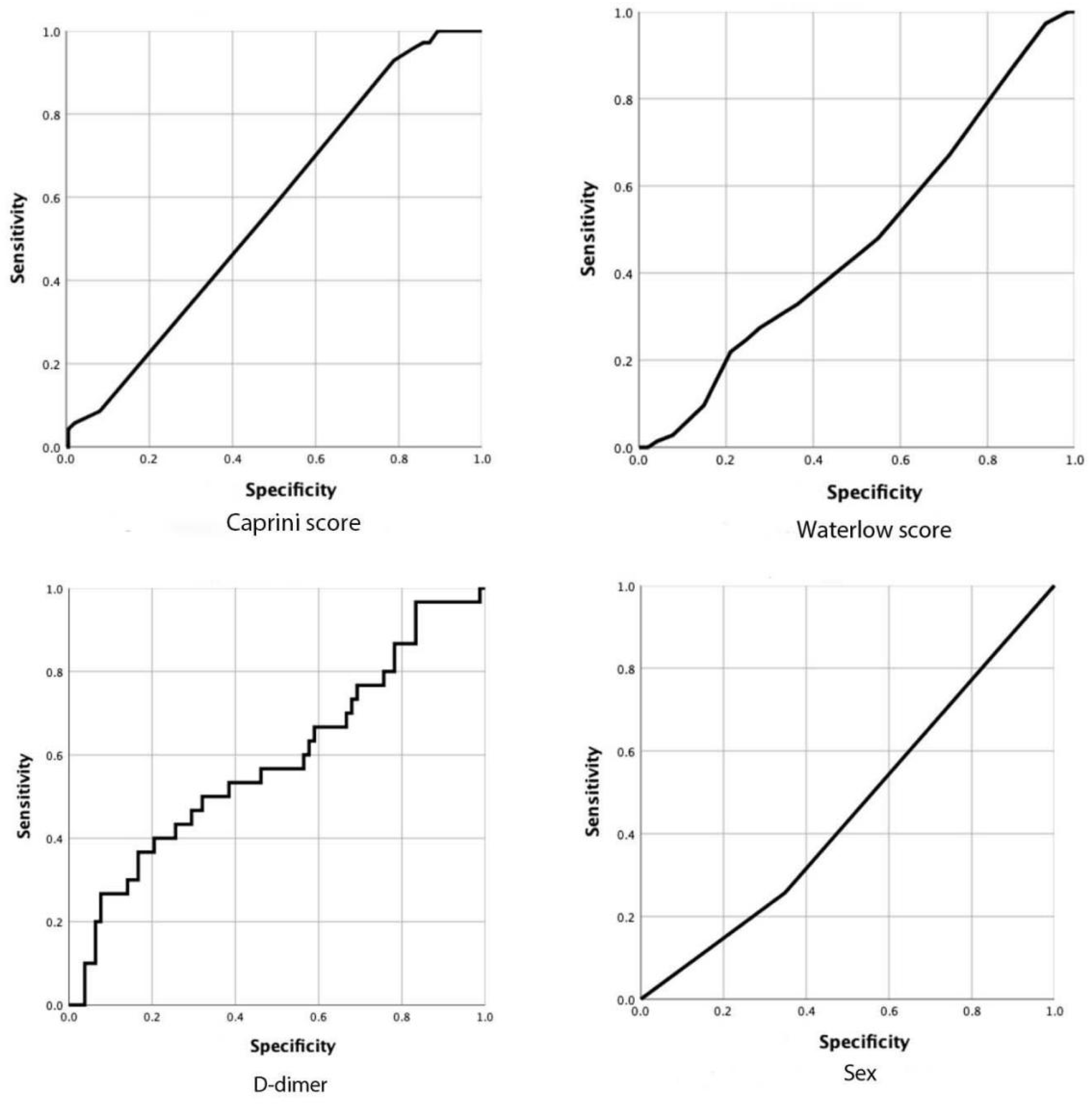
| Caprini score | 0.593 | 0.520 | 0.667 | 0.019 |
| Waterlow score | 0.474 | 0.398 | 0.550 | 0.515 |
| Sex | 0.503 | 0.425 | 0.581 | 0.943 |
| D-dimer | 0.585 | 0.460 | 0.710 | 0.17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhuang, Q.; He, Q.; Aikebaier, A.; Chen, W.; Liu, J.; Wang, D. The Risk Factors for New-Onset Calf Muscle Venous Thrombosis after Hip Fracture Surgery. J. Pers. Med. 2023, 13, 257. https://doi.org/10.3390/jpm13020257
Zhuang Q, He Q, Aikebaier A, Chen W, Liu J, Wang D. The Risk Factors for New-Onset Calf Muscle Venous Thrombosis after Hip Fracture Surgery. Journal of Personalized Medicine. 2023; 13(2):257. https://doi.org/10.3390/jpm13020257
Chicago/Turabian StyleZhuang, Qianzheng, Qifei He, Aobulikasimu Aikebaier, Wenshi Chen, Jianquan Liu, and Daping Wang. 2023. "The Risk Factors for New-Onset Calf Muscle Venous Thrombosis after Hip Fracture Surgery" Journal of Personalized Medicine 13, no. 2: 257. https://doi.org/10.3390/jpm13020257