


PD-L1, CD4+, and CD8+ Tumor-Infiltrating Lymphocytes (TILs) Expression Profiles in Melanoma Tumor Microenvironment Cells

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Group
2.2. TILs Evaluation
2.3. Immunohistochemical (IHC) Analysis
2.4. Statistical Analysis
3. Results
3.1. Clinico-Pathological Analysis of Melanoma Tumor Microenvironment Cells, Associated with IHC Patterns of PD-L1 (+/-) Expression
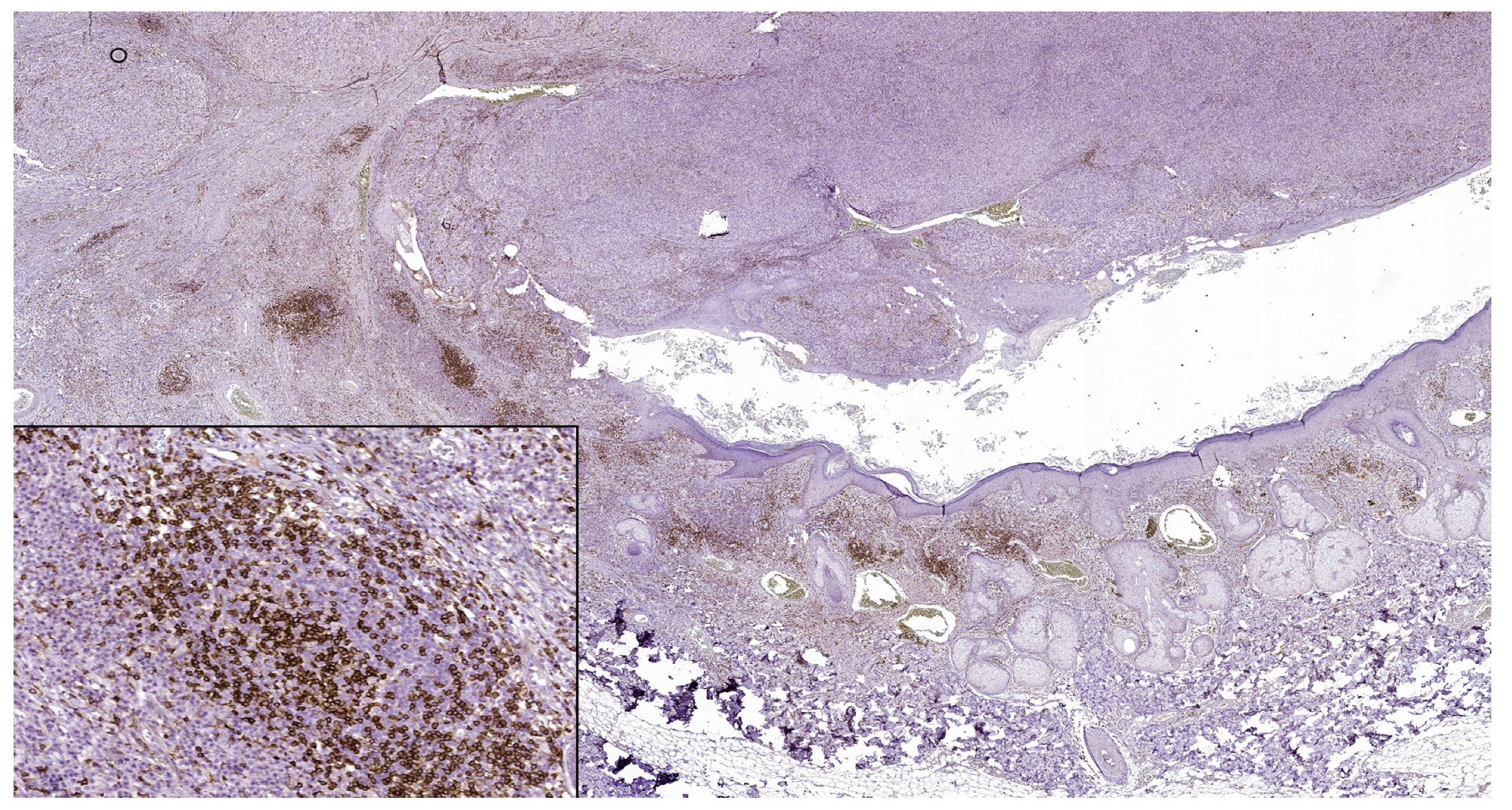
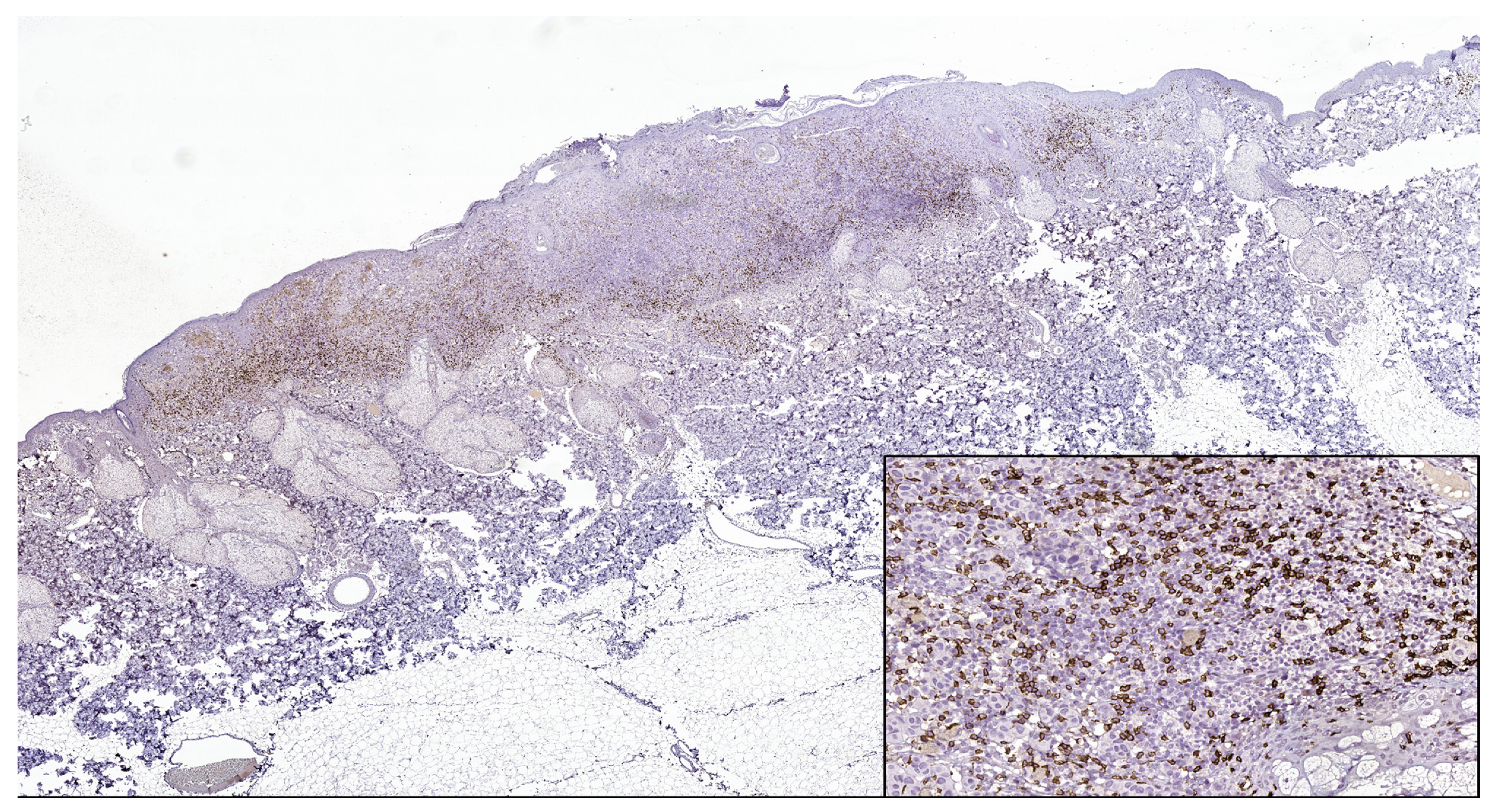
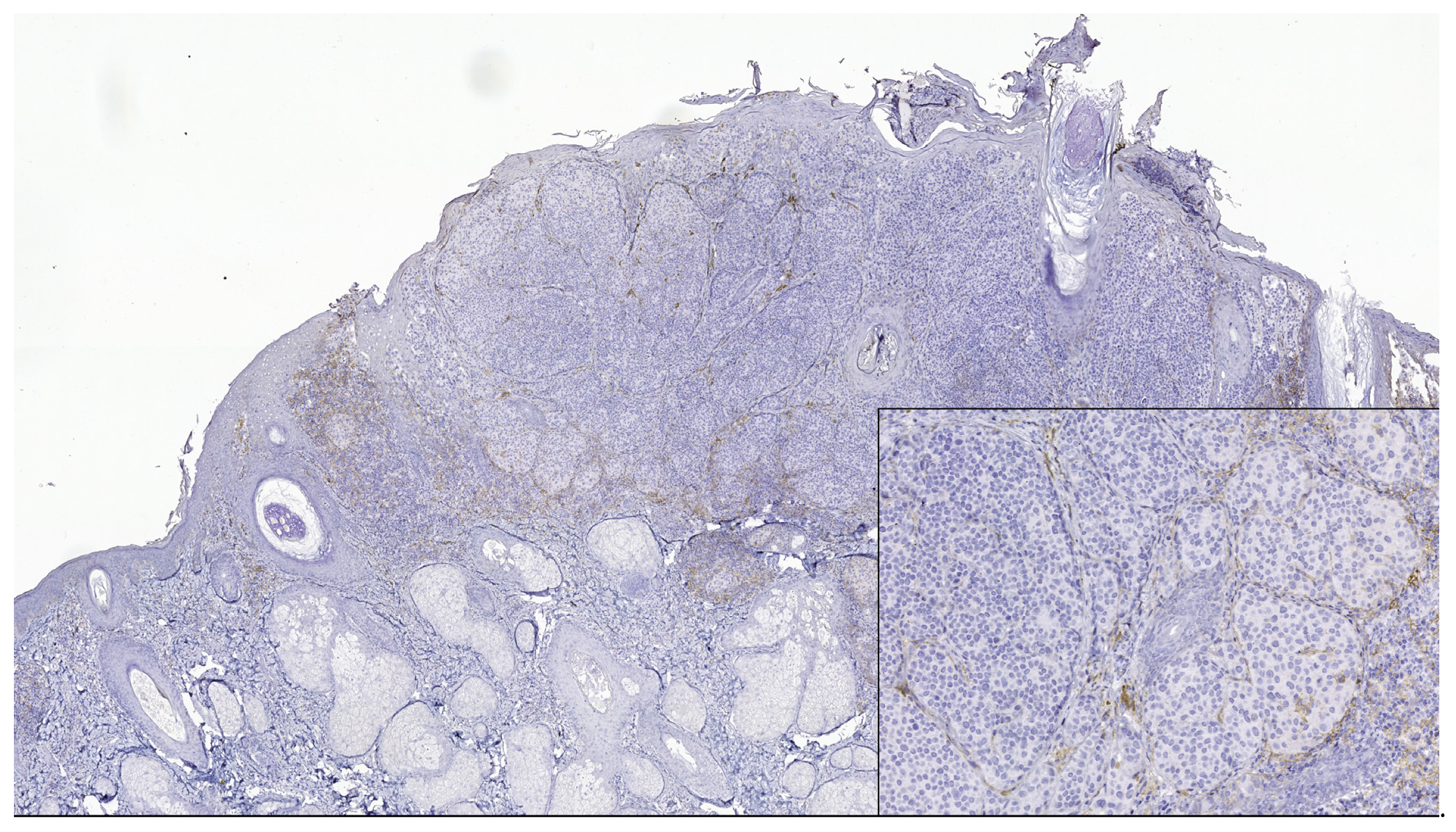
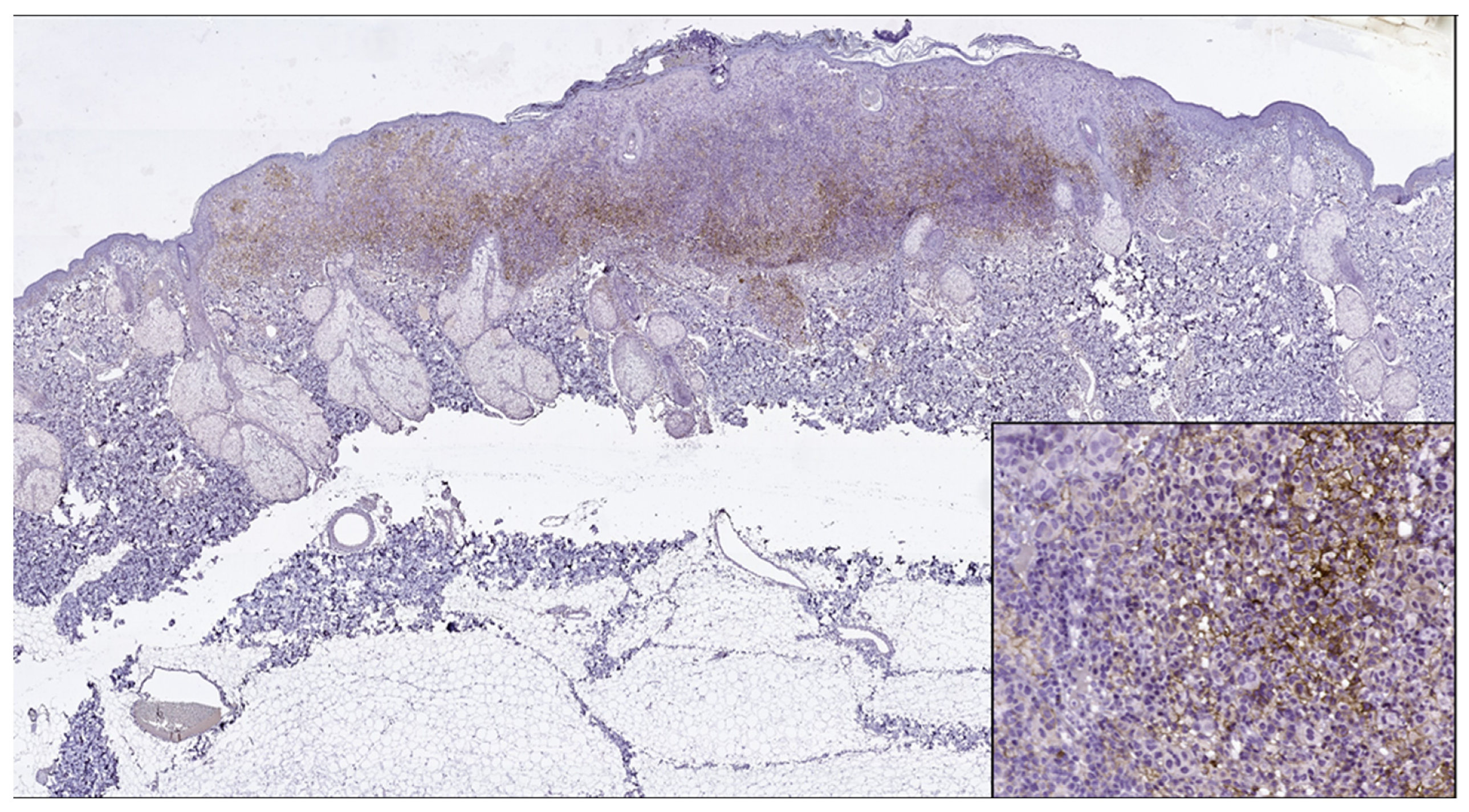
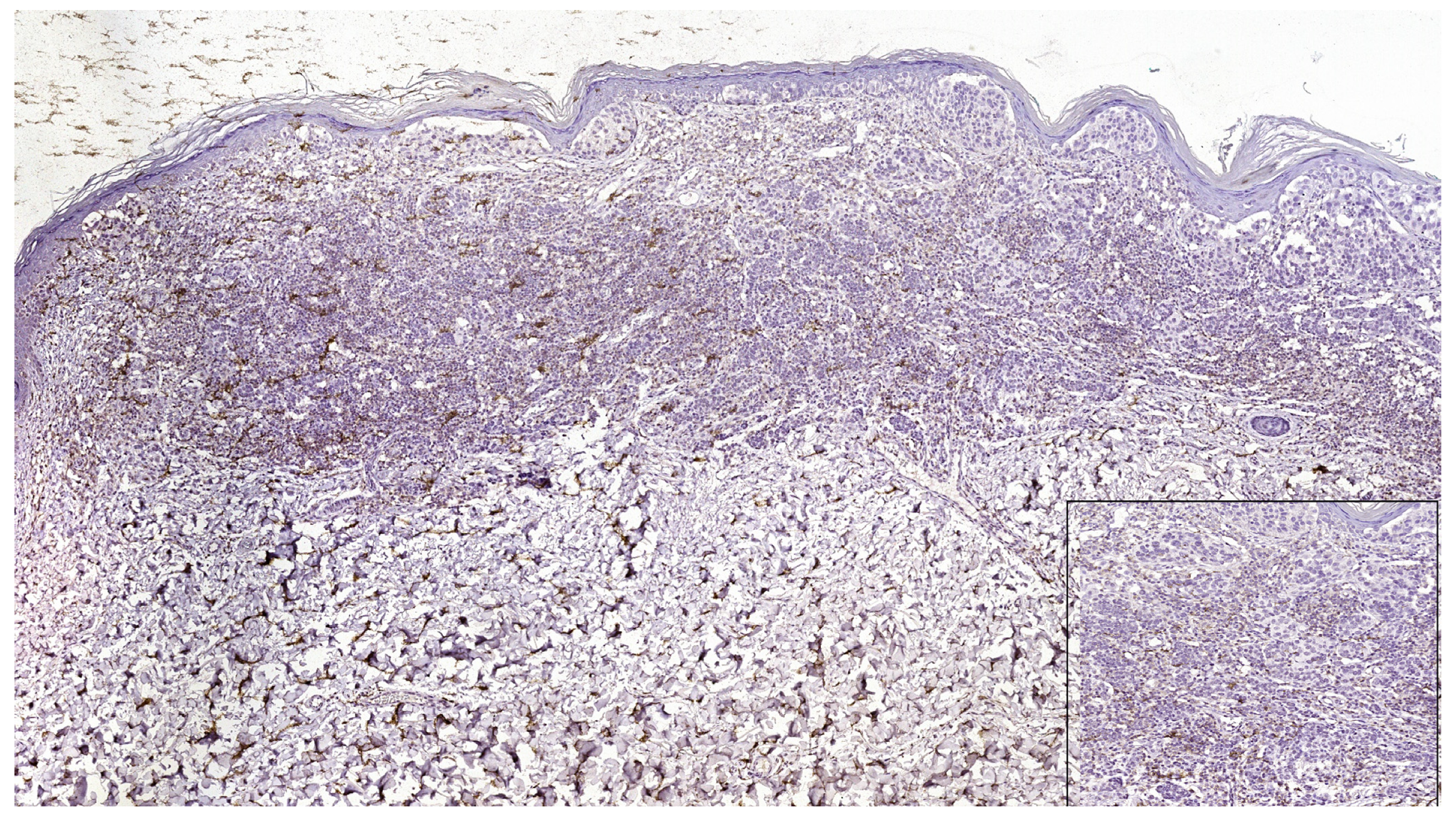
3.2. PD-L1 Expression in Tumor Cells and Immune-Infiltrating Cells in Various Morphological Types of Melanoma and Tils Quantification and Characterization
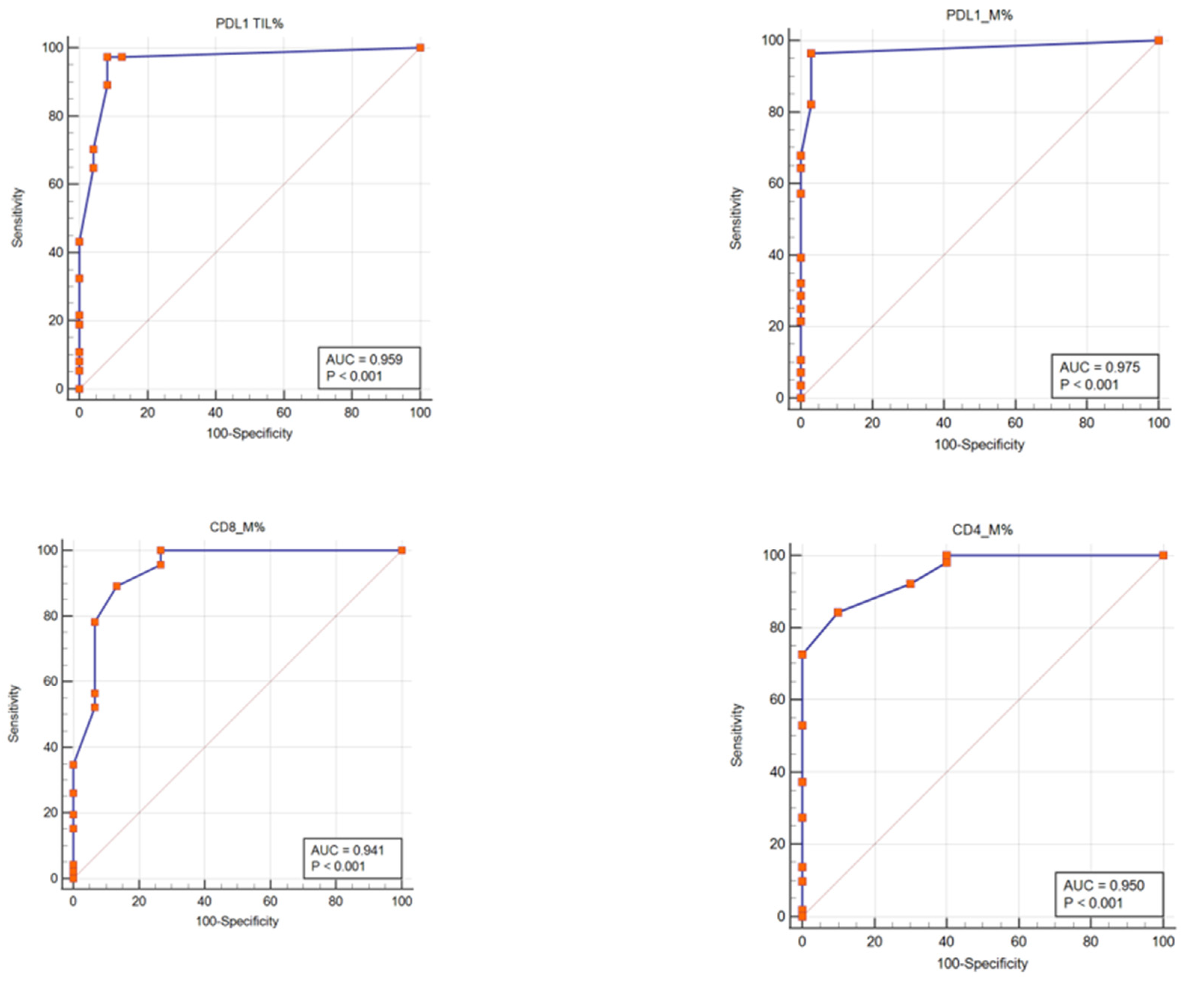
3.3. Predictive and Prognostic Roles of PD-L1, CD4, and CD8 Tumor-Infiltrating Lymphocytes Biomarkers in Melanoma Tumor Microenvironment Cells
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- O’Neill, C.H.; Scoggins, C.R. Melanoma. J. Surg. Oncol. 2019, 120, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Rodić, N.; Anders, R.A.; Eshleman, J.R.; Lin, M.-T.; Xu, H.; Kim, J.H.; Beierl, K.; Chen, S.; Luber, B.S.; Wang, H.; et al. PD-L1 expression in melanocytic lesions does not correlate with the BRAF V600E mutation. Cancer Immunol. Res. 2015, 3, 110–115. [Google Scholar] [CrossRef] [Green Version]
- Fujimura, T.; Fujisawa, Y.; Kambayashi, Y.; Aiba, S. Significance of BRAF kinase inhibitors for melanoma treatment: From bench to bedside. Cancers 2019, 11, 1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiss, S.A.; Wolchok, J.D.; Sznol, M. Immunotherapy of melanoma: Facts and hopes. Clin Cancer Res. 2019, 25, 5191–5201. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Dong, M.; Shui, Y.; Zhang, Y.; Zhang, Z.; Mi, Y.; Zuo, X.; Jiang, L.; Liu, K.; Liu, Z.; et al. A pooled analysis of the prognostic value of PD-L1 in melanoma: Evidence from 1062 patients. Cancer Cell Int. 2020, 20, 96. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Jiang, C.C.; Jin, L.; Zhang, X.D. Regulation of PD-L1: A novel role of pro-survival signalling in cancer. Ann. Oncol. 2016, 27, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Wei, R.; Guo, L.B.; Wang, Q.S.; Miao, J.; Kwok, H.F.; Lin, Y. Targeting PD-L1 protein: Translation, modification and transport. Curr. Protein Pept. Sci. 2019, 20, 82–91. [Google Scholar] [CrossRef]
- Jiang, X.J.; Wang, J.; Deng, X.Y.; Xiong, F.; Ge, J.S.; Xiang, B.; Wu, X.; Ma, J.; Zhou, M.; Li, X.L.; et al. Role of the tumor microenvironment in PD-L1/PD-1-mediated tumor immune escape. Mol. Cancer 2019, 18, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.P.; Han, X. Anti-PD-1/PD-L1 therapy of human cancer: Past, present, and future. J. Clin. Investig. 2015, 125, 3384–3391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, H.; Strome, S.E.; Salomao, D.R.; Tamura, H.; Hirano, F.; Flies, D.B.; Roche, P.C.; Lu, J.; Zhu, G.; Tamada, K.; et al. Tumor-associated B7-H1 promotes T-cell apoptosis: A potential mechanism of immune evasion. Nat. Med. 2002, 8, 793–800. [Google Scholar] [CrossRef]
- Madore, J.; Strbenac, D.; Vilain, R.; Menzies, A.M.; Yang, J.Y.H.; Thompson, J.F.; Long, G.V.; Mann, G.J.; Scolyer, R.A.; Wilmott, J.S. PD-L1 Negative Status is Associated with Lower Mutation Burden, Differential Expression of Immune-Related Genes, and Worse Survival in Stage III Melanoma. Clin. Cancer Res. 2016, 22, 3915–3923. [Google Scholar] [CrossRef] [Green Version]
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Maio, M.; Mortier, L.; Hassel, J.C.; Rutkowski, P.; McNeil, C.; Kalinka-Warzocha, E.; et al. Nivolumab in previously untreated melanoma without BRAF mutation. N. Engl. J. Med. 2015, 372, 320–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weber, J.S.; D’Angelo, S.P.; Minor, D.; Hodi, F.S.; Gutzmer, R.; Neyns, B.; Hoeller, C.; Khushalani, N.I.; Miller, W.H., Jr.; Lao, C.D.; et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): A randomized, controlled, open-label, phase 3 trial. Lancet Oncol. 2015, 16, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Sunshine, J.C.; Nguyen, P.L.; Kaunitz, G.J.; Cottrell, T.R.; Berry, S.; Esandrio, J.; Xu, H.; Ogurtsova, A.; Bleich, K.B.; Cornish, T.C.; et al. PD-L1 Expression in Melanoma: A Quantitative Immunohistochemical Antibody Comparison. Clin. Cancer Res. 2017, 23, 4938–4944. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.; Boyle, T.A.; Zhou, C.; Rimm, D.L.; Hirsch, F.R. PD-L1 expression in lung cancer. J. Thorac. Oncol. 2016, 11, 964–975. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.X.; Wang, X.S.; Wang, Y.F.; Hu, X.C.; Yan, J.Q.; Zhang, Y.L.; Wang, W.; Yang, R.J.; Feng, Y.Y.; Gao, S.G.; et al. Prognostic significance of PD-L1 expression in patients with gastric cancer in East Asia: A meta-analysis. Oncotarg. Ther. 2016, 9, 2649–2654. [Google Scholar]
- Huang, L.J.; Deng, X.F.; Chang, F.; Wu, X.L.; Wu, Y.; Diao, Q.Z. Prognostic significance of programmed cell death ligand 1 expression in patients with ovarian carcinoma A systematic review and meta-analysis. Medicine 2018, 97, 43. [Google Scholar]
- Wu, Z.; Zhang, L.; Peng, J.; Xu, S.; Zhou, L.; Lin, Y.; Wang, Y.; Lu, J.; Yin, W.; Lu, J. Predictive and prognostic value of PDL1 protein expression in breast cancer patients in neoadjuvant setting. Cancer Biol. Ther. 2019, 20, 941–947. [Google Scholar] [CrossRef] [Green Version]
- Gevensleben, H.; Dietrich, D.; Golletz, C.; Steiner, S.; Jung, M.; Thiesler, T.; Majores, M.; Stein, J.; Uhl, B.; Muller, S.; et al. The immune checkpoint regulator PD-L1 is highly expressed in aggressive primary prostate cancer. Clin. Cancer Res. 2016, 22, 1969–1977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, B.; Pan, W.; Yang, M.; Yang, W.; He, W.; Chen, X.; Bi, J.; Jiang, N.; Huang, J.; Lin, T. Programmed death ligand-1 is associated with tumor infiltrating lymphocytes and poorer survival in urothelial cell carcinoma of the bladder. Cancer Sci. 2019, 110, 489–498. [Google Scholar] [CrossRef]
- Gu, X.; Dong, M.; Liu, Z.; Mi, Y.; Yang, J.; Zhang, Z.; Liu, K.; Jiang, L.; Zhang, Y.; Dong, S.; et al. Elevated PD-L1 expression predicts poor survival outcomes in patients with cervical cancer. Cancer Cell Int. 2019, 19, 146. [Google Scholar] [CrossRef]
- Lee, L.H.; Cavalcanti, M.S.; Segal, N.H.; Hechtman, J.F.; Weiser, M.R.; Smith, J.J.; Garcia-Aguilar, J.; Sadot, E.; Ntiamoah, P.; Markowitz, A.J.; et al. Patterns and prognostic relevance of PD-1 and PD-L1 expression in colorectal carcinoma. Mod. Pathol. 2016, 29, 1433–1442. [Google Scholar] [CrossRef] [Green Version]
- Liang, X.; Sun, J.; Wu, H.; Luo, Y.; Wang, L.; Lu, J.; Zhang, Z.; Guo, J.; Liang, Z.; Liu, T. PD-L1 in pancreatic ductal adenocarcinoma: A retrospective analysis of 373 Chinese patients using an in vitro diagnostic assay. Diagn. Pathol. 2018, 13, 5. [Google Scholar] [CrossRef] [PubMed]
- Motoshima, T.; Komohara, Y.; Ma, C.; Dewi, A.K.; Noguchi, H.; Yamada, S.; Nakayama, T.; Kitada, S.; Kawano, Y.; Takahashi, W.; et al. PD-L1 expression in papillary renal cell carcinoma. BMC Urol. 2017, 17, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, J.; Ahn, S.; Yoo, K.H.; Kim, J.H.; Choi, S.H.; Jang, K.T.; Lee, J. Treatment outcome of PD-1 immune checkpoint inhibitor in Asian metastatic melanoma patients: Correlative analysis with PD-L1 immunohistochemistry. Invest. N. Drugs 2016, 34, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Gadiot, J.; Hooijkaas, A.I.; Kaiser, A.D.M.; van Tinteren, H.; van Boven, H.; Blank, C. Overall survival and PD-L1 expression in metastasized malignant melanoma. Cancer 2011, 117, 2192–2201. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.B.; Bordeaux, J.; Kim, J.Y.; Vaupel, C.; Rimm, D.L.; Ho, T.H.; Joseph, R.W.; Daud, A.I.; Conry, R.M.; Gaughan, E.M.; et al. Quantitative spatial profiling of PD-1/PD-L1 interaction and HLA-DR/IDO-1 predicts improved outcomes of anti-PD-1 therapies in metastatic melanoma. Clin. Cancer Res. 2018, 24, 5250–5260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madonna, G.; Ballesteros-Merino, C.; Feng, Z.; Bifulco, C.; Capone, M.; Giannarelli, D.; Mallardo, D.; Simeone, E.; Grimaldi, A.M.; Caraco, C.; et al. PD-L1 expression with immune-infiltrate evaluation and outcome prediction in melanoma patients treated with ipilimumab. Oncoimmunology 2018, 7, e1405206. [Google Scholar] [CrossRef] [Green Version]
- Madore, J.; Vilain, R.E.; Menzies, A.M.; Kakavand, H.; Wilmott, J.S.; Hyman, J.; Yearley, J.H.; Kefford, R.F.; Thompson, J.F.; Long, G.V.; et al. PD-L1 expression in melanoma shows marked heterogeneity within and between patients: Implications for anti-PD-1/PD-L1 clinical trials. Pigment Cell Melanoma Res. 2015, 28, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Massi, D.; Brusa, D.; Merelli, B.; Falcone, C.; Xue, G.; Carobbio, A.; Nassini, R.; Baroni, G.; Tamborini, E.; Cattaneo, L.; et al. The status of PD-L1 and tumor infiltrating immune cells predict resistance and poor prognosis in BRAF treated melanoma patients harboring mutant BRAFV600. Ann. Oncol. 2015, 26, 1980–1987. [Google Scholar] [CrossRef] [PubMed]
- Morrison, C.; Pabla, S.; Conroy, J.M.; Nesline, M.K.; Glenn, S.T.; Dressman, D.; Papanicolau-Sengos, A.; Burgher, B.; Andreas, J.; Giamo, V.; et al. Predicting response to checkpoint inhibitors in melanoma beyond PD-L1 and mutational burden. J. Immunother. Cancer 2018, 6, 32. [Google Scholar] [CrossRef] [PubMed]
- Obeid, J.M.; Erdag, G.; Smolkin, M.E.; Deacon, D.H.; Patterson, J.W.; Chen, L.; Bullock, T.N.; Slingluff, C.L. PD-L1, PD-L2 and PD-1 expression in metastatic melanoma: Correlation with tumor-infiltrating immune cells and clinical outcome. Oncoimmunology 2016, 5, e1235107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, M.; Dai, B.; Kong, Y.Y.; Lv, J.J.; Cai, X. PD-L1 expression in tumour-infiltrating lymphocytes is a poor prognostic factor for primary acral melanoma patients. Histopathology 2018, 73, 386–396. [Google Scholar] [CrossRef]
- Ren, Y.; Lv, Q.; Yue, W.; Liu, B.; Zou, Z. The programmed cell death protein-1/programmed cell death ligand 1 expression, CD3+ T cell infiltration, NY-ESO-1 expression, and microsatellite instability phenotype in primary cutaneous melanoma and mucosal melanoma and their clinical significance and prognostic value: A study of 89 consecutive cases. Melanoma Res. 2019, 30, 85–101. [Google Scholar]
- Schaper-Gerhardt, K.; Okoye, S.; Herbst, R.; Ulrich, J.; Terheyden, P.; Pfohler, C.; Utikal, J.S.; Kreuter, A.; Mohr, P.; Dippel, E.; et al. PD-L1 status does not predict the outcome of BRAF inhibitor therapy in metastatic melanoma. Eur. J. Cancer 2018, 88, 67–76. [Google Scholar] [CrossRef]
- Thierauf, J.; Veit, J.A.; Affolter, A.; Bergmann, C.; Grunow, J.; Laban, S.; Lennerz, J.K.; Grunmuller, L.; Mauch, C.; Plinkert, P.K.; et al. Identification and clinical relevance of PD-L1 expression in primary mucosal malignant melanoma of the head and neck. Melanoma Res. 2015, 25, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.Y.; Wu, X.Y.; Zhang, X.; Yang, X.H.; Long, Y.K.; Feng, Y.F.; Wang, F. Prevalence of NRAS mutation, PD-L1 expression and amplification, and overall survival analysis in 36 primary vaginal melanomas. Oncologist 2019, 25, e291–e301. [Google Scholar] [CrossRef] [Green Version]
- Tumeh, P.C.; Harview, C.L.; Yearley, J.H.; Shintaku, I.P.; Taylor, E.J.M.; Robert, L.; Chmielowski, B.; Spasic, M.; Henry, G.; Ciobanu, V.; et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 2014, 515, 568–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kluger, H.M.; Zito, C.R.; Turcu, G.; Baine, M.K.; Zhang, H.; Adeniran, A.; Sznol, M.; Rimm, D.L.; Kluger, Y.; Chen, L.; et al. PD-L1 Studies Across Tumor Types, its Differential Expression and Predictive Value in Patients Treated with Immune Checkpoint Inhibitors. Clin. Cancer Res. 2017, 23, 4270–4279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kakavand, H.; Rawson, R.V.; Pupo, G.M.; Yang, J.Y.H.; Menzies, A.M.; Carlino, M.S.; Kefford, R.F.; Howle, J.R.; Saw, R.P.; Thompson, J.F.; et al. PD-L1 expression and immune escape in melanoma resistance to MAPK inhibitors. Clin. Cancer Res. 2017, 23, 6054–6061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cancer Genome Atlas Network. Genomic Classification of Cutaneous Melanoma. Cell 2015, 161, 1681–1696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ionescu, C.A.; Aschie, M.; Matei, E.; Cozaru, G.C.; Deacu, M.; Mitroi, A.F.; Baltatescu, G.I.; Nicolau, A.A.; Mazilu, L.; Tuta, L.A.; et al. Characterization of the Tumor Microenvironment and the Biological Processes with a Role in Prostatic Tumorigenesis. Biomedicines 2022, 10, 1672. [Google Scholar] [CrossRef] [PubMed]
- Bosoteanu, C.; Bosoteanu, M.; Aschie, M. Differential diagnosis issues in a case of gastric carcinoma associated with leukemoid reaction. Rom. J. Morphol. Embryol. 2009, 50, 701–705. [Google Scholar]
- Goggins, W.B.; Finkelstein, D.M.; Tsao, H. Evidence for an association between cutaneous melanoma and non-Hodgkin lymphoma. Cancer 2001, 91, 874–880. [Google Scholar] [CrossRef] [PubMed]
- Matei, E.; Aschie, M.; Mitroi, A.F.; Ghinea, M.M.; Gheorghe, E.; Petcu, L.; Dobrin, N.; Chisoi, A.; Mihaela, M. Biomarkers involved in evaluation of platelets function in South-Eastern Romanian patients with hematological malignancies subtypes. Medicine 2021, 100, e25944. [Google Scholar] [CrossRef] [PubMed]
- Brinzan, C.; Așchie, M.; Matei, E.; Mitroi, A.F.; Cozaru, G.C. Molecular expression profiles of selected microRNAs in colorectal adenocarcinoma in patients from south-eastern part of Romania. Medicine 2019, 98, e18122. [Google Scholar] [CrossRef] [Green Version]
- Karydis, I.; Chan, P.Y.; Wheater, M.; Arriola, E.; Szlosarek, P.W.; Ottensmeier, C. Clinical activity and safety of Pembrolizumab in Ipilimumab pre-treated patients with uveal melanoma. Oncoimmunology 2016, 5, e1143997. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.-J.; Lim, H.J.; Choi, Y.H.; Chang, Y.H.; Lee, W.J.; Kim, D.W.; Yoon, G.S. The clinical significance of tumor infiltrating lymphocytes and microscopic satellites in acral melanoma in a Korean population. Ann. Dermatol. 2013, 25, 61–66. [Google Scholar] [CrossRef] [Green Version]
- Song, H.; Wu, Y.; Ren, G.; Guo, W.; Wang, L. Prognostic factors of oral mucosal melanoma: Histopathological analysis in a retrospective cohort of 82 cases. Histopathology 2015, 67, 548–556. [Google Scholar] [CrossRef]
- Kaunitz, G.J.; Cottrell, T.R.; Lilo, M.; Muthappan, V.; Esandrio, J.; Berry, S.; Xu, H.; Ogurtsova, A.; Anders, R.A.; Fischer, A.H.; et al. Melanoma subtypes demonstrate distinct PD-L1 expression profiles. Lab. Investig. 2017, 97, 1063–1071. [Google Scholar] [CrossRef] [Green Version]
- Elder, D.E.; Massi, D.; Scolyer, R.; Willemze, R. WHO Classification of Skin Tumours, 4th ed.; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Elder, D.E. Lever’s Histopathology of the Skin, 11th ed.; Wolters-Kluwer: Alphen aan den Rijn, The Netherlands, 2014; pp. 488–547. [Google Scholar]
- Calonje, E.; Brenn, T.; Lazar, A. McKee PH McKee’s Pathology of the Skin, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2012; pp. 1126–1267. [Google Scholar]
- Massi, D.; Brusa, D.; Merelli, B.; Ciano, M.; Audrito, V.; Serra, S.; Buonincontri, R.; Baroni, G.; Nassini, R.; Minocci, D.; et al. PD-L1 marks a subset of melanomas with a shorter overall survival and distinct genetic and morphological characteristics. Ann. Oncol. 2014, 25, 2433–2442. [Google Scholar] [CrossRef]
- Schramm, S.J.; Mann, G.J. Melanoma prognosis: A REMARK-based systematic review and bioinformatic analysis of immunohistochemical and gene microarray studies. Mol. Cancer Ther. 2011, 10, 1520–1528. [Google Scholar] [CrossRef] [Green Version]
- Nicolau, A.A.; Caraban, B.M.; Gheorghe, E.; Hangan, T.L.; Cojocaru, O.; Orasanu, C.I.; Voda, R.I. Proteomic Implications of Tumoral Infiltrating Lymphocytes in Melanoma: PD-L1, CD4 and CD8—Short Review. ARS Med. Tomitana 2020, 3, 117–121. [Google Scholar] [CrossRef]
- Taube, J.M.; Anders, R.A.; Young, G.D.; Xu, H.; Sharma, R.; McMiller, T.L.; Chen, S.; Klein, A.P.; Pardoll, D.M.; Topalian, S.L.; et al. Colocalization of inflammatory response with B7-H1 expression in human melanocytic lesions supports an adaptive resistance mechanism of immune escape. Sci. Transl. Med. 2012, 4, 127ra37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taube, J.M.; Klein, A.; Brahmer, J.R.; Xu, H.; Pan, X.; Kim, J.H.; Chen, L.; Pardoll, D.M.; Topalian, S.L.; Anders, R.A. Association of PD-1, PD-1 ligands, and other features of the tumor immune microenvironment with response to anti-PD-1 therapy. Clin. Cancer Res. 2014, 20, 5064–5074. [Google Scholar] [CrossRef] [Green Version]
- Ahmadzadeh, M.; Johnson, L.A.; Heemskerk, B.; Wunderlich, J.R.; Dudley, M.E.; White, D.E.; Rosenberg, S.A. Tumor antigen-specific CD8 T cells infiltrating the tumor express high levels of PD-1 and are functionally impaired. Blood 2009, 114, 1537–1544. [Google Scholar] [CrossRef] [PubMed]
- Mandala, M.; Merelli, B.; Massi, D. PD-L1 in melanoma: Facts and myths. Melanoma Manag. 2016, 3, 187–194. [Google Scholar] [CrossRef]
- Bønnelykke-Behrndtz, M.L.; Steiniche, T.; Damsgaard, T.E.; Georgsen, J.B.; Danielsen, A.; Bastholt, L.; Møller, H.J.; Nørgaard, P.H.; Schmidt, H. Melanoma negative spindle-cell associated melanoma, a distinct inflammatory phenotype correlated with dense infiltration of CD163 macrophages and loss of E-cadherin. Melanoma Res. 2015, 25, 113–118. [Google Scholar] [CrossRef]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 blockade in tumors with mismatch-repair deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef] [Green Version]
- Robert, C.; Ribas, A.; Wolchok, J.D.; Hodi, F.S.; Hamid, O.; Kefford, R.; Weber, J.S.; Joshua, A.M.; Hwu, W.-J.; Gangadhar, T.C.; et al. Anti-programmed-death-receptor 1 treatment with pembrolizumab in ipilimumab-refractory advanced melanoma: A randomised dose-comparison cohort of a phase 1 trial. Lancet 2014, 384, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Dermani, F.K.; Samadi, P.; Rahmani, G.; Kohlan, A.K.; Najafi, R. PD-1/PD-L1 immune checkpoint: Potential target for cancer therapy. J. Cell Physiol. 2019, 234, 1313–1325. [Google Scholar] [CrossRef]
- Zou, W.P.; Wolchok, J.D.; Chen, L.P. PD-L1 (B7-H1) and PD-1 pathway blockade for cancer therapy: Mechanisms, response biomarkers, and combinations. Sci. Transl. Med. 2016, 8, 328. [Google Scholar] [CrossRef] [Green Version]
- Clark, C.A.; Gupta, H.B.; Sareddy, G.; Pandeswara, S.; Lao, S.; Yuan, B.; Drerup, J.M.; Padron, A.; Conejo-Garcia, J.; Murthy, K.; et al. Tumor-intrinsic PD-L1 signals regulate cell growth, pathogenesis, and autophagy in ovarian cancer and melanoma. Cancer Res. 2016, 76, 6964–6974. [Google Scholar] [CrossRef] [Green Version]
- Jilaveanu, L.B.; Shuch, B.; Zito, C.R.; Parisi, F.; Barr, M.; Kluger, Y.; Chen, L.; Kluger, H.M. PD-L1 expression in clear cell renal cell carcinoma: An analysis of nephrectomy and sites of metastases. J Cancer 2014, 5, 166–172. [Google Scholar] [CrossRef] [Green Version]
- Schalper, K.A.; Velcheti, V.; Carvajal, D.; Wimberly, H.; Brown, J.; Pusztai, L.; Rimm, D.L. In situ tumor PD-L1 mRNA expression is associated with increased TILs and better outcome in breast carcinomas. Clin. Cancer Res. 2014, 20, 2773–2782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velcheti, V.; Schalper, K.A.; Carvajal, D.E.; Anagnostou, V.K.; Syrigos, K.N.; Sznol, M.; Herbst, R.S.; Gettinger, S.N.; Chen, L.; Rimm, D.L. Programmed death ligand-1 expression in non-small cell lung cancer. Lab. Investig. 2014, 94, 107–116. [Google Scholar] [CrossRef] [Green Version]
- Topalian, S.L.; Sznol, M.; McDermott, D.F.; Kluger, H.M.; Carvajal, R.D.; Sharfman, W.H.; Brahmer, J.R.; Lawrence, D.P.; Atkins, M.B.; Powderly, J.D.; et al. Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J. Clin. Oncol. 2014, 32, 1020–1030. [Google Scholar] [CrossRef] [PubMed]
- Ribas, A.; Puzanov, I.; Dummer, R.; Schadendorf, D.; Hamid, O.; Robert, C.; Hodi, F.S.; Schachter, J.; Pavlick, A.C.; Lewis, K.D.; et al. Pembrolizumab versus investigator-choice chemotherapy for ipilimumab-refractory melanoma (KEYNOTE-002): A randomised, controlled, phase 2 trial. Lancet Oncol. 2015, 16, 908–918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Topalian, S.L.; Drake, C.G.; Pardoll, D.M. Immune checkpoint blockade: A common denominator approach to cancer therapy. Cancer Cell 2015, 27, 450–461. [Google Scholar] [CrossRef] [Green Version]
- Kwong, F.N.K.; Laggner, U.; McKinney, O.; Croud, J.; Rice, A.; Nicholson, A.G. Expression of PD-L1 correlates with pleomorphic morphology and histological patterns of non-small-cell lung carcinomas. Histopathology 2018, 72, 1024–1032. [Google Scholar] [CrossRef]
- Ghebeh, H.; Mohammed, S.; Al-Omair, A.; Qattant, A.; Lehe, C.; Al-Qudaihi, G.; Elkum, N.; Alshabanah, M.; Bin Amer, S.; Tulbah, A.; et al. The B7-H1 (PD-L1) T lymphocyte-inhibitory molecule is expressed in breast cancer patients with infiltrating ductal carcinoma: Correlation with important high-risk prognostic factors. Neoplasia 2006, 8, 190–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hino, R.; Kabashima, K.; Kato, Y.; Yagi, H.; Nakamura, M.; Honjo, T.; Okazaki, T.; Tokura, Y. Tumor cell expression of programmed cell death-1 ligand 1 is a prognostic factor for malignant melanoma. Cancer 2010, 116, 1757–1766. [Google Scholar] [CrossRef] [PubMed]
- Krönig, H.; Falchner, K.J.; Odendahl, M.; Brackertz, B.; Conrad, H.; Muck, D.; Hein, R.; Blank, C.; Peschel, C.; Haller, B.; et al. PD-1 expression on Melan-A-reactive T cells increases during progression to metastatic disease. Int. J. Cancer 2012, 130, 2327–2336. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, N.; Dieterich, L.C. Mechanisms and Clinical Significance of Tumor Lymphatic Invasion. Cells 2021, 10, 2585. [Google Scholar] [CrossRef] [PubMed]
- Brinzan, C.; Așchie, M.; Grasa, C.N.; Mitroi, A.F.; Matei, E.; Cozaru, G.C. The Mutation Profiles of KRAS and BRAF Genes in a Romanian Colorectal Cancer Cohort. Rev. Chim. 2019, 70, 1346–1350. [Google Scholar] [CrossRef]
- Iacovelli, R.; Nole, F.; Verri, E.; Renne, G.; Paglino, C.; Santoni, M.; Rocca, M.C.; Giglione, P.; Aurilio, G.; Cullura, D.; et al. Prognostic role of PD-L1 expression in renal cell carcinoma. a systematic review and meta-analysis. Target. Oncol. 2016, 11, 143–148. [Google Scholar] [CrossRef]
- Pyo, J.S.; Kang, G.; Kim, J.Y. Prognostic role of PD-L1 in malignant solid tumors: A meta-analysis. Int. J. Biol. Markers 2017, 32, E68–E74. [Google Scholar] [CrossRef]
- Zhao, S.; Zhang, M.H.; Zhang, Y.; Meng, H.X.; Wang, Y.; Liu, Y.P.; Jing, J.; Huang, L.; Sun, M.Q.; Zhang, Y.; et al. The prognostic value of programmed cell death ligand 1 expression in non-Hodgkin lymphoma: A meta-analysis. Cancer Biol. Med. 2018, 15, 290–298. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nb. | Clinico- Pathological Aspects | PD-L1 Expression in TILs | X2 Score | p-Value | PD-L1 Expression in MTCs | X2 Score | p-Value | ||
|---|---|---|---|---|---|---|---|---|---|
| Negative n (%) | Positive n (%) | Negative n (%) | Positive n (%) | ||||||
| 1. | Age <65 years >65 years | 8 (33.33%) 16 (66.67%) | 20 (54.05%) 17 (54.95%) | 2.517 | 0.126 | 17 (51.52%) 16 (48.48%) | 11 (39.29%) 17 (60.71%) | 0.912 | 0.243 |
| 2. | Gender Males Females | 9 (37.50%) 15 (62.50%) | 22 (59.46%) 15 (40.54%) | 2.809 | 0.120 | 15 (45.45%) 18 (54.55%) | 16 (57.14%) 12 (42.86%) | 0.828 | 0.444 |
| 3. | Localization Acral Upper body Cervico-cranial Limbs | 3 (12.5%) 7 (29.17%) 9 (37.5% 5 (20.83%) | 2 (5.41%) 19 (51.35%) 3 (8.11%) 13 (35.14%) | 9.603 * | 0.018 | 3 (9.1%) 11 (33.33%) 7 (21.2%) 12 (36.36%) | 2 (7.1%) 15 (53.62%) 5 (17.86%) 6 (21.43%) | 2.791 | 0.443 |
| 4. | Clark level of invasion I II III IV V | 6 (25%) 2 (8.33%) 4(16.67%) 11(45.83%) 1(4.17%) | 3 (8.11%) 4 (10.81%) 6(16.22%) 21 (56.76%) 3 (8.11%) | 3.584 | 0.494 | 7 (21.22%) 1 (3.03%) 3 (9.09%) 19 (57.58%) 3 (9.09%) | 2(7.14%) 5 (17.86%) 7 (25.00%) 13 (46.43%) 1 (3.57%) | 8.819 | 0.068 |
| 5. | Breslow tumor thickness <1 mm 1–2 mm 2–4 mm >4 mm | 4 (16.67%) 0 (0%) 3 (12.50%) 17 (70.83%) | 2 (5.41%) 3 (8.11%) 12 (32.43%) 20 (54.05%) | 6.851 | 0.086 | 6 (18.18%) 0 (0%) 6 (18.18%) 21 (63.64%) | 0 (0%) 3 (10.71%) 9 (32.14%) 16 (57.14%) | 9.933 * | 0.014 |
| 6. | Lymphovascular invasion Present Absent | 10 (41.67%) 14(52.14%) | 24 (64.86%) 13(35.14%) | 3.175 | 0.113 | 16 (48.48%) 17 (51.52%) | 18 (64.29%) 10 (35.71%) | 1.533 | 0.216 |
| 7. | Perineural invasion Present Absent | 5 (20.83%) 19 (79.17%) | 9 (14.75%) 33 (89.19) | 1.163 | 0.298 | 5 (15.15%) 28 (84.85%) | 4 (14.29%) 24 (85.71%) | 0.009 | 0.926 |
| Nb. | Morphological Features | Infiltrating Immune Cells | X2 Score | p-Value | Melanoma Tumor Cells | X2 Score | p-Value | ||
|---|---|---|---|---|---|---|---|---|---|
| PD-L1 (-) n (%) | PD-L1 (+) n (%) | PD-L1 (-) n (%) | PD-L1 (+) n (%) | ||||||
| 1. | Morphologic type LMM SSM SSM with VGN NM | 2 (8.33%) 7 (29.17%) 6 (25%) 9 (37.50%) | 1 (2.70%) 14 (37.84%) 14 (37.84%) 8 (21.62%) | 3.305 | 0.332 | 3 (9.09%) 8 (24.24%) 13 (39.39%) 9 (27.27%) | 0 (0%) 13 (46.43%) 7 (25%) 8 (28.57%) | 5.678 | 0.144 |
| 2. | TILs evaluation Absent Brisk Non-brisk | 8 (33.33%) 3 (12.50%) 13 (54.17%) | 2 (5.41%) 8 (21.62%) 27 (72.97%) | 8.383 * | 0.020 | 7 (21.21%) 4 (12.12%) 22 (66.67%) | 3 (10.71%) 7 (25%) 18 (64.29%) | 2.425 | 0.287 |
| 3. | CD8 TIL’s Negative <5% 5–50% >50% | 9(37.50%) 1(4.17%) 14(58.33%) 0 (0.00%) | 2 (5.41%) 1 (2.70%) 32 (69.57%) 2 (5.41%) | 11.238 ** | 0.003 | 7 (21.21%) 0(0.00%) 25 (75.76%) 1 (50.00%) | 4 (14.29%) 2 (7.14%) 21 (75.00%) 1 (50.00%) | 2.775 | 0.514 |
| 4. | CD4 TIL’s Negative <5% 5–50% >50 | 6 (25.00%) 1 (4.17%) 17 (70.83%) 0 (0.00%) | 0 (0.00%) 0 (0.00%) 36 (97.30%) 1 (2.70%) | 12.614 ** | 0.001 | 3 (9.09%) 0 (0.00%) 29 (87.88%) 1 (3.03%) | 3 (10.71%) 1 (3.57%) 24 (85.71%) 0 (0.00%) | 2.076 | 0.906 |
| Nb. | Biomarkers | AUC | 95% CI * | p-Value | Youden J Index | Cut-Off Value | Sensitivity | Specificity |
|---|---|---|---|---|---|---|---|---|
| 1. | PD-L1 TILs | 0.959 | 0.875 to 0.993 | <0.001 | 0.889 | >3 | 97.30 | 91.67 |
| 2. | PD-L1 M | 0.975 | 0.898 to 0.998 | <0.001 | 0.934 | >0 | 96.43 | 96.97 |
| 3. | CD4 M | 0.950 | 0.862 to 0.989 | <0.001 | 0.743 | >15 | 84.31 | 90.00 |
| 4. | CD8 M | 0.941 | 0.850 to 0.985 | <0.001 | 0.758 | >10 | 89.13 | 86.67 |
| Nb. | Clinical Variables | Multivariate Analysis | ||
|---|---|---|---|---|
| Melanoma Tumor Microenvironment Cells | ||||
| Hazard Ratio | p-Value | 95% CI * | ||
| 1. | Lymphovascular invasion | 3.049 | 0.528 | 0.095−97.914 |
| 2. | Perineural invasion | 0.026 * | 0.023 | 0.001−0.607 |
| 3. | PD-L1 | 2.700 | 0.455 | 0.198−36.683 |
| 4. | CD4 TILs | 11.838 * | 0.023 | 1.386−101.108 |
| 5. | CD8 TILs | 7.748 * | 0.018 | 1.408−42.622 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caraban, B.M.; Matei, E.; Cozaru, G.C.; Aşchie, M.; Deacu, M.; Enciu, M.; Bălţătescu, G.I.; Chisoi, A.; Dobrin, N.; Petcu, L.; et al. PD-L1, CD4+, and CD8+ Tumor-Infiltrating Lymphocytes (TILs) Expression Profiles in Melanoma Tumor Microenvironment Cells. J. Pers. Med. 2023, 13, 221. https://doi.org/10.3390/jpm13020221
Caraban BM, Matei E, Cozaru GC, Aşchie M, Deacu M, Enciu M, Bălţătescu GI, Chisoi A, Dobrin N, Petcu L, et al. PD-L1, CD4+, and CD8+ Tumor-Infiltrating Lymphocytes (TILs) Expression Profiles in Melanoma Tumor Microenvironment Cells. Journal of Personalized Medicine. 2023; 13(2):221. https://doi.org/10.3390/jpm13020221
Chicago/Turabian StyleCaraban, Bogdan Marian, Elena Matei, Georgeta Camelia Cozaru, Mariana Aşchie, Mariana Deacu, Manuela Enciu, Gabriela Izabela Bălţătescu, Anca Chisoi, Nicolae Dobrin, Lucian Petcu, and et al. 2023. "PD-L1, CD4+, and CD8+ Tumor-Infiltrating Lymphocytes (TILs) Expression Profiles in Melanoma Tumor Microenvironment Cells" Journal of Personalized Medicine 13, no. 2: 221. https://doi.org/10.3390/jpm13020221