


Correlation Studies between S100 Protein Level and Soluble MIA or Tissue MelanA and gp100 (HMB45) Expression in Cutaneous Melanoma
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Group of Patients
2.2. Blood Sampling and Methods
2.3. Tissue Sampling and Staining
2.4. Statistical Analysis
3. Results
3.1. Soluble Levels of S100B and MIA Expression in Melanoma Patients
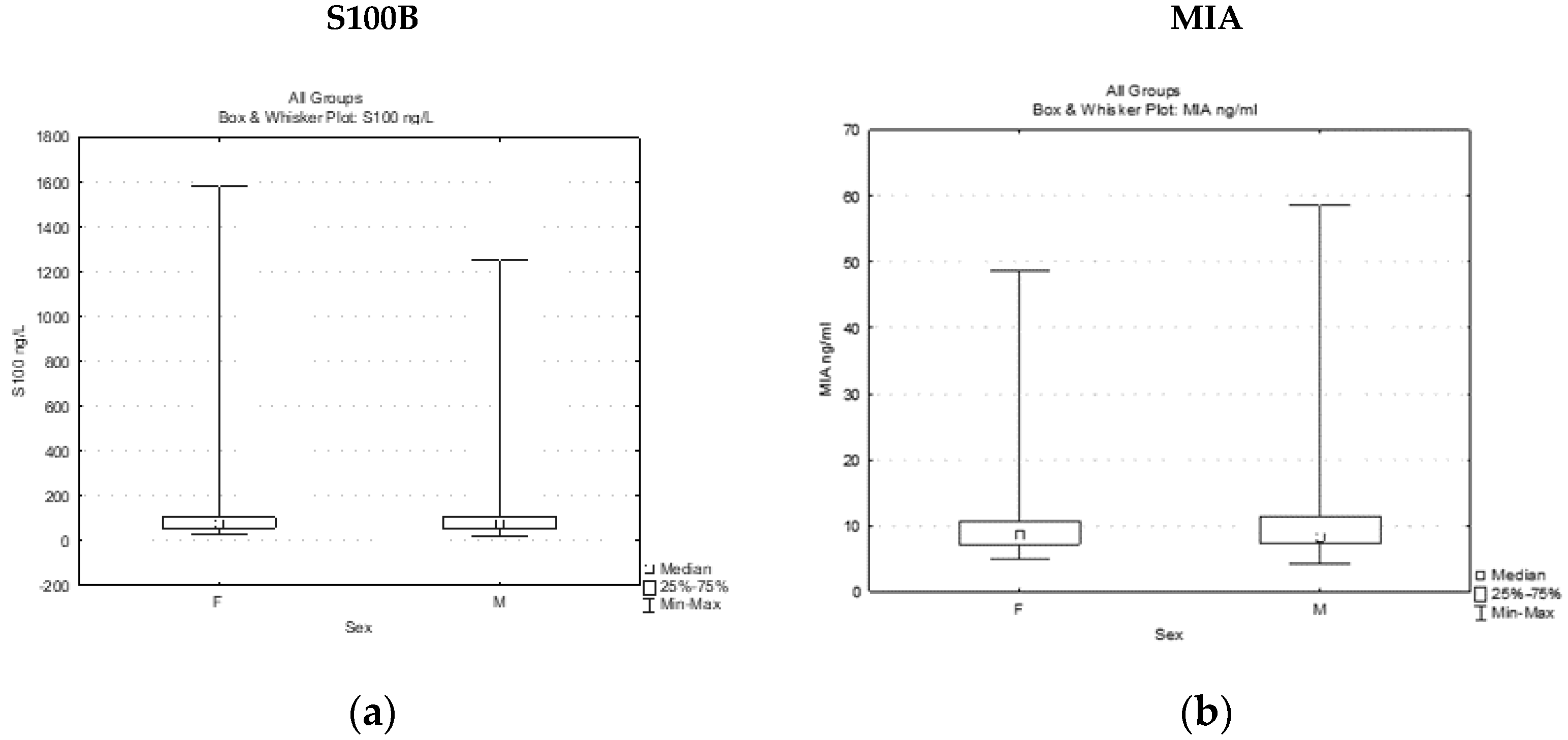
3.1.1. Circulating Levels of S100B and MIA in Melanoma Patients
3.1.2. Circulating Levels of S100B and MIA Depending on the Stage of the Disease
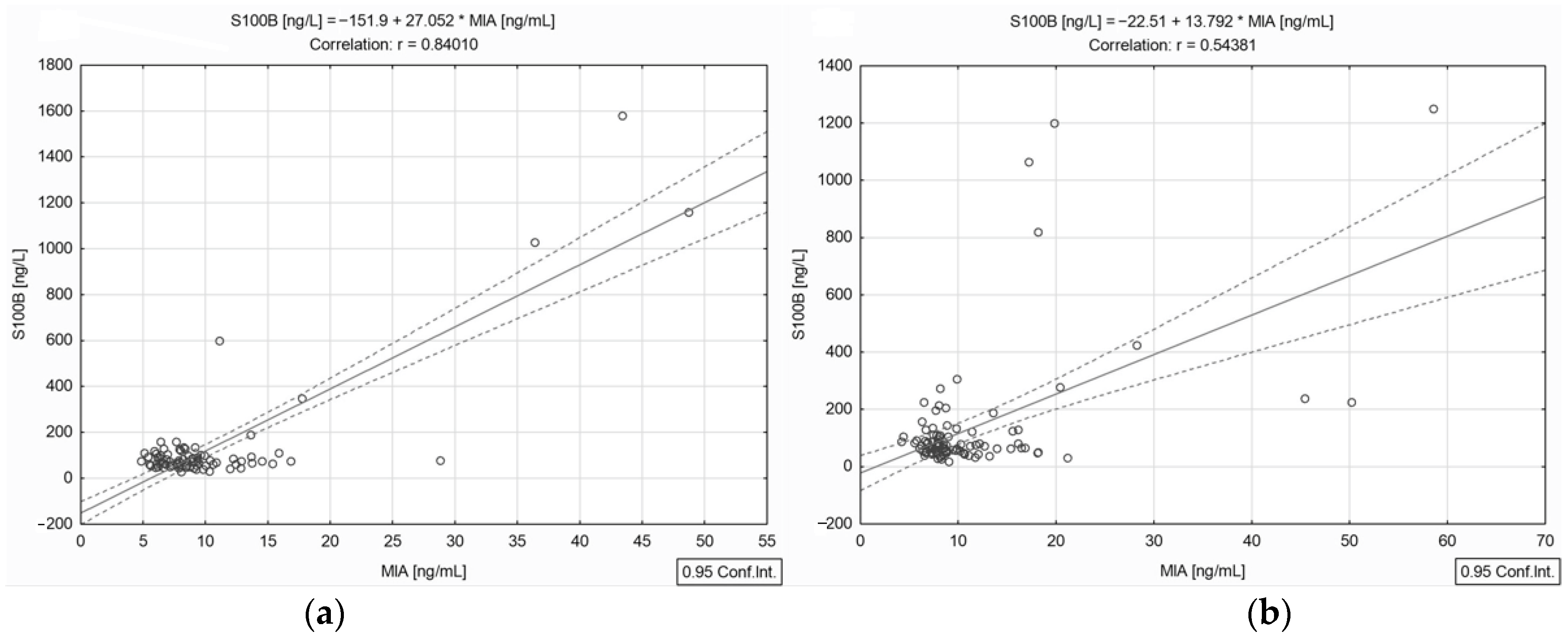
3.1.3. Correlation Analysis between Circulating S100B and MIA Levels
3.1.4. Correlation between Circulating S100B and MIA Levels in Distinct Stages of the Disease
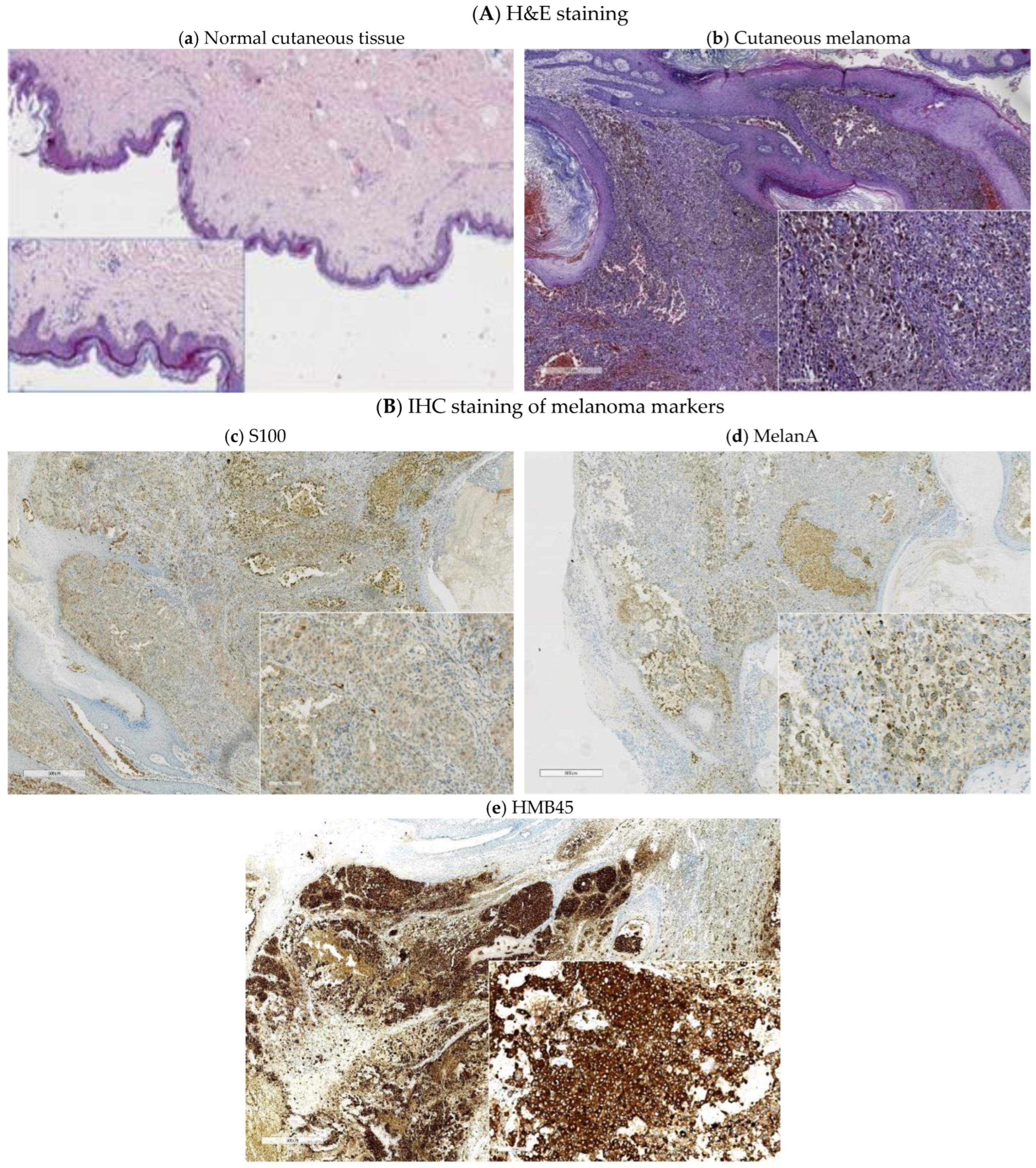
3.2. Tissue Expression of Melanoma Markers
3.2.1. Immunohistochemical Analysis (IHC) of Melanoma Lesions
3.2.2. Correlation Analysis between Tissue Expressions of Melanoma Markers
3.2.3. Soluble Expression of Melanoma Markers in Different Groups of IHC Tested Melanoma Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef] [PubMed]
- Gershenwald, J.E.; Scolyer, R.A. Melanoma Staging: American Joint Committee on Cancer (AJCC) 8th Edition and Beyond. Ann. Surg. Oncol. 2018, 25, 2105–2110. [Google Scholar] [CrossRef] [PubMed]
- Keung, E.Z.; Gershenwald, J.E. The eighth edition American Joint Committee on Cancer (AJCC) melanoma staging system: Implications for melanoma treatment and care. Expert Rev. Anticancer Ther. 2018, 18, 775–784. [Google Scholar] [CrossRef]
- Bomar, L.; Senithilnathan, A.; Ahn, C. Systemic therapies for advanced melanoma. Dermatol. Clin. 2019, 37, 409–423. [Google Scholar] [CrossRef] [PubMed]
- Belter, B.; Haase-Kohn, C.; Pietzsch, J. Biomarkers in malignant melanoma: Recent Trends and Critical Perspective. In Cutaneous Melanoma: Etiology and Therapy; Ward, W.H., Farma, J.M., Eds.; Codon Publications: Brisbane, Australia, 2017; pp. 39–56. [Google Scholar]
- Ma, Y.; Xia, R.; Ma, X.; Judson-Torres, R.L.; Zeng, H. Mucosal Melanoma: Pathological Evolution, Pathway Dependency and Targeted Therapy. Front. Oncol. 2021, 11, e702287. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, X.T.S.; Watson, I.R. Melanomics: Comprehensive Molecular Analysis of Normal and Neoplastic Melanocytes. In Melanoma; Fisher, D.E., Bastian, B.C., Eds.; Springer: New York, NY, USA, 2019; pp. 181–224. [Google Scholar]
- Deacon, D.C.; Smith, E.A.; Judson-Torres, R.L. Molecular biomarkers for melanoma screening, diagnosis and prognosis: Current state and future prospects. Front. Med. 2021, 8, e642380. [Google Scholar] [CrossRef]
- Ding, L.; Gosh, A.; Lee, D.J.; Emri, G.; Huss, W.J.; Bogner, P.N.; Paragh, G. Prognostic biomarkers of cutaneous melanoma. Photodermatol. Photoimmunol. Photomed. 2022, 38, 418–434. [Google Scholar] [CrossRef]
- Georgescu, S.R.; Mitran, C.I.; Mitran, M.I.; Matei, C.; Constantin, C.; Neagu, M.; Tampa, M. Apprising diagnostic and prognostic biomarkers in cutaneous melanoma—Persistent updating. J. Pers. Med. 2022, 12, 1506. [Google Scholar] [CrossRef]
- Wagstaff, W.; Mwamba, R.N.; Grullon, K.; Armstrong, M.; Zhao, P.; Hendren-Santiago, B.; Qin, K.H.; Li, A.J.; Hu, D.A.; Youssef, A.; et al. Melanoma: Molecular genetics, metastasis, targeted therapies, immunotherapies, and therapeutic resistance. Genes Dis. 2022, 9, 1608–1623. [Google Scholar] [CrossRef]
- Hessler, M.; Jalilian, E.; Xu, Q.; Reddy, S.; Horton, L.; Elkin, K.; Manwar, R.; Tsoukas, M.; Mehregan, D.; Avanaki, K. Melanoma biomarkers and their potential application for in vivo diagnostic imaging modalities. Int. J. Mol. Sci. 2020, 21, 9583. [Google Scholar] [CrossRef]
- Hyams, D.M.; Cook, R.W.; Buzaid, A.C. Identification of risk in cutaneous melanoma patients: Prognostic and predictive markers. J. Surg. Oncol. 2019, 119, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Revythis, A.; Shah, S.; Kutka, M.; Moschetta, M.; Ozturk, M.A.; Pappas-Gogos, G.; Ioannidou, E.; Sheriff, M.; Rassy, E.; Boussios, S. Unraveling the Wide Spectrum of Melanoma Biomarkers. Diagnostics 2021, 11, 1341. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Ali, S.A. Multifunctional Role of S100 Protein Family in the Immune System: An Update. Cells 2022, 11, 2274. [Google Scholar] [CrossRef] [PubMed]
- Bresnick, A.R.; Weber, D.J.; Zimmer, D.B. S100 proteins in cancer. Nat. Rev. Cancer 2015, 15, 96–109. [Google Scholar] [CrossRef] [PubMed]
- Salzmann, M.; Enk, A.H.; Hassel, J.C. S100 as Serum Tumor Marker in Advanced Uveal Melanoma. Biomolecules 2023, 13, 529. [Google Scholar] [CrossRef] [PubMed]
- Michielin, O.J.; van Akkooi, A.C.J.; Ascierto, P.A.; Dummer, R.; Keilholz, U. Cutaneous melanoma: ESMO Clinical Practice, Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 1884–1901. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, D.; Leininger, J.; Hamby, C.; Safai, B. Diagnostic and prognostic biomarkers in melanoma. J. Clin. Aesthetic Dermatol. 2014, 7, 13–24. [Google Scholar]
- Ohsie, S.J.; Sarantopoulos, G.P.; Cochran, A.J.; Binder, S.W. Immunohistochemical characteristics of melanoma. J. Cutan. Pathol. 2008, 35, 433–444. [Google Scholar] [CrossRef]
- Xiong, T.F.; Pan, F.Q.; Li, D. Expression and clinical significance of S100 family genes in patients with melanoma. Melanoma Res. 2019, 29, 23–29. [Google Scholar] [CrossRef]
- Janka, E.A.; Várvölgyi, T.; Sipos, Z.; Soós, A.; Hegyi, P.; Kiss, S.; Dembrovszky, F.; Csupor, D.; Kéringer, P.; Pécsi, D.; et al. Predictive performance of serum S100B versus LDH in melanoma patients: A systematic review and meta-analysis. Front. Oncol. 2021, 11, e772165. [Google Scholar] [CrossRef]
- Ricci, C.; Dika, E.; Ambrosi, F.; Lambertini, M.; Veronesi, G.; Barbara, C. Cutaneous Melanomas: A Single Center Experience on the Usage of Immunohistochemistry Applied for the Diagnosis. Int. J. Mol. Sci. 2022, 23, 5911. [Google Scholar] [CrossRef] [PubMed]
- Davis, L.E.; Shalin, S.C.; Tackett, A.J. Current state of melanoma diagnosis and treatment. Cancer Biol. Ther. 2019, 20, 1366–1379. [Google Scholar] [CrossRef] [PubMed]
- Harvey, N.T.; Wood, B.A. A Practical Approach to the Diagnosis of Melanocytic Lesions. Arch. Pathol. Lab. Med. 2019, 143, 789–810. [Google Scholar] [CrossRef] [PubMed]
- Elder, D.E.; Bastian, B.C.; Cree, I.A. The 2018 World Health Organization Classification of Cutaneous, Mucosal, and Uveal Melanoma Detailed Analysis of 9 Distinct Subtypes Defined by Their Evolutionary Pathway. Arch. Pathol. Lab. Med. 2020, 144, 500–522. [Google Scholar] [CrossRef] [PubMed]
- Jing, X.; Michael, C.W.; Theoharis, C.G. The use of immunocytochemical study in the cytologic diagnosis of melanoma: Evaluation of three antibodies. Diagn. Cytopathol. 2013, 41, 126–130. [Google Scholar] [CrossRef]
- Berset, M.; Cerottini, J.P.; Guggisberg, D.; Romero, P.; Burri, F.; Rimoldi, D.; Panizzon, R.G. Expression of melan-a/MART-1 antigen as a prognostic factor in primary cutaneous melanoma. Int. J. Cancer 2001, 95, 73–77. [Google Scholar] [CrossRef]
- Lam, G.T.; Prabhakaran, S.; Sorvina, A.; Martini, C.; Ung, B.S.Y.; Karageorgos, L.; Hickey, S.M.; Lazniewska, J.; Johnson, I.R.D.; Williams, D.B.; et al. Pitfalls in Cutaneous Melanoma Diagnosis and the Need for New Reliable Markers. Mol. Diagn. Ther. 2023, 27, 49–60. [Google Scholar] [CrossRef]
- Saliba, E.; Bhawan, J. Aberrant Expression of Immunohistochemical Markers in Malignant Melanoma: A Review Aberrant Expression of Immunohistochemical Markers in Malignant Melanoma: A Review. Dermatopathology 2021, 8, 359–370. [Google Scholar] [CrossRef]
- Bosserhoff, A.K.; Kaufmann, M.; Kaluza, B.; Bartke, I.; Zirngibl, H.; Hein, R.; Stolz, W.; Buettner, R. Melanoma-inhibiting Activity, a Novel Serum Marker for Progression of Malignant Melanoma. Cancer Res. 1997, 57, 3149–3153. [Google Scholar]
- Fan, S.; Liu, X.; Wu, Y.; Li, K.; Zhao, X.; Lin, W.; Liu, J. Prognostic Value of Lactate Dehydrogenase, Melanoma Inhibitory Protein, and S-100B Protein in Patients with Malignant Melanoma. Evid. Based Complement. Alternat. Med. 2022, 2022, 9086540. [Google Scholar] [CrossRef]
- Riechers, A.; Bosserhoff, A.K. Melanoma inhibitory activity in melanoma diagnostics and therapy—A small protein is looming large. Exp. Dermatol. 2014, 23, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Sasahira, T.; Kirita, T.; Nishiguchi, Y.; Kurihara, M.; Nakashima, C.; Bosserhoff, A.K.; Kuniyasu, H. A comprehensive expression analysis of the MIA gene family in malignancies: MIA gene family members are novel, useful markers of esophageal, lung, and cervical squamous cell carcinoma. Oncotarget 2016, 7, 31137–31152. [Google Scholar] [CrossRef] [PubMed]
- Muller-Ladner, U.; Bosserhoff, A.K.; Dreher, K.; Hein, R.; Neidhart, M.; Gay, S.; Scholmerich, J.; Buettner, R.; Lang, B. MIA (melanoma inhibitory activity): A potential serum marker for rheumatoid arthritis. Rheumatology 1999, 38, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Sandru, A.; Panaitescu, E.; Voinea, S.; Bolovan, M.; Stanciu, A.; Cinca, S.; Blidaru, A. Prognostic value of melanoma inhibitory activity protein in localized cutaneous malignant melanoma. J. Skin Cancer 2014, 2014, 843214. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. Ca Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Garbe, C.; Amaral, T.; Peris, K.; Hauschild, A.; Arenberger, P.; Basset-Seguin, N.; Bastholt, L.; Bataille, V.; Del Marmol, V.; Dréno, B.; et al. European Dermatology Forum (EDF), the European Association of Dermato-Oncology (EADO), and the European Organization for Research and Treatment of Cancer (EORTC). European consensus-based interdisciplinary guideline for melanoma. Part 1: Diagnostics: Update 2022. Eur. J. Cancer 2022, 170, 236–255. [Google Scholar]
- Vucetić, B.; Rogan, S.A.; Hrabac, P.; Hudorović, N.; Cupić, H.; Lukinac, L.; Ledinsky, M.; Matejcić, A.; Lovricević, I.; Zekan, M. Biological value of melanoma inhibitory activity serum concentration in patients with primary skin melanoma. Melanoma Res. 2008, 18, 201–207. [Google Scholar] [CrossRef]
- Uslu, U.; Schliep, S.; Schliep, K.; Erdmann, M.; Koch, H.; Parsch, H.; Rosenheinrich, S.; Anzengruber, D.; Bosserhoff, A.K.; Schuler, G.; et al. Comparison of the Serum Tumor Markers S100 and Melanoma-inhibitory Activity (MIA) in the Monitoring of Patients with Metastatic Melanoma Receiving Vaccination Immunotherapy with Dendritic Cells. Anticancer Res. 2017, 37, 5033–5037. [Google Scholar]
- Allgöwer, C.; Kretz, A.L.; von Karstedt, S.; Wittau, M.; Henne-Bruns, D.; Lemke, J. Friend or Foe: S100 Proteins in Cancer. Cancers 2020, 12, 2037. [Google Scholar] [CrossRef]
- Voinea, S.; Sandru, A.; Gherghe, M. Pitfalls in cutaneous melanoma lymphatic drainage. Chirurgia 2016, 111, 87–89. [Google Scholar]
- Voinea, S.; Sandru, A.; Gherghe, M.; Blidaru, A. Peculiarities of lymphatic drainage in cutaneous malignant melanoma: Clinical experience in 75 cases. Chirurgia 2014, 109, 26–33. [Google Scholar] [PubMed]
- Fayne, R.A.; Macedo, F.I.; Rodgers, S.E.; Möller, M.G. Evolving management of positive regional lymph nodes in melanoma: Past, present and future directions. Oncol. Rev. 2019, 13, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Xu, C.; Jin, Q.; Liu, Z. S100 protein family in human cancer. Am. J. Cancer Res. 2014, 4, 89–115. [Google Scholar] [PubMed]
- Yen, M.C.; Huang, Y.C.; Kan, J.Y.; Kuo, P.L.; Hou, M.F.; Hsu, Y.L. S100B expression in breast cancer as a predictive marker for cancer metastasis. Int. J. Oncol. 2018, 52, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Song, J.; Wang, V.; Kan, J.; Ge, Y.; Wang, D.; Zhang, R.; Zhang, W.; Liu, Y. A Novel S100 Family-Based Signature Associated with Prognosis and Immune Microenvironment in Glioma. J. Oncol. 2021, 2021, 3586589. [Google Scholar] [CrossRef]
- Donato, R.; Sorci, G.; Riuzzi, F.; Arcuri, C.; Bianchi, R.; Brozzi, F.; Tubaro, C.; Giambanco, I. S100B’s double life: Intracellular regulator and extracellular signal. Biochim. Biophys. Acta 2009, 1793, 1008–1030. [Google Scholar] [CrossRef]
- Donato, R.; Cannon, B.R.; Sorci, G.; Riuzzi, F.; Hsu, K.; Weber, D.J.; Geczy, C.L. Functions of S100 proteins. Curr. Mol. Med. 2013, 13, 24–57. [Google Scholar] [CrossRef]
- Díaz-Lagares, A.; Alegre, E.; Arroyo, A.; González-Cao, M.; Zudaire, M.E.; Viteri, S.; Martín-Algarra, S.; González, A. Evaluation of multiple serum markers in advanced melanoma. Tumor Biol. 2011, 32, 1155–1161. [Google Scholar] [CrossRef]
- Gonzalez, L.L.; Garrie, K.; Turner, M.D. Role of S100 proteins in health and disease. Biochim. Biophys. Acta Mol. Cell Res. 2020, 1867, e118677. [Google Scholar] [CrossRef]
- Lugowska, I.; Kowalska, M.; Fuksiewicz, M.; Kotowicz, B.; Mierzejewska, E.; Koseła-Paterczyk, H.; Szamotulska, K.; Rutkowski, P. Serum markers in early-stage and locally advanced melanoma. Tumor Biol. 2015, 36, 8277–8285. [Google Scholar] [CrossRef]
- Napoli, S.; Scuderi, C.; Gattuso, G.; Di Bella, V.; Candido, S.; Basile, M.S.; Libra, M.; Falzone, L. Functional roles of matrix metalloproteinases and their inhibitors in melanoma. Cells 2020, 9, 1151. [Google Scholar] [CrossRef] [PubMed]
- Viray, H.; Bradley, W.R.; Schalper, K.A.; Rimm, D.L.; Gould Rothberg, B.E. Marginal and joint distributions of S100, HMB-45 and Melan-A across a large series of cutaneous melanomas. Arch. Pathol. Lab. Med. 2013, 137, 1063–1073. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | Female | Male | Melanoma Group |
|---|---|---|---|
| Number of patients | 78 | 98 | 176 |
| S100B ng/L (mean ± SD) | 132.92 ± 241.86 | 131.33 ± 210.81 | 132.04 ± 224.43 |
| Minimum | 25.53 | 15.61 | 15.61 |
| Maximum | 1580.32 | 1250 | 1580.32 |
| MIA ng/mL (mean ± SD) | 10.61 ± 7.46 | 11.09 ± 8.37 | 10.88 ± 7.968 |
| Minimum | 4.89 | 4.20 | 4.20 |
| Maximum | 48.74 | 58.61 | 58.61 |
| No. of Patients | Mean ± SD | Minimum | Maximum | |
|---|---|---|---|---|
| S100B (cut-off 90 ng/L) | ||||
| Stage I | 27 | 67.44 ± 21.71 | 31.33 | 128.60 |
| Stage II | 53 | 66.43 ± 23.20 | 15.61 | 132.30 |
| Stage III | 74 | 135.71 ± 186.10 | 25.53 | 1157.00 |
| Stage IV | 22 | 357.00 ± 477.65 | 47.55 | 1580.32 |
| MIA (cut-off 9.4 ng/mL) | ||||
| Stage I | 27 | 8.61 ± 2.55 | 5.59 | 16.49 |
| Stage II | 53 | 8.92 ± 3.73 | 4.20 | 28.85 |
| Stage III | 74 | 11.23 ± 8.07 | 4.42 | 50.21 |
| Stage IV | 22 | 17.19 ± 14.19 | 5.11 | 58.61 |
| No | Clinico-Pathogical Characteristics | S100+ n (%) | HMB45+ n (%) | MelanA+ n (%) | S100+/HMB45+ n (%) | S100+/MelanA+ n (%) | HMB45+/MelanA+ n (%) | S100+/HMB45+/ MelanA+ n (%) |
|---|---|---|---|---|---|---|---|---|
| 1 | Number of patients (n) | 51 | 61 | 65 | 37 | 42 | 55 | 33 |
| 2 | Age | |||||||
| <65 years | 32 (62.75%) | 34 (55.74%) | 39 (60%) | 21 (56.75%) | 25 (59.53%) | 32 (58.18%) | 19 (57.57%) | |
| >65 years | 19 (37.25%) | 27 (44.26%) | 26 (40%) | 16 (43.25%) | 17 (40.47%) | 23 (41.82%) | 14 (42.43%) | |
| 3 | Sex | |||||||
| Males | 24 (47.05%) | 33 (54.09%) | 33 (50.77%) | 20 (54.05%) | 20 (47.62%) | 29 (52.73%) | 16 (48.48%) | |
| Females | 27 (52.95%) | 28 (45.91%) | 32 (49.23%) | 17 (45.95%) | 22 (52.38%) | 26 (47.27%) | 17 (51.52%) | |
| 4 | Localization | |||||||
| Chest | 29 (56.87%) | 32 (52.45%) | 32 (49.23%) | 22 (59.46%) | 23 (54.77%) | 30 (54.54%) | 21 (63.64%) | |
| Inferior limbs | 12 (23.52%) | 13 (21.31%) | 16 (24.61%) | 7 (18.92%) | 10 (23.81%) | 10 (18.18%) | 5 (15.15%) | |
| Superior limbs | 7 (13.72%) | 9 (14.75%) | 10 (15.38%) | 5 (13.51%) | 6 (14.28%) | 8 (14.55%) | 4 (12.12%) | |
| Head and neck | 2 (3.93%) | 4 (6.55%) | 4 (6.16%) | 2 (5.40%) | 2 (4.76%) | 4 (7.28%) | 2 (6.06%) | |
| Hips | 1 (1.96%) | 3 (4.91%) | 3 (4.62%) | 1 (2.71%) | 1 (2.38%) | 3 (5.45%) | 1 (3.03%) | |
| 5 | Histological subtype | |||||||
| Superficial spreading | 38 (74.50%) | 45 (73.77%) | 48 (73.84%) | 25 (67.56%) | 29 (69.04%) | 39 (70.90%) | 16 (48.49%) | |
| Nodular | 12 (23.53%) | 14 (22.95%) | 14 (21.54%) | 12 (32.44%) | 12 (28.57%) | 14 (25.46%) | 14 (42.42%) | |
| Acral | 1 (1.97%) | 1 (1.64%) | 2 (3.08%) | - | 1 (2.39%) | 1 (1.82%) | 2 (6.06%) | |
| Lentigo | - | 1 (1.64%) | 1 (1.54%) | - | - | 1 (1.82%) | 1 (3.03%) | |
| 6 | Breslow thickness | |||||||
| <1 mm | 10 (19.61%) | 8 (13.11%) | 7 (10.77%) | 4 (10.81%) | 4 (9.52%) | 5 (9.09%) | 2 (6.06%) | |
| 1–2 mm | 8 (15.69%) | 17 (27.87%) | 18 (27.69%) | 7 (18.91%) | 11 (26.19%) | 14 (25.46%) | 4 (12.12%) | |
| 2–4 mm | 15 (29.41%) | 23 (37.70%) | 26 (40%) | 18 (48.65%) | 15 (35.71%) | 24 (43.63%) | 17 (51.52%) | |
| >4 mm | 18 (35.29%) | 13 (21.32%) | 14 (21.44%) | 8 (21.63%) | 12 (28.58%) | 12 (21.8%) | 10 (30.30%) | |
| 7 | Stage | |||||||
| I | 12 (23.53%) | 14 (22.95%) | 15 (23.08%) | 8 (21.62%) | 10 (23.80%) | 12 (21.82%) | 7 (21.21%) | |
| II | 26 (50.98%) | 29 (47.54%) | 30 (46.15%) | 19 (51.35%) | 20 (47.62%) | 27 (49.09%) | 17 (51.52%) | |
| III | 12 (23.53%) | 16 (26.23%) | 18 (27.69%) | 9 (24.32%) | 11 (26.19%) | 15 (27.27%) | 9 (27.27%) | |
| IV | 1(1.96%) | 2 (3.28%) | 2 (3.08%) | 1 (2.71%) | 1 (2.39%) | 1 (1.82%) | - | |
| 8 | Tissue expression | |||||||
| Positive | 48 (94.12%) | 52 (85.25%) | 56 (86.15%) | - | - | - | - | |
| Negative | 3 (5.88%) | 9 (14.75%) | 9 (13.85%) | - | - | - | - | |
| +/+ | - | - | - | 32 (86.48%) | 37 (88.09%) | 45 (81.82%) | - | |
| −/− | - | - | - | 1 (2.70%) | 2 (4.76%) | 5 (9.09%) | - | |
| +/− | - | - | - | 4 (10.82%) | 2 (4.76%) | 2 (3.64%) | - | |
| −/+ | - | - | - | - | 1 (2.39%) | 3 (5.45%) | - | |
| +/+/+ | - | - | - | - | - | - | 26 (78.79%) | |
| −/−/− | - | - | - | - | - | - | 1 (3.03%) | |
| +/−/+, +/−/−, +/+/− | - | - | - | - | - | - | 6 (18.18%) |
| S100 vs. HMB45 | S100 vs. MelanA | HMB45 vs. MelanA | |
|---|---|---|---|
| Number of patients | 37 | 42 | 55 |
| Pearson’s r correlation coefficient | 0.476 | 0.610 | 0.623 |
| p-value | <0.01 | <0.001 | <0.001 |
| S100 vs. HMB45 | S100 vs. MelanA | HMB45 vs. MelanA | |
|---|---|---|---|
| Number of patients (n = 33) | |||
| Pearson’s r correlation coefficient | 0.438 | 0.493 | 0.357 |
| p-value | <0.01 | <0.01 | >0.05 |
| Tissue Melanoma Markers | IHC Cohort n (%) | S100 n (%) | HMB45 n (%) | MelanA n (%) | S100+ HMB45 n (%) | S100+ MelanA n (%) | HMB45+ MelanA n (%) | S100 + HMB45+ MelanA n (%) |
|---|---|---|---|---|---|---|---|---|
| Number of patients | 76 | 51 | 61 | 65 | 37 | 42 | 55 | 33 |
| Soluble MIA | ||||||||
| Positive | 31 (40.79%) | 22 (43.14%) | 24 (39.34%) | 28 (43.07%) | 15 (40.54%) | 19 (45.24%) | 23 (41.82%) | 14 (42.42%) |
| Negative | 45 (59.21%) | 29 (56.86%) | 37 (60.66%) | 37 (58.46%) | 22 (59.46%) | 23 (54.76%) | 32 (58.18%) | 19 (57.58%) |
| Soluble S100B | ||||||||
| Positive | 15 (19.74%) | 11 (21.57%) | 7 (11.48%) | 12 (18.46%) | 3 (8.11%) | 8 (19.05%) | 7 (12.73%) | 3 (9.10%) |
| Negative | 61 (80.26%) | 40 (78.43%) | 54 (88.52%) | 53 (81.53%) | 34 (91.89%) | 34 (80.95%) | 48 (82.27%) | 30 (90.90%) |
| Soluble S100B + MIA | ||||||||
| S100B+/MIA+ | 9 (11.84%) | 7 (13.73%) | 4 (6.56%) | 8 (12.31%) | 2 (5.41%) | 6 (14.29%) | 4 (7.27%) | 2 (6.06%) |
| S100B+/MIA− | 6 (7.89%) | 4 (7.84%) | 3 (4.92%) | 4 (6.15%) | 1 (2.70%) | 2 (4.76%) | 3 (5.45%) | 1 (3.03%) |
| S100B−/MIA+ | 22 (28.95%) | 15 (29.41%) | 20 (32.79%) | 20 (30.77%) | 13 (35.14%) | 13 (30.95%) | 19 (34.55%) | 12 (36.36%) |
| S100B−/MIA− | 39 (51.32%) | 25 (49.02%) | 34 (55.73%) | 33 (50.77%) | 21 (56.75%) | 21 (50%) | 29 (52.73%) | 18 (54.55%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bolovan, L.M.; Ceausu, M.; Stanciu, A.E.; Panait, M.E.; Busca, A.; Hotnog, C.M.; Bleotu, C.; Gales, L.N.; Georgescu, M.T.; Prunoiu, V.M.; et al. Correlation Studies between S100 Protein Level and Soluble MIA or Tissue MelanA and gp100 (HMB45) Expression in Cutaneous Melanoma. J. Pers. Med. 2023, 13, 898. https://doi.org/10.3390/jpm13060898
Bolovan LM, Ceausu M, Stanciu AE, Panait ME, Busca A, Hotnog CM, Bleotu C, Gales LN, Georgescu MT, Prunoiu VM, et al. Correlation Studies between S100 Protein Level and Soluble MIA or Tissue MelanA and gp100 (HMB45) Expression in Cutaneous Melanoma. Journal of Personalized Medicine. 2023; 13(6):898. https://doi.org/10.3390/jpm13060898
Chicago/Turabian StyleBolovan, Lucica Madalina, Mihai Ceausu, Adina Elena Stanciu, Marieta Elena Panait, Antonela Busca, Camelia Mia Hotnog, Coralia Bleotu, Laurentia Nicoleta Gales, Mihai Teodor Georgescu, Virgiliu Mihail Prunoiu, and et al. 2023. "Correlation Studies between S100 Protein Level and Soluble MIA or Tissue MelanA and gp100 (HMB45) Expression in Cutaneous Melanoma" Journal of Personalized Medicine 13, no. 6: 898. https://doi.org/10.3390/jpm13060898