
Validation Study of the Richards-Campbell Sleep Questionnaire in Patients with Acute Stroke
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Information Collected
2.2. Sleep Assessment
2.3. RCSQ and PSG Comparison
- Total score of the scale compared with the Sleep Efficiency Index (SEI) measured on the sleep period time (SPT, defined as the total time from the sleep onset to the last awakening) of PSG.
- Perceived sleep depth compared with the time spent in stage N3 over the sleep period time (N3%) provided by PSG.
- The subjective time to fall asleep compared with sleep latency (SL) measured by PSG.
- The perceived time spent awake compared with wake after sleep onset (WASO) measured by PSG.
- Returning to sleep after an awakening compared with the mean duration of awakenings lasting longer than two minutes (AW).
- The perceived quality of sleep compared with Arousal Index (AI) of PSG. Arousals were scored according to the American Sleep Disorders Association criteria [9].
2.4. Statistical Analysis
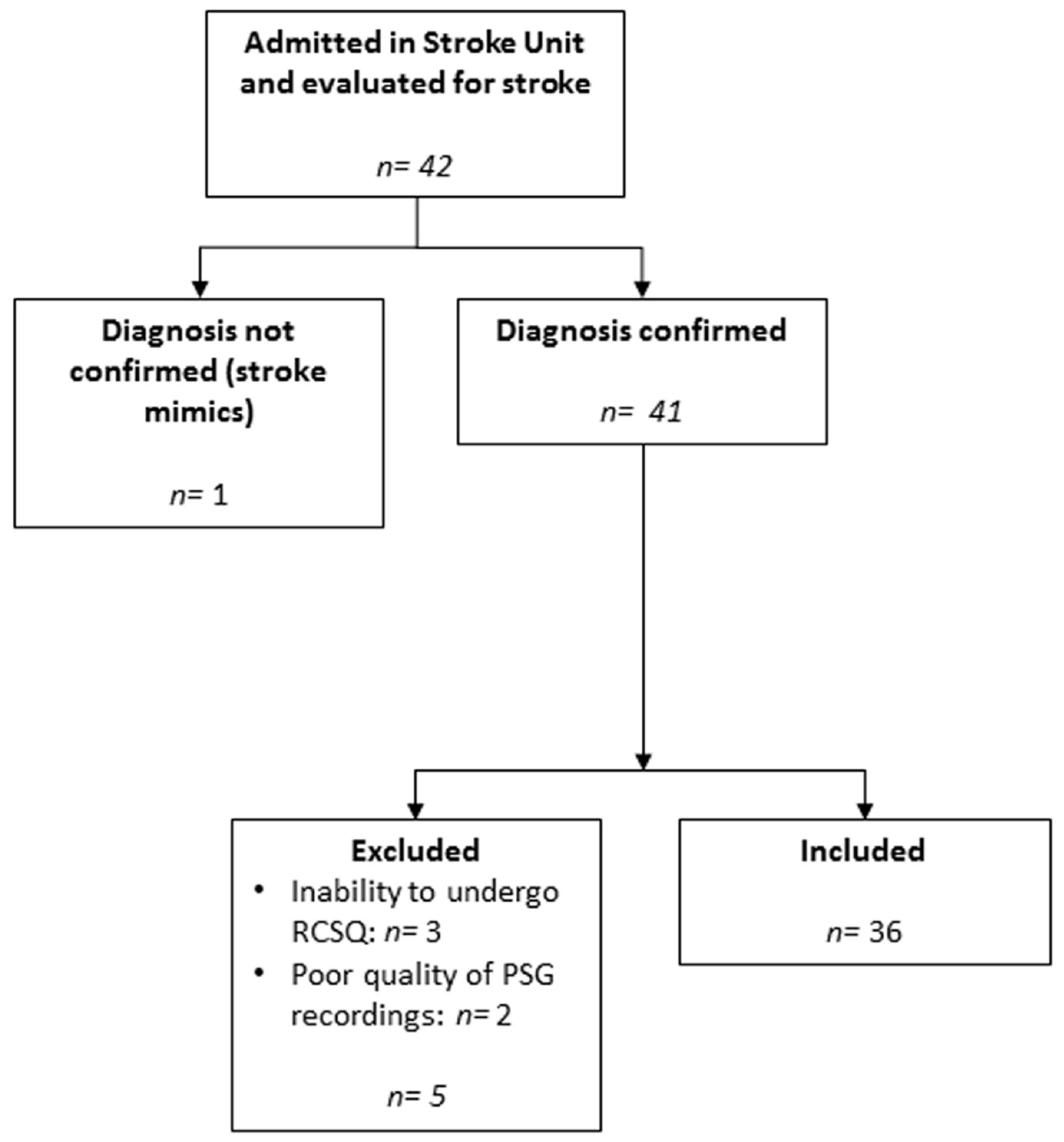
3. Results
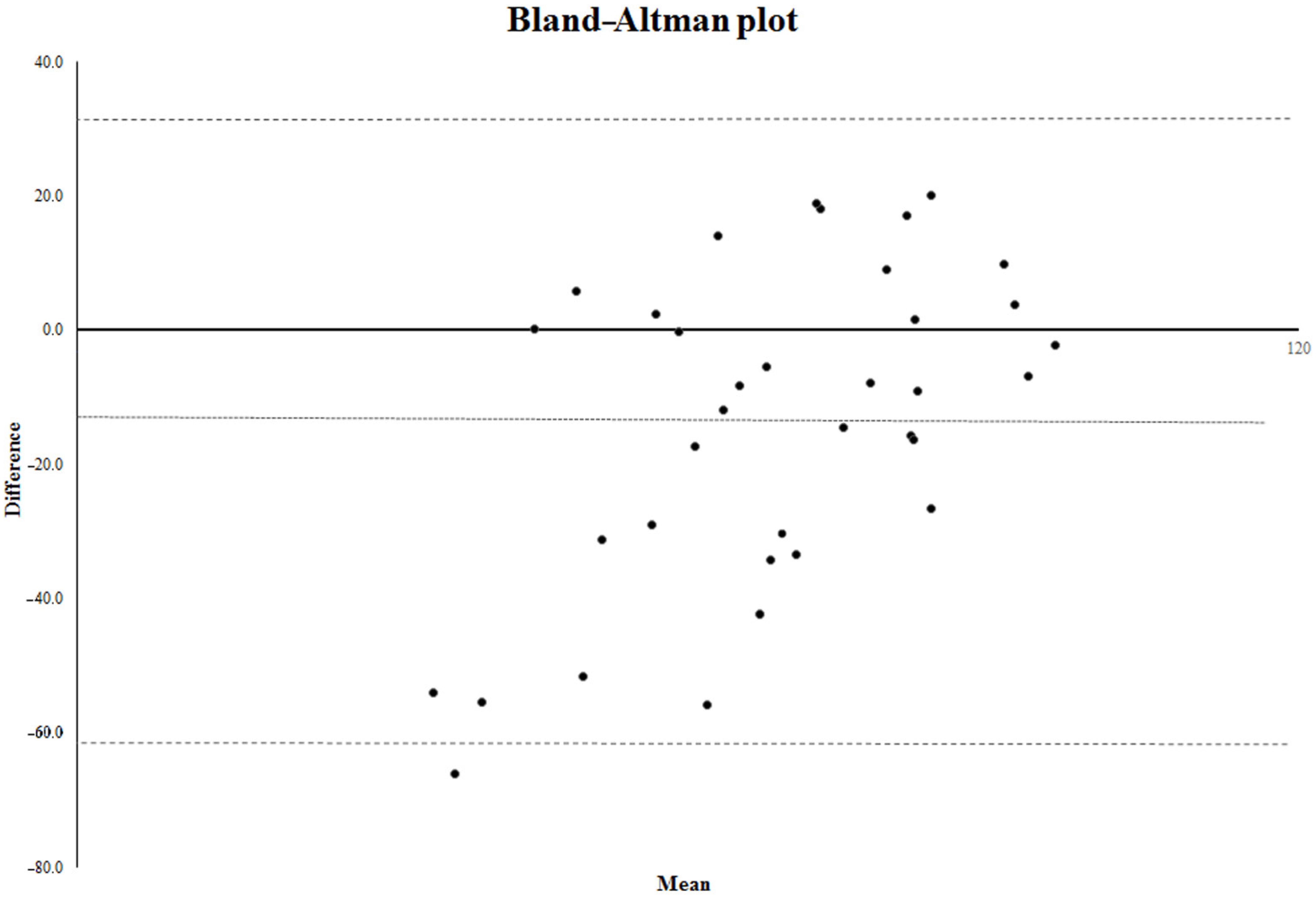
3.1. Bland–Altman Analysis
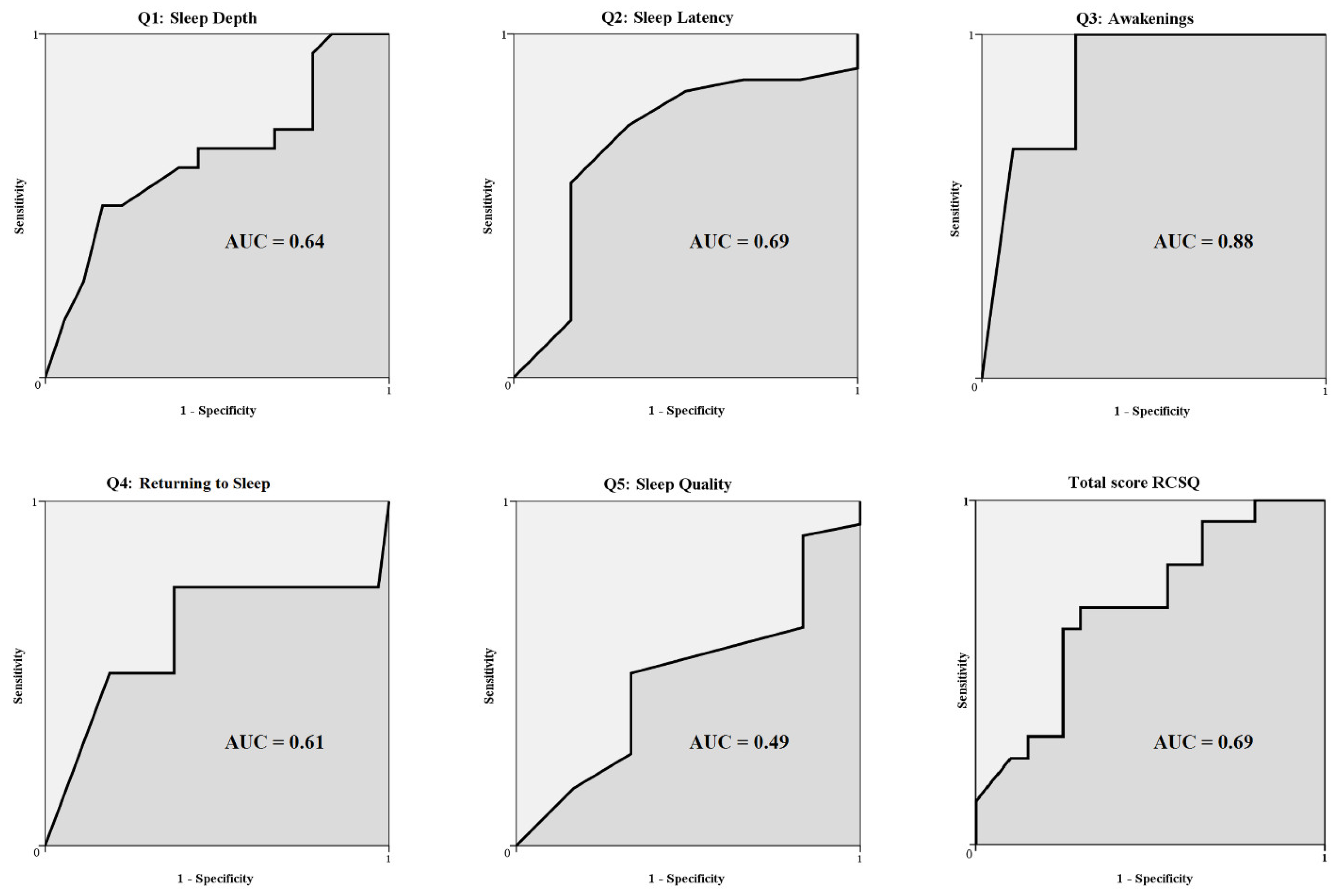
3.2. Accuracy, Sensitivity, and Specificity
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bassetti, C.L.; Randerath, W.; Vignatelli, L.; Ferini-Strambi, L.; Brill, A.-K.; Bonsignore, M.R.; Grote, L.; Jennum, P.; Leys, D.; Minnerup, J.; et al. EAN/ERS/ESO/ESRS statement on the impact of sleep disorders on risk and outcome of stroke. Eur. Respir. J. 2020, 55, 1901104. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, E.; Landau, E.; Baxter, H.; Werden, E.; Howard, M.E.; Brodtmann, A. The bidirectional impact of sleep and circadian rhythm dysfunction in human ischaemic stroke: A systematic review. Sleep Med. Rev. 2019, 45, 54–69. [Google Scholar] [CrossRef] [PubMed]
- Duss, S.B.; Seiler, A.; Schmidt, M.; Pace, M.; Adamantidis, A.; Müri, R.M.; Bassetti, C.L. The role of sleep in recovery following ischemic stroke: A review of human and animal data. Neurobiol. Sleep Circadian Rhythm. 2016, 2, 94–105. [Google Scholar] [CrossRef]
- Khot, S.P.; Morgenstern, L.B. Sleep and Stroke. Stroke 2019, 50, 1612–1617. [Google Scholar] [CrossRef] [PubMed]
- Richards, K.; O’Sullivan, P.; Phillips, R.L. Measurement of Sleep in Critically Ill Patients. J. Nurs. Meas. 2000, 8, 131–144. [Google Scholar] [CrossRef]
- Jeffs, E.L.; Darbyshire, J. Measuring Sleep in the Intensive Care Unit: A Critical Appraisal of the Use of Subjective Methods. J. Intensiv. Care Med. 2017, 34, 751–760. [Google Scholar] [CrossRef]
- Kakar, E.; Priester, M.; Wessels, P.; Slooter, A.J.; Louter, M.; van der Jagt, M. Sleep assessment in critically ill adults: A systematic review and meta-analysis. J. Crit. Care 2022, 71, 154102. [Google Scholar] [CrossRef]
- Silber, M.H.; Ancoli-Israel, S.; Bonnet, M.H.; Chokroverty, S.; Grigg-Damberger, M.M.; Hirshkowitz, M.; Kapen, S.; Keenan, S.A.; Kryger, M.H.; Penzel, T.; et al. The Visual Scoring of Sleep in Adults. J. Clin. Sleep Med. 2007, 3, 121–131. [Google Scholar] [CrossRef]
- Atlas Task Force of the American Sleep Disorders Association. EEG Arousals: Scoring Rules and Examples. Sleep 1992, 15, 173–184. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Zou, K.H.; O’Malley, A.J.; Mauri, L. Receiver-Operating Characteristic Analysis for Evaluating Diagnostic Tests and Predictive Models. Circulation 2007, 115, 654–657. [Google Scholar] [CrossRef] [PubMed]
- Kamdar, B.; Shah, P.; King, L.M.; Kho, M.; Zhou, X.; Colantuoni, E.; Collop, N.A.; Needham, D.M. Patient-Nurse Interrater Reliability and Agreement of the Richards-Campbell Sleep Questionnaire. Am. J. Crit. Care 2012, 21, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Manconi, M.; Ferri, R.; Sagrada, C.; Punjabi, N.M.; Tettamanzi, E.; Zucconi, M.; Oldani, A.; Castronovo, V.; Strambi, L.F. Measuring the error in sleep estimation in normal subjects and in patients with insomnia. J. Sleep Res. 2010, 19, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Jaramillo, V.; Jendoubi, J.; Maric, A.; Mensen, A.; Heyse, N.C.; Eberhard-Moscicka, A.K.; Wiest, R.; Bassetti, C.L.A.; Huber, R. Thalamic Influence on Slow Wave Slope Renormalization During Sleep. Ann. Neurol. 2021, 90, 821–833. [Google Scholar] [CrossRef] [PubMed]
- Baglioni, C.; Nissen, C.; Schweinoch, A.; Riemann, D.; Spiegelhalder, K.; Berger, M.; Weiller, C.; Sterr, A. Polysomnographic Characteristics of Sleep in Stroke: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0148496. [Google Scholar] [CrossRef]
- Johnson, K.G.; Johnson, D.C. Frequency of Sleep Apnea in Stroke and TIA Patients: A Meta-analysis. J. Clin. Sleep Med. 2010, 6, 131–137. [Google Scholar] [CrossRef]
- Hasan, F.; Gordon, C.; Wu, D.; Huang, H.-C.; Yuliana, L.T.; Susatia, B.; Marta, O.F.D.; Chiu, H.-Y. Dynamic Prevalence of Sleep Disorders Following Stroke or Transient Ischemic Attack. Stroke 2021, 52, 655–663. [Google Scholar] [CrossRef]
- Bassetti, C.L.; Hermann, D.M. Sleep and stroke. Handb. Clin. Neurol. 2011, 99, 1051–1072. [Google Scholar] [CrossRef]
- Lisabeth, L.D.; Sánchez, B.N.; Lim, D.; Chervin, R.D.; Case, E.; Morgenstern, L.B.; Tower, S.; Brown, D. Sleep-disordered breathing and poststroke outcomes. Ann. Neurol. 2019, 86, 241–250. [Google Scholar] [CrossRef]
- Yoon, C.W.; Park, H.-K.; Bae, E.-K.; Rha, J.-H. Sleep Apnea and Early Neurological Deterioration in Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 104510. [Google Scholar] [CrossRef]
- Brown, D.L.; Jiang, X.; Li, C.; Case, E.; Sozener, C.B.; Chervin, R.D.; Lisabeth, L.D. Sleep apnea screening is uncommon after stroke. Sleep Med. 2018, 59, 90–93. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Richards-Campbell Sleep Questionnaire | |
|---|---|
| Measure | Question |
| Q1: Sleep depth | My sleep last night was: light sleep (0) … deep sleep (100) |
| Q2: Sleep latency | Last night, the first time I got to sleep, I: just never could fall asleep (0) … fell asleep almost immediately (100) |
| Q3: Awakenings | Last night, I was: awake all night long (0) … awake very little (100) |
| Q4: Returning to sleep | Last night, when I woke up or was awakened, I: could not get back to sleep (0) … got back to sleep immediately (100) |
| Q5: Sleep quality | I would describe my sleep last night as: a bad night’s sleep (0) … a good night’s sleep (100) |
| Mean (SD) | N (%) | |
|---|---|---|
| Clinical data | ||
| Males | 17 (47.2%) | |
| Age (yr) | 74.1 (12.9) | |
| Stroke type | ||
| Ischemic | 31 (86.1%) | |
| Haemorragic | 5 (13.9%) | |
| side (left) | 24 (66.6%) | |
| NIHSS | 3.1 (3.0) | |
| LVO | 24 (66.6%) | |
| IVT | 11 (30.6%) | |
| EVT | 22 (61.1%) | |
| CNS acting drugs | 6 (16.6%) | |
| Polysomnography | ||
| TST (min) | 366.7 (77.9) | |
| SPT (min) | 488.0 (106.7) | |
| SL (min) | 22.9 (34.8) | |
| SEI (%) | 75.5 (13.9) | |
| WASO (min) | 133.4 (74.1) | |
| AW (min) | 32.2 (23.4) | |
| AI | 9.4 (16.5) | |
| W (%) | 24.9 (13.8) | |
| N1 (%) | 8.6 (4.5) | |
| N2 (%) | 39.2 (11.5) | |
| N3 (%) | 15.4 (11.4) | |
| REM (%) | 8.2 (4.9) | |
| AHI-Ob | 28.5 (22.7) | |
| AHI-C | 6.5 (11.6) | |
| ODI | 32.9 (27.8) | |
| RCSQ | Mean (SD) | PSG | Mean (SD) | Concordance | Kendall W Coefficient |
|---|---|---|---|---|---|
| Total score | 61.4 (24.8) | SEI (%) | 75.5 (13.9) | Total score vs. SEI | 0.686 |
| Q1: sleep depth | 59.8 (29.9) | N3 (%) | 15.4 (11.4) | Q1 vs. N3 | 0.551 |
| Q2: sleep latency | 64.2 (28.0) | SL (min) | 22.9 (34.8) | Q2 vs. SL | 0.468 |
| Q3: awakenings | 57.5 (28.4) | WASO (min) | 133.4 (74.1) | Q3 vs. WASO | 0.234 |
| Q4: returning to sleep | 65.3 (29.3) | AW (min) | 32.2 (23.4) | Q4 vs. AW | 0.305 |
| Q5: sleep quality | 60.1 (28.7) | AI | 9.4 (16.5) | Q5 vs. AI | 0.453 |
| Sensitivity | Specificity | Accuracy | Cut-Off PSG | Cut-Off RCSQ | |
|---|---|---|---|---|---|
| Total score RCSQ | 71% | 68% | 70% | 80 | 65 |
| Q1: Sleep depth | 61% | 60% | 61% | 15 | 65 |
| Q2: Sleep latency | 60% | 83% | 64% | 30 | 65 |
| Q3: Awakenings | 100% | 58% | 61% | 30 | 65 |
| Q4: Returning to sleep | 60% | 57% | 58% | 5 | 65 |
| Q5: Sleep quality | 61% | 70% | 64% | 10 | 65 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rollo, E.; Della Marca, G.; Scala, I.; Buccarella, C.; Rozera, T.; Vollono, C.; Frisullo, G.; Broccolini, A.; Brunetti, V. Validation Study of the Richards-Campbell Sleep Questionnaire in Patients with Acute Stroke. J. Pers. Med. 2022, 12, 1473. https://doi.org/10.3390/jpm12091473
Rollo E, Della Marca G, Scala I, Buccarella C, Rozera T, Vollono C, Frisullo G, Broccolini A, Brunetti V. Validation Study of the Richards-Campbell Sleep Questionnaire in Patients with Acute Stroke. Journal of Personalized Medicine. 2022; 12(9):1473. https://doi.org/10.3390/jpm12091473
Chicago/Turabian StyleRollo, Eleonora, Giacomo Della Marca, Irene Scala, Cristina Buccarella, Tommaso Rozera, Catello Vollono, Giovanni Frisullo, Aldobrando Broccolini, and Valerio Brunetti. 2022. "Validation Study of the Richards-Campbell Sleep Questionnaire in Patients with Acute Stroke" Journal of Personalized Medicine 12, no. 9: 1473. https://doi.org/10.3390/jpm12091473