
Comparison of Postoperative Coronal Leg Alignment in Customized Individually Made and Conventional Total Knee Arthroplasty

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
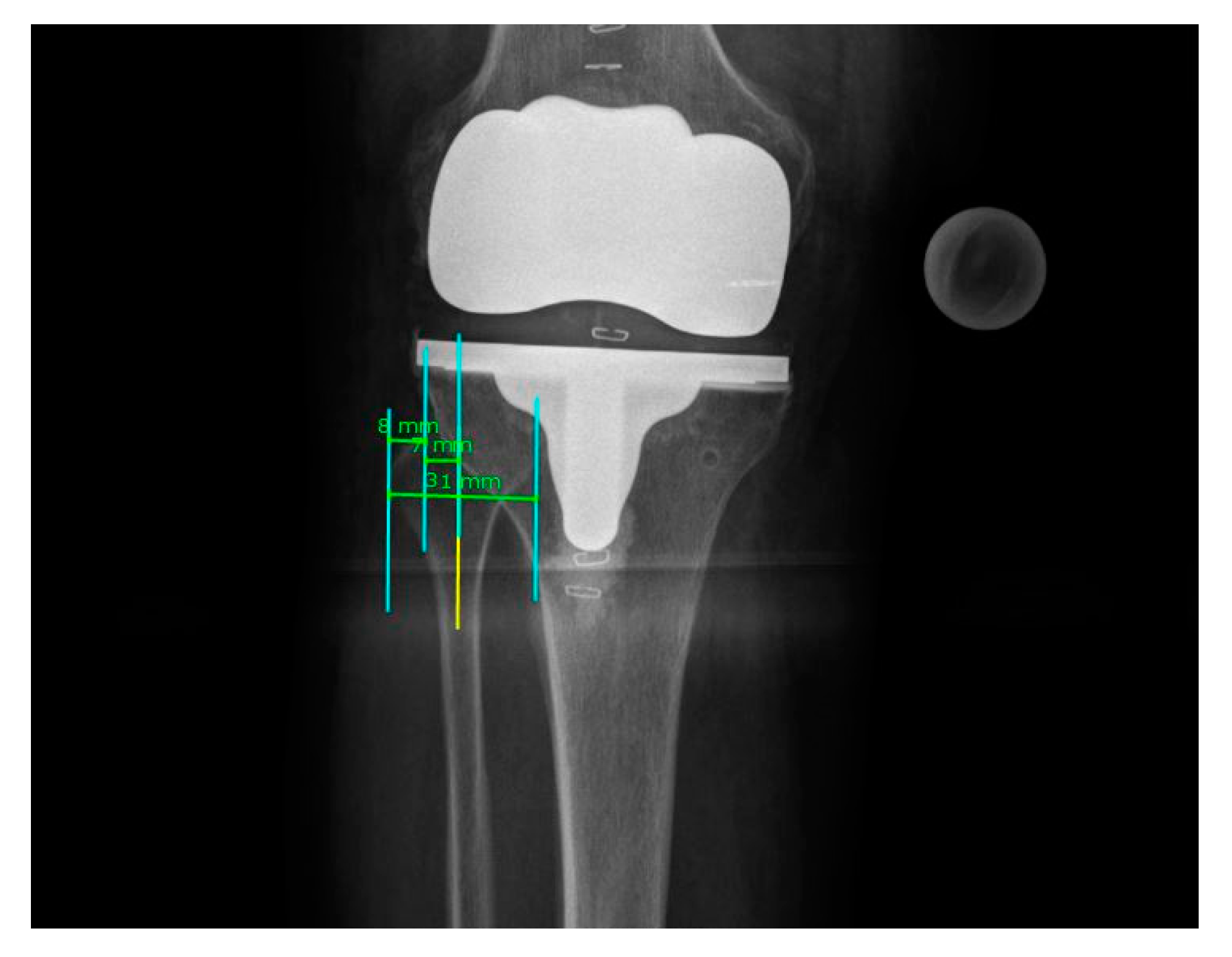
3.1. Rotational Correction
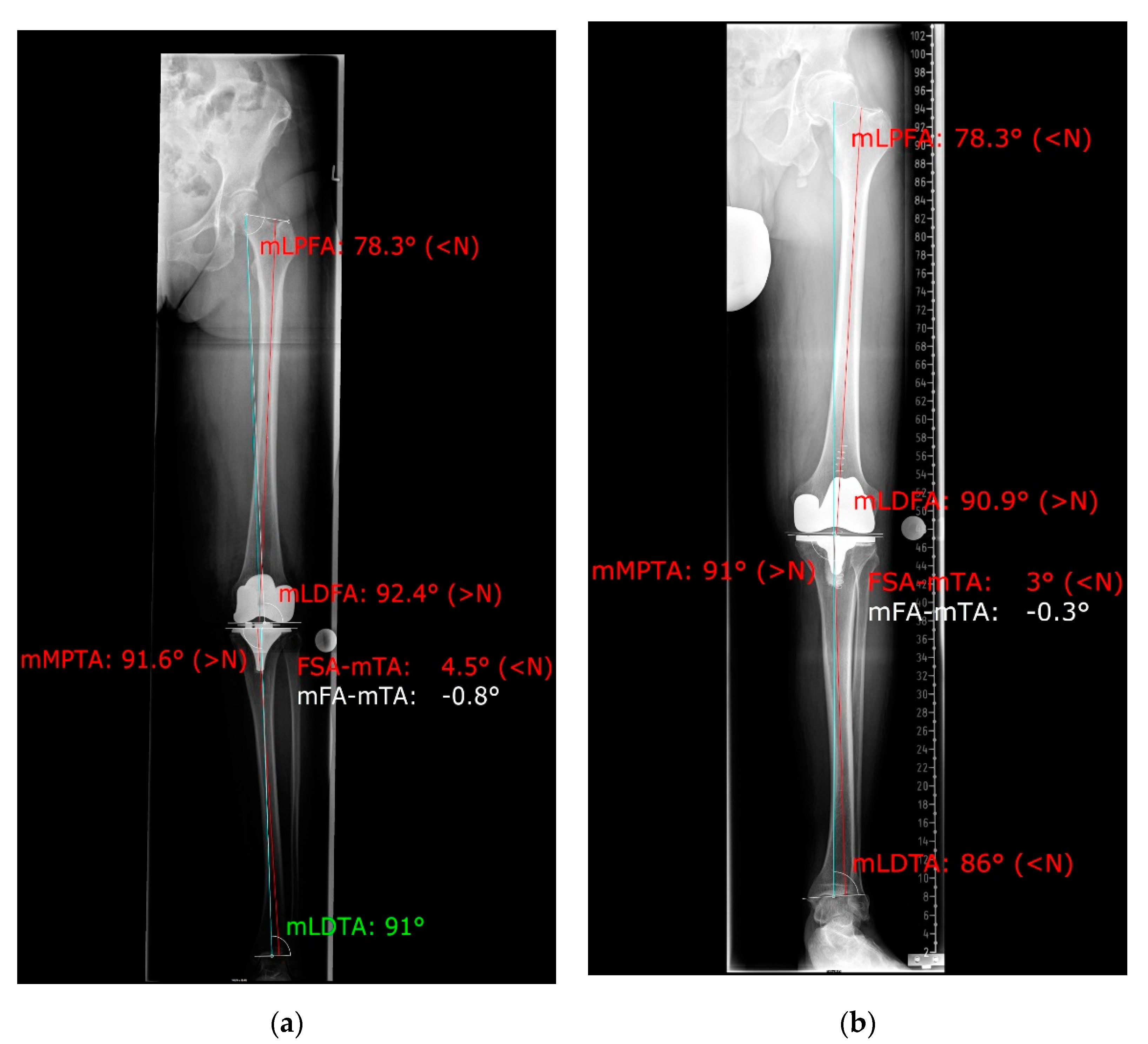
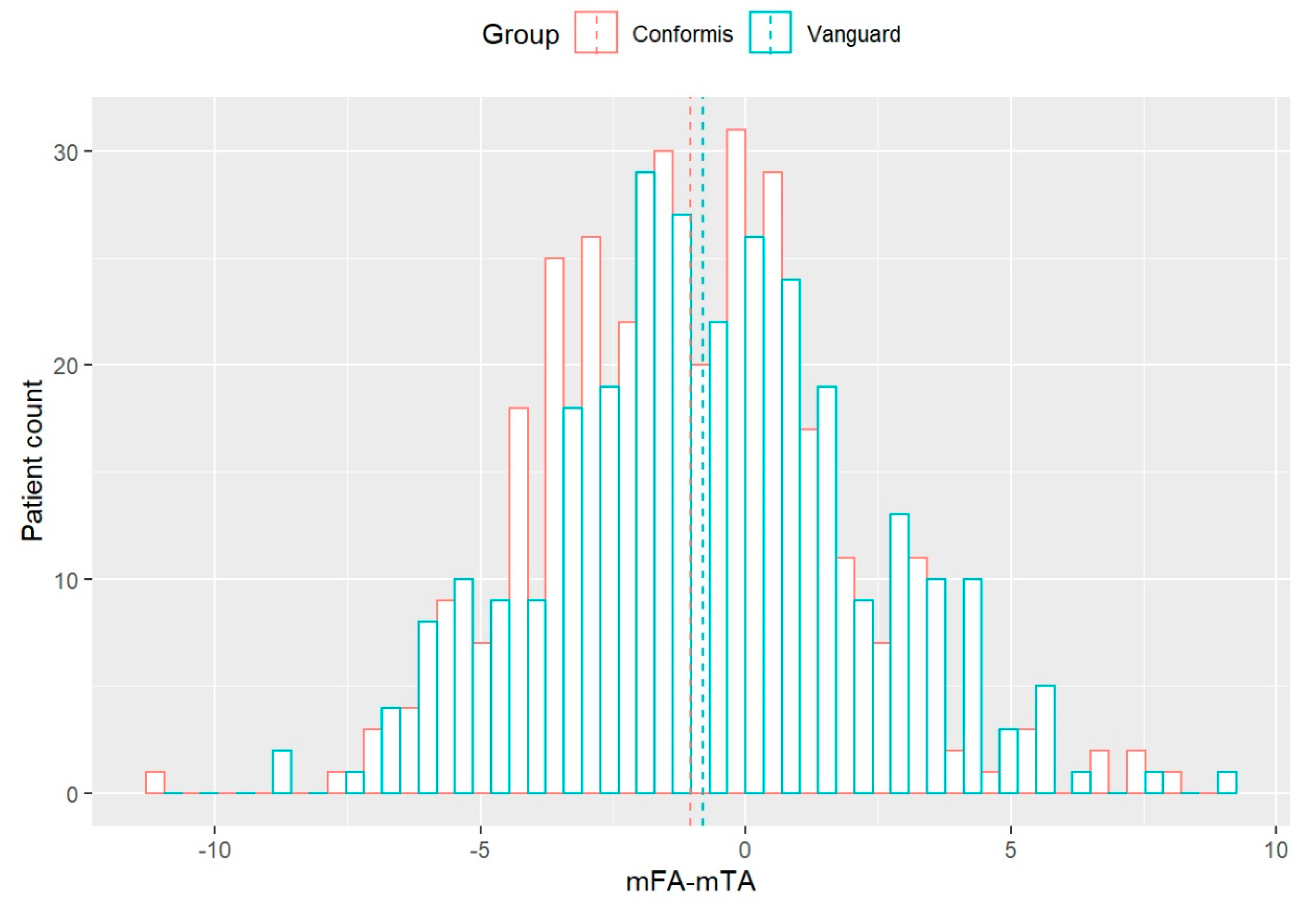
3.2. Coronal Alignment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bourne, R.B.; Chesworth, B.M.; Davis, A.M.; Mahomed, N.N.; Charron, K.D.J. Patient Satisfaction after Total Knee Arthroplasty: Who is Satisfied and Who is Not? Clin. Orthop. Relat. Res. 2010, 468, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeffery, R.S.; Morris, R.W.; A Denham, R. Coronal alignment after total knee replacement. J. Bone Jt. Surg. Ser. B 1991, 73, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Sikorski, J.M. Alignment in total knee replacement. J. Bone Jt. Surgery. Br. Vol. 2008, 90, 1121–1127. [Google Scholar] [CrossRef]
- Sharkey, P.F.; Lichstein, P.M.; Shen, C.; Tokarski, A.T.; Parvizi, J. Why Are Total Knee Arthroplasties Failing Today—Has Anything Changed After 10 Years? J. Arthroplast. 2014, 29, 1774–1778. [Google Scholar] [CrossRef]
- Collier, M.B.; Engh, C.A.; McAuley, J.P.; Engh, G.A. Factors associated with the loss of thickness of polyethylene tibial bearings after knee arthroplasty. J. Bone Jt. Surg.Ser. A 2007, 89, 1306–1314. [Google Scholar] [CrossRef]
- Steinert, A.F.; Sefrin, L.; Jansen, B.; Schroder, L.; Horzapfel, B.M.; Arnholdt, J.; Rudert, M. Patient-specific cruciate-retaining total knee replacement with individualized implants and instruments (iTotalTM CR G2). Oper. Orthop. Traumatol. 2021, 33, 170–180. [Google Scholar] [CrossRef]
- Schwechter, E.M.; Fitz, W. Design rationale for customized TKA: A new idea or revisiting the past? Curr. Rev. Musculoskelet. Med. 2012, 5, 303–308. [Google Scholar] [CrossRef] [Green Version]
- Arnholdt, J.; Kamawal, Y.; Horas, K.; Holzapfel, B.M.; Gilbert, F.; Ripp, A.; Rudert, M.; Steinert, A.F. Accurate implant fit and leg alignment after cruciate-retaining patient-specific total knee arthroplasty. BMC Musculoskelet. Disord. 2020, 21, 1–8. [Google Scholar] [CrossRef]
- Arbab, D.; Reimann, P.; Brucker, M.; Bouillon, B.; Lüring, C. Alignment in total knee arthroplasty—A comparison of patient-specific implants with the conventional technique. Knee 2018, 25, 882–887. [Google Scholar] [CrossRef]
- Maderbacher, G.; Schaumburger, J.; Baier, C.; Zeman, F.; Springorum, H.-R.; Dornia, C.; Grifka, J.; Keshmiri, A. Predicting knee rotation by the projection overlap of the proximal fibula and tibia in long-leg radiographs. Knee Surgery, Sports Traumatol. Arthrosc. 2014, 22, 2982–2988. [Google Scholar] [CrossRef] [PubMed]
- Maderbacher, G.; Matussek, J.; Greimel, F.; Grifka, J.; Schaumburger, J.; Baier, C.; Keshmiri, A. Lower Limb Malrotation Is Regularly Present in Long-Leg Radiographs Resulting in Significant Measurement Errors. J. Knee Surg. 2021, 34, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Reed, S.C.; Gollish, J. The accuracy of femoral intramedullary guides in total knee arthroplasty. J. Arthroplast. 1997, 12, 677–682. [Google Scholar] [CrossRef]
- Chauhan, S.K.; Scott, R.G.; Breidahl, W. Computer-assisted knee arthroplasty versus a conventional jig-based technique. A randomised, prospective trial. J. Bone Jt. Surg. Ser. B 2004, 86, 372–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hart, R.; Janecek, M.; Chaker, A. Total knee arthroplasty implanted with and without kinematic navigation. Int. Orthop. 2003, 27, 366–369. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, T.; Tsumura, N.; Kurosaka, M.; Muratsu, H.; Kuroda, R.; Ishimoto, K.; Tsujimoto, K.; Shiba, R. Prosthetic alignment and sizing in computer-assisted total knee arthroplasty. Int. Orthop. 2004, 28, 282–285. [Google Scholar] [CrossRef] [Green Version]
- Noriega-Fernandez, A.; Hernández-Vaquero, D.; Suarez-Vazquez, A.; Sandoval-Garcia, M.A. Computer Assistance Increases Precision of Component Placement in Total Knee Arthroplasty with Articular Deformity. Clin. Orthop. Relat. Res. 2010, 468, 1237–1241. [Google Scholar]
- Bäthis, H.; Perlick, L.; Tingart, M.; Lüring, C.; Zurakowski, D.; Grifka, J. Alignment in total knee arthroplasty. A comparison of computer-assisted surgery with the conventional technique. J. Bone Jt. Surg. Ser. B 2004, 86, 682–687. [Google Scholar] [CrossRef]
- Nam, D.; Park, A.; Stambough, J.B.; Johnson, S.R.; Nunley, R.M.; Barrack, R.L. The Mark Coventry Award: Custom Cutting Guides Do Not Improve Total Knee Arthroplasty Clinical Outcomes at 2 Years Followup. Clin. Orthop. Relat. Res. 2016, 474, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Lonner, J.H.; Laird, M.T.; Stuchin, S.A. Effect of Rotation and Knee Flexion on Radiographic Alignment in Total Knee Arthroplasties. Clin. Orthop. Relat. Res. 1996, 331, 102–106. [Google Scholar] [CrossRef]
- Maderbacher, G.; Baier, C.; Benditz, A.; Wagner, F.; Greimel, F.; Grifka, J.; Keshmiri, A. Presence of rotational errors in long leg radiographs after total knee arthroplasty and impact on measured lower limb and component alignment. Int. Orthop. 2017, 41, 1553–1560. [Google Scholar] [CrossRef]
- Hinman, R.S.; May, R.L.; Crossley, K.M. Is There an Alternative to the Full-Leg Radiograph for Determining Knee Joint Alignment in Osteoarthritis? Arthritis Care Res. 2006, 55, 306–313. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | CIM (iTotal CR G2) | OTS (Vanguard CR) |
|---|---|---|
| Age (years) (mean (SD)) | 69.5 (10.3) | 71.7 (10.4) |
| Gender | ||
| male | 149 | 105 |
| female | 134 | 174 |
| Side of Surgery | ||
| left | 90 | 115 |
| right | 108 | 127 |
| both | 85 | 37 |
| Previous operation on affected leg (%) | 24 (8.5%) | 15 (5.3%) |
| iTotal™ CR G2 (n = 283) | Vanguard™ CR (n = 279) | |
|---|---|---|
| HKA uncorrected | 179.2° ± 2.9° | 179.6° ± 3.1° |
| HKA corrected | 179.0° ± 2.8° | 179.2° ± 3.1° |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wunderlich, F.; Azad, M.; Westphal, R.; Klonschinski, T.; Belikan, P.; Drees, P.; Eckhard, L. Comparison of Postoperative Coronal Leg Alignment in Customized Individually Made and Conventional Total Knee Arthroplasty. J. Pers. Med. 2021, 11, 549. https://doi.org/10.3390/jpm11060549
Wunderlich F, Azad M, Westphal R, Klonschinski T, Belikan P, Drees P, Eckhard L. Comparison of Postoperative Coronal Leg Alignment in Customized Individually Made and Conventional Total Knee Arthroplasty. Journal of Personalized Medicine. 2021; 11(6):549. https://doi.org/10.3390/jpm11060549
Chicago/Turabian StyleWunderlich, Felix, Maheen Azad, Ruben Westphal, Thomas Klonschinski, Patrick Belikan, Philipp Drees, and Lukas Eckhard. 2021. "Comparison of Postoperative Coronal Leg Alignment in Customized Individually Made and Conventional Total Knee Arthroplasty" Journal of Personalized Medicine 11, no. 6: 549. https://doi.org/10.3390/jpm11060549