
Updates on Robotic CME for Right Colon Cancer: A Qualitative Systematic Review


Abstract
:1. Background
2. Methods
3. Results
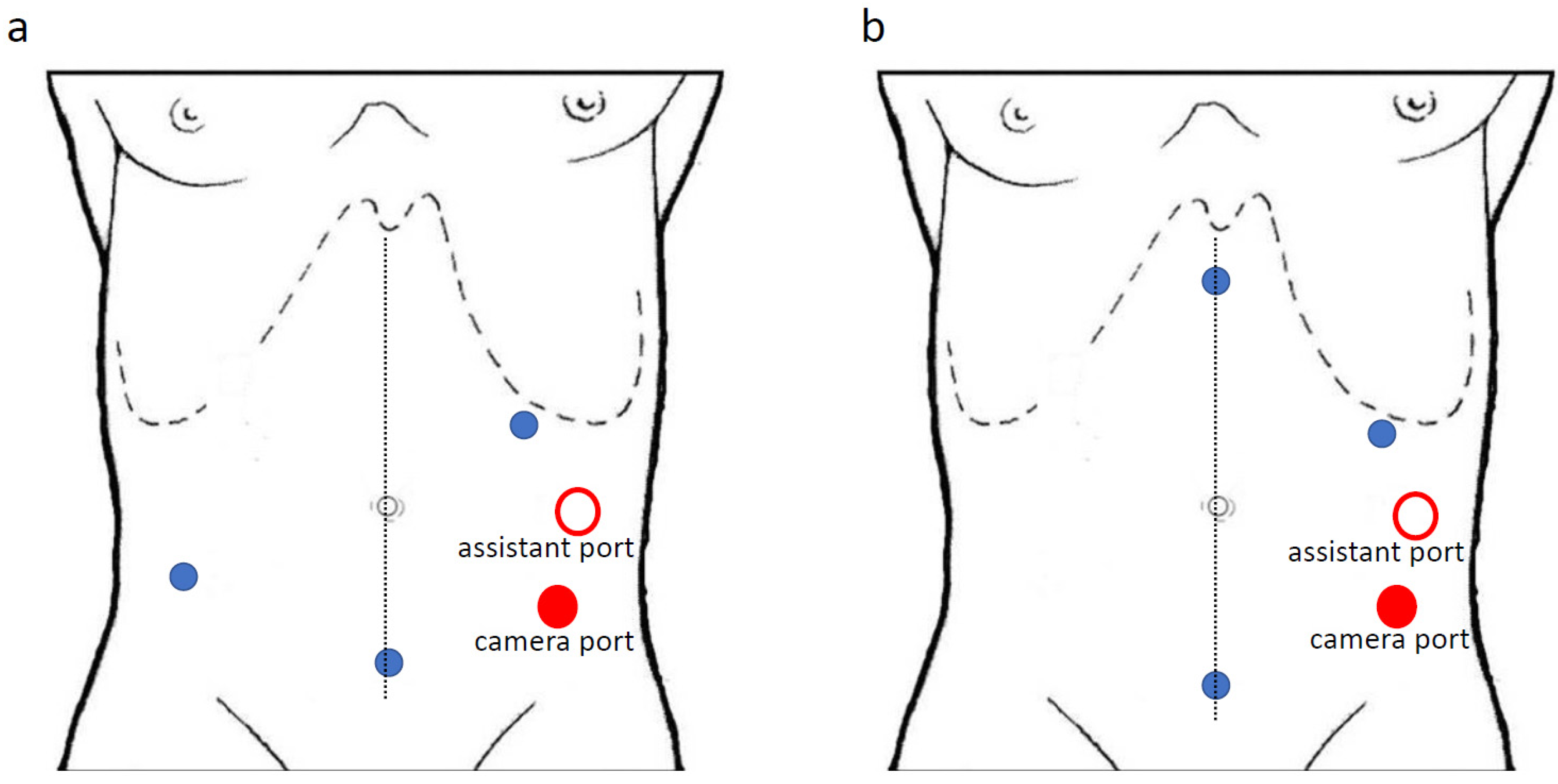
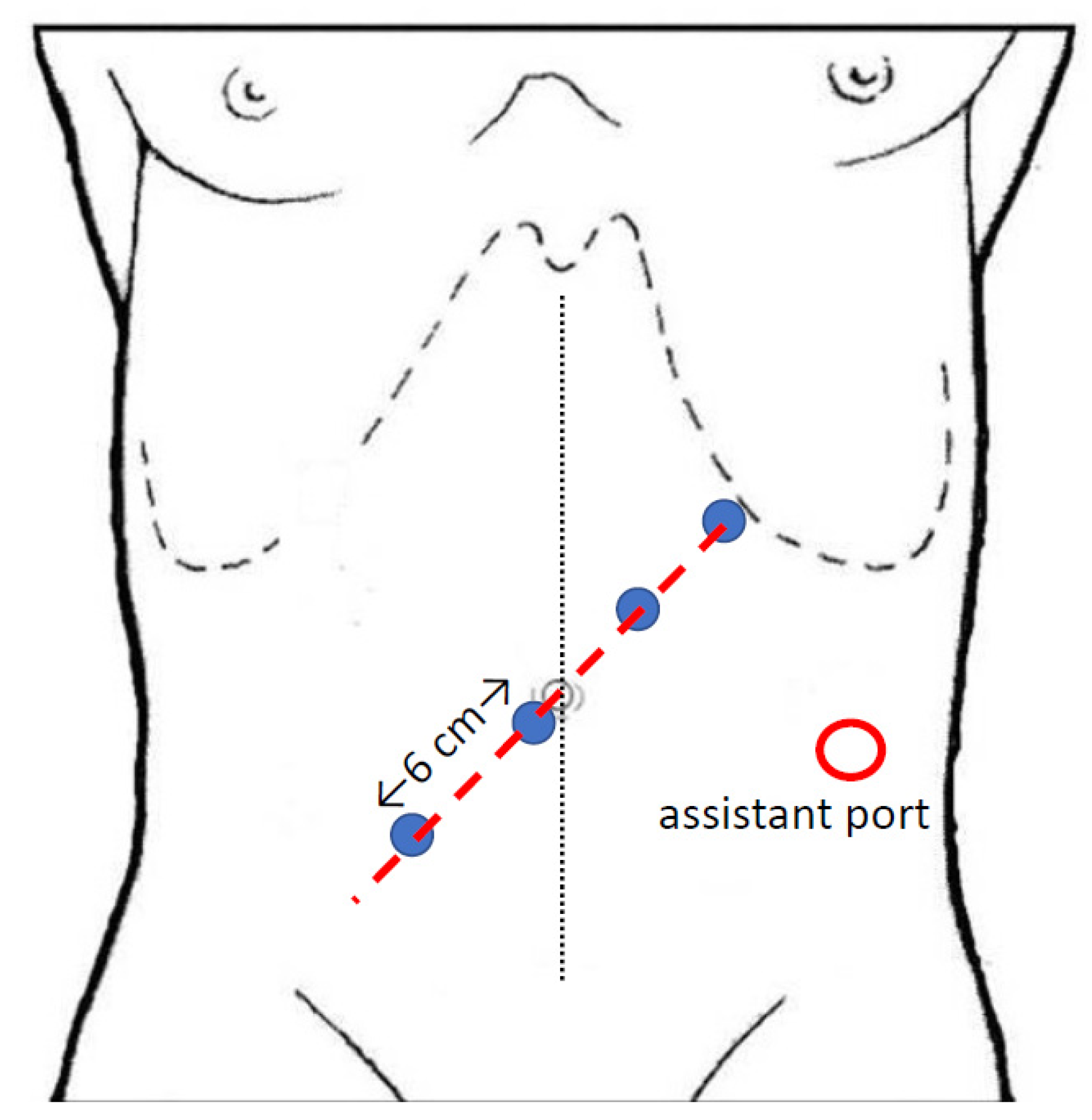
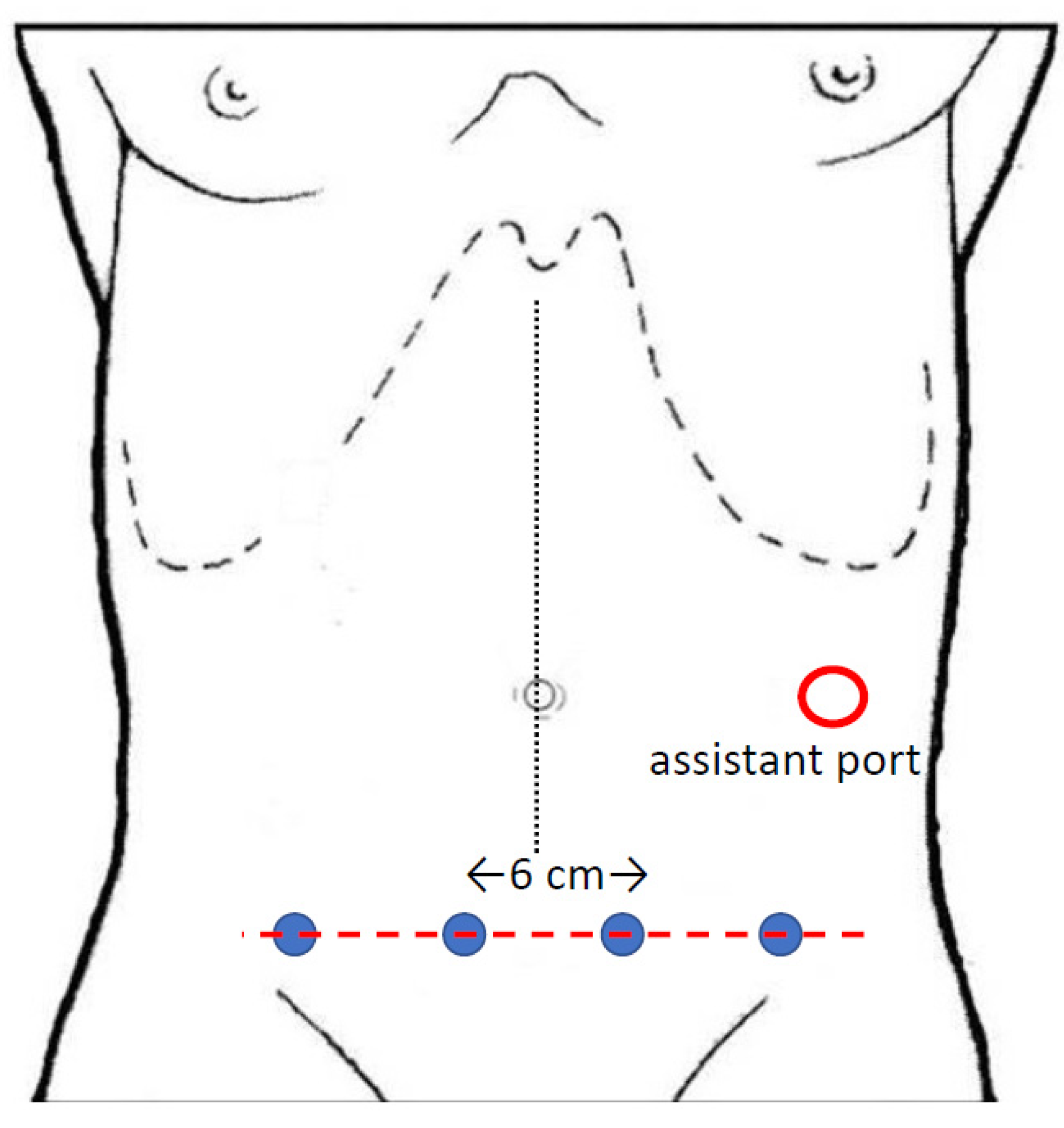
4. Technical Considerations
5. Clinical Outcomes
5.1. Operative Results
5.2. Early Clinical Results
6. Oncologic Outcomes
7. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- West, N.P.; Morris, E.J.; Rotimi, O.; Cairns, A.; Finan, P.J.; Quirke, P. Pathology grading of colon cancer surgical resection and its association with survival: A retrospective observational study. Lancet Oncol. 2008, 9, 857–865. [Google Scholar] [CrossRef]
- Hohenberger, W.; Weber, K.; Matzel, K.; Papadopoulos, T.; Merkel, S. Standardized surgery for colonic cancer: Complete mesocolic excision and central ligation—Technical notes and outcome. Colorectal Dis. 2009, 11, 354–364. [Google Scholar] [CrossRef] [PubMed]
- Japanese Society for Cancer of the Colon and Rectum. Japanese Classification of Colorectal Carcinoma, 2nd ed.; Kanehara & Co., Ltd.: Tokyo, Japan, 2009. [Google Scholar]
- Bokey, E.L.; Chapuis, P.H.; Dent, O.F.; Mander, B.J.; Bissett, I.; Newland, R.C. Surgical Technique and Survival in Patients Having a Curative Resection for Colon Cancer. Dis. Colon Rectum 2003, 46, 860–866. [Google Scholar] [CrossRef] [PubMed]
- Ovrebo, K.; Rokke, O. Extended lymph node dissection in colorectal cancer surgery. Reliability and reproducibility in assessments of operative reports. Int. J. Colorectal Dis. 2010, 25, 213–222. [Google Scholar] [CrossRef] [PubMed]
- West, N.P.; Hohenberger, W.; Weber, K.; Perrakis, A.; Finan, P.J.; Quirke, P. Complete Mesocolic Excision with Central Vascular Ligation Produces an Oncologically Superior Specimen Compared with Standard Surgery for Carcinoma of the Colon. J. Clin. Oncol. 2010, 28, 272–278. [Google Scholar] [CrossRef] [Green Version]
- Storli, K.E.; Søndenaa, K.; Furnes, B.; Nesvik, I.; Gudlaugsson, E.; Bukholm, I.; Eide, G.E. Short term results of complete (D3) vs. standard (D2) mesenteric excision in colon cancer shows improved outcome of complete mesenteric excision in patients with TNM stages I–II. Tech. Coloproctol. 2013, 18, 557–564. [Google Scholar] [CrossRef]
- Søndenaa, K.; Quirke, P.; Hohenberger, W.; Sugihara, K.; Kobayashi, H.; Kessler, H.; Brown, G.; Tudyka, V.; D’Hoore, A.; Kennedy, R.H.; et al. The rationale behind complete mesocolic excision (CME) and a central vascular ligation for colon cancer in open and laparoscopic surgery. Int. J. Colorectal Dis. 2014, 29, 419–428. [Google Scholar] [CrossRef]
- Bertelsen, C.A.; Neuenschwander, A.U.; Jansen, J.E.; Wilhelmsen, M.; Kirkegaard-Klitbo, A.; Tenma, J.R.; Bols, B.; Ingeholm, P.; Rasmussen, L.A.; Jepsen, L.V.; et al. Disease-free survival after complete mesocolic excision compared with conventional colon cancer surgery: A retrospective, population-based study. Lancet Oncol. 2015, 16, 161–168. [Google Scholar] [CrossRef]
- Liang, J.-T.; Lai, H.-S.; Huang, J.; Sun, C.-T. Long-term oncologic results of laparoscopic D3 lymphadenectomy with complete mesocolic excision for right-sided colon cancer with clinically positive lymph nodes. Surg. Endosc. 2015, 29, 2394–2401. [Google Scholar] [CrossRef]
- Spinoglio, G.; Marano, A.; Bianchi, P.P.; Priora, F.; Lenti, L.M.; Ravazzoni, F.; Formisano, G. Robotic Right Colectomy with Modified Complete Mesocolic Excision: Long-Term Oncologic Outcomes. Ann. Surg. Oncol. 2016, 23, 684–691. [Google Scholar] [CrossRef]
- Bernhoff, R.; Martling, A.; Sjövall, A.; Granath, F.; Hohenberger, W.; Holm, T. Improved survival after an educational project on colon cancer management in the county of Stockholm—A population based cohort study. Eur. J. Surg. Oncol. (EJSO) 2015, 41, 1479–1484. [Google Scholar] [CrossRef] [PubMed]
- Paquette, I.M.; Madoff, R.D.; Sigurdson, E.R.; Chang, G.J. Impact of Proximal Vascular Ligation on Survival of Patients with Colon Cancer. Ann. Surg. Oncol. 2016, 25, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Ow, Z.G.W.; Sim, W.; Nistala, K.R.Y.; Ng, C.H.; Koh, F.H.-X.; Wong, N.W.; Foo, F.J.; Tan, K.-K.; Chong, C.S. Comparing complete mesocolic excision versus conventional colectomy for colon cancer: A systematic review and meta-analysis. Eur. J. Surg. Oncol. (EJSO) 2021, 47, 732–737. [Google Scholar] [CrossRef] [PubMed]
- Argilés, G.; Tabernero, J.; Labianca, R.; Hochhauser, D.; Salazar, R.; Iveson, T.; Laurent-Puig, P.; Quirke, P.; Yoshino, T.; Taieb, J.; et al. Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1291–1305. [Google Scholar] [CrossRef]
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Colon Cancer. Version 2.2021—21 January. Available online: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf (accessed on 15 April 2021).
- Glynne-Jones, R.; Wyrwicz, L.; Tiret, E.; Brown, G.; Rödel, C.; Cervantes, A.; Arnold, D. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv22–iv40. [Google Scholar] [CrossRef]
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Rectal Cancer. Version 1.2021—22 December. Available online: https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf (accessed on 15 April 2021).
- Killeen, S.; Mannion, M.; Devaney, A.; Winter, D.C. Complete mesocolic resection and extended lymphadenectomy for colon cancer: A systematic review. Colorectal Dis. 2014, 16, 577–594. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2013. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 15 April 2021).
- Trastulli, S.; Desiderio, J.; Farinacci, F.; Ricci, F.; Listorti, C.; Cirocchi, R.; Boselli, C.; Noya, G.; Parisi, A. Robotic right colectomy for cancer with intracorporeal anastomosis: Short-term outcomes from a single institution. Int. J. Colorectal Dis. 2013, 28, 807–814. [Google Scholar] [CrossRef]
- Petz, W.; Ribero, D.; Bertani, E.; Borin, S.; Formisano, G.; Esposito, S.; Spinoglio, G.; Bianchi, P. Suprapubic approach for robotic complete mesocolic excision in right colectomy: Oncologic safety and short-term outcomes of an original technique. Eur. J. Surg. Oncol. (EJSO) 2017, 43, 2060–2066. [Google Scholar] [CrossRef] [PubMed]
- Spinoglio, G.; Bianchi, P.P.; Marano, A.; Priora, F.; Lenti, L.M.; Ravazzoni, F.; Petz, W.; Borin, S.; Ribero, D.; Formisano, G.; et al. Robotic Versus Laparoscopic Right Colectomy with Complete Mesocolic Excision for the Treatment of Colon Cancer: Perioperative Outcomes and 5-Year Survival in a Consecutive Series of 202 Patients. Ann. Surg. Oncol. 2018, 25, 3580–3586. [Google Scholar] [CrossRef] [PubMed]
- Ngu, J.C.-Y.; Ng, Y.Y.-R. Robotics confers an advantage in right hemicolectomy with intracorporeal anastomosis when matched against conventional laparoscopy. J. Robot. Surg. 2018, 12, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Yozgatli, T.K.; Aytac, E.; Ozben, V.; Bayram, O.; Gurbuz, B.; Baca, B.; Balik, E.; Hamzaoglu, I.; Karahasanoglu, T.; Bugra, D. Robotic Complete Mesocolic Excision Versus Conventional Laparoscopic Hemicolectomy for Right-Sided Colon Cancer. J. Laparoendosc. Adv. Surg. Tech. 2019, 29, 671–676. [Google Scholar] [CrossRef]
- Yang, Y.; Malakorn, S.; Zafar, S.N.; Nickerson, T.P.; Sandhu, L.; Chang, G.J. Superior Mesenteric Vein-First Approach to Robotic Complete Mesocolic Excision for Right Colectomy: Technique and Preliminary Outcomes. Dis. Colon Rectum 2019, 62, 894–897. [Google Scholar] [CrossRef] [PubMed]
- Esch, J.S.A.; Iosivan, S.-I.; Steinfurth, F.; Mahdi, A.; Förster, C.; Wilkens, L.; Nasser, A.; Sarikaya, H.; Benhidjeb, T.; Krüger, M. A standardized suprapubic bottom-to-up approach in robotic right colectomy: Technical and oncological advances for complete mesocolic excision (CME). BMC Surg. 2019, 19, 72. [Google Scholar] [CrossRef]
- Bae, S.U.; Yang, S.Y.; Min, B.S. Totally robotic modified complete mesocolic excision and central vascular ligation for right-sided colon cancer: Technical feasibility and mid-term oncologic outcomes. Int. J. Colorectal Dis. 2018, 34, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Ramachandra, C.; Sugoor, P.; Karjol, U.; Arjunan, R.; Altaf, S.; Patil, V.; Kumar, H.; Beesanna, G.; Abhishek, M. Robotic Complete Mesocolic Excision with Central Vascular Ligation for Right Colon Cancer: Surgical Technique and Short-term Outcomes. Indian J. Surg. Oncol. 2020, 11, 674–683. [Google Scholar] [CrossRef]
- Petz, W.; Bertani, E.; Borin, S.; Fiori, G.; Ribero, D.; Spinoglio, G. Fluorescence-guided D3 lymphadenectomy in robotic right colectomy with complete mesocolic excision. Int. J. Med. Robot. Comput. Assist. Surg. 2021, 17, eRCS2217. [Google Scholar] [CrossRef]
- Ceccarelli, G.; Costa, G.; Ferraro, V.; De Rosa, M.; Rondelli, F.; Bugiantella, W. Robotic or three-dimensional (3D) laparoscopy for right colectomy with complete mesocolic excision (CME) and intracorporeal anastomosis? A propensity score-matching study comparison. Surg. Endosc. 2021, 35, 2039–2048. [Google Scholar] [CrossRef]
- Larach, J.T.; Rajkomar, A.K.S.; Narasimhan, V.; Kong, J.; Smart, P.J.; Heriot, A.G.; Warrier, S.K. Robotic complete mesocolic excision and central vascular ligation for right-sided colon cancer: Short-term outcomes from a case series. ANZ J. Surg. 2021, 91, 117–123. [Google Scholar] [CrossRef]
- Siddiqi, N.; Stefan, S.; Jootun, R.; Mykoniatis, I.; Flashman, K.; Beable, R.; David, G.; Khan, J. Robotic Complete Mesocolic Excision (CME) is a safe and feasible option for right colonic cancers: Short and midterm results from a single-centre experience. Surg. Endosc. 2021, 1–9. [Google Scholar] [CrossRef]
- Bianchi, P.P.; Salaj, A.; Giuliani, G.; Ferraro, L.; Formisano, G. Feasibility of robotic right colectomy with complete mesocolic excision and intracorporeal anastomosis: Short-term outcomes of 161 consecutive patients. Updates Surg. 2021, 73, 1065–1072. [Google Scholar] [CrossRef]
- Fleshman, J.; Sargent, D.J.; Green, E.; Anvari, M.; Stryker, S.J.; Beart, R.W.; Hellinger, M.; Flanagan, R.; Peters, W.; Nelson, H. Laparoscopic Colectomy for Cancer Is Not Inferior to Open Surgery Based on 5-Year Data From the COST Study Group Trial. Ann. Surg. 2007, 246, 655–664. [Google Scholar] [CrossRef]
- Buunen, M.; Veldkamp, R.; Hop, W.C.J.; Kuhry, E.; Jeekel, J.; Haglind, E.; Pahlman, L.; Cuesta, M.A.; Msika, S.; Morino, M.; et al. Survival after laparoscopic surgery versus open surgery for colon cancer: Long-term outcome of a randomised clinical trial. Lancet Oncol. 2009, 10, 44–52. [Google Scholar] [CrossRef]
- Green, B.L.; Marshall, H.; Collinson, F.; Quirke, P.; Guillou, P.; Jayne, D.G.; Brown, J.M. Long-term follow-up of the Medical Research Council CLASICC trial of conventional versus laparoscopically assisted resection in colorectal cancer. BJS 2012, 100, 75–82. [Google Scholar] [CrossRef]
- Bae, S.U.; Saklani, A.P.; Lim, D.R.; Kim, D.W.; Hur, H.; Min, B.S.; Baik, S.H.; Lee, K.Y.; Kim, N.K. Laparoscopic-Assisted Versus Open Complete Mesocolic Excision and Central Vascular Ligation for Right-Sided Colon Cancer. Ann. Surg. Oncol. 2014, 21, 2288–2294. [Google Scholar] [CrossRef]
- Storli, K.E.; Søndenaa, K.; Furnes, B.; Eide, G.E. Outcome after Introduction of Complete Mesocolic Excision for Colon Cancer Is Similar for Open and Laparoscopic Surgical Treatments. Dig. Surg. 2013, 30, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Athanasiou, C.; Markides, G.A.; Kotb, A.; Xia, X.; Gonsalves, S.; Miskovic, D. Open compared with laparoscopic complete mesocolic excision with central lymphadenectomy for colon cancer: A systematic review and meta-analysis. Colorectal Dis. 2016, 18. [Google Scholar] [CrossRef]
- Chow, C.F.K.; Kim, S.H. Laparoscopic complete mesocolic excision: West meets East. World J. Gastroenterol. 2014, 20, 14301–14307. [Google Scholar] [CrossRef] [PubMed]
- Spasojevic, M.; Stimec, B.V.; Dyrbekk, A.P.H.; Tepavcevic, Z.; Edwin, B.; Bakka, A.; Ignjatovic, D. Lymph Node Distribution in the D3 Area of the Right Mesocolon. Dis. Colon Rectum 2013, 56, 1381–1387. [Google Scholar] [CrossRef] [PubMed]
- Bertelsen, C.A.; Neuenschwander, A.U.; Jansen, J.E.; Kirkegaard-Klitbo, A.; Tenma, J.R.; Wilhelmsen, M.; Rasmussen, L.A.; Jepsen, L.V.; Kristensen, B.; Gögenur, I.; et al. Short-term outcomes after complete mesocolic excision compared with ‘conventional’ colonic cancer surgery. BJS 2016, 103, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Su, X.; He, Z.; Zhang, C.; Lu, J.; Zhang, G.; Sun, Y.; Du, X.; Chi, P.; Wang, Z.; et al. Short-term outcomes of complete mesocolic excision versus D2 dissection in patients undergoing laparoscopic colectomy for right colon cancer (RELARC): A randomised, controlled, phase 3, superiority trial. Lancet Oncol. 2021, 22, 391–401. [Google Scholar] [CrossRef]
- Waters, P.S.; Cheung, F.P.; Peacock, O.; Heriot, A.G.; Warrier, S.K.; O’Riordain, D.S.; Pillinger, S.; Lynch, A.C.; Stevenson, A.R.L. Successful patient-oriented surgical outcomes in robotic vs. laparoscopic right hemicolectomy for cancer—A systematic review. Colorectal Dis. 2020, 22, 488–499. [Google Scholar] [CrossRef]
- Sun, Z.; Kim, J.; Adam, M.A.; Nussbaum, D.P.; Speicher, P.J.; Mantyh, C.R.; Migaly, J. Minimally Invasive Versus Open Low Anterior Resection. Ann. Surg. 2016, 263, 1152–1158. [Google Scholar] [CrossRef]
- Trastulli, S.; Coratti, A.; Guarino, S.; Piagnerelli, R.; Annecchiarico, M.; Coratti, F.; Di Marino, M.; Ricci, F.; Desiderio, J.; Cirocchi, R.; et al. Robotic right colectomy with intracorporeal anastomosis compared with laparoscopic right colectomy with extracorporeal and intracorporeal anastomosis: A retrospective multicentre study. Surg. Endosc. 2015, 29, 1512–1521. [Google Scholar] [CrossRef]
- Morpurgo, E.; Contardo, T.; Molaro, R.; Zerbinati, A.; Orsini, C.; D’Annibale, A. Robotic-Assisted Intracorporeal Anastomosis Versus Extracorporeal Anastomosis in Laparoscopic Right Hemicolectomy for Cancer: A Case Control Study. J. Laparoendosc. Adv. Surg. Tech. 2013, 23, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Lujan, H.J.; Maciel, V.H.; Romero, R.; Plasencia, G. Laparoscopic versus robotic right colectomy: A single surgeon’s experience. J. Robot. Surg. 2011, 7, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Park, J.S.; Choi, G.; Park, S.Y.; Kim, H.J.; Ryuk, J.P. Randomized clinical trial of robot-assisted versus standard laparoscopic right colectomy. BJS 2012, 99, 1219–1226. [Google Scholar] [CrossRef] [PubMed]
- Chengwu, J.; Jin, C.; Hu, T.; Wei, M.; Wang, Z. Intracorporeal Versus Extracorporeal Anastomosis in Laparoscopic Right Colectomy: A Systematic Review and Meta-Analysis. J. Laparoendosc. Adv. Surg. Tech. 2017, 27, 348–357. [Google Scholar] [CrossRef]
- Ricci, C.; Casadei, R.; Alagna, V.; Zani, E.; Taffurelli, G.; Pacilio, C.A.; Minni, F. A critical and comprehensive systematic review and meta-analysis of studies comparing intracorporeal and extracorporeal anastomosis in laparoscopic right hemicolectomy. Langenbeck’s Arch. Surg. 2017, 402, 417–427. [Google Scholar] [CrossRef]
- Emile, S.H.; Elfeki, H.; Shalaby, M.; Sakr, A.; Bassuni, M.; Christensen, P.; Wexner, S.D. Intracorporeal versus extracorporeal anastomosis in minimally invasive right colectomy: An updated systematic review and meta-analysis. Tech. Coloproctol. 2019, 23, 1023–1035. [Google Scholar] [CrossRef]
- Benz, S.; Tannapfel, A.; Tam, Y.; Grünenwald, A.; Vollmer, S.; Stricker, I. Proposal of a new classification system for complete mesocolic excison in right-sided colon cancer. Tech. Coloproctol. 2019, 23, 251–257. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author | Year | Type of Study (Retrosp./Prosp.) | Type of Study (Comp./Non Comp.) | Pat. N | Conversion Rate | Mortality | Leaks | OS | DFS |
|---|---|---|---|---|---|---|---|---|---|
| Trastulli [22] | 2013 | retrospective | non comparative | 20 | 0 | 0 | 0 | nd | nd |
| Petz [23] | 2017 | retrospective | non comparative | 20 | 0 | 0 | 0 | nd | nd |
| Spinoglio [24] | 2018 | retrospective | comparative | 202 | 0 | 1% | 1% | 77% (5 years) | 85% (5 years) |
| Ngu [25] | 2018 | retrospective | comparative | 23 | 0 | nd | nd | nd | nd |
| Yozgatli [26] | 2019 | prospective | comparative | 96 | 0 | nd | 0 | nd | nd |
| Yang [27] | 2019 | retrospective | non comparative | 66 | 1.5% | 0 | 0 | nd | nd |
| Shulte am Esch [28] | 2019 | retrospective | non comparative | 31 | 0 | 0 | 0 | nd | nd |
| Bae [29] | 2019 | retrospective | non comparative | 43 | 0 | 0 | 2.3% | 93.6% (55 months) | 81.1% (55 months) |
| Ramachandra [30] | 2020 | retrospective | non comparative | 52 | 3.84% | 0 | 1.92% | nd | nd |
| Petz [31] | 2020 | retrospective | non comparative | 50 | 0 | 0 | 2% | nd | nd |
| Ceccarelli [32] | 2020 | retrospective | comparative | 55 | 0 | 0 | 0 | nd | nd |
| Larach [33] | 2021 | retrospective | non comparative | 20 | 0 | 0 | 0 | nd | nd |
| Siddiqui [34] | 2021 | retrospective | non comparative | 77 | 0 | 0 | 0 | 94% (3 years) | 94% (3 years) |
| Bianchi [35] | 2021 | retrospective | non comparative | 161 | 3.7% | 0 | 0.6% | nd | nd |
| Author | Type of Study | NOS | Overall Risk of Biases |
|---|---|---|---|
| Trastulli [22] | non comparative | 7 (S4, C1, O2) | low |
| Petz [23] | non comparative | 7 (S4, C1, O2) | low |
| Spinoglio [24] | comparative | 6 (S2, C1, E3) | high |
| Ngu [25] | comparative | 6 (S2, C1, E3) | high |
| Yozgatli [26] | comparative | 6 (S2, C1, E3) | high |
| Yang [27] | non comparative | 7 (S4, C1, O2) | low |
| Shulte am Esch [28] | non comparative | 7 (S4, C1, O2) | low |
| Bae [29] | non comparative | 8 (S4, C1, O3) | low |
| Ramachandra [30] | non comparative | 7 (S4, C1, O2) | low |
| Petz [31] | non comparative | 7 (S4, C1, O2) | low |
| Ceccarelli [32] | comparative | 6 (S2, C1, E3) | high |
| Larach [33] | non comparative | 7 (S4, C1, O2) | low |
| Siddiqui [34] | non comparative | 8 (S4, C1, O3) | low |
| Bianchi [35] | non comparative | 7 (S4, C1, O2) | low |
| Surgical Approach | |||||
|---|---|---|---|---|---|
| Medial-to-Lateral | Bottom-Up | Top-to-Down | SMV First | p | |
| Pat. n. | 329 | 328 | 96 | 163 | |
| Op. time (median, min) | 248 | 238 | 286 | 180 | 0.07 * |
| Conversions (median) | 0.9% | 0.6% | 0 | 0.6% | 0.88 ° |
| Postop. compl (median, Dindo III–IV) | 3.8% | 5.1% | 3% | 1.8% | 0.18 ° |
| Harvested LN (median) | 24 | 34 | 41 | 33 | 0.15 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petz, W.; Borin, S.; Fumagalli Romario, U. Updates on Robotic CME for Right Colon Cancer: A Qualitative Systematic Review. J. Pers. Med. 2021, 11, 550. https://doi.org/10.3390/jpm11060550
Petz W, Borin S, Fumagalli Romario U. Updates on Robotic CME for Right Colon Cancer: A Qualitative Systematic Review. Journal of Personalized Medicine. 2021; 11(6):550. https://doi.org/10.3390/jpm11060550
Chicago/Turabian StylePetz, Wanda, Simona Borin, and Uberto Fumagalli Romario. 2021. "Updates on Robotic CME for Right Colon Cancer: A Qualitative Systematic Review" Journal of Personalized Medicine 11, no. 6: 550. https://doi.org/10.3390/jpm11060550