
The Orthopedic-Vascular Multidisciplinary Approach Improves Patient Safety in Surgery for Musculoskeletal Tumors: A Large-Volume Center Experience

 ,
,  and
and 
Abstract
:1. Introduction
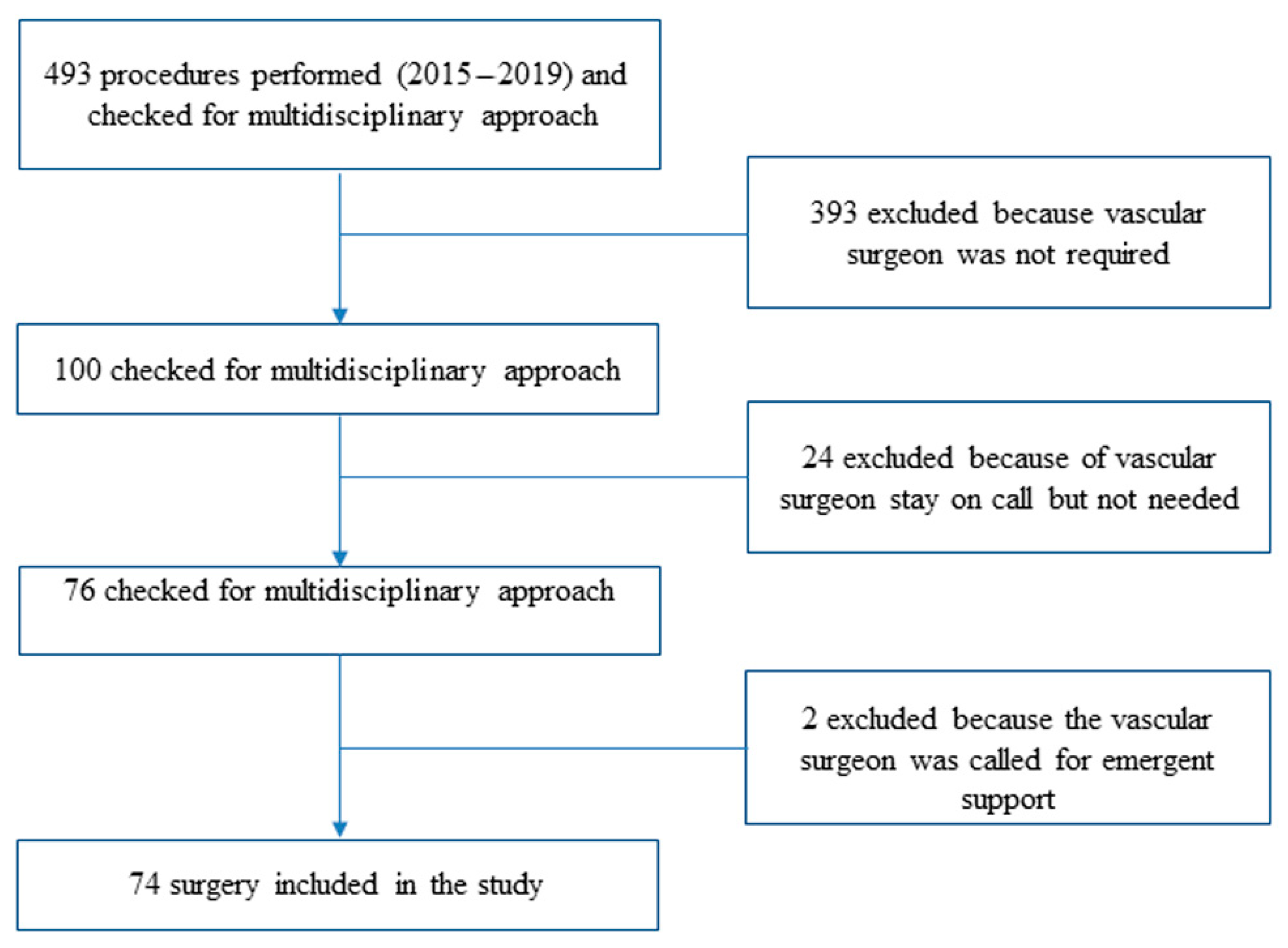
2. Materials and Methods
3. Results
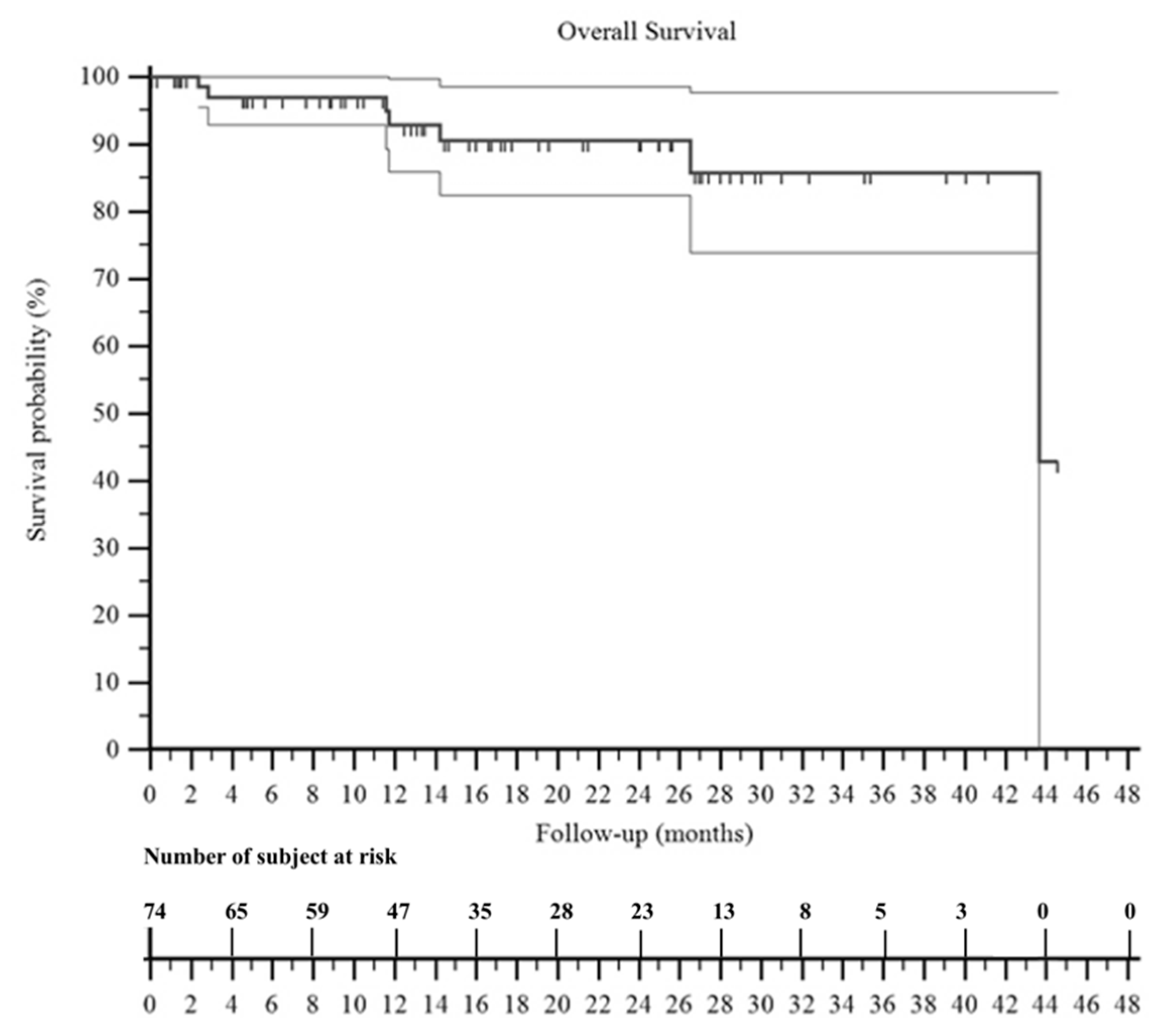
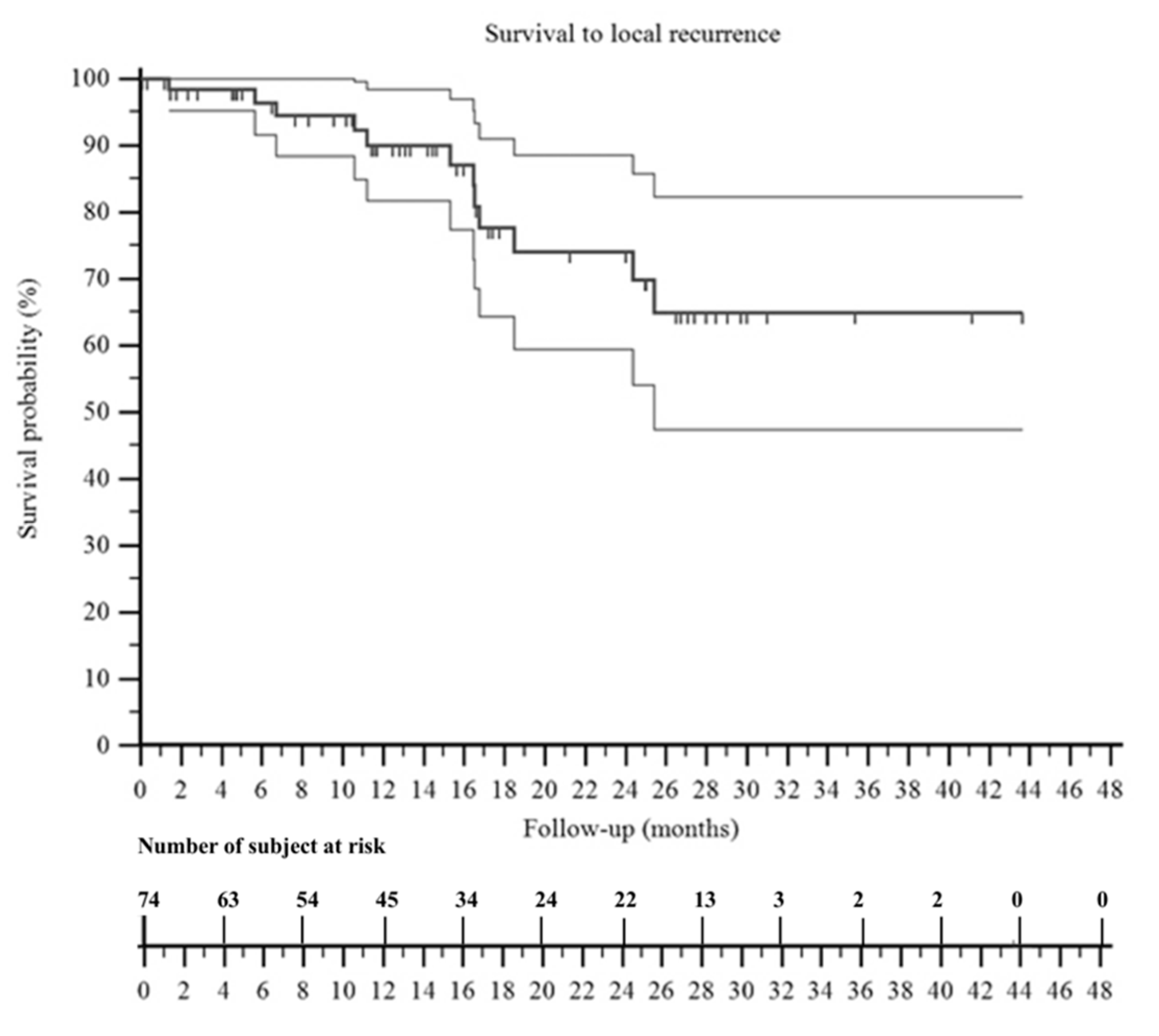
3.1. Oncological Outcome
3.2. Complication Rate
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mavrogenis, A.F.; Angelini, A.; Errani, C.; Rimondi, E. How should musculoskeletal biopsies be performed? Orthopedics 2014, 37, 585–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blakely, M.L.; Spurbeck, W.W.; Pappo, A.S.; Pratt, C.B.; Rodriguez-Galindo, C.; Santana, V.M.; Merchant, T.E.; Prichard, M.; Rao, B.N. The impact of margin of resection on outcome in pediatric nonrhabdomyosarcoma soft tissue sarcoma. J. Pediatr. Surg. 1999, 34, 672–675. [Google Scholar] [CrossRef]
- Davis, A.M.; Kandel, R.A.; Wunder, J.S.; Unger, R.; Meer, J.; O’Sullivan, B.; Catton, C.N.; Bell, R.S. The impact of residual disease on local recurrence in patients treated by initial unplanned resection for soft tissue sarcoma of the extremity. J. Surg. Oncol. 1997, 66, 81–87. [Google Scholar] [CrossRef]
- Campanacci, M. Bone and Soft Tissue Tumors: Clinical Features, Imaging, Pathology and Treatment; Springer: New York, NY, USA, 1999; pp. 1–70. [Google Scholar]
- Mogannam, A.C.; Chavez de Paz, C.; Sheng, N.; Patel, S.; Bianchi, C.; Chiriano, J.; Teruya, T.; Abou-Zamzam, A.M., Jr. Early vascular consultation in the setting of oncologic resections: Benefit for patients and a continuing source of open vascular surgical training. Ann. Vasc. Surg. 2015, 29, 810–815. [Google Scholar] [CrossRef]
- Manzur, M.F.; Ham, S.W.; Elsayed, R.; Abdoli, S.; Simcox, T.; Han, S.; Rowe, V.; Weaver, F.A. Vascular surgery: An essential hospital resource in modern health care. J. Vasc. Surg. 2017, 65, 1786–1792. [Google Scholar] [CrossRef] [Green Version]
- Awad, N.; Lackman, R.; McMackin, K.; Kim, T.W.; Lombardi, J.; Caputo, F. Multidisciplinary Approach to Treatment of Soft Tissue Sarcomas Requiring Complex Oncologic Resections. Ann. Vasc. Surg. 2018, 53, 212–216. [Google Scholar] [CrossRef]
- Clavien, P.A.; Sanabria, J.R.; Strasberg, S.M. Proposed classification of complications of surgery with examples of utility in cholecystectomy. Surgery 1992, 111, 518–526. [Google Scholar]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Enneking, W.F. A system of staging musculoskeletal neoplasms. Clin. Orthop. Relat. Res. 1986, 204, 9–24. [Google Scholar] [CrossRef]
- Wittekind, C.; Compton, C.; Quirke, P.; Nagtegaal, I.; Merkel, S.; Hermanek, P.; Sobin, L.H. A uniform residual tumor (R) classification: Integration of the R classification and the circumferential margin status. Cancer 2009, 115, 3483–3488. [Google Scholar] [CrossRef]
- Schwarzbach, M.H.; Hormann, Y.; Hinz, U.; Bernd, L.; Willeke, F.; Mechtersheimer, G.; Böckler, D.; Schumacher, H.; Herfarth, C.; Büchler, M.W.; et al. Results of limb-sparing surgery with vascular replacement for soft tissue sarcoma in the lower extremity. J. Vasc. Surg. 2005, 42, 88–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angelini, A.; Tiengo, C.; Sonda, R.; Berizzi, A.; Bassetto, F.; Ruggieri, P. One-Stage Soft Tissue Reconstruction Following Sarcoma Excision: A Personalized Multidisciplinary Approach Called “Orthoplasty”. J. Pers. Med. 2020, 10, 278. [Google Scholar] [CrossRef] [PubMed]
- Poultsides, G.A.; Tran, T.B.; Zambrano, E.; Janson, L.; Mohler, D.G.; Mell, M.W.; Avedian, R.S.; Visser, B.C.; Lee, J.T.; Ganjoo, K.; et al. Sarcoma Resection With and Without Vascular Reconstruction: A Matched Case-control Study. Ann. Surg. 2015, 262, 632–640. [Google Scholar] [CrossRef] [Green Version]
- Davis, L.A.; Dandachli, F.; Turcotte, R.; Steinmetz, O.K. Limb-sparing surgery with vascular reconstruction for malignant lower extremity soft tissue sarcoma. J. Vasc. Surg. 2017, 65, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Radaelli, S.; Fiore, M.; Colombo, C.; Ford, S.; Palassini, E.; Sanfilippo, R.; Stacchiotti, S.; Sangalli, C.; Morosi, C.; Casali, P.G.; et al. Vascular resection en-bloc with tumor removal and graft reconstruction is safe and effective in soft tissue sarcoma (STS) of the extremities and retroperitoneum. Surg. Oncol. 2016, 25, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Tsukushi, S.; Nishida, Y.; Sugiura, H.; Nakashima, H.; Ishiguro, N. Results of limb-salvage surgery with vascular reconstruction for soft tissue sarcoma in the lower extremity: Comparison between only arterial and arterovenous reconstruction. J. Surg. Oncol. 2008, 97, 216–220. [Google Scholar] [CrossRef]
- Fortner, J.G.; Kim, D.K.; Shiu, M.H. Limb-preserving vascular surgery for malignant tumors of the lower extremity. Arch. Surg. 1977, 112, 391–394. [Google Scholar] [CrossRef] [PubMed]
- Hohenberger, P.; Allenberg, J.R.; Schlag, P.M.; Reichardt, P. Results of surgery and multimodal therapy for patients with soft tissue sarcoma invading to vascular structures. Cancer 1999, 85, 396–408. [Google Scholar] [CrossRef]
- Bianchi, C.; Ballard, J.L.; Bergan, J.H.; Killeen, J.D. Vascular reconstruction and major resection for malignancy. Arch. Surg. 1999, 134, 851–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umezawa, H.; Sakuraba, M.; Miyamoto, S.; Nagamatsu, S.; Kayano, S.; Taji, M. Analysis of immediate vascular reconstruction for lower-limb salvage in patients with lower-limb bone and soft-tissue sarcoma. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 608–616. [Google Scholar] [CrossRef] [PubMed]
- Faenza, A.; Ferraro, A.; Gigli, M.; De Paolis, M.; Errani, C.; Mercuri, M. Vascular homografts for vessel substitution in skeletal and soft tissue sarcomas of the limbs. Transplant. Proc. 2005, 37, 2692–2693. [Google Scholar] [CrossRef]
- Bonardelli, S.; Nodari, F.; Maffeis, R.; Ippolito, V.; Saccalani, M.; Lussardi, L.; Giulini, S. Limb salvage in lower-extremity sarcomas and technical details about vascular reconstruction. J. Orthop. Sci. 2000, 5, 555–560. [Google Scholar] [CrossRef]
- Wortmann, M.; Alldinger, I.; Böckler, D.; Ulrich, A.; Hyhlik-Dürr, A. Vascular reconstruction after retroperitoneal and lower extremity sarcoma resection. Eur. J. Surg. Oncol. 2017, 43, 407–415. [Google Scholar] [CrossRef] [PubMed]
- McKay, A.; Motamedi, M.; Temple, W.; Mack, L.; Moore, R. Vascular reconstruction with the superficial femoral vein following major oncologic resection. J. Surg. Oncol. 2007, 96, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Muramatsu, K.; Ihara, K.; Miyoshi, T.; Yoshida, K.; Taguchi, T. Clinical outcome of limb-salvage surgery after wide resection of sarcoma and femoral vessel reconstruction. Ann. Vasc. Surg. 2011, 25, 1070–1077. [Google Scholar] [CrossRef]
- Kawai, A.; Hashizume, H.; Inoue, H.; Uchida, H.; Sano, S. Vascular reconstruction in limb salvage operations for soft tissue tumors of the extremities. Clin. Orthop. Relat. Res. 1996, 332, 215–222. [Google Scholar] [CrossRef]
- Baxter, B.T.; Mahoney, C.; Johnson, P.J.; Selmer, K.M.; Pipinos, I.I.; Rose, J.; Neff, J.R. Concomitant arterial and venous reconstruction with resection of lower extremity sarcomas. Ann. Vasc. Surg. 2007, 21, 272–279. [Google Scholar] [CrossRef]
- Adelani, M.A.; Holt, G.E.; Dittus, R.S.; Passman, M.A.; Schwartz, H.S. Revascularization after segmental resection of lower extremity soft tissue sarcomas. J. Surg. Oncol. 2007, 95, 455–460. [Google Scholar] [CrossRef]
- Karakousis, C.P.; Karmpaliotis, C.; Driscoll, D.L. Major vessel resection during limb-preserving surgery for soft tissue sarcomas. World J. Surg. 1996, 20, 345–349. [Google Scholar] [CrossRef]
- Koperna, T.; Teleky, B.; Vogl, S.; Windhager, R.; Kainberger, F.; Schatz, K.D.; Kotz, R.; Polterauer, P. Vascular reconstruction for limb salvage in sarcoma of the lower extremity. Arch. Surg. 1996, 131, 1103–1107. [Google Scholar] [CrossRef]
- Nishinari, K.; Krutman, M.; Aguiar Junior, S.; Pignataro, B.S.; Yazbek, G.; Zottele, B.G.A.; Teivelis, M.P.; Wolosker, N. Surgical outcomes of vascular reconstruction in soft tissue sarcomas of the lower extremities. J. Vasc. Surg. 2015, 62, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Leggon, R.E.; Huber, T.S.; Scarborough, M.T. Limb salvage surgery with vascular reconstruction. Clin. Orthop. Relat. Res. 2001, 387, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Park, D.; Cho, S.; Han, A.; Choi, C.; Ahn, S.; Min, S.I.; Ha, J.; Min, S.K. Outcomes after Arterial or Venous Reconstructions in Limb Salvage Surgery for Extremity Soft Tissue Sarcoma. J. Korean Med. Sci. 2018, 33, e265. [Google Scholar] [CrossRef]
- Enneking, W.F.; Dunham, W.; Gebhardt, M.C.; Malawar, M.; Pritchard, D.J. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin. Orthop. Relat. Res. 1993, 286, 241–246. [Google Scholar] [CrossRef]
- Ruggieri, P.; Mavrogenis, A.F.; Mercuri, M. Quality of life following limb-salvage surgery for bone sarcomas. Expert Rev. Pharmacoecon. Outcomes Res. 2011, 11, 59–73. [Google Scholar] [CrossRef]
- Ghert, M.A.; Davis, A.M.; Griffin, A.M.; Alyami, A.H.; White, L.; Kandel, R.A.; Ferguson, P.; O’Sullivan, B.; Catton, C.N.; Lindsay, T.; et al. The surgical and functional outcome of limb-salvage surgery with vascular reconstruction for soft tissue sarcoma of the extremity. Ann. Surg. Oncol. 2005, 12, 1102–1110. [Google Scholar] [CrossRef] [PubMed]
- Akgül, T.; Sormaz, İ.C.; Aksoy, M.; Uçar, A.; Özger, H.; Eralp, L. Results and functional outcomes of en-bloc resection and vascular reconstruction in extremity musculoskeletal tumors. Acta Orthop. Traumatol. Turc. 2018, 52, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Emori, M.; Hamada, K.; Omori, S.; Joyama, S.; Tomita, Y.; Hashimoto, N.; Takami, H.; Naka, N.; Yoshikawa, H.; Araki, N. Surgery with vascular reconstruction for soft-tissue sarcomas in the inguinal region: Oncologic and functional outcomes. Ann. Vasc. Surg. 2012, 26, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Cetinkaya, O.A.; Celik, S.U.; Kalem, M.; Basarir, K.; Koksoy, C.; Yildiz, H.Y. Clinical Characteristics and Surgical Outcomes of Limb-Sparing Surgery with Vascular Reconstruction for Soft Tissue Sarcomas. Ann. Vasc. Surg. 2019, 56, 73–80. [Google Scholar] [CrossRef]
- Haubner, F.; Ohmann, E.; Pohl, F.; Strutz, J.; Gassner, H.G. Wound healing after radiation therapy: Review of the literature. Radiat. Oncol. 2012, 7, 162. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data | Patients (n) | % |
|---|---|---|
| Age (mean years) | 46 (range, 9–88) | - |
| Gender (male/female) | 37/37 | - |
| Obesity | 16 | 21.6 |
| Hypertension | 15 | 20.3 |
| Smoking | 13 | 17.6 |
| Dyslipidemia | 6 | 8.1 |
| Type II diabetes | 4 | 5.4 |
| Peripheral arterial disease | 4 | 5.4 |
| Coronary artery disease | 1 | 1.4 |
| Previous deep vein thrombosis | 3 | 4.1 |
| >1 cardiovascular risk factors | 45 | 60.8 |
| American Society of Anesthesiologists (ASA) Score 1 | 14 | 18.9 |
| American Society of Anesthesiologists (ASA) Score 2 | 45 | 60.8 |
| American Society of Anesthesiologists (ASA) Score 3 | 15 | 20.3 |
| Bone tumors | 54 | 73 |
| Symptoms: | ||
| Pain | 38 | 70.4 |
| Swelling | 8 | 14.8 |
| Functional limitation | 9 | 16.7 |
| Pathological fracture | 7 | 13 |
| Asymptomatic | 9 | 16.7 |
| Histological diagnosis: | ||
| Osteosarcoma | 19 | 35.1 |
| Chondrosarcoma | 16 | 29.6 |
| Ewing’s sarcoma | 3 | 5.6 |
| Chordoma | 1 | 1.9 |
| Metastatic bone disease | 11 | 20.4 |
| Hematological malignancies | 4 | 7.4 |
| Site: | ||
| Proximal tibia | 15 | 27.8 |
| Proximal femur | 12 | 22.2 |
| Pelvis/sacrum | 9 | 16.7 |
| Distal femur | 9 | 16.7 |
| Proximal humerus | 6 | 11.1 |
| Scapula | 1 | 1.9 |
| Humeral shaft | 1 | 1.9 |
| Proximal tibia/distal tibia | 1 | 1.9 |
| Soft tissue tumors | 20 | 27 |
| Symptoms: | ||
| Mass/Swelling | 13 | 65 |
| Pain | 8 | 40 |
| Functional limitation | 2 | 10 |
| Asymptomatic | 3 | 15 |
| Histological diagnosis: | ||
| Synovial sarcoma | 7 | 35 |
| Leiomyosarcoma | 2 | 10 |
| Liposarcoma | 2 | 10 |
| Pleomorphic sarcoma | 2 | 10 |
| Other | 7 | 35 |
| Site: | ||
| Thigh | 9 | 45 |
| Popliteal fossa | 3 | 15 |
| Hip | 2 | 10 |
| Buttocks | 2 | 10 |
| Forearm | 2 | 10 |
| Knee | 1 | 5 |
| Pelvis | 1 | 5 |
| Metastases at time of surgery (bone and soft tissue tumors) | 10 | 13.5 |
| Lung metastases: | 9 | 12.2 |
| Skip metastases | 1 | 1.4 |
| Data | * Postop | Early | Late | N. Events/n. pts | Relative % ** | Absolute % °° |
|---|---|---|---|---|---|---|
| Grade I | 15/17 | 42.50% | 22.90% | |||
| Edema of the limb (13) | 7 | 6 | - | |||
| Delayed wound healing (4) | 4 | - | - | |||
| Grade II | 16/13 | 32.50% | 17.60% | |||
| Subtotal bypass occlusion (2) | - | 2 | - | |||
| Superficial infection (2) | 1 | 1 | - | |||
| Wound dehiscence and partial necrosis (5) | 4 | 1 | - | |||
| Sieroma or haematoma (2) | - | 2 | - | |||
| Deep vein thrombosis (4) | 2 | 2 | - | |||
| Periprosthetic fracture with cast (1) | - | - | 1 | |||
| Grade III | 28/22 | 55% | 29.70% | |||
| Deep hematoma or sieroma (5) | 4 | 1 | - | |||
| Complete wound dehiscence (11) | 7 | 3 | 1 | |||
| Wound necrosis and infection (4) | 2 | 2 | - | |||
| Active bleeding (1) | 1 | - | - | |||
| Deep infection (6) | 2 | - | 4 | |||
| Prosthetic dislocation (1) | - | - | 1 | |||
| Grade IV | 2 | 5% | 2.70% | |||
| Myocardial infarction (1) | 1 | - | - | |||
| Systemic sepsis (1) | - | 1 | - | |||
| Grade V | - | - | - | - | -% | -% |
| Variables | Cut Off n. Events/pts Hazard Ratio (95%CI) | Cut Off n. Events/pts Hazard Ratio (95% CI) | p-Value |
|---|---|---|---|
| Age | <65 years | >65 years | 0.9641 |
| 17/57 (29.8%) | 5/17 (29.4%) | ||
| HR 1.0231 | HR 0.9775 | ||
| Gender | Female | Male | 0.0914 |
| 14/37 (37.8%) | 8/37 (21.6%) | ||
| HR 2.0658 | HR 0.4841 | ||
| Cardiovascular risk factors | Yes | No | 0.8347 |
| 13/45 (28.9%) | 9/29 (31.0%) | ||
| HR 0.9124 | HR 1.0960 | ||
| Type 2 diabetes mellitus | Yes | No | 0.7487 |
| 1/4 (25.0%) | 21/70 (30.0%) | ||
| HR 1.3288 | HR 0.7526 | ||
| Obesity | Yes | No | 0.1726 |
| 5/16 (31.2%) | 17/58 (29.3%) | ||
| HR 2.0448 | HR 0.8547 | ||
| Preoperative radiotherapy | Yes | No | 0.1 |
| 8/16 (50.0%) | 14/58 (24.1%) | ||
| HR 2.3397 | HR 0.4274 | ||
| Neoplasia volume | <100 mL | >100 mL | 0.6754 |
| 12/38 (31.6%) | 10/36 (27.8%) | ||
| HR 1.1961 | HR 0.8360 | ||
| Intervention time | Less 4 h | >4 h | 0.0364 * |
| 6/35 (17.1%) | 16/39 (41.0%) | ||
| HR 0.4083 | HR 2.4491 | ||
| Vascular bypass | Yes | No | 0.2772 |
| 4/9 (44.4%) | 18/65 (27.7%) | ||
| HR 2.1040 | HR 0.4753 | ||
| Flap (yes vs. no) | Yes | No | 0.2984 |
| 8/21 (38.1%) | 14/53 (26.4%) | ||
| HR 1.6540 | HR 0.6046 | ||
| Tumor site (pelvis vs. other sites) | Pelvis | Other sites | 0.0564 * |
| 6/10 (60.0%) | 16/64 (25.0%) | ||
| HR 3.0753 | HR 0.3252 |
| Variables | Odds ratio | C.I. 95% | p-Value |
|---|---|---|---|
| Age (<65 years) | 1.4684 | 0.2550–8.4556 | p = 0.6671 |
| Gender (F) | 2.3379 | 0.6725–8.1272 | p = 0.1816 |
| Cardiovascular risk factors | 1.4685 | 0.3449–6.2517 | p = 0.6032 |
| Type 2 diabetes mellitus | 1.4414 | 0.0613–33.8653 | p = 0.8204 |
| Obesity | 2.3910 | 0.1913–29.8893 | p = 0.4988 |
| Preoperative radiotherapy | 4.7287 | 1.0535–21.2256 | p = 0.0426 * |
| Tumor volume > 100 mL | 1.2882 | 0.3609–4.5978 | p = 0.6965 |
| Surgical time > 4 h | 2.0073 | 0.4204–9.5837 | p = 0.3823 |
| Vascular bypass | 1.8550 | 0.2875–11.9707 | p = 0.5160 |
| Flap reconstruction | 3.2670 | 0.7090–15.0548 | p = 0.1288 |
| Site (pelvis) | 10.6054 | 1.4601–77.0316 | p = 0.0196 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angelini, A.; Piazza, M.; Pagliarini, E.; Trovarelli, G.; Spertino, A.; Ruggieri, P. The Orthopedic-Vascular Multidisciplinary Approach Improves Patient Safety in Surgery for Musculoskeletal Tumors: A Large-Volume Center Experience. J. Pers. Med. 2021, 11, 462. https://doi.org/10.3390/jpm11060462
Angelini A, Piazza M, Pagliarini E, Trovarelli G, Spertino A, Ruggieri P. The Orthopedic-Vascular Multidisciplinary Approach Improves Patient Safety in Surgery for Musculoskeletal Tumors: A Large-Volume Center Experience. Journal of Personalized Medicine. 2021; 11(6):462. https://doi.org/10.3390/jpm11060462
Chicago/Turabian StyleAngelini, Andrea, Michele Piazza, Elisa Pagliarini, Giulia Trovarelli, Andrea Spertino, and Pietro Ruggieri. 2021. "The Orthopedic-Vascular Multidisciplinary Approach Improves Patient Safety in Surgery for Musculoskeletal Tumors: A Large-Volume Center Experience" Journal of Personalized Medicine 11, no. 6: 462. https://doi.org/10.3390/jpm11060462