
Highly Cancellous Titanium Alloy (TiAl6V4) Surfaces on Three-Dimensionally Printed, Custom-Made Intercalary Tibia Prostheses: Promising Short- to Intermediate-Term Results


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Characteristics
2.2. Indication
- Primary malignant bone tumor of the diaphysis and metaphysis of the distal tibia;
- Remaining bone stock in the distal tibia excluded use of off-the-shelf intercalary tibial megaendoprosthetic implants and stems;
- Absence of comorbidities affecting bone and wound healing, such as diabetes mellitus, peripheral artery occlusive disease, or positive smoking history;
- Patient consent to undergo this reconstruction rather than below-knee amputation or other biological reconstruction.
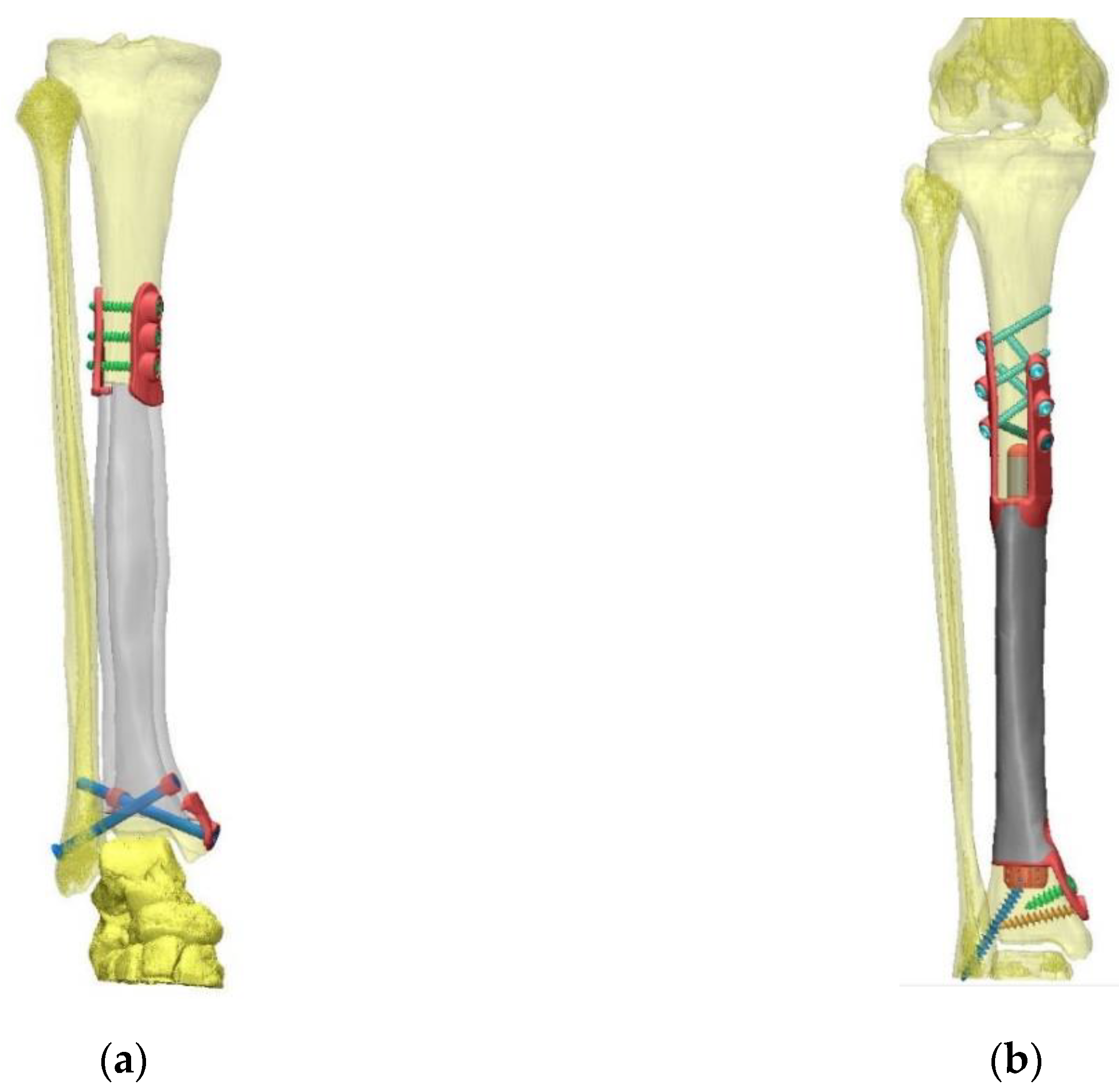
2.3. Pre-Operative Planning and Production
2.4. Implant Properties and Highly Cancellous Implant Surface (EPORE®, Implantcast, Buxtehude, Germany)
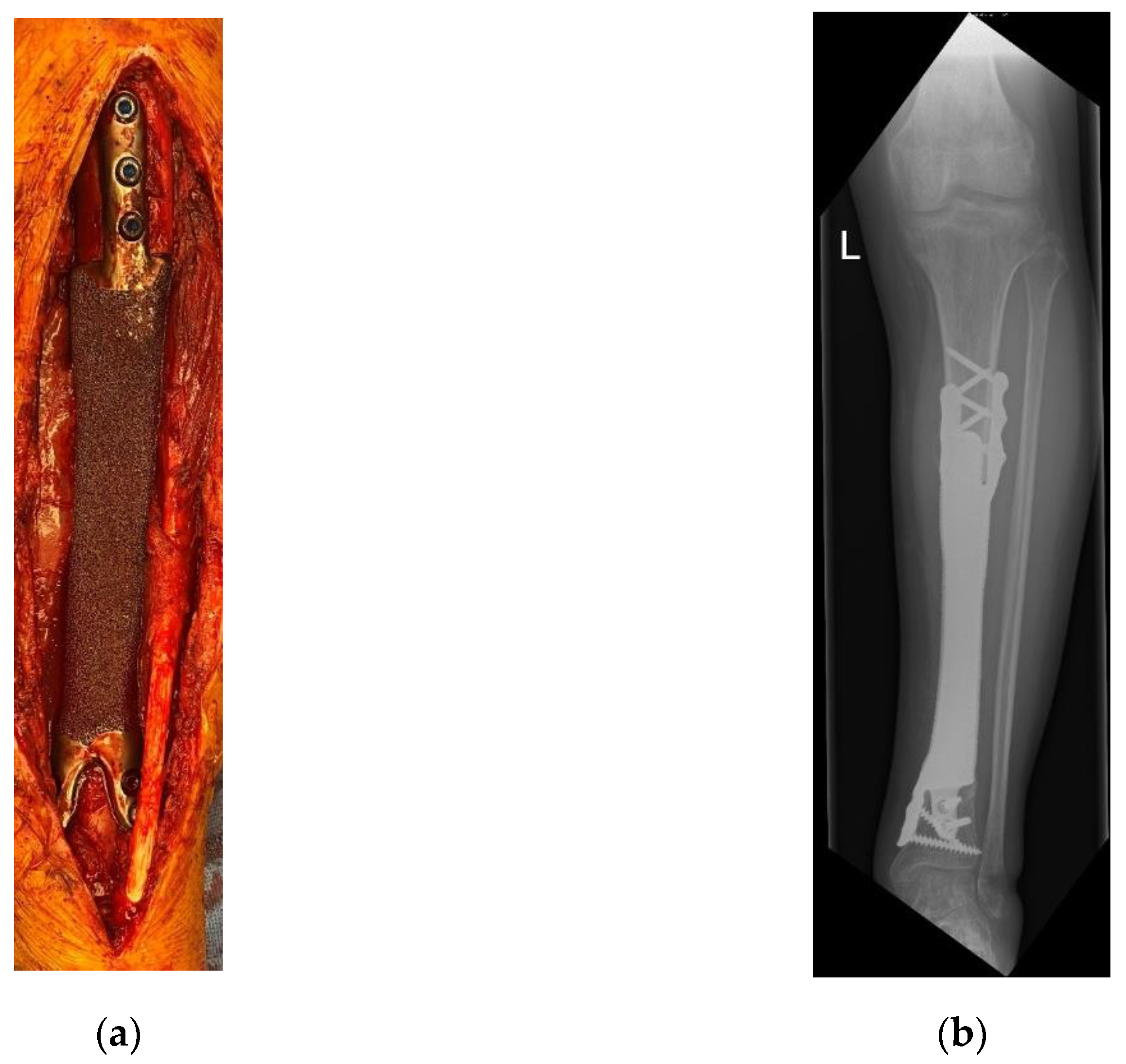
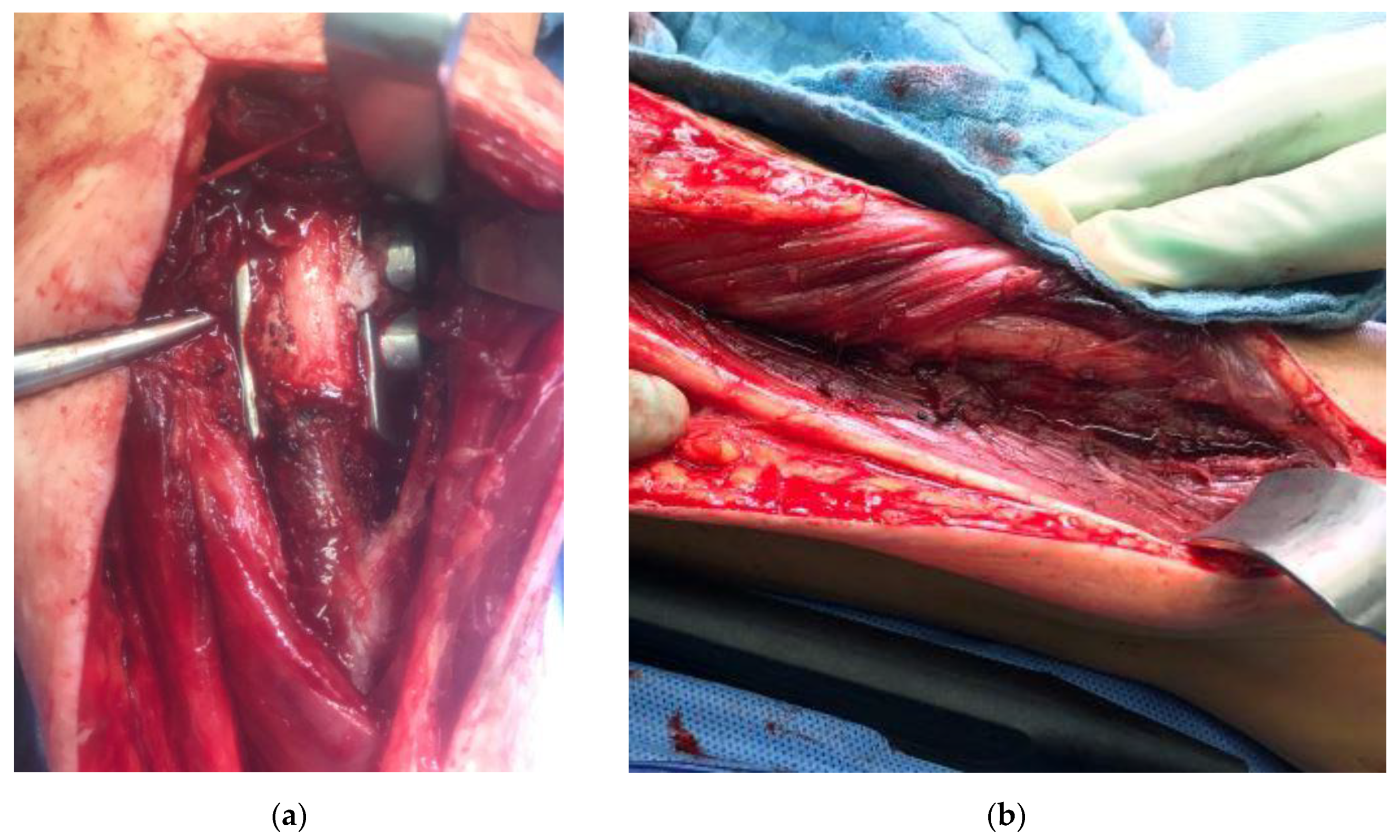
2.5. Surgical Technique
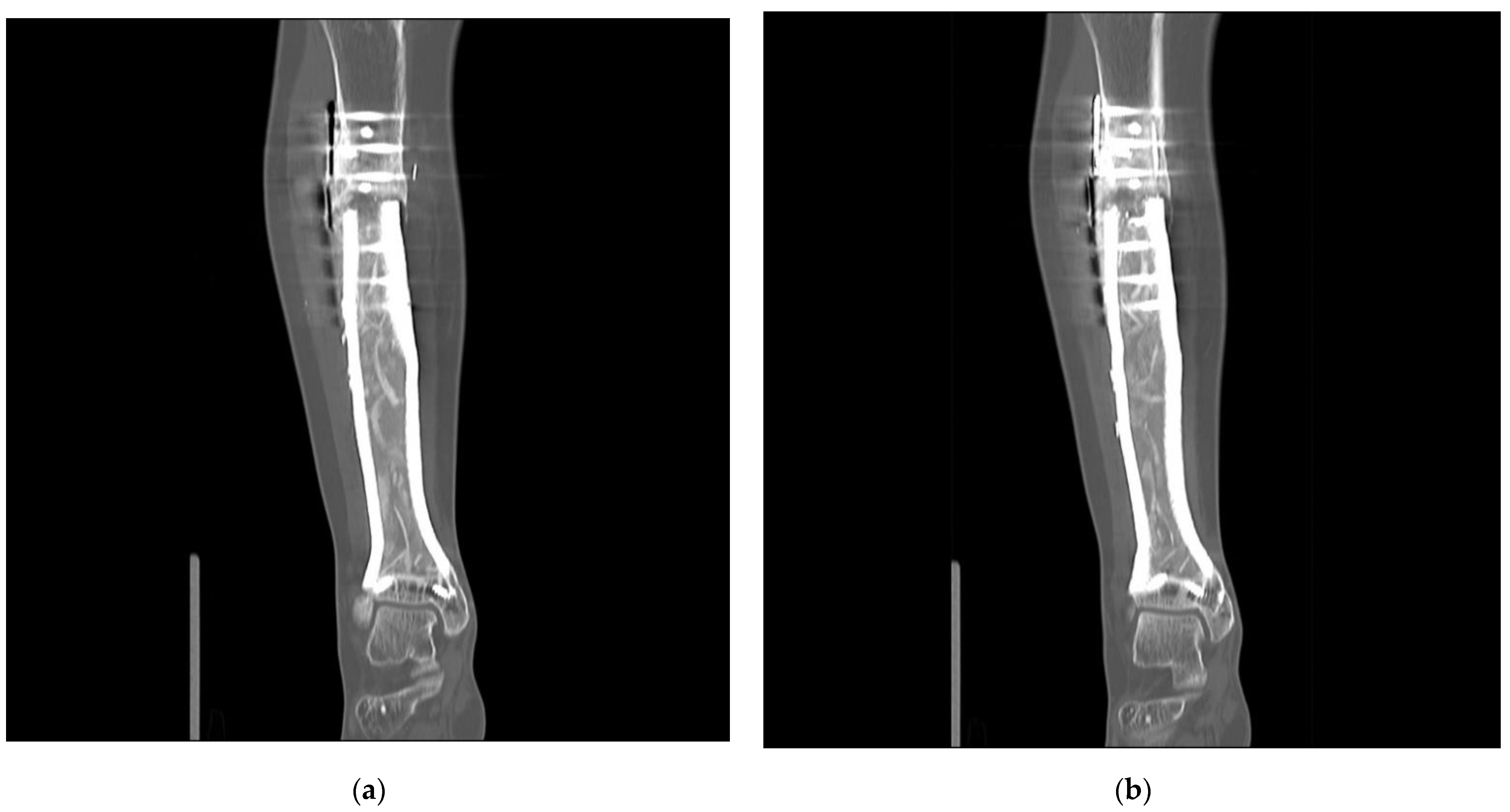
2.6. Bone Ingrowth
2.7. Complication Assessment
2.8. Functional Assessment
3. Results
3.1. Bone Ingrowth
3.2. Soft Tissue Ingrowth
3.3. Complications
3.4. Functional Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hardes, J.; Guder, W.; Dudda, M.; Nottrott, M.; Podleska, L.-E.; Streitbürger, A. Aktuelle Ergebnisse der Tumorendoprothetik bei Jugendlichen und Erwachsenen. Orthopäde 2019, 48, 744–751. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Evans, S.; Khan, Z.; Abudu, A.; Jeys, L.; Grimer, R. Reconstruction of the Distal Tibia Following Resection of Aggressive Bone Tumours Using a Custom-made Megaprosthesis. J. Orthop. 2017, 14, 406–409. [Google Scholar] [CrossRef] [PubMed]
- Shekkeris, A.S.; Hanna, S.A.; Sewell, M.D.; Spiegelberg, B.G.I.; Aston, W.J.S.; Blunn, G.W.; Cannon, S.R.; Briggs, T.W.R. Endoprosthetic Reconstruction of the Distal Tibia and Ankle Joint after Resection of Primary Bone Tumours. J. Bone Jt. Surgery. Br. Vol. 2009, 91, 1378–1382. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Yan, T.; Guo, W.; Yang, R.; Tang, X.; Wang, W. Surgical Options and Reconstruction Strategies for Primary Bone Tumors of Distal Tibia: A Systematic Review of Complications and Functional Outcome. J. Bone Oncol. 2019, 14, 100209. [Google Scholar] [CrossRef]
- Abudu, A.; Grimer, R.J.; Tillman, R.M.; Carter, S.R. Endoprosthetic Replacement of the Distal Tibia and Ankle Joint for Aggressive Bone Tumours. Int. Orthop. 1999, 23, 291–294. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.H.; Kim, H.-S.; Park, Y.-B.; Rhie, T.-Y.; Lee, H.K. Prosthetic Reconstruction for Tumours of the Distal Tibia and Fibula. J. Bone Jt. Surgery. Br. Vol. 1999, 81, 803–807. [Google Scholar] [CrossRef]
- Natarajan, M.V.; Annamalai, K.; Williams, S.; Selvaraj, R.; Rajagopal, T.S. Limb Salvage in Distal Tibial Osteosarcoma Using a Custom Mega Prosthesis. Int. Orthop. 2000, 24, 282–284. [Google Scholar] [CrossRef] [Green Version]
- Feng, D.; He, J.; Zhang, C.; Wang, L.; Gu, X.; Guo, Y. 3D-Printed Prosthesis Replacement for Limb Salvage after Radical Resection of an Ameloblastoma in the Tibia with 1 Year of Follow Up: A Case Report. Yonsei Med J. 2019, 60, 882–886. [Google Scholar] [CrossRef]
- Angelini, A.; Kotrych, D.; Trovarelli, G.; Szafrański, A.; Bohatyrewicz, A.; Ruggieri, P. Analysis of Principles Inspiring Design of Three-dimensional-printed Custom-made Prostheses in Two Referral Centres. Int. Orthop. 2020, 44, 829–837. [Google Scholar] [CrossRef]
- Streitbürger, A.; Hardes, J.; Nottrott, M.; Guder, W.K. Reconstruction Survival of Segmental Megaendoprostheses: A Retrospective Analysis of 28 Patients Treated for Intercalary Bone Defects after Musculoskeletal Tumor Resections. Arch. Orthop. Trauma Surg. 2020, 1–16. [Google Scholar] [CrossRef]
- Fang, C.; Cai, H.; Kuong, E.; Chui, E.; Siu, Y.C.; Ji, T.; Drstvenšek, I. Surgical Applications of Three-dimensional Printing in the Pelvis and Acetabulum: From Models and Tools to Implants. Unfallchirurg 2019, 122, 278–285. [Google Scholar] [CrossRef] [Green Version]
- Crovace, A.M.; Lacitignola, L.; Forleo, D.M.; Staffieri, F.; Francioso, E.; Di Meo, A.; Becerra, J.; Crovace, A.; Santos-Ruiz, L. 3D Biomimetic Porous Titanium (Ti6Al4V ELI) Scaffolds for Large Bone Critical Defect Reconstruction: An Experimental Study in Sheep. Animals 2020, 10, 1389. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.J.; Wang, Z.; Bai, H.; Li, J.M.; Cai, H. A Preliminary Study on Investigating the Attachment of Soft Tissue onto Micro-arc Oxidized Titanium Alloy Implants. Biomed. Mater. 2009, 4, 015017. [Google Scholar] [CrossRef] [PubMed]
- Pala, E.; Trovarelli, G.; Calabrò, T.; Angelini, A.; Abati, C.N.; Ruggieri, P. Survival of Modern Knee Tumor Megaprostheses: Failures, Functional Results, and a Comparative Statistical Analysis. Clin. Orthop. Relat. Res. 2015, 473, 891–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enneking, W.F.; Dunham, W.; Gebhardt, M.C.; Malawar, M.; Pritchard, D.J. A System for the Functional Evaluation of Reconstructive Procedures After Surgical Treatment of Tumors of the Musculoskeletal System. Clin. Orthop. Relat. Res. 1993. [Google Scholar] [CrossRef]
- Davis, A.M.; Wright, J.G.; Williams, J.I.; Bombardier, C.; Griffin, A.; Bell, R.S. Development of a Measure of Physical Function for Patients with Bone and Soft Tissue Sarcoma. Qual. Life Res. 1996, 5, 508–516. [Google Scholar] [CrossRef] [PubMed]
- Jämsen, E.; Huhtala, H.; Puolakka, T.; Moilanen, T. Risk Factors for Infection after Knee Arthroplasty. JBJS 2009, 91, 38–47. [Google Scholar] [CrossRef]
- Peersman, G.; Laskin, R.; Davis, J.; Peterson, M. Infection in Total Knee Replacement: A Retrospective Review of 6489 Total Knee Replacements. Clin. Orthop. Relat. Res. 2001, 392, 15–23. [Google Scholar] [CrossRef]
- Hardes, J.; Von Eiff, C.; Streitbuerger, A.; Balke, M.; Budny, T.; Henrichs, M.P.; Hauschild, G.; Ahrens, H. Reduction of Periprosthetic Infection with Silver-coated Megaprostheses in Patients with Bone Sarcoma. J. Surg. Oncol. 2010, 101, 389–395. [Google Scholar] [CrossRef]
- McConoughey, S.J.; Howlin, R.; Granger, J.F.; Manring, M.M.; Calhoun, J.H.; Shirtliff, M.; Kathju, S.; Stoodley, P. Biofilms in Periprosthetic Orthopedic Infections. Futur. Microbiol. 2014, 9, 987–1007. [Google Scholar] [CrossRef] [Green Version]
- Cordero, J.; Munuera, L.; Folgueira, M. The Influence of the Chemical Composition and Surface of the Implant on Infection. INJ 1996, 27, S/C34–S/C37. [Google Scholar] [CrossRef]
- Tanaka, K.; Maehara, H.; Kanaya, F. Vascularized Fibular Graft for Bone Defects after Wide Resection of Musculoskeletal Tumors. J. Orthop. Sci. 2012, 17, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Khira, Y.M.; Badawy, H.A. Pedicled Vascularized Fibular Graft with Ilizarov External Fixator for Reconstructing a Large Bone Defect of the Tibia after Tumor Resection. J. Orthop. Traumatol. 2013, 14, 91–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donati, D.; Di Liddo, M.; Zavatta, M.; Manfrini, M.; Bacci, G.; Picci, P.; Capanna, R.; Mercuri, M. Massive Bone Allograft Reconstruction in High-grade Osteosarcoma. Clin. Orthop. Relat. Res. 2000, 377, 186–194. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| # | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Age (years) | 25 | 19 | 22 | 54 |
| Diagnosis | Adamantinoma | Ewing | Ewing | UPS |
| Grading | low-grade | high-grade | high-grade | high-grade |
| Resection length (mm) | 175 | 200 | 160 | 165 |
| Remaining distal tibia (mm) | 5 | 30 | 45 | 35 |
| Operation time (minutes) | NA | 210 | 125 | 106 |
| Margin (R) | 0 | 0 | 0 | 0 |
| Chemotherapy | - | + | + | + |
| Radiation | - | - | - | - |
| Complication | Non-union (proximal) | - | - | - |
| MSTS | 20 | 29 | 25 | 20 |
| TESS | 86 | 100 | 96 | 70 |
| Follow-up (months) | 52 | 18 | 10 | 5 |
| # | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Reconstruction Length (mm) | 175 | 200 | 160 | 165 |
| Implant body | hollow | solid | solid | solid |
| Proximal stem (mm) | none | Solid 14 × 20 | solid 14 × 28 | solid 11 × 25 |
| Proximal extracortical plates (mm) | ||||
| medial | 41 | 55 | 60 | 67 |
| lateral | 38 | 65 | 55 | 76 |
| Distal stem (mm) | none | none | none | hollow 20 × 10 |
| Distal extracortical plates (mm) | ||||
| medial | 12 | 25 | 38 | 28 |
| ventral | - | 18 | 28 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guder, W.K.; Hardes, J.; Nottrott, M.; Podleska, L.E.; Streitbürger, A. Highly Cancellous Titanium Alloy (TiAl6V4) Surfaces on Three-Dimensionally Printed, Custom-Made Intercalary Tibia Prostheses: Promising Short- to Intermediate-Term Results. J. Pers. Med. 2021, 11, 351. https://doi.org/10.3390/jpm11050351
Guder WK, Hardes J, Nottrott M, Podleska LE, Streitbürger A. Highly Cancellous Titanium Alloy (TiAl6V4) Surfaces on Three-Dimensionally Printed, Custom-Made Intercalary Tibia Prostheses: Promising Short- to Intermediate-Term Results. Journal of Personalized Medicine. 2021; 11(5):351. https://doi.org/10.3390/jpm11050351
Chicago/Turabian StyleGuder, Wiebke K., Jendrik Hardes, Markus Nottrott, Lars E. Podleska, and Arne Streitbürger. 2021. "Highly Cancellous Titanium Alloy (TiAl6V4) Surfaces on Three-Dimensionally Printed, Custom-Made Intercalary Tibia Prostheses: Promising Short- to Intermediate-Term Results" Journal of Personalized Medicine 11, no. 5: 351. https://doi.org/10.3390/jpm11050351