
Deep Learning-Based Prediction Model for Gait Recovery after a Spinal Cord Injury

Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Variables
2.3. Analysis
3. Results
3.1. Descriptive Statistics
3.2. Model Peformance
3.3. Vairable Importance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mayo Clinic. Spinal Cord Injury. Updated on 2 October 2021. Available online: https://www.mayoclinic.org/diseases-conditions/spinal-cord-injury/symptoms-causes/syc-20377890 (accessed on 1 November 2023).
- National Institute of Health. Spinal Cord Injury. Updated on 20 January 2023. Available online: https://www.ninds.nih.gov/health-information/disorders/spinal-cord-injury (accessed on 1 November 2023).
- Ding, W.; Hu, S.; Wang, P.; Kang, H.; Peng, R.; Dong, Y.; Li, F. Spinal cord injury: The global incidence, prevalence, and disability From the Global Burden of Disease Study 2019. Spine 2022, 47, 1532–1540. [Google Scholar] [CrossRef]
- Kim, H.K.; Leigh, J.H.; Choi, Y.; Lee, J.H.; Bang, M.S. Spinal cord injury fact sheet in Korea. Ann. Rehabil. Med. 2023, 47, 4–10. [Google Scholar] [CrossRef]
- Kawanishi, C.Y.; Greguol, M. Physical activity, quality of life, and functional autonomy of adults with spinal cord injuries. Adapt. Phys. Act. Q. 2013, 30, 317–337. [Google Scholar] [CrossRef]
- Burns, A.S.; Marino, R.J.; Kalsi-Ryan, S.; Middleton, J.W.; Tetreault, L.A.; Dettori, J.R.; Mihalovich, K.E.; Fehlings, M.G. Type and timing of rehabilitation following acute and subacute spinal cord injury: A systematic review. Glob. Spine J. 2017, 7, 175S–194S. [Google Scholar] [CrossRef] [PubMed]
- Scivoletto, G.; Tamburella, F.; Laurenza, L.; Torre, M.; Molinari, M. Who is going to walk? A review of the factors influencing walking recovery after spinal cord injury. Front. Hum. Neurosci. 2014, 8, 141. [Google Scholar] [CrossRef] [PubMed]
- van Middendorp, J.J.; Hosman, A.J.; Donders, A.R.; Pouw, M.H.; Ditunno, J.F., Jr.; Curt, A.; Geurts, A.C.; Van de Meent, H.; EM-SCI Study Group. A clinical prediction rule for ambulation outcomes after traumatic spinal cord injury: A longitudinal cohort study. Lancet 2011, 377, 1004–1010. [Google Scholar] [CrossRef] [PubMed]
- Hupp, M.; Pavese, C.; Bachmann, L.M.; Koller, R.; EMSCI Study Group; Schubert, M. Electrophysiological multimodal assessments improve outcome prediction in traumatic cervical spinal cord injury. J. Neurotrauma 2018, 35, 2916–2923. [Google Scholar] [CrossRef] [PubMed]
- Iseli, E.; Cavigelli, A.; Dietz, V.; Curt, A. Prognosis and recovery in ischaemic and traumatic spinal cord injury: Clinical and electrophysiological evaluation. J. Neurol. Neurosurg. Psychiatry 1999, 67, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Dietz, N.; Vaitheesh Jaganathan Alkin, V.; Mettille, J.; Boakye, M.; Drazin, D. Machine learning in clinical diagnosis, prognostication, and management of acute traumatic spinal cord injury (SCI): A systematic review. J. Clin. Orthop. Trauma 2022, 35, 102046. [Google Scholar] [CrossRef]
- DeVries, Z.; Hoda, M.; Rivers, C.S.; Maher, A.; Wai, E.; Moravek, D.; Stratton, A.; Kingwell, S.; Fallah, N.; Paquet, J.; et al. Development of an unsupervised machine learning algorithm for the prognostication of walking ability in spinal cord injury patients. Spine J. 2020, 20, 213–224. [Google Scholar] [CrossRef]
- Facchinello, Y.; Beauséjour, M.; Richard-Denis, A.; Thompson, C.; Mac-Thiong, J.M. Use of regression tree analysis for predicting the functional outcome after traumatic spinal cord injury. J. Neurotrauma 2021, 38, 1285–1291. [Google Scholar] [CrossRef] [PubMed]
- McCoy, D.B.; Dupont, S.M.; Gros, C.; Cohen-Adad, J.; Huie, R.J.; Ferguson, A.; Duong-Fernandez, X.; Thomas, L.H.; Singh, V.; Narvid, J.; et al. Talbott. Convolutional neural network–based automated segmentation of the spinal cord and contusion injury: Deep learning biomarker correlates of motor impairment in acute spinal cord injury. Am. J. Neuroradiol. 2019, 40, 737–744. [Google Scholar] [PubMed]
- Yu, Y.; Si, X.; Hu, C.; Zhang, J. A review of recurrent neural networks: LSTM cells and network architectures. Neural Comput. 2019, 31, 1235–1270. [Google Scholar] [CrossRef] [PubMed]
- Holden, M.K.; Gill, K.M.; Magliozzi, M.R.; Nathan, J.; Piehl-Baker, L. Clinical gait assessment in the neurologically impaired. Reliability and meaningfulness. Phys. Ther. 1984, 64, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.R.; Cadotte, D.W.; Fehlings, M.G. Clinical predictors of neurological outcome, functional status, and survival after traumatic spinal cord injury: A systematic review. J. Neurosurg. Spine 2012, 17 (Suppl. S1), 11–26. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.R.; Grossman, R.G.; Frankowski, R.F.; Kiss, A.; Davis, A.M.; Kulkarni, A.V.; Harrop, J.S.; Aarabi, B.; Vaccaro, A.; Tator, C.H.; et al. A clinical prediction model for long-term functional outcome after traumatic spinal cord injury based on acute clinical and imaging factors. J. Neurotrauma 2012, 29, 2263–2271. [Google Scholar] [CrossRef]
- Rupp, R.; Biering-Sørensen, F.; Burns, S.P.; Graves, D.E.; Guest, J.; Jones, L.; Read, M.S.; Rodriguez, G.M.; Schuld, C.; Tansey-Md, K.E.; et al. International Standards for Neurological Classification of Spinal Cord Injury: Revised 2019. Top. Spinal Cord Inj. Rehabil. 2021, 27, 1–22. [Google Scholar] [CrossRef]
- Wasiak, K.; Frasuńska, J.; Tarnacka, B. Can the Initial Parameters of Functional Scales Predict Recovery in Patients with Complete Spinal Cord Injury? A Retrospective Cohort Study. Diagnostics 2024, 14, 129. [Google Scholar] [CrossRef]
- Sharif, S.; Ali, M.Y.J. Outcome prediction in spinal cord injury: Myth or reality. World Neurosurg. 2020, 140, 574–590. [Google Scholar] [CrossRef]
- Hirota, R.; Terashima, Y.; Ohnishi, H.; Yamashita, T.; Yokogawa, N.; Sasagawa, T.; Kato, S. Prognostic factors for respiratory dysfunction for cervical spinal cord injury and/or cervical fractures in elderly patients: A multicenter survey. Glob. Spine J. 2024, 14, 101–112. [Google Scholar] [CrossRef]
- Khan, O.; Badhiwala, J.H.; Wilson, J.R.F.; Jiang, F.; Martin, A.R.; Fehlings, M.G. Predictive Modeling of Outcomes After Traumatic and Nontraumatic Spinal Cord Injury Using Machine Learning: Review of Current Progress and Future Directions. Neurospine 2019, 16, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Fallah, N.; Noonan, V.K.; Waheed, Z.; Rivers, C.S.; Plashkes, T.; Bedi, M.; Etminan, M.; Thorogood, N.P.; Ailon, T.; Chan, E.; et al. Development of a machine learning algorithm for predicting in-hospital and 1-year mortality after traumatic spinal cord injury. Spine J. 2022, 22, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Fan, G.; Yang, S.; Liu, H.; Xu, N.; Chen, Y.; He, J.; Su, X.; Pang, M.; Liu, B.; Han, L.; et al. Machine Learning-based Prediction of Prolonged Intensive Care Unit Stay for Critical Patients with Spinal Cord Injury. Spine 2022, 47, E390–E398. [Google Scholar] [CrossRef] [PubMed]
- Kato, C.; Uemura, O.; Sato, Y.; Tsuji, T. Functional Outcome Prediction After Spinal Cord Injury Using Ensemble Machine Learning. Arch. Phys. Med. Rehabil. 2024, 105, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Bransford, R.J.; Chapman, J.R.; Skelly, A.C.; VanAlstyne, E.M. What do we currently know about thoracic spinal cord injury recovery and outcomes? A systematic review. J. Neurosurg. Spine 2012, 17 (Suppl. S1), 52–64. [Google Scholar] [CrossRef] [PubMed]
- Nevin, A.N.; Steenson, J.; Vivanti, A.; Hickman, I.J. Investigation of measured and predicted resting energy needs in adults after spinal cord injury: A systematic review. Spinal Cord 2016, 54, 248–253. [Google Scholar] [CrossRef]
- AlHuthaifi, F.; Krzak, J.; Hanke, T.; Vogel, L.C. Predictors of functional outcomes in adults with traumatic spinal cord injury following inpatient rehabilitation: A systematic review. J. Spinal Cord Med. 2017, 40, 282–294. [Google Scholar] [CrossRef] [PubMed]
- Noller, C.M.; Groah, S.L.; Nash, M.S. Inflammatory stress effects on health and function after spinal cord injury. Top. Spinal Cord Inj. Rehabil. 2017, 23, 207–217. [Google Scholar] [CrossRef]
- Ikpeze, T.C.; Mesfin, A. Spinal cord injury in the geriatric population: Risk factors, treatment options, and long-term management. Geriatr. Orthop. Surg. Rehabil. 2017, 8, 115–118. [Google Scholar] [CrossRef]
- Yue, J.K.; Winkler, E.A.; Rick, J.W.; Deng, H.; Partow, C.P.; Upadhyayula, P.S.; Birk, H.S.; Chan, A.K.; Dhall, S.S. Update on critical care for acute spinal cord injury in the setting of polytrauma. Neurosurg. Focus 2017, 43, e19–e28. [Google Scholar] [CrossRef]
- Green, B.N.; Johnson, C.D.; Haldeman, S.; Griffith, E.; Clay, M.B.; Kane, E.J.; Castellote, J.M.; Rajasekaran, S.; Smuck, M.; Hurwitz, E.L.; et al. A scoping review of biopsychosocial risk factors and co-morbidities for common spinal disorders. PLoS ONE 2018, 13, e0197987–e0198015. [Google Scholar] [CrossRef] [PubMed]
- Silver, D.; Huang, A.; Maddison, C.J.; Guez, A.; Sifre, L.; van den Driessche, G.; Schrittwieser, J.; Antonoglou, I.; Panneershelvam, V.; Lanctot, M.; et al. Mastering the game of Go with deep neural networks and tree search. Nature 2016, 529, 484–489. [Google Scholar] [CrossRef] [PubMed]
- Hambly, B.; Xu, R.; Yang, H. Recent advances in reinforcement learning in finance. arXiv 2022, arXiv:2112.04553. [Google Scholar]
- Yu, C.; Liu, J.; Nemati, S. Reinforcement learning in healthcare: A survey. arXiv 2020, arXiv:1908.08796. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Min | 25% | 50% | 75% | Max | SD | Correlation |
|---|---|---|---|---|---|---|---|
| FAC_DC | 0 | 1 | 2 | 4 | 5 | 1.7 | 1.00 |
| Age | 38 | 52 | 64 | 74 | 98 | 15.8 | −0.03 |
| Period—Acute Care | 0 | 17 | 38 | 133 | 10,642 | 945.2 | −0.09 |
| Period—Rehab | 0 | 20 | 27 | 33 | 349 | 34.0 | −0.13 |
| Motor-UER | 0 | 17 | 24 | 25 | 25 | 6.5 | 0.30 |
| Motor-UEL | 0 | 17 | 23 | 25 | 25 | 6.7 | 0.32 |
| Motor-LER | 0 | 7 | 19 | 22 | 25 | 8.8 | 0.64 |
| Motor-LEL | 0 | 8 | 18 | 22 | 25 | 8.7 | 0.64 |
| Sensory-LTR | 2 | 32 | 44 | 55 | 56 | 12.0 | 0.38 |
| Sensory-LTL | 2 | 32 | 45 | 55 | 56 | 12.5 | 0.36 |
| Sensory-PPR | 0 | 33 | 45 | 56 | 56 | 13.1 | 0.40 |
| Sensory-PPL | 0 | 32 | 45 | 56 | 56 | 13.2 | 0.37 |
| Hip flexor,_Rt. | 0 | 2 | 3 | 4 | 5 | 1.7 | 0.65 |
| Knee extensor,_Rt. | 0 | 2 | 4 | 5 | 5 | 1.8 | 0.62 |
| Ankle dorsiflexor,_Rt. | 0 | 1 | 4 | 4 | 5 | 1.9 | 0.62 |
| Long toe extensor,_Rt. | 0 | 1 | 3 | 4 | 5 | 1.8 | 0.61 |
| Ankle plantarflexor,_Rt. | 0 | 2 | 4 | 5 | 5 | 1.8 | 0.61 |
| Hip flexor,_Lt. | 0 | 2 | 3 | 4 | 5 | 1.7 | 0.66 |
| Knee extensor,_Lt. | 0 | 2 | 4 | 5 | 5 | 1.8 | 0.63 |
| Ankle dorsiflexor,_Lt. | 0 | 1 | 4 | 4 | 5 | 1.9 | 0.63 |
| Long toe extensor,_Lt. | 0 | 1 | 4 | 4 | 5 | 1.8 | 0.62 |
| Ankle plantarflexor,_Lt. | 0 | 2 | 4 | 5 | 5 | 1.8 | 0.61 |
| LT_L1_Rt | 0 | 1 | 1 | 2 | 2 | 0.6 | 0.44 |
| LT_L2_Rt | 0 | 1 | 1 | 2 | 2 | 0.6 | 0.44 |
| LT_L3_Rt | 0 | 1 | 1 | 2 | 2 | 0.6 | 0.43 |
| LT_L4_Rt | 0 | 1 | 1 | 2 | 2 | 0.6 | 0.45 |
| LT_L5_Rt | 0 | 1 | 1 | 2 | 2 | 0.6 | 0.42 |
| LT_S1_Rt | 0 | 1 | 1 | 2 | 2 | 0.6 | 0.44 |
| LT_S2_Rt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.45 |
| LT_S3_Rt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.45 |
| LT_S4-5_Rt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.43 |
| LT_L1_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.41 |
| LT_L2_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.41 |
| LT_L3_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.40 |
| LT_L4_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.42 |
| LT_L5_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.39 |
| LT_S1_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.42 |
| LT_S2_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.42 |
| LT_S3_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.40 |
| LT_S4-5_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.38 |
| PP_L1_Rt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.43 |
| PP_L2_Rt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.45 |
| PP_L3_Rt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.46 |
| PP_L4_Rt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.46 |
| PP_L5_Rt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.45 |
| PP_S1_Rt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.47 |
| PP_S2_Rt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.47 |
| PP_S3_Rt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.46 |
| PP_S4-5_Rt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.44 |
| PP_L1_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.42 |
| PP_L2_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.42 |
| PP_L3_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.45 |
| PP_L4_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.45 |
| PP_L5_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.43 |
| PP_S1_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.45 |
| PP_S2_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.45 |
| PP_S3_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.44 |
| PP_S4-5_Lt | 0 | 1 | 1 | 2 | 2 | 0.7 | 0.42 |
| Initial FAC | 0 | 0 | 1 | 2 | 5 | 1.4 | 0.74 |
| All Participants (n = 405) | Participants with Traumatic SCI (n = 175) | Participants with Non-Traumatic SCI (n = 230) | ||
|---|---|---|---|---|
| FAC Included | Motor Included | |||
| RNN | 0.3738 | 0.3727 | 0.3728 | |
| Linear Regression | 2.3831 | 1.7176 | 1.7516 | |
| Ridge | 1.3161 | 1.3914 | 1.1012 | |
| Lasso | 1.0246 | 1.3524 | 0.8889 | |
| FAC Excluded | Motor Included | |||
| RNN | 0.3727 | 0.3727 | 0.3732 | |
| Linear Regression | 2.2952 | 2.1961 | 1.5994 | |
| Ridge | 1.4387 | 1.6006 | 1.2638 | |
| Lasso | 1.1107 | 1.6058 | 1.1576 | |
| FAC Included | Motor Upperexcluded | |||
| RNN | 0.3732 | 0.3727 | 0.3731 | |
| Linear Regression | 1.9811 | 1.6266 | 1.9296 | |
| Ridge | 1.2287 | 1.3526 | 1.1840 | |
| Lasso | 1.0387 | 1.2526 | 0.9177 | |
| FAC Included | Motor Excluded | |||
| RNN | 0.3727 | 0.3727 | 0.3728 | |
| Linear Regression | 1.2074 | 1.6294 | 1.8930 | |
| Ridge | 1.1506 | 1.3383 | 1.1870 | |
| Lasso | 1.0568 | 1.2258 | 0.9178 |
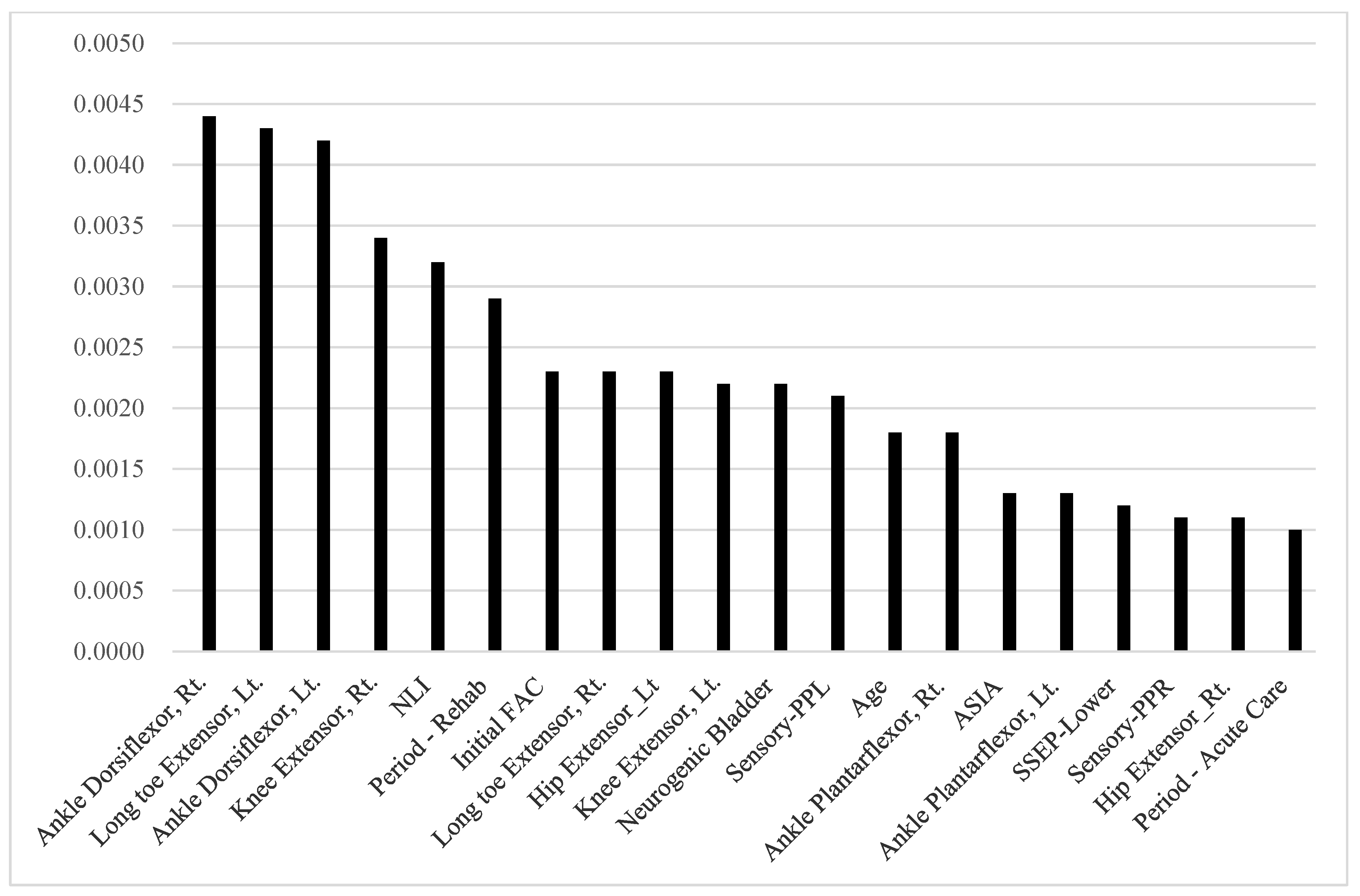
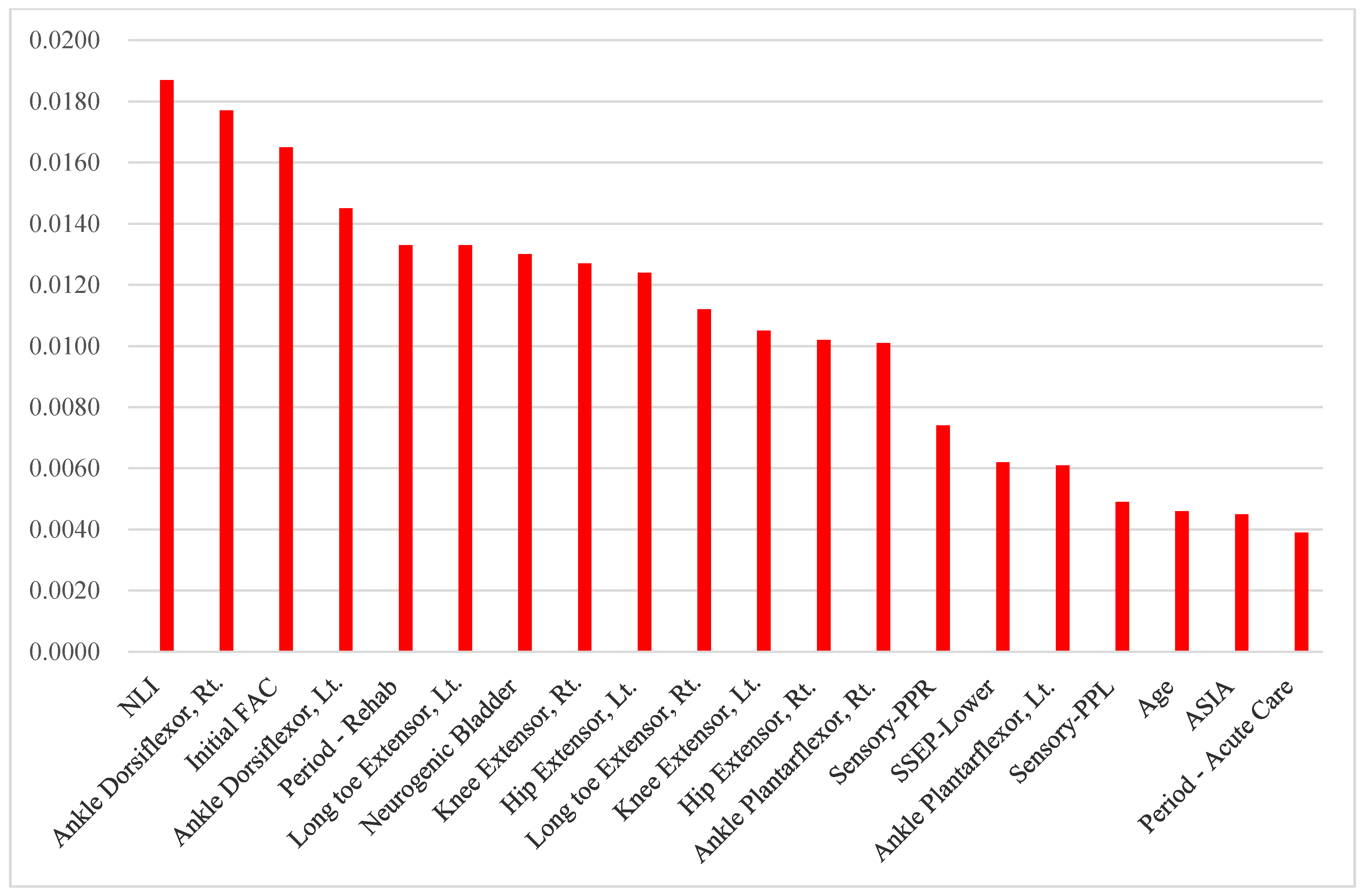
| Variable | All Participants (n = 405) | Participants with Traumatic SCI (n = 175) | Participants with Non-Traumatic SCI (n = 230) | |||
|---|---|---|---|---|---|---|
| VI | Ranking | VI | Ranking | VI | Ranking | |
| Age | 0.0018 | 13 | 0.0046 | 18 | 0.0124 | 13 |
| Period—Acute Care | 0.0010 | 20 | 0.0039 | 20 | 0.0059 | 20 |
| Period—Rehab | 0.0029 | 6 | 0.0133 | 5 | 0.0161 | 11 |
| AIS | 0.0013 | 15 | 0.0045 | 19 | 0.0099 | 18 |
| NLI | 0.0032 | 5 | 0.0187 | 1 | 0.0239 | 7 |
| Sensory-PPR | 0.0011 | 18 | 0.0074 | 14 | 0.0103 | 17 |
| Sensory-PPL | 0.0021 | 12 | 0.0049 | 17 | 0.0174 | 10 |
| Hip flexor, Rt. | 0.0011 | 18 | 0.0102 | 12 | 0.0113 | 14 |
| Knee extensor, Rt. | 0.0034 | 4 | 0.0127 | 8 | 0.0253 | 3 |
| Ankle dorsiflexor, Rt. | 0.0044 | 1 | 0.0177 | 2 | 0.0329 | 1 |
| Long toe extensor, Rt. | 0.0023 | 8 | 0.0112 | 10 | 0.0250 | 4 |
| Ankle plantarflexor, Rt. | 0.0018 | 13 | 0.0101 | 13 | 0.0087 | 19 |
| Hip flexor, Lt. | 0.0023 | 8 | 0.0124 | 9 | 0.0228 | 8 |
| Knee extensor, Lt. | 0.0022 | 10 | 0.0105 | 11 | 0.0152 | 12 |
| Ankle dorsiflexor, Lt. | 0.0042 | 3 | 0.0145 | 4 | 0.0262 | 2 |
| Long toe extensor, Lt. | 0.0043 | 2 | 0.0133 | 5 | 0.0246 | 5 |
| Ankle plantarflexor, Lt. | 0.0013 | 15 | 0.0061 | 16 | 0.0108 | 16 |
| Neurogenic Bladder | 0.0022 | 10 | 0.0130 | 7 | 0.0244 | 6 |
| Initial FAC | 0.0023 | 7 | 0.0165 | 3 | 0.0177 | 9 |
| SSEP-Lower | 0.0012 | 17 | 0.0062 | 15 | 0.0111 | 15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, H.-J.; Lee, K.-S.; Koo, B.; Yong, C.-W.; Kim, C.-W. Deep Learning-Based Prediction Model for Gait Recovery after a Spinal Cord Injury. Diagnostics 2024, 14, 579. https://doi.org/10.3390/diagnostics14060579
Yoo H-J, Lee K-S, Koo B, Yong C-W, Kim C-W. Deep Learning-Based Prediction Model for Gait Recovery after a Spinal Cord Injury. Diagnostics. 2024; 14(6):579. https://doi.org/10.3390/diagnostics14060579
Chicago/Turabian StyleYoo, Hyun-Joon, Kwang-Sig Lee, Bummo Koo, Chan-Woo Yong, and Chae-Won Kim. 2024. "Deep Learning-Based Prediction Model for Gait Recovery after a Spinal Cord Injury" Diagnostics 14, no. 6: 579. https://doi.org/10.3390/diagnostics14060579