
Imaging Techniques and Clinical Application of the Marrow–Blood Barrier in Hematological Malignancies
 ,
,
Abstract
:1. Introduction
2. Cellular Components and Function of the MBB
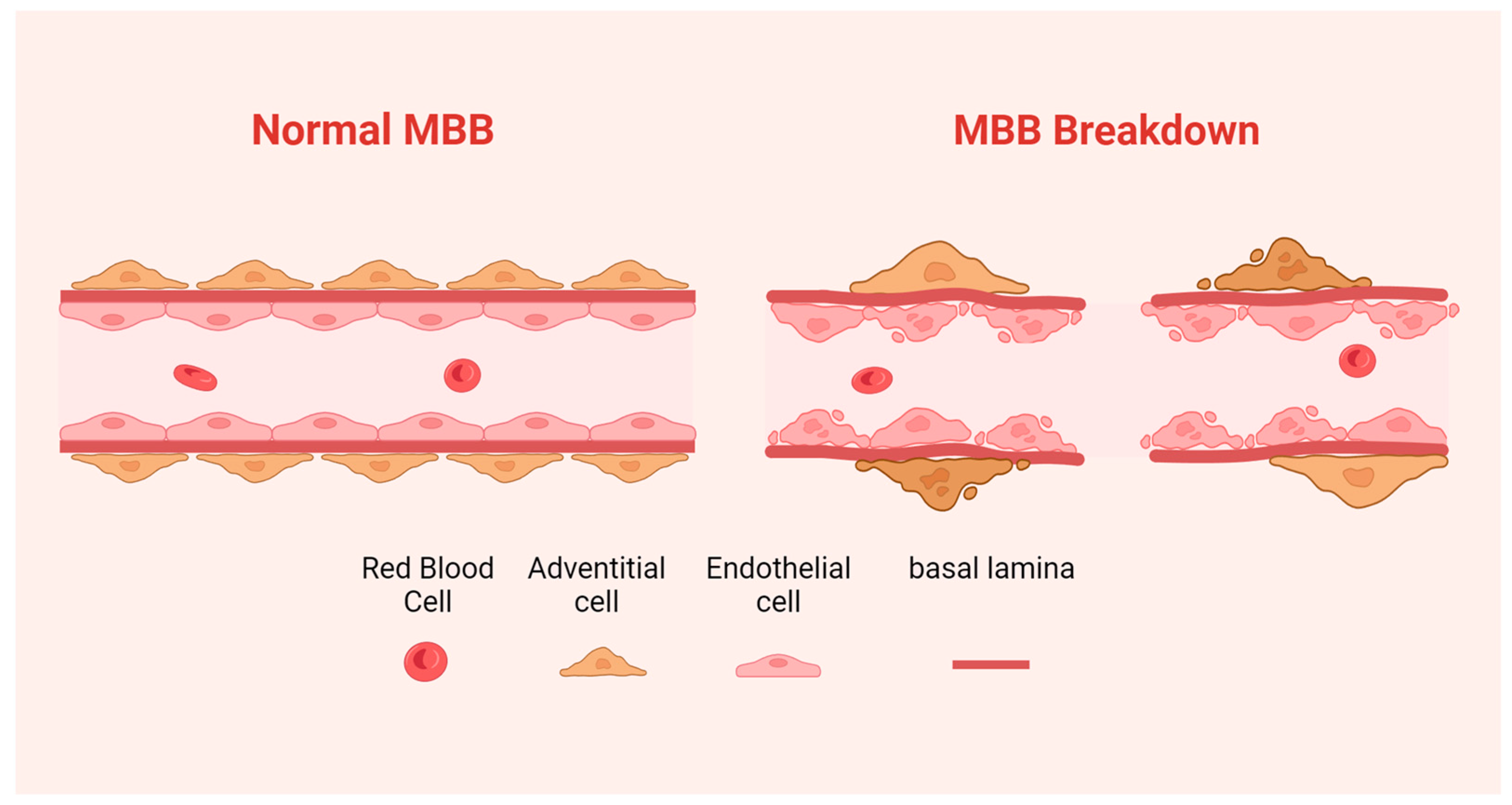
- The endothelial cells are located on the medial surface of the medullary sinus, and a large number of fenestrae make the medullary sinus communicate with the hematopoietic tissues outside the medullary sinus. Fenestrated structures within vascular endothelial cells in the medullary sinus possess the ability to expand, contract, or close [8], thereby influencing both the number and timing of mature blood cells released from the hematopoietic zone into the blood circulation. Under TEM, endothelial cells were found to be thin, and the attenuated cytoplasm varied in thickness and was occasionally interrupted by fenestrations of different sizes. Under SEM, the fenestrations can be divided into two categories by size: one category comprises larger fenestrations that allow for the migration of blood cells, while another category consists of smaller pores forming a cribriform plate through aggregation [9].
- Adventitial cells reside in the outermost layer of the medullary sinus, wrapping vascular endothelial cells and covering two-thirds of the surface area of vascular endothelial cells. Adventitial cells regulate the area covering vascular endothelial cells and control the fenestra size by shrinking the cell body and stretching the surface processes of vascular endothelial cells, which can cooperate with vascular endothelial cells to regulate the volume of the medullary sinus and the flow of blood cells into and out of the hematopoietic area [10,11]. Elongated cytoplasmic processes provide a framework for extravascular tissue [12].
- The basement membrane is composed primarily of laminin and a small amount of type II collagen, which are non-continuously distributed on the outer surface of vascular endothelial cells in the medullary sinus, as well as between reticular cells and vascular endothelial cells in the outer membrane, and can effectively regulate the exchange and entry of chemicals and cells inside and outside the medullary sinus.
2.1. Normal MBB
2.2. Abnormal MBB

{kind=link}
{kind=link}
| Components | Location | Morphology of Cells | Function | Functional Damage |
|---|---|---|---|---|
| Endothelial cells | On the internal surface. | Thin and flat, the two ends of the cell are tapered and form the thin portion [9]. | Regulate the number and timing of mature blood cells entering the blood circulation from the hematopoietic region [9]. | Large gaps or damaged zones appeared in the endothelium and the continuity was poor [20]. |
| Adventitial cells | On the outermost layer. | Showed a pyramidal shape whose top was protruded vertically into the myeloid tissue [9]. | Regulate the coverage area and control the size of endothelial cell fenestra [10,11]. | Adventitial cell cover rate was significantly reduced [21]. |
| Basement membrane | On the medial surface. | Basement membrane in the bone marrow sinus often discontinuous [9]. | Regulates the exchange and entry of chemicals and cells inside and outside the medullary sinus. | Basement membrane degeneration [20]. |
3. Assessment Methods of MBB
3.1. Search Strategy
3.2. DCE-MRI
3.2.1. Imaging Methods That Need Small Molecular Contrast Agents
3.2.2. Clinical Applications
- Leukemia
- 2.
- Multiple Myeloma
3.2.3. Imaging Methods That Need Macromolecular Contrast Agents
3.2.4. Clinical Applications
- Leukemia
- 2.
- Lymphomas
- 3.
- Total Body Irradiation
3.2.5. Advantages and Disadvantages
3.3. IVIM
3.3.1. Clinical Applications
3.3.2. Advantages and Disadvantages
3.4. ASL
3.4.1. Clinical Applications
3.4.2. Advantages and Disadvantages
3.5. BOLD-MRI
3.5.1. Advantages and Disadvantages
3.6. Other
3.6.1. Clinical Applications
3.6.2. Advantages and Disadvantages
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tavassoli, M. The marrow-blood barrier. Br. J. Haematol. 1979, 41, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Wagner, N.; Mott, K.; Upcin, B.; Stegner, D.; Schulze, H.; Ergün, S. CXCL12-Abundant Reticular (CAR) Cells Direct Megakaryocyte Protrusions across the Bone Marrow Sinusoid Wall. Cells 2021, 10, 722. [Google Scholar] [CrossRef] [PubMed]
- Ayala, F.; Dewar, R.; Kieran, M.; Kalluri, R. Contribution of bone microenvironment to leukemogenesis and leukemia progression. Leukemia 2009, 23, 2233–2241. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, J.K.; Lichtman, M.A. Marrow cell egress: Specificity of the site of penetration into the sinus. Blood 1978, 52, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Bianco, P. Bone and the hematopoietic niche: A tale of two stem cells. Blood 2011, 117, 5281–5288. [Google Scholar] [CrossRef] [PubMed]
- Pease, D.C. Marrow cells seen with the electron microscopy after ultrathin sectioning. Rev. Hematol. 1955, 10, 324–344. [Google Scholar]
- Wickramasinghe, S.N. Observations on the ultrastructure of sinusoids and reticular cells in human bone marrow. Clin. Lab. Haematol. 1991, 13, 263–278. [Google Scholar] [CrossRef] [PubMed]
- Lichtman, M.A.; Koury, M.J. Williams Hematology, 8th ed.; McGraw-Hill: New York, NY, USA, 2010; pp. 62–104. [Google Scholar]
- Muto, M. A scanning and transmission electron microscopic study on rat bone marrow sinuses and transmural migration of blood cells. Arch. Histol. Jpn. 1976, 39, 51–66. [Google Scholar] [CrossRef]
- Campbell, F.R. Ultrastructural studies of transmural migration of blood cells in the bone marrow of rats, mice and guinea pigs. Am. J. Anat. 1972, 135, 521–535. [Google Scholar] [CrossRef]
- Yamada, E. Scanning electron microscopy of the bone marrow. In Proceedings of the Tenth International Congress of Anatomists, Tokyo, Science Council of Japan, Tokyo, Japan, 25–30 August 1975; p. 362. [Google Scholar]
- Valdez, R.; Zutter, M.; Florea, A.D. Rubin’s Pathology: Clinicopathologic Foundations of Medicine, 6th ed.; Lippincott Williams & Wilkins: New York, NY, USA, 2012; pp. 947–1036. [Google Scholar]
- Lichtman, M.A. Cellular deformability during maturation of the myeloblast. Possible role in marrow egress. N. Engl. J. Med. 1970, 283, 943–948. [Google Scholar] [CrossRef]
- Lichtman, M.A.; Weed, R.I. Alteration of the cell periphery during granulocyte maturation: Relationship to cell function. Blood 1972, 39, 301–316. [Google Scholar] [CrossRef] [PubMed]
- Leblond, P.F.; LaCelle, P.L.; Weed, R.I. Cellular deformability: A possible determinant of the normal release of maturing erythrocytes from the bone marrow. Blood 1971, 37, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Shaklai, M.; Tavassoli, M. Endothelial cell membrane: Differences in the density of intramembranous particles between tissue- and blood-fronts revealed by freeze-fracture. Am. J. Anat. 1978, 151, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Hudson, G.; Yoffey, J.M. Ultrastructure of reticuloendothelial elements in guinea-pig bone marrow. J. Anat. 1968, 103, 515–525. [Google Scholar] [PubMed]
- De Bruyn, P.P.; Michelson, S.; Becker, R.P. Endocytosis, transfer tubules, and lysosomal activity in myeloid sinusoidal endothelium. J. Ultrastruct. Res. 1975, 53, 133–151. [Google Scholar] [CrossRef] [PubMed]
- Nagaoka, T.; Kuto, F.; Watanabe, Y.; Fujino, Y.; Hirasawa, Y.; Tokuhiro, H. Bone marrow sinus and cell egress in human leukaemia: A morphometric study of core biopsies using wide-field electron microscopy. Br. J. Haematol. 1986, 63, 737–747. [Google Scholar] [CrossRef]
- Chen, L.T.; Handler, E.E.; Handler, E.S.; Weiss, L. An electron microscopic study of the bone marrow of the rat in an experimental myelogenous leukemia. Blood 1972, 39, 99–112. [Google Scholar] [CrossRef]
- Petrides, P.E.; Dittmann, K.H. How do normal and leukemic white blood cells egress from the bone marrow? Morphological facts and biochemical riddles. Blut 1990, 61, 3–13. [Google Scholar] [CrossRef]
- Giordano, G.F.; Lichtman, M.A. Marrow cell egress. The central interaction of barrier pore size and cell maturation. J. Clin. Investig. 1973, 52, 1154–1164. [Google Scholar] [CrossRef]
- Carmeliet, P.; Jain, R.K. Molecular mechanisms and clinical applications of angiogenesis. Nature 2011, 473, 298–307. [Google Scholar] [CrossRef]
- Haouas, H. Angiogenesis and acute myeloid leukemia. Hematology 2014, 19, 311–323. [Google Scholar] [CrossRef] [PubMed]
- Carmeliet, P.; Jain, R.K. Angiogenesis in cancer and other diseases. Nature 2000, 407, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Passaro, D.; Di Tullio, A.; Abarrategi, A.; Rouault-Pierre, K.; Foster, K.; Ariza-McNaughton, L.; Montaner, B.; Chakravarty, P.; Bhaw, L.; Diana, G.; et al. Increased Vascular Permeability in the Bone Marrow Microenvironment Contributes to Disease Progression and Drug Response in Acute Myeloid Leukemia. Cancer Cell. 2017, 32, 324–341. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.B.; Hsu, C.Y.; Yu, C.W.; Liang, P.C.; Hsu, C.; Hsu, C.H.; Cheng, A.L.; Shih, T.T. Dynamic Contrast-enhanced MR Imaging of Advanced Hepatocellular Carcinoma: Comparison with the Liver Parenchyma and Correlation with the Survival of Patients Receiving Systemic Therapy. Radiology 2016, 281, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Carroll, T.J.; Ginat, D.T. Using Dynamic Contrast-enhanced MRI as an Imaging Biomarker for Migraine: Proceed with Caution. Radiology 2019, 292, 721–722. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Cho, N.; Park, I.A.; Kwon, B.R.; Shin, S.U.; Kim, S.Y.; Lee, S.H.; Chang, J.M.; Moon, W.K. Dynamic Contrast-enhanced Breast MRI for Evaluating Residual Tumor Size after Neoadjuvant Chemotherapy. Radiology 2018, 289, 327–334. [Google Scholar] [CrossRef]
- Oostendorp, M.; Post, M.J.; Backes, W.H. Vessel growth and function: Depiction with contrast-enhanced MR imaging. Radiology 2009, 251, 317–335. [Google Scholar] [CrossRef]
- Choyke, P.L.; Dwyer, A.J.; Knopp, M.V. Functional tumor imaging with dynamic contrast-enhanced magnetic resonance imaging. J. Magn. Reson. Imaging 2003, 17, 509–520. [Google Scholar] [CrossRef]
- Zha, Y.; Li, M.; Yang, J. Dynamic contrast enhanced magnetic resonance imaging of diffuse spinal bone marrow infiltration in patients with hematological malignancies. Korean J. Radiol. 2010, 11, 187–194. [Google Scholar] [CrossRef]
- Teo, Q.Q.; Thng, C.H.; Koh, T.S.; Ng, Q.S. Dynamic contrast-enhanced magnetic resonance imaging: Applications in oncology. Clin. Oncol. (R Coll Radiol.) 2014, 26, e9–e20. [Google Scholar] [CrossRef]
- Hansford, B.G.; Peng, Y.; Jiang, Y.; Vannier, M.W.; Antic, T.; Thomas, S.; McCann, S.; Oto, A. Dynamic Contrast-enhanced MR Imaging Curve-type Analysis: Is It Helpful in the Differentiation of Prostate Cancer from Healthy Peripheral Zone? Radiology 2015, 275, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Tofts, P.S.; Brix, G.; Buckley, D.L.; Evelhoch, J.L.; Henderson, E.; Knopp, M.V.; Larsson, H.B.; Lee, T.Y.; Mayr, N.A.; Parker, G.J.; et al. Estimating kinetic parameters from dynamic contrast-enhanced T(1)-weighted MRI of a diffusable tracer: Standardized quantities and symbols. J. Magn. Reson. Imaging 1999, 10, 223–232. [Google Scholar] [CrossRef]
- Maijer, K.I.; van der Leij, C.; de Hair, M.J.; Tas, S.W.; Maas, M.; Gerlag, D.M.; Tak, P.P.; Lavini, C. Dynamic Contrast-Enhanced Magnetic Resonance Imaging Using Pharmacokinetic Modeling: Initial Experience in Patients with Early Arthritis. Arthritis Rheumatol. 2016, 68, 587–596. [Google Scholar] [CrossRef] [PubMed]
- O'Connor, J.P.; Jackson, A.; Parker, G.J.; Jayson, G.C. DCE-MRI biomarkers in the clinical evaluation of antiangiogenic and vascular disrupting agents. Br. J. Cancer 2007, 96, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Tofts, P.S. Modeling tracer kinetics in dynamic Gd-DTPA MR imaging. J. Magn. Reson. Imaging 1997, 7, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Zwick, S.; Brix, G.; Tofts, P.S.; Strecker, R.; Kopp-Schneider, A.; Laue, H.; Semmler, W.; Kiessling, F. Simulation-based comparison of two approaches frequently used for dynamic contrast-enhanced MRI. Eur. Radiol. 2010, 20, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Testa, U.; Riccioni, R.; Militi, S.; Coccia, E.; Stellacci, E.; Samoggia, P.; Latagliata, R.; Mariani, G.; Rossini, A.; Battistini, A.; et al. Elevated expression of IL-3Ralpha in acute myelogenous leukemia is associated with enhanced blast proliferation, increased cellularity, and poor prognosis. Blood 2002, 100, 2980–2988. [Google Scholar] [CrossRef]
- Shih, T.T.; Tien, H.F.; Liu, C.Y.; Su, W.P.; Chan, W.K.; Yang, P.C. Functional MR imaging of tumor angiogenesis predicts outcome of patients with acute myeloid leukemia. Leukemia 2006, 20, 357–362. [Google Scholar] [CrossRef]
- Shih, T.T.; Hou, H.A.; Liu, C.Y.; Chen, B.B.; Tang, J.L.; Chen, H.Y.; Wei, S.Y.; Yao, M.; Huang, S.Y.; Chou, W.C.; et al. Bone marrow angiogenesis magnetic resonance imaging in patients with acute myeloid leukemia: Peak enhancement ratio is an independent predictor for overall survival. Blood 2009, 113, 3161–3167. [Google Scholar] [CrossRef]
- Chen, B.B.; Hsu, C.Y.; Yu, C.W.; Hou, H.A.; Liu, C.Y.; Wei, S.Y.; Chou, W.C.; Tien, H.F.; Shih, T.T. Dynamic contrast-enhanced MR imaging measurement of vertebral bone marrow perfusion may be indicator of outcome of acute myeloid leukemia patients in remission. Radiology 2011, 258, 821–831. [Google Scholar] [CrossRef]
- Kyle, R.A.; Rajkumar, S.V. Criteria for diagnosis, staging, risk stratification and response assessment of multiple myeloma. Leukemia 2009, 23, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, A.; Anderson, K. Multiple myeloma. N. Engl. J. Med. 2011, 364, 1046–1060. [Google Scholar] [CrossRef] [PubMed]
- Folkman, J.; Watson, K.; Ingber, D.; Hanahan, D. Induction of angiogenesis during the transition from hyperplasia to neoplasia. Nature 1989, 339, 58–61. [Google Scholar] [CrossRef] [PubMed]
- Vacca, A.; Ribatti, D.; Roccaro, A.M.; Ria, R.; Palermo, L.; Dammacco, F. Bone marrow angiogenesis and plasma cell angiogenic and invasive potential in patients with active multiple myeloma. Acta Haematol. 2001, 106, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Rana, C.; Sharma, S.; Agrawal, V.; Singh, U. Bone marrow angiogenesis in multiple myeloma and its correlation with clinicopathological factors. Ann. Hematol. 2010, 89, 789–794. [Google Scholar] [CrossRef] [PubMed]
- Moulopoulos, L.A.; Maris, T.G.; Papanikolaou, N.; Panagi, G.; Vlahos, L.; Dimopoulos, M.A. Detection of malignant bone marrow involvement with dynamic contrast-enhanced magnetic resonance imaging. Ann. Oncol. 2003, 14, 152–158. [Google Scholar] [CrossRef]
- Huang, S.Y.; Chen, B.B.; Lu, H.Y.; Lin, H.H.; Wei, S.Y.; Hsu, S.C.; Shih, T.T. Correlation among DCE-MRI measurements of bone marrow angiogenesis, microvessel density, and extramedullary disease in patients with multiple myeloma. Am. J. Hematol. 2012, 87, 837–839. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Xu, Y.; Xu, Q.; Duan, J.; Zhang, H.; Liu, T.; Li, L.; Chan, Q.; Xie, S.; Wang, W. Correlation Between Intravoxel Incoherent Motion and Dynamic Contrast-Enhanced Magnetic Resonance Imaging Parameters in Rectal Cancer. Acad. Radiol. 2019, 26, e134–e140. [Google Scholar] [CrossRef]
- Daldrup-Link, H.E.; Link, T.M.; Rummeny, E.J.; August, C.; Könemann, S.; Jürgens, H.; Heindel, W. Assessing permeability alterations of the blood-bone marrow barrier due to total body irradiation: In Vivo quantification with contrast enhanced magnetic resonance imaging. Bone Marrow Transpl. 2000, 25, 71–78. [Google Scholar] [CrossRef]
- Berthezène, Y.; Vexler, V.; Kuwatsuru, R.; Rosenau, W.; Mühler, A.; Clément, O.; Price, D.C.; Brasch, R.C. Differentiation of alveolitis and pulmonary fibrosis with a macromolecular MR imaging contrast agent. Radiology 1992, 185, 97–103. [Google Scholar] [CrossRef]
- Brasch, R.C. New directions in the development of MR imaging contrast media. Radiology 1992, 183, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Brasch, R.; Pham, C.; Shames, D.; Roberts, T.; van Dijke, K.; van Bruggen, N.; Mann, J.; Ostrowitzki, S.; Melnyk, O. Assessing tumor angiogenesis using macromolecular MR imaging contrast media. J. Magn. Reson. Imaging 1997, 7, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Daldrup, H.; Shames, D.M.; Wendland, M.; Okuhata, Y.; Link, T.M.; Rosenau, W.; Lu, Y.; Brasch, R.C. Correlation of dynamic contrast-enhanced magnetic resonance imaging with histologic tumor grade: Comparison of macromolecular and small-molecular contrast media. Pediatr. Radiol. 1998, 28, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Metz, S.; Lohr, S.; Settles, M.; Beer, A.; Woertler, K.; Rummeny, E.J.; Daldrup-Link, H.E. Ferumoxtran-10-enhanced MR imaging of the bone marrow before and after conditioning therapy in patients with non-Hodgkin lymphomas. Eur. Radiol. 2006, 16, 598–607. [Google Scholar] [CrossRef] [PubMed]
- Daldrup, H.E.; Link, T.M.; Blasius, S.; Strozyk, A.; Könemann, S.; Jürgens, H.; Rummeny, E.J. Monitoring radiation-induced changes in bone marrow histopathology with ultra-small superparamagnetic iron oxide (USPIO)-enhanced MRI. J. Magn. Reson. Imaging 1999, 9, 643–652. [Google Scholar] [CrossRef]
- Vande Berg, B.C.; Lecouvet, F.E.; Kanku, J.P.; Jamart, J.; Van Beers, B.E.; Maldague, B.; Malghem, J. Ferumoxides-enhanced quantitative magnetic resonance imaging of the normal and abnormal bone marrow: Preliminary assessment. J. Magn. Reson. Imaging 1999, 9, 322–328. [Google Scholar] [CrossRef]
- Zhao, X.; Zhao, H.; Chen, Z.; Lan, M. Ultrasmall superparamagnetic iron oxide nanoparticles for magnetic resonance imaging contrast agent. J. Nanosci. Nanotechnol. 2014, 14, 210–220. [Google Scholar] [CrossRef]
- Matuszewski, L.; Persigehl, T.; Wall, A.; Meier, N.; Bieker, R.; Kooijman, H.; Tombach, B.; Mesters, R.; Berdel, W.E.; Heindel, W.; et al. Assessment of bone marrow angiogenesis in patients with acute myeloid leukemia by using contrast-enhanced MR imaging with clinically approved iron oxides: Initial experience. Radiology 2007, 242, 217–224. [Google Scholar] [CrossRef]
- Bremer, C.; Mustafa, M.; Bogdanov, A., Jr.; Ntziachristos, V.; Petrovsky, A.; Weissleder, R. Steady-state blood volume measurements in experimental tumors with different angiogenic burdens a study in mice. Radiology 2003, 226, 214–220. [Google Scholar] [CrossRef]
- Shirota, T.; Tavassoli, M. Cyclophosphamide-induced alterations of bone marrow endothelium: Implications in homing of marrow cells after transplantation. Exp. Hematol. 1991, 19, 369–373. [Google Scholar]
- Shirota, T.; Tavassoli, M. Alterations of bone marrow sinus endothelium induced by ionizing irradiation: Implications in the homing of intravenously transplanted marrow cells. Blood Cells. 1992, 18, 197–214. [Google Scholar] [PubMed]
- Tavassoli, M.; Yoffey, J. Bone Marrow Structure and Function, 2nd ed.; AR Liss: New York, NY, USA, 1983; pp. 85–102. [Google Scholar]
- Montgomery, P.O.; Karney, D.; Reynolds, R.C.; McLendon, D. Cellular and subcellular effects of ionizing radiations. Am. J. Pathol. 1964, 44, 727–746. [Google Scholar] [PubMed]
- Stefani, S.; Chandra, S.; Tonaki, H. Ultrastructural events in the cytoplasmic death of lethally-irradiated human lymphocytes. Int. J. Radiat. Biol. Relat. Stud. Phys. Chem. Med. 1977, 31, 215–225. [Google Scholar] [CrossRef] [PubMed]
- Fan, R.; Zhu, H.; Niu, J.; Li, J.; Zheng, R.; Song, X. Correlation of histological marrow characteristics and intravoxel incoherent motion-derived parameters in benign and malignant hematological disorders. Eur. J. Radiol. 2020, 123, 108745. [Google Scholar] [CrossRef] [PubMed]
- Burtea, C.; Laurent, S.; Vander Elst, L.; Muller, R.N. Contrast agents: Magnetic resonance. Handb. Exp. Pharmacol. 2008, 185, 135–165. [Google Scholar]
- Le Bihan, D.; Breton, E.; Lallemand, D.; Grenier, P.; Cabanis, E.; Laval-Jeantet, M. MR imaging of intravoxel incoherent motions: Application to diffusion and perfusion in neurologic disorders. Radiology 1986, 161, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Koh, D.M.; Collins, D.J.; Orton, M.R. Intravoxel incoherent motion in body diffusion-weighted MRI: Reality and challenges. AJR Am. J. Roentgenol. 2011, 196, 1351–1361. [Google Scholar] [CrossRef]
- Takahara, T.; Kwee, T.C. Low b-value diffusion-weighted imaging: Emerging applications in the body. J. Magn. Reson. Imaging 2012, 35, 1266–1273. [Google Scholar] [CrossRef]
- Li, J.; Li, W.; Niu, J.; Song, X.; Wu, W.; Gong, T.; Zheng, R.; Shih, T.T.; Li, W.; Zhou, X.J. Intravoxel Incoherent Motion Diffusion-weighted MRI of Infiltrated Marrow for Predicting Overall Survival in Newly Diagnosed Acute Myeloid Leukemia. Radiology 2020, 295, 155–161. [Google Scholar] [CrossRef]
- Le Bihan, D.; Turner, R. The capillary network: A link between IVIM and classical perfusion. Magn. Reson. Med. 1992, 27, 171–178. [Google Scholar] [CrossRef]
- Federau, C.; O’Brien, K.; Meuli, R.; Hagmann, P.; Maeder, P. Measuring brain perfusion with intravoxel incoherent motion (IVIM): Initial clinical experience. J. Magn. Reson. Imaging 2014, 39, 624–632. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Lee, S.S.; Kim, N.; Kim, E.; Kim, Y.J.; Yun, S.C.; Kühn, B.; Kim, I.S.; Park, S.H.; Kim, S.Y.; et al. Intravoxel incoherent motion diffusion-weighted MR imaging of the liver: Effect of triggering methods on regional variability and measurement repeatability of quantitative parameters. Radiology 2015, 274, 405–415. [Google Scholar] [CrossRef] [PubMed]
- Federau, C.; Meuli, R.; O'Brien, K.; Maeder, P.; Hagmann, P. Perfusion measurement in brain gliomas with intravoxel incoherent motion MRI. AJNR Am. J. Neuroradiol. 2014, 35, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Gong, T.; Niu, J.; Li, W.; Li, J.; Song, X.; Cui, S.; Bian, W.; Wang, J. Study of bone marrow microstructure in healthy young adults using intravoxel incoherent motion diffusion-weighted MRI. Front. Endocrinol. 2022, 13, 958151. [Google Scholar] [CrossRef] [PubMed]
- Niu, J.; Li, W.; Wang, H.; Wu, W.; Gong, T.; Huang, N.; Wang, J.; Qi, Y. Intravoxel incoherent motion diffusion-weighted imaging of bone marrow in patients with acute myeloid leukemia: A pilot study of prognostic value. J. Magn. Reson. Imaging 2017, 46, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Bourillon, C.; Rahmouni, A.; Lin, C.; Belhadj, K.; Beaussart, P.; Vignaud, A.; Zerbib, P.; Pigneur, F.; Cuenod, C.A.; Bessalem, H.; et al. Intravoxel Incoherent Motion Diffusion-weighted Imaging of Multiple Myeloma Lesions: Correlation with Whole-Body Dynamic Contrast Agent-enhanced MR Imaging. Radiology 2015, 277, 773–783. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Rha, S.Y.; Chung, Y.E.; Shim, H.S.; Kim, Y.J.; Hur, J.; Hong, Y.J.; Choi, B.W. Tumor perfusion-related parameter of diffusion-weighted magnetic resonance imaging: Correlation with histological microvessel density. Magn. Reson. Med. 2014, 71, 1554–1558. [Google Scholar] [CrossRef]
- Bäuerle, T.; Seyler, L.; Münter, M.; Jensen, A.; Brand, K.; Fritzsche, K.H.; Kopp-Schneider, A.; Schüssler, M.; Schlemmer, H.P.; Stieltjes, B.; et al. Diffusion-weighted imaging in rectal carcinoma patients without and after chemoradiotherapy: A comparative study with histology. Eur. J. Radiol. 2013, 82, 444–452. [Google Scholar] [CrossRef]
- Podgórska, J.; Pasicz, K.; Skrzyński, W.; Gołębiewski, B.; Kuś, P.; Jasieniak, J.; Kiliszczyk, A.; Rogowska, A.; Benkert, T.; Pałucki, J. Perfusion-Diffusion Ratio: A New IVIM Approach in Differentiating Solid Benign and Malignant Primary Lesions of the Liver. Biomed. Res. Int. 2022, 2022, 2957759. [Google Scholar] [CrossRef]
- Hussong, J.W.; Rodgers, G.M.; Shami, P.J. Evidence of increased angiogenesis in patients with acute myeloid leukemia. Blood 2000, 95, 309–313. [Google Scholar] [CrossRef]
- Li, J.; Zheng, R.; Niu, J.; Song, X.; Wu, W.; Fan, R.; Gong, T. Correlation of Intravoxel Incoherent Motion Parameters and Histological Characteristics from Infiltrated Marrow in Patients with Acute Leukemia. J. Magn. Reson. Imaging 2020, 51, 1720–1726. [Google Scholar] [CrossRef] [PubMed]
- Le Bihan, D. What can we see with IVIM MRI? Neuroimage 2019, 187, 56–67. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Johnson, C.P.; Ellermann, J. Measuring Knee Bone Marrow Perfusion Using Arterial Spin Labeling at 3 T. Sci. Rep. 2020, 10, 5260. [Google Scholar] [CrossRef] [PubMed]
- Fenchel, M.; Konaktchieva, M.; Weisel, K.; Kraus, S.; Brodoefel, H.; Claussen, C.D.; Horger, M. Early response assessment in patients with multiple myeloma during anti-angiogenic therapy using arterial spin labelling: First clinical results. Eur. Radiol. 2010, 20, 2899–2906. [Google Scholar] [CrossRef] [PubMed]
- Detre, J.A.; Leigh, J.S.; Williams, D.S.; Koretsky, A.P. Perfusion imaging. Magn. Reson. Med. 1992, 23, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Garcia, L.; Lahiri, A.; Schollenberger, J. Recent progress in ASL. Neuroimage 2019, 187, 3–16. [Google Scholar] [CrossRef]
- Wolf, R.L.; Detre, J.A. Clinical neuroimaging using arterial spin-labeled perfusion magnetic resonance imaging. Neurotherapeutics 2007, 4, 346–359. [Google Scholar] [CrossRef]
- Horger, M.; Pereira, P.; Claussen, C.D.; Kanz, L.; Vonthein, R.; Denecke, B.; Driessen, C. Hyperattenuating bone marrow abnormalities in myeloma patients using whole-body non-enhanced low-dose MDCT: Correlation with haematological parameters. Br. J. Radiol. 2008, 81, 386–396. [Google Scholar] [CrossRef]
- Schor-Bardach, R.; Alsop, D.C.; Pedrosa, I.; Solazzo, S.A.; Wang, X.; Marquis, R.P.; Atkins, M.B.; Regan, M.; Signoretti, S.; Lenkinski, R.E.; et al. Does arterial spin-labeling MR imaging-measured tumor perfusion correlate with renal cell cancer response to antiangiogenic therapy in a mouse model? Radiology 2009, 251, 731–742. [Google Scholar] [CrossRef]
- Partovi, S.; von Tengg-Kobligk, H.; Bhojwani, N.; Karmonik, C.; Maurer, M.; Robbin, M.R. Advanced Noncontrast MR Imaging in Musculoskeletal Radiology. Radiol. Clin. N. Am. 2015, 53, 549–567. [Google Scholar] [CrossRef]
- Duan, L.S.; Wang, M.J.; Sun, F.; Zhao, Z.J.; Xing, M.; Zang, Y.F.; Louis, S.; Cui, S.J.; Cui, J.L.; Zhang, H. Characterizing the Blood Oxygen Level-Dependent Fluctuations in Musculoskeletal Tumours Using Functional Magnetic Resonance Imaging. Sci. Rep. 2016, 6, 36522. [Google Scholar] [CrossRef] [PubMed]
- Potente, M.; Carmeliet, P. The Link Between Angiogenesis and Endothelial Metabolism. Annu. Rev. Physiol. 2017, 79, 43–66. [Google Scholar] [CrossRef] [PubMed]
- Thacker, J.; Zhang, J.L.; Franklin, T.; Prasad, P. BOLD quantified renal pO2 is sensitive to pharmacological challenges in rats. Magn. Reson. Med. 2017, 78, 97–302. [Google Scholar] [CrossRef] [PubMed]
- Park, S.E.; Georgescu, A.; Huh, D. Organoids-on-a-chip. Science 2019, 364, 960–965. [Google Scholar] [CrossRef]
- Sui, C.; Zilberberg, J.; Lee, W. Microfluidic device engineered to study the trafficking of multiple myeloma cancer cells through the sinusoidal niche of bone marrow. Sci. Rep. 2022, 12, 1439. [Google Scholar] [CrossRef]
- Ribatti, D.; Vacca, A. Role of Endothelial Cells and Fibroblasts in Multiple Myeloma Angiogenic Switch. Cancer Treat. Res. 2016, 169, 51–61. [Google Scholar]
- Ferrarini, M.; Steimberg, N.; Ponzoni, M.; Belloni, D.; Berenzi, A.; Girlanda, S.; Caligaris-Cappio, F.; Mazzoleni, G.; Ferrero, E. Ex-vivo dynamic 3-D culture of human tissues in the RCCS™ bioreactor allows the study of Multiple Myeloma biology and response to therapy. PLoS ONE 2013, 8, e71613. [Google Scholar] [CrossRef]


| Authors | Year | Modality Imaging | Subjects | Tracer | Parameter | Associated with MVD | Findings |
|---|---|---|---|---|---|---|---|
| Zha et al. [32] | 2010 | DCE-MRI | 6 MM patients, 11 AL patients, 7 chronic myeloid leukemia patients, and 2 NHL patients vs. 20 normal volunteers. | Gadolinium | Emax, Eslope, and TTP | - | Emax, Eslope, and TTP can reflect the malignancies’ histological grade. |
| Shih et al. [41] | 2006 | DCE-MRI | 17 AML patients vs. 17 normal volunteers. | Gadopentetate dimeglumine | Emax, Eslope | - | AML patients with high slope and high peak had significantly decreased OS. |
| Shih et al. [42] | 2009 | DCE-MRI | 78 AML patients. | Gadopentetate dimeglumine | Peak, Amp, Ktrans | - | Peak and Amp can predict OS with AML patients. |
| Chen et al. [43] | 2011 | DCE-MRI | 51 pretreatment AML patients. | Gadodiamide | Peak, Eslope, Amp, and Kep | - | High values of peak, slope, amplitude, and Kep were associated with shorter OS. |
| Huang et al. [50] | 2012 | DCE-MRI | 49 MM patients. | Gadodiamide | Peak, Eslope, Amp, Kep, and Kel | Apart from Kep, all parameters correlate positively with MVD. | High Amp values as a possible risk factor associated with the development of extramedullary disease in MM patients. |
| Daldrup et al. [52] | 2000 | DCE-MRI | 20 6-week-old female New Zealand white rabbits. | CMD-Gd-DOTA | ΔSI | - | Using CMD-Gd-DOTA-enhanced MRI, the integrity of the blood–bone marrow barrier could be accurately defined in vivo. |
| Stephan et al. [57] | 2006 | DCE-MRI | 22 NHL patients. | Ferumoxtran-10 | ΔSI | - | Increased ferumoxtran-10 accumulation correlated with alterations of the MBB. |
| Matuszewski et al. [61] | 2007 | DCE-MRI | 11 AML patients vs. 6 normal volunteers. | Iron oxide blood pool contrast agent | R2*, VVF | ∆R2*and VVF correlate positively with MVD. | Blood pool contrast agents can noninvasively image tissue angiogenesis. |
| Authors | Year | Modality Imaging | Subjects | Tracer | Parameter | Associated with MVD | Findings |
|---|---|---|---|---|---|---|---|
| Fan et al. [68] | 2020 | IVIM | 15 Anemia patients vs. 28 AL patients. | - | f, D, D* | f value is positively correlated with the histological features of marrow. | MVD and f values of AL were higher than those of anemia. |
| Li et al. [73] | 2020 | IVIM | 53 AML patients. | - | f, D, D* | - | Higher f value and lower D value were indicative of unfavorable OS; f value was shown as an independent prognostic factor. |
| Niu et al. [79] | 2017 | IVIM | 53 AML patients. | - | D, D*, f, and ADC | - | D and f values can be used to predict the treatment response of AML patients. |
| Bourillon et al. [80] | 2015 | IVIM/DCE-MRI | 27 MM patients. | -/Gadolinium chelate | f, D, D*, ADC, Emax | - | D and ADC values positively correlated with Emax. |
| Li et al. [85] | 2020 | IVIM | 20 AL patients. | - | f, D, D* | f value is positively correlated with the histological MVD. | IVIM parameters combined with histological parameters can evaluate the microstructure of AL bone marrow. |
| Authors | Year | Modality Imaging | Subjects | Tracer | Parameter | Associated with MVD | Findings |
|---|---|---|---|---|---|---|---|
| Li et al. [87] | 2020 | ASL | 8 healthy volunteers vs. 2 juvenile osteochondritis dissecans. | - | Perfusion signal. | - | ASL imaging can detect disease-related bone marrow perfusion changes. |
| Fenchel et al. [88] | 2010 | ASL | 19 MM patients. | - | Perfusion signal. | - | Correlation of ASL perfusion with outcome was significant. |
| Duan et al. [95] | 2016 | BOLD-MRI | 52 musculoskeletal tumor patients. | - | Frequency band. | - | BOLD signal is positively related to blood flow or the partial pressure of oxygen in normal tissue or tumor tissue. |
| Sui. et al. [99] | 2022 | Microfluidic devices | - | - | - | - | Microfluidic devices can be used to study the trafficking of MM cells through the sinusoidal niche of the BM. |
| Ferrarini. et al. [101] | 2013 | 3-D culture models | 5 MM patients vs. 4 joint replacement patients. | - | - | - | 3-D culture models can assess the metabolic activity of MM cells and their microenvironment. |
| Methods | Principle | Advantages | Limitations | Previous Study and Clinical Significance |
|---|---|---|---|---|
| DCE-MRI | Evaluates the structure and function of micro-vessels by tracking the pharmacokinetic changes of molecular contrast agents [30,31]. | Imaging methods that require small molecular contrast agents are non-invasive examination methods [32]. | Have high trans-endothelial permeability in both normal and tumor micro-vessels and there is no unified pharmacokinetic model [51]; longer scan time. |
|
| The distribution of macromolecular contrast media in healthy tissues is comparable to that of BVs and has a longer plasma half-life [52,53,54,55,56]. | Sometimes produce a strong susceptibility effect that causes organ boundaries to distort or disappear [69]; decreased temporal resolution. |
| ||
| IVIM | Using multiple b-values and a biexponential signal model to obtain information on the diffusion of tissues and capillary perfusion [70,71,72]. | Simultaneously obtain diffusion and perfusion quantification in a single image without an intravenous contrast agent [73]. | The parameter values are affected by many factors, such as respiratory motion artifacts; parameter values are highly variable; susceptibility artifacts. |
|
| ASL | Using endogenous blood as reagent, the perfusion image was obtained with a subtraction technique [91]. | Noninvasive and non-contrast-enhanced perfusion imaging method that is highly reproducible [87]. | Relatively poor parameters, time and space resolution, and low SNR. | |
| BOLD-MRI | Using endogenous deoxygenated hemoglobin to transform microscopic magnetic fields and de-phase spin protons [94,95]. | Non-invasive and non-contrast-enhanced perfusion imaging method [94,95]. | Lack of unified technical standards at home and abroad, and lack of effective calibration method. |
|
| Microfluidic Devices | Simulate the physiological function of tissue cells with organ-specific biological, chemical, and physical factors [98]. | Can directly observe the changes of tissues in various states; small and accurate. [99,100]. | Consumables are expensive and the demand is small. |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, J.; Huang, Q.; Bian, W.; Wang, J.; Guan, H.; Niu, J. Imaging Techniques and Clinical Application of the Marrow–Blood Barrier in Hematological Malignancies. Diagnostics 2024, 14, 18. https://doi.org/10.3390/diagnostics14010018
Zhang J, Huang Q, Bian W, Wang J, Guan H, Niu J. Imaging Techniques and Clinical Application of the Marrow–Blood Barrier in Hematological Malignancies. Diagnostics. 2024; 14(1):18. https://doi.org/10.3390/diagnostics14010018
Chicago/Turabian StyleZhang, Jianling, Qianqian Huang, Wenjin Bian, Jun Wang, Haonan Guan, and Jinliang Niu. 2024. "Imaging Techniques and Clinical Application of the Marrow–Blood Barrier in Hematological Malignancies" Diagnostics 14, no. 1: 18. https://doi.org/10.3390/diagnostics14010018