
Diagnostic Accuracy of Up-Front PET/CT and MRI for Detecting Cervical Lymph Node Metastases in T1–T2 Oral Cavity Cancer—A Prospective Cohort Study

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
- Examination by an experienced head and neck surgeon, including palpation and ultrasonography of the cervical lymph nodes. Fine needle aspiration was only performed when a strong malignancy suspicion was present.
- Up-front PET/CT and MRI scans.
- Biopsy of the primary tumor.
- Multi-disciplinary team conference.
2.3. Up-Front 18F-FDG PET/CT
2.4. MRI
2.5. Assessment of Scans
- True positive (TP) was defined as a positive PET/CT and a positive histopathology.
- True negative (TN) was defined as a negative PET/CT and a negative histopathology.
- False positive (FP) was defined as a positive PET/CT and a negative histopathology.
- False negative (FN) was defined as a negative PET/CT and a positive histopathology.
2.6. Multi-Disciplinary Team Conference
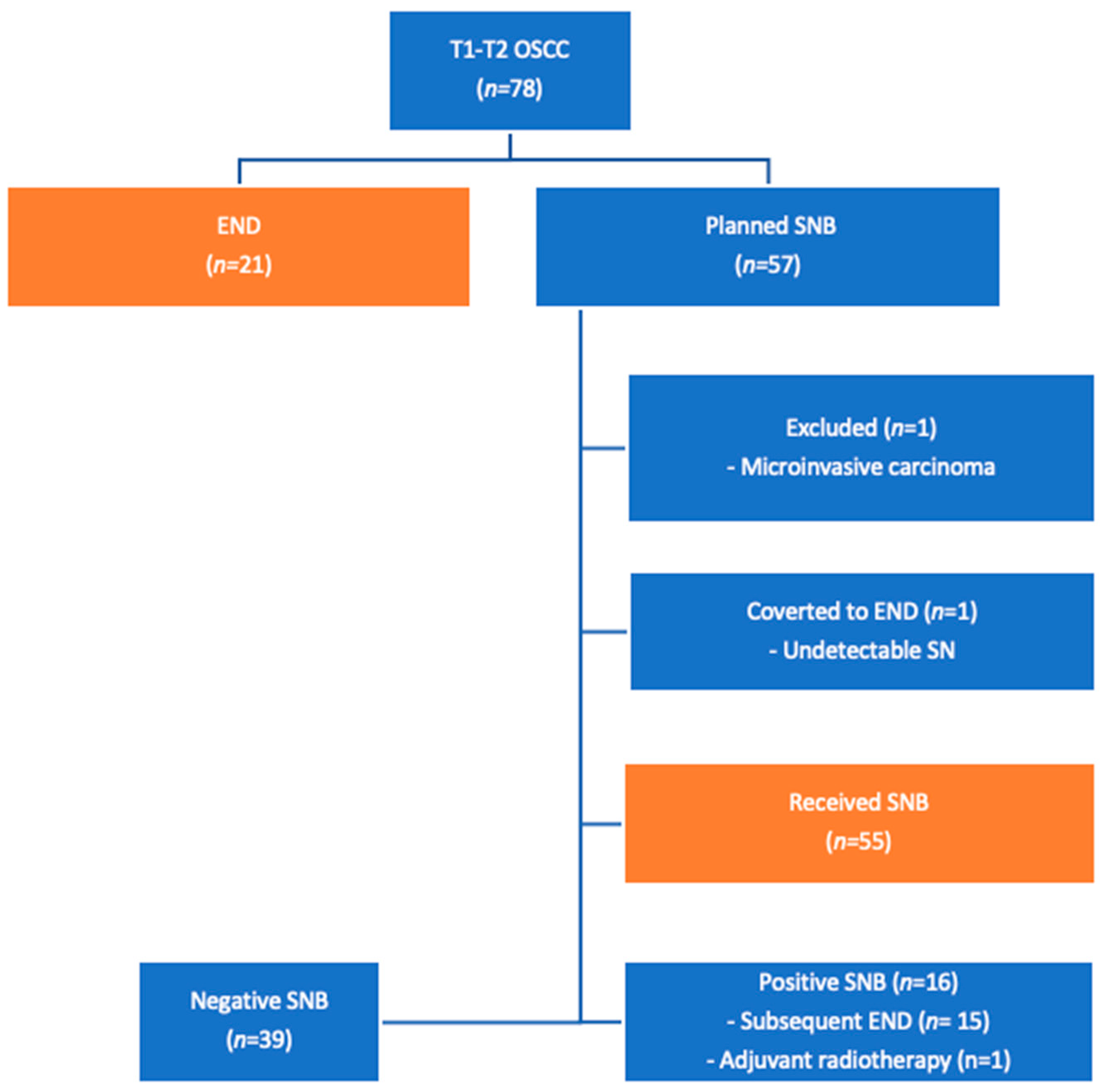
2.7. Sentinel Node Biopsy
2.8. Statistics
3. Results
4. Discussion
4.1. Main Findings
4.2. Strengths and Limitations in Relation to Other Studies
4.3. Strengths and Limitations
4.4. Challenges
4.5. Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kovács, A.F.; Stefenelli, U.; Seitz, O.; Middendorp, M.; Diener, J.; Sader, R.; Grünwald, F. Positive sentinel lymph nodes are a negative prognostic factor for survival in T1-2 oral/oropharyngeal cancer—A long-term study on 103 patients. Ann. Surg. Oncol. 2009, 16, 233–239. [Google Scholar] [CrossRef]
- Shah, J.P.; Candela, F.C.; Poddar, A.K. The patterns of cervical lymph node metastases from squamous carcinoma of the oral cavity. Cancer 1990, 66, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Stoeckli, S.J.; Pfaltz, M.; Steinert, H.; Schmid, S. Histopathological features of occult metastasis detected by sentinel lymph node biopsy in oral and oropharyngeal squamous cell carcinoma. Laryngoscope 2002, 112, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Stoeckli, S.J.; Steinert, H.; Pfaltz, M.; Schmid, S. Sentinel lymph node evaluation in squamous cell carcinoma of the head and neck. Otolaryngol. Head. Neck Surg. 2001, 125, 221–226. [Google Scholar] [CrossRef]
- Liao, C.T.; Wang, H.M.; Huang, S.F.; Chen, I.H.; Kang, C.J.; Lin, C.Y.; Fan, K.H.; Ng, S.H.; Hsueh, C.; Lee, L.Y.; et al. PET and PET/CT of the neck lymph nodes improves risk prediction in patients with squamous cell carcinoma of the oral cavity. J. Nucl. Med. 2011, 52, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, U.; Dietlein, M.; Wittekindt, C.; Ortmann, M.; Stuetzer, H.; Vent, J.; Jungehuelsing, M.; Krug, B. Is there a need for positron emission tomography imaging to stage the N0 neck in T1–T2 squamous cell carcinoma of the oral cavity or oropharynx? Ann. Otol. Rhinol. Laryngol. 2008, 117, 854–863. [Google Scholar] [CrossRef]
- Stoeckli, S.J.; Steinert, H.; Pfaltz, M.; Schmid, S. Is there a role for positron emission tomography with 18F-fluorodeoxyglucose in the initial staging of nodal negative oral and oropharyngeal squamous cell carcinoma. Head Neck 2002, 24, 345–349. [Google Scholar] [CrossRef]
- Zhang, H.; Seikaly, H.; Biron, V.L.; Jeffery, C.C. Utility of PET-CT in detecting nodal metastasis in cN0 early stage oral cavity squamous cell carcinoma. Oral Oncol. 2018, 80, 89–92. [Google Scholar] [CrossRef]
- Cramer, J.D.; Sridharan, S.; Ferris, R.L.; Duvvuri, U.; Samant, S. Sentinel Lymph Node Biopsy Versus Elective Neck Dissection for Stage I to II Oral Cavity Cancer. Laryngoscope 2019, 129, 162–169. [Google Scholar] [CrossRef]
- Schilling, C.; Stoeckli, S.J.; Haerle, S.K.; Broglie, M.A.; Huber, G.F.; Sorensen, J.A.; Bakholdt, V.; Krogdahl, A.; von Buchwald, C.; Bilde, A.; et al. Sentinel European Node Trial (SENT): 3-year results of sentinel node biopsy in oral cancer. Eur. J. Cancer 2015, 51, 2777–2784. [Google Scholar] [CrossRef]
- Thompson, C.F.; St John, M.A.; Lawson, G.; Grogan, T.; Elashoff, D.; Mendelsohn, A.H. Diagnostic value of sentinel lymph node biopsy in head and neck cancer: A meta-analysis. Eur. Arch. Otorhinolaryngol. 2013, 270, 2115–2122. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Zhou, J.; Wu, H. Diagnostic value of sentinel lymph node biopsy for cT1/T2N0 tongue squamous cell carcinoma: A meta-analysis. Eur. Arch. Otorhinolaryngol. 2017, 274, 3843–3852. [Google Scholar] [CrossRef] [PubMed]
- Crocetta, F.M.; Botti, C.; Pernice, C.; Murri, D.; Castellucci, A.; Menichetti, M.; Costantini, M.; Venturelli, F.; Bassi, M.C.; Ghidini, A. Sentinel node biopsy versus elective neck dissection in early-stage oral cancer: A systematic review. Eur. Arch. Otorhinolaryngol. 2020, 277, 3247–3260. [Google Scholar] [CrossRef] [PubMed]
- Ding, Z.; Li, Y.; Pan, X.; Xuan, M.; Xie, H.; Wang, X. Sentinel lymph node biopsy versus elective neck dissection in squamous cell carcinoma of the oral cavity with a clinically N0 neck: Systematic review and meta-analysis of prospective studies. Head Neck 2021, 43, 3185–3198. [Google Scholar] [CrossRef]
- Gupta, T.; Maheshwari, G.; Kannan, S.; Nair, S.; Chaturvedi, P.; Agarwal, J.P. Systematic review and meta-analysis of randomized controlled trials comparing elective neck dissection versus sentinel lymph node biopsy in early-stage clinically node-negative oral and/or oropharyngeal squamous cell carcinoma: Evidence-base for practice and implications for research. Oral Oncol. 2022, 124, 105642. [Google Scholar] [CrossRef]
- Bae, M.R.; Roh, J.L.; Kim, J.S.; Lee, J.H.; Cho, K.J.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. (18)F-FDG PET/CT versus CT/MR imaging for detection of neck lymph node metastasis in palpably node-negative oral cavity cancer. J. Cancer Res. Clin. Oncol. 2020, 146, 237–244. [Google Scholar] [CrossRef]
- Ng, S.H.; Yen, T.C.; Liao, C.T.; Chang, J.T.; Chan, S.C.; Ko, S.F.; Wang, H.M.; Wong, H.F. 18F-FDG PET and CT/MRI in oral cavity squamous cell carcinoma: A prospective study of 124 patients with histologic correlation. J. Nucl. Med. 2005, 46, 1136–1143. [Google Scholar]
- Mazzola, R.; Alongi, P.; Ricchetti, F.; Fiorentino, A.; Fersino, S.; Giaj-Levra, N.; Salgarello, M.; Alongi, F. 18F-Fluorodeoxyglucose-PET/CT in locally advanced head and neck cancer can influence the stage migration and nodal radiation treatment volumes. Radiol. Med. 2017, 122, 952–959. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef]
- Rohde, M.; Nielsen, A.L.; Johansen, J.; Sørensen, J.A.; Diaz, A.; Asmussen, J.T.; Gerke, O.; Thomassen, A.; Gyldenkerne, N.; Døssing, H.; et al. Up-front PET/CT changes treatment intent in patients with head and neck squamous cell carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 613–621. [Google Scholar] [CrossRef]
- Sørensen, J.A.; Bakholdt, V.T.; Grupe, P.; Thomsen, J.B. Sentinel lymph node biopsy for oral cancer. J. Vis. Surgery 2018, 4, 5. [Google Scholar] [CrossRef]
- Bluemel, C.; Rubello, D.; Colletti, P.M.; de Bree, R.; Herrmann, K. Sentinel lymph node biopsy in oral and oropharyngeal squamous cell carcinoma: Current status and unresolved challenges. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1469–1480. [Google Scholar] [CrossRef] [PubMed]
- Haerle, S.K.; Hany, T.F.; Strobel, K.; Sidler, D.; Stoeckli, S.J. Is there an additional value of SPECT/CT over planar lymphoscintigraphy for sentinel node mapping in oral/oropharyngeal squamous cell carcinoma? Ann. Surg. Oncol. 2009, 16, 3118–3124. [Google Scholar] [CrossRef] [PubMed]
- Meerwein, C.M.; Sekine, T.; Veit-Haibach, P.; Bredell, M.G.; Huber, G.F.; Huellner, M.W. Multi-slice SPECT/CT vs. lymphoscintigraphy and intraoperative gamma ray probe for sentinel node mapping in HNSCC. Eur. Arch. Otorhinolaryngol. 2017, 274, 1633–1642. [Google Scholar] [CrossRef]
- Linz, C.; Brands, R.C.; Herterich, T.; Hartmann, S.; Müller-Richter, U.; Kübler, A.C.; Haug, L.; Kertels, O.; Bley, T.A.; Dierks, A.; et al. Accuracy of 18-F Fluorodeoxyglucose Positron Emission Tomographic/Computed Tomographic Imaging in Primary Staging of Squamous Cell Carcinoma of the Oral Cavity. JAMA Netw. Open 2021, 4, e217083. [Google Scholar] [CrossRef] [PubMed]
- Niu, L.; Zheng, D.; Wang, D.; Zhang, J.; Fei, J.; Guo, C. Accuracy of (18) F-FDG PET/CT in Detection of Neck Metastases of Oral Squamous Cell Carcinoma in Patients Without Large Palpable Lymph Nodes. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 129, 418–426. [Google Scholar] [CrossRef]
- Sharma, A.; Kim, J.W.; Paeng, J.Y. Clinical analysis of neck node metastasis in oral cavity cancer. J. Korean Assoc. Oral Maxillofac. Surg. 2018, 44, 282–288. [Google Scholar] [CrossRef]
- Thoenissen, P.; Heselich, A.; Burck, I.; Sader, R.; Vogl, T.; Ghanaati, S. The role of magnetic resonance imaging and computed tomography in oral squamous cell carcinoma patients’ preoperative staging. Front. Oncol. 2023, 13, 972042. [Google Scholar] [CrossRef]
- Laimer, J.; Lauinger, A.; Steinmassl, O.; Offermanns, V.; Grams, A.E.; Zelger, B.; Bruckmoser, E. Cervical Lymph Node Metastases in Oral Squamous Cell Carcinoma-How Much Imaging Do We Need? Diagnostics 2020, 10, 199. [Google Scholar] [CrossRef]
- Souren, C.; Kloss-Brandstätter, A.; Stadler, A.; Kross, K.; Yamauchi, K.; Ketelsen, D.; Kessler, P.; Lethaus, B. Ultrasound-guided fine-needle aspiration cytology as a diagnostic tool in comparison to ultrasound and MRI for staging in oral- and oropharyngeal squamous cell tumors. J. Craniomaxillofac. Surg. 2016, 44, 197–201. [Google Scholar] [CrossRef]
- Yang, B.; Olsen, M.; Vali, Y.; Langendam, M.W.; Takwoingi, Y.; Hyde, C.J.; Bossuyt, P.M.M.; Leeflang, M.M.G. Study designs for comparative diagnostic test accuracy: A methodological review and classification scheme. J. Clin. Epidemiol. 2021, 138, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Bloch, D.A. Comparing two diagnostic tests against the same “gold standard” in the same sample. Biometrics 1997, 53, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Siepe, B.; Hoilund-Carlsen, P.F.; Gerke, O.; Weber, W.A.; Motschall, E.; Vach, W. The move from accuracy studies to randomized trials in PET: Current status and future directions. J. Nucl. Med. 2014, 55, 1228–1234. [Google Scholar] [CrossRef] [PubMed]
- Vach, W.; Høilund-Carlsen, P.F.; Gerke, O.; Weber, W.A. Generating evidence for clinical benefit of PET/CT in diagnosing cancer patients. J. Nucl. Med. 2011, 52 (Suppl. S2), 77s–85s. [Google Scholar] [CrossRef]
- Euser, A.M.; Zoccali, C.; Jager, K.J.; Dekker, F.W. Cohort studies: Prospective versus retrospective. Nephron Clin. Pract. 2009, 113, c214–c217. [Google Scholar] [CrossRef]
- Baba, A.; Hashimoto, K.; Kayama, R.; Yamauchi, H.; Ikeda, K.; Ojiri, H. Radiological approach for the newly incorporated T staging factor, depth of invasion (DOI), of the oral tongue cancer in the 8th edition of American Joint Committee on Cancer (AJCC) staging manual: Assessment of the necessity for elective neck dissection. Jpn. J. Radiol. 2020, 38, 821–832. [Google Scholar] [CrossRef]
- Mishra, A.; Das, A.; Dhal, I.; Shankar, R.; Bhavya, B.M.; Singh, N.; Tripathi, P.; Daga, D.; Rai, A.; Gupta, M.; et al. Worst pattern of invasion in oral squamous cell carcinoma is an independent prognostic factor. J. Oral Biol. Craniofac Res. 2022, 12, 771–776. [Google Scholar] [CrossRef]
- Hasegawa, Y.; Tsukahara, K.; Yoshimoto, S.; Miura, K.; Yokoyama, J.; Hirano, S.; Uemura, H.; Sugasawa, M.; Yoshizaki, T.; Homma, A.; et al. Neck Dissections Based on Sentinel Lymph Node Navigation Versus Elective Neck Dissections in Early Oral Cancers: A Randomized, Multicenter, and Noninferiority Trial. J. Clin. Oncol. 2021, 39, 2025–2036. [Google Scholar] [CrossRef]
- LeRose, C.C.; Boura, J.; Ramirez, C.A. Investigating the Reliability of Fluorodeoxyglucose 18 Positive Emission Tomography-Computed Tomography Detection of Regional Lymph Node Metastasis in Head and Neck Malignancy. J. Oral Maxillofac. Surg. 2020, 78, 1631–1638. [Google Scholar] [CrossRef]
- Crippa, F.; Leutner, M.; Belli, F.; Gallino, F.; Greco, M.; Pilotti, S.; Cascinelli, N.; Bombardieri, E. Which kinds of lymph node metastases can FDG PET detect? A clinical study in melanoma. J. Nucl. Med. 2000, 41, 1491–1494. [Google Scholar]
- Choi, K.Y.; Park, S.C.; Kim, J.H.; Lee, D.J. The occult nodal metastasis rate of early tongue cancer (T1–T2): A protocol for a systematic review and meta-analysis. Medicine 2021, 100, e24327. [Google Scholar] [CrossRef] [PubMed]
- Baeyens, J.P.; Serrien, B.; Goossens, M.; Clijsen, R. Questioning the “SPIN and SNOUT” rule in clinical testing. Arch. Physiother. 2019, 9, 4. [Google Scholar] [CrossRef] [PubMed]
- Rohde, M.; Nielsen, A.L.; Johansen, J.; Sorensen, J.A.; Nguyen, N.; Diaz, A.; Nielsen, M.K.; Asmussen, J.T.; Christiansen, J.M.; Gerke, O.; et al. Head-to-Head Comparison of Chest X-Ray/Head and Neck MRI, Chest CT/Head and Neck MRI, and (18)F-FDG PET/CT for Detection of Distant Metastases and Synchronous Cancer in Oral, Pharyngeal, and Laryngeal Cancer. J. Nucl. Med. 2017, 58, 1919–1924. [Google Scholar] [CrossRef] [PubMed]
- Rohde, M.; Nielsen, A.L.; Pareek, M.; Johansen, J.; Sørensen, J.A.; Diaz, A.; Nielsen, M.K.; Christiansen, J.M.; Asmussen, J.T.; Nguyen, N.; et al. A PET/CT-Based Strategy Is a Stronger Predictor of Survival Than a Standard Imaging Strategy in Patients with Head and Neck Squamous Cell Carcinoma. J. Nucl. Med. 2018, 59, 575–581. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Descriptive Statistics |
|---|---|
| Number of patients | 76 |
| Sex | Male: 52 (68%) |
| Female: 24 (32%) | |
| Median age (range) | 63 years (21–85 years) |
| Location of primary tumor | Floor of mouth: 27 (36%) |
| 2/3 anterior tongue: 34 (45%) | |
| Upper alveolus: 1 (1%) | |
| Lower alveolus: 7 (9%) | |
| Buccal mucosa: 5 (7%) | |
| Hard palate: 1 (1%) | |
| Retromolar area: 1 (1%) | |
| T-stage | T1: 53 (70%) |
| T2: 23 (30%) | |
| Median tumor size (range) | 18 mm (5–40 mm) |
| Regional * recurrence rate | SNB: 9/55 (16%) |
| END: 8/21 (38%) | |
| Median follow up (range) | SNB: 57 months (1–70 months) |
| END: 30 months (3–80 months) |
| PET/CT | Histopathology | |
|---|---|---|
| Positive | Negative | |
| Positive | 23 TP | 18 FP |
| Negative | 8 FN | 27 TN |
| Neck MRI | Histopathology | |
|---|---|---|
| Positive | Negative | |
| Positive | 8 TP | 5 FP |
| Negative | 22 FN | 38 TN |
| Parameter | PET/CT | Neck MRI | p-Value |
|---|---|---|---|
| Sensitivity (95% CI) | 74% (55–88%) | 27% (12–46%) | 0.0001 |
| Specificity (95% CI) | 60% (44–74%) | 88% (75–96%) | 0.001 |
| Accuracy (95% CI) | 66% (54–76%) | 63% (51–74%) | 0.85 |
| PPV (95% CI) | 56% (40–72%) | 62% (32–86%) | 0.73 |
| NPV (95% CI) | 77% (60–90%) | 63% (50–75%) | 0.16 |
| Publication | Population | Year | PET | Neck MRI | ||
|---|---|---|---|---|---|---|
| Sensitivity | Specificity | Sensitivity | Specificity | |||
| Bae et al. [16] | T1–T4 OCC | 2020 | 69.1% | 77.9% | ||
| Niu et al. [26] | T1–T4 OCC | 2020 | 83.9% | 73.1% | ||
| Thoenissen et al. [28] | T1–T4 OCC | 2023 | 66% | 68% | ||
| Laimer et al. [29] | T1–T4 OCC | 2020 | 85.7% | 75.6% | ||
| Souren et al. [30] | T1–T4 OCC | 2015 | 83.1% | 75.7% | ||
| Linz et al. [25] | T1–T4 OCC | 2021 | 82.4% | 83.5% | 70.6% | 62.6% |
| Our results | T1–T2 OCC | 74% | 60% | 27% | 88% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Madsen, C.B.; Rohde, M.; Gerke, O.; Godballe, C.; Sørensen, J.A. Diagnostic Accuracy of Up-Front PET/CT and MRI for Detecting Cervical Lymph Node Metastases in T1–T2 Oral Cavity Cancer—A Prospective Cohort Study. Diagnostics 2023, 13, 3414. https://doi.org/10.3390/diagnostics13223414
Madsen CB, Rohde M, Gerke O, Godballe C, Sørensen JA. Diagnostic Accuracy of Up-Front PET/CT and MRI for Detecting Cervical Lymph Node Metastases in T1–T2 Oral Cavity Cancer—A Prospective Cohort Study. Diagnostics. 2023; 13(22):3414. https://doi.org/10.3390/diagnostics13223414
Chicago/Turabian StyleMadsen, Christoffer Bing, Max Rohde, Oke Gerke, Christian Godballe, and Jens Ahm Sørensen. 2023. "Diagnostic Accuracy of Up-Front PET/CT and MRI for Detecting Cervical Lymph Node Metastases in T1–T2 Oral Cavity Cancer—A Prospective Cohort Study" Diagnostics 13, no. 22: 3414. https://doi.org/10.3390/diagnostics13223414