
Microembolizations in the Arterial Cerebral Circulation in Patients with Atrial Fibrillation Ablation Using the Cryoballoon Technique—Protocol and Methodology of a Prospective Observational Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
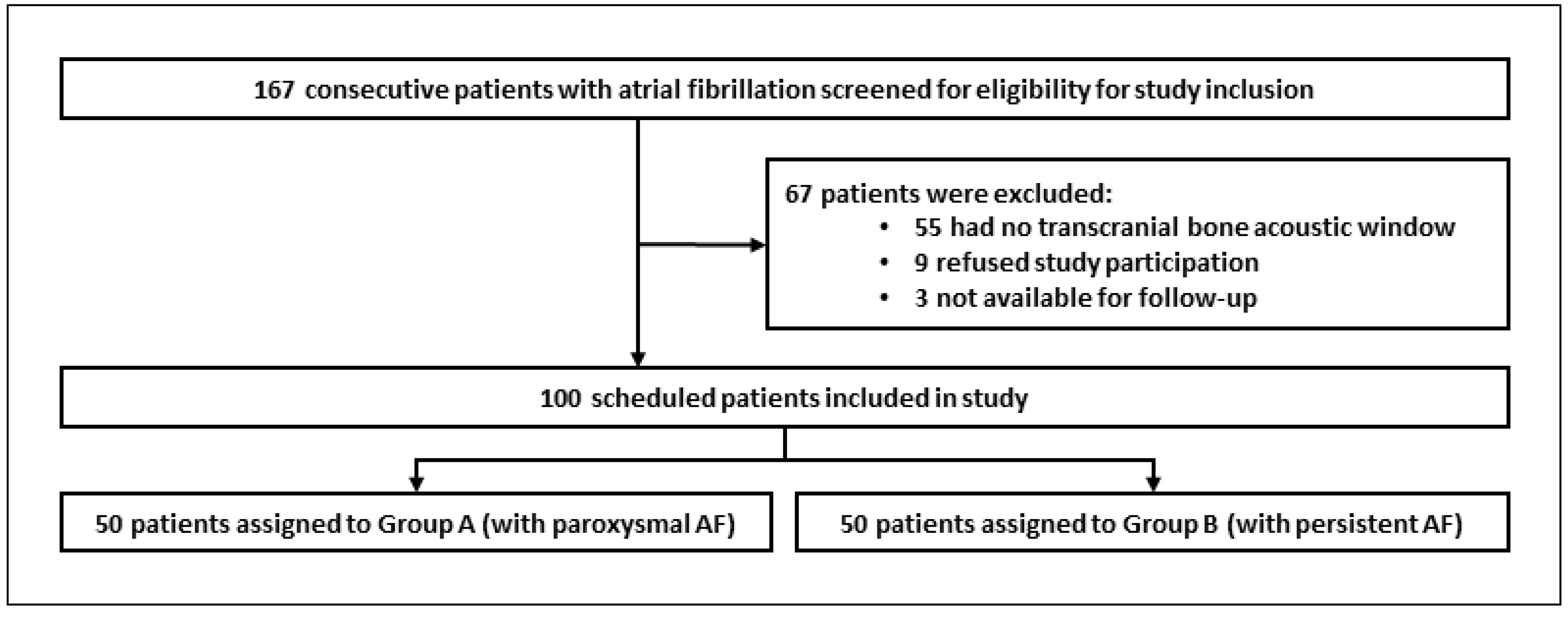
2.1. Patient Population
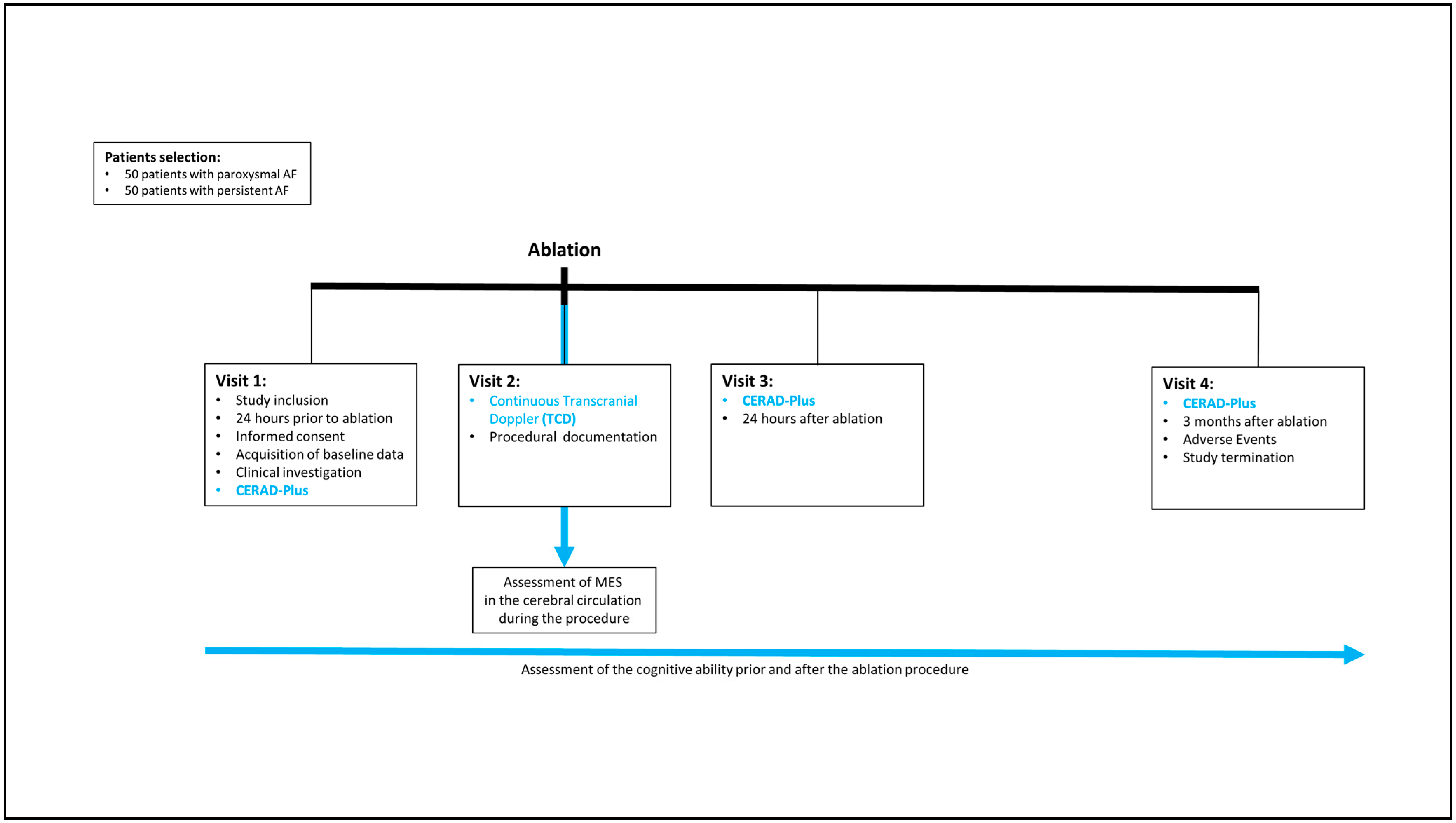
2.2. Study Design and Objectives
- (1)
- Technical variables that relate to the electrophysiological procedure (venous access, trans-septal puncture, pulmonary vein/left atrium angiography, cryoballoon introduction into the left atrium, balloon- and contrast-agent-guided pulmonary vein occlusion, balloon freeze cycle and thawing phase for each PV, LARA freeze cycles, and thawing phase and sheath retreat to the RA);
- (2)
- Individual factors:
- (a)
- Investigator dependency (effect of the examiner’s experience in cryoballoon ablation evaluated by the procedure time, amount of contrast agent used, and number of freezes);
- (b)
- Patient dependency (demographics/comorbidities, type of atrial fibrillation, CHA2DS2VASc score, electrocardiography data, echocardiography data, laboratory values, and medication intake).
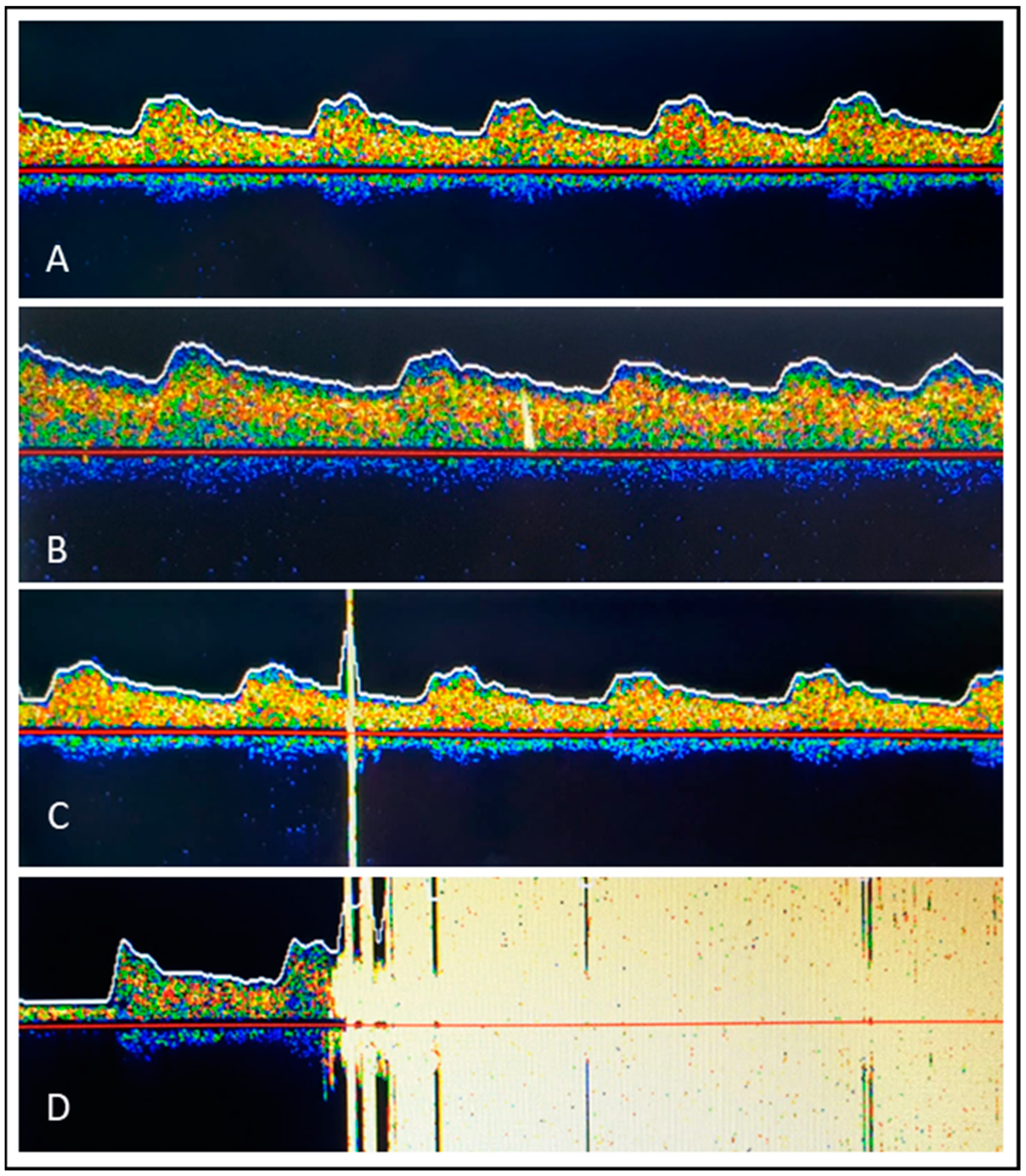
2.3. Microembolic Signal Detection Using Transcranial Doppler Ultrasonography
2.4. Neuropsychological Testing
- Verbal fluency (animals): Measures disturbances in verbal production and examines semantic memory and language
- Boston naming test: Assesses the patient’s verbal ability to name line drawings
- MMSE total score: Tests spatial orientation problems, memory, attention, arithmetic, and language
- Word list learning sum: Assesses how well patients retain newly learned information
- Constructional praxis: Examines constructive practice
- Word list recall: Tests the ability to remember a list of words viewed previously
- Word list visual recall: Tests verbal memory, delayed verbal memory, recognition, and recall versus memory deficits
- Constructional praxis recall: Tests nonverbal memory, delayed figural memory, and free reproduction
- Trail making test A: Measures psychomotor speed
- Trail making test B: Reflects the performance of executive functions
- Verbal fluency (s-words): Tests verbal fluency in a strategy-oriented manner
2.5. Atrial Fibrillation Ablation Procedure
2.6. Anticoagulation Management
2.7. Gastroesophageal Endoscopy
- Type 1: erythema
- Type 2a: superficial ulcer
- Type 2b: deep ulcer
- Type 3a: perforation without communication with the atria
- Type 3b: perforation with atrioesophageal fistula
2.8. Statistical Analysis
2.8.1. Statistical Study Planning and Sample Volume Calculation
2.8.2. Current Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Staerk, L.; Sherer, J.A.; Ko, D.; Benjamin, E.J.; Helm, R.H. Atrial fibrillation: Epidemiology, pathophysiology, and clinical outcomes. Circ. Res. 2017, 120, 1501–1517. [Google Scholar] [CrossRef] [PubMed]
- Mou, L.; Norby, F.L.; Chen, L.Y.; O’Neal, W.T.; Lewis, T.T.; Loehr, L.R.; Soliman, E.Z.; Alonso, A. Lifetime risk of atrial fibrillation by race and socioeconomic status: ARIC study (Atherosclerosis Risk in Communities). Circ. Arrhythm. Electrophysiol. 2018, 11, e006350. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Muntner, P.; Alonso, A.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Das, S.R.; et al. Heart disease and stroke statistics 2019 update: A report from the American Heart Association. Circulation 2019, 139, e56–e528. [Google Scholar] [CrossRef] [PubMed]
- Colilla, S.; Crow, A.; Petkun, W.; Singer, D.E.; Simon, T.; Liu, X. Estimates of current and future incidence and prevalence of atrial fibrillation in the US adult population. Am. J. Cardiol. 2013, 112, 1142–1147. [Google Scholar] [CrossRef]
- Di Carlo, A.; Bellino, L.; Consoli, D.; Mori, F.; Zaninelli, A.; Baldereschi, M.; Baldereschi, M.; Cattarinussi, A.; D’Alfonso, M.G.; Gradia, C.; et al. Prevalence of atrial fibrillation in the Italian elderly population and projections from 2020 to 2060 for Italy and the European Union: The FAI Project. Europace 2019, 21, 1468–1475. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar]
- Kuniss, M.; Pavlovic, N.; Velagic, V.; Hermida, J.S.; Healey, S.; Arena, G.; Badenco, N.; Meyer, C.; Chen, J.; Lacopino, S.; et al. Cryoballoon ablation vs. antiarrhythmic drugs: First-line therapy for patients with paroxysmal atrial fibrillation. Europace 2021, 23, 1033–1041. [Google Scholar] [CrossRef]
- Andrade, J.G.; Wells, G.A.; Deyell, M.W.; Bennett, M.; Essebag, V.; Champagne, J.; Roux, J.F.; Yung, D.; Skanes, A.; Khaykin, Y.; et al. Cryoablation or drug therapy for initial treatment of atrial fibrillation. N. Engl. J. Med. 2021, 384, 305–315. [Google Scholar] [CrossRef]
- Wazni, O.M.; Dandamudi, G.; Sood, N.; Hoyt, R.; Tyler, J.; Durrani, S.; Niebauer, M.; Makati, K.; Halperin, B.; Gauri, A.; et al. Cryoballoon ablation as initial therapy for atrial fibrillation. N. Engl. J. Med. 2021, 384, 316–324. [Google Scholar] [CrossRef]
- Kuck, K.H.; Lebedev, D.S.; Mikhaylov, E.N.; Romanov, A.; Geller, L.; Kalejs, O.; Neumann Thomas Davtyan, K.; On, Y.K.; Popov, S.; Bongiorni, M.G.; et al. Catheter ablation or medical therapy to delay progression of atrial fibrillation: The randomized controlled atrial fibrillation progression trial (ATTEST). Europace 2021, 23, 362–369. [Google Scholar] [CrossRef]
- Kuniss, M.; Akkaya, E.; Berkowitsch, A.; Zaltsberg, S.; Greiss, H.; Rechner, M.; Weipert, K.; Hain, A.; Hamm, C.W.; Neumann, T. Left atrial roof ablation in patients with persistent atrial fibrillation using the second-generation cryoballoon: Benefit or wasted time? Clin. Res. Cardiol. 2020, 109, 714–724. [Google Scholar] [CrossRef] [PubMed]
- Akkaya, E.; Berkowitsch, A.; Rieth, A.; Erkapic, D.; Hamm, C.W.; Neumann, T.; Kuniss, M. Clinical outcome and left atrial function after left atrial roof ablation using the cryoballoon technique in patients with symptomatic persistent atrial fibrillation. Int. J. Cardiol. 2019, 292, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Kuniss, M.; Greiß, H.; Pajitnev, D.; Akkaya, E.; Deubner, N.; Hain, A.; Bodammer, L.; Berkowitsch, A.; Chierchia, G.B.; Hamm, C.W.; et al. Cryoballoon ablation of persistent atrial fibrillation: Feasibility and safety of left atrial roof ablation with generation of con- duction block in addition to antral pulmonary vein isolation. Europace 2017, 19, 1109–1115. [Google Scholar] [CrossRef] [PubMed]
- Herrera Siklódy, C.; Deneke, T.; Hocini, M.; Lehrmann, H.; Shin, D.I.; Miyazaki, S.; Henschke, S.; Fluegel, P.; Schiebeling-Römer, J.; Bansmann, P.M.; et al. Incidence of asymptomatic intracranial embolic events after pulmonary vein isolation: Comparison of different atrial fibrillation ablation technologies in a multicenter study. J. Am. Coll. Cardiol. 2011, 58, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Deneke, T.; Jais, P.; Scaglione, M.; Schmitt, R.; di Biase, L.; Chritopoulos, G.; Schade, A.; Mügge, A.; Bansmann, M.; Nentwich, K.; et al. Silent cerebral events/lesions related to atrial fibrillation ablation: A clinical review. J. Cardiovasc. Electrophysiol. 2015, 26, 455–463. [Google Scholar] [CrossRef]
- Neumann, T.; Kuniss, M.; Conradi, G.; Janin, S.; Berkowitsch, A.; Wojcik, M.; Rixe, J.; Erkapic, D.; Zaltsberg, S.; Rolf, A.; et al. MEDAFI-Trial (Microembolization during ablation of atrial fibrillation): Comparison of pulmonary vein isolation using cryoballoon technique vs. radiofrequence energy. Europace 2011, 13, 37–44. [Google Scholar] [CrossRef]
- Haeusler, K.G.; Koch, L.; Herm, J.; Kopp, U.A.; Heuschmann, P.U.; Endres, M.; Schultheiss, H.-P.; Schirdewan, A.; Fiebach, J.B. 3 Tesla MRI-detected brain lesions after pulmonary vein isolation for atrial fibrillation: Results of the MACPAF study. J. Cardiovasc. Electrophysiol. 2013, 24, 14–21. [Google Scholar] [CrossRef]
- Dittrich, R.; Ringelstein, E. Occurrence and clinical impact of microembolic signals during or after cardiosurgical procedures. Stroke 2008, 39, 503–511. [Google Scholar] [CrossRef]
- Schwarz, N.; Kuniss, M.; Nedelmann, M.; Kaps, M.; Bachmann, G.; Neumann, T.; Pitschner, H.F.; Gerriets, T. Neuropsychological decline after catheter ablation of atrial fibrillation. Heart Rhythm 2010, 7, 1761–1767. [Google Scholar] [CrossRef]
- Zhang, J.; Xia, S.J.; Du, X.; Jiang, C.; Lai, Y.W.; Wang, Y.F.; Jia, Z.X.; He, L.; Tang, R.B.; Dong, J.Z.; et al. Incidence and risk factors of post-operative cognitive decline after ablation for atrial fibrillation. BMC Cardiovasc. Disord. 2021, 21, 241. [Google Scholar] [CrossRef]
- Sauren, L.D.; Van Belle, Y.; De Roy, L.; Pison, L.; Meir, M.L.; Van der Veen, F.; Crijns, H.; Jordaens, L.; Mess, W.H.; Maessen, J.G. Transcranial Measurement of cerebral microembolic signals during endocardial pulmonary vein isolation: Comparison of 3 different ablation techniques. J. Cardiovasc. Electrophysiol. 2009, 20, 1102–1107. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, S.; Watanabe, T.; Kajiyama, T.; Iwasawa, J.; Ichijo, S.; Nakamura, H.; Taniguchi, H.; Hirao, K.; Iesaka, Y. Thromboembolic Risks of the prodecural process in second-generation cryoballoon ablation procedures. Circ. Arrhythm. Electrophysiol. 2017, 10, e005612. [Google Scholar] [CrossRef] [PubMed]
- Von Bary, C.; Deneke, T.; Arentz, T.; Schade, A.; Lehrmann, H.; Schwab-Malek, S.; Fredersdorf, S.; Baldaranov, D.; Maier, L.; Schlachetzki, F. Clinical Impact of the Miroembolic Signal Burden During Catheter Ablation for Atrial Fibrillation. Just a Lot of Noise? J. Ultrasound Med. 2018, 37, 1091–1101. [Google Scholar] [CrossRef] [PubMed]
- Spencer, M.P.; Thomas, G.I.; Nicholls, S.C.; Sauvage, L.R. Detection of middle cerebral artery emboli during carotid endarterectomy using transcranial Doppler ultrasonography. Stroke 1990, 21, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Russel, D.; Madden, K.P.; Clark, W.M.; Sandset, P.M.; Zivin, J.A. Detection of arterial emboli using Doppler ultrasound in rabbits. Stroke 1991, 22, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Markus, H.S.; Loh, A.; Brown, M.M. Detection of circulating cerebral emboli using Doppler ultrasound in a seep model. J. Neurol. Sci. 1994, 122, 117–124. [Google Scholar] [CrossRef]
- Ringelstein, E.B.; Droste, D.W.; Babikian, V.L.; Evans, D.H.; Groset, D.G.; Kaps, M.; Markus, H.S.; Russel, D.; Siebler, M. Consensus on Microembolus Detection by TCD. Stroke 1998, 29, 725–729. [Google Scholar] [CrossRef]
- Morris, J.C.; Mohs, R.C.; Rogers, H.; Fillenbaum, G.; Heyman, A. Consortium to establish a registry for Alzheimer’s disease (CERAD) clinical and neuropsychological assessment of Alzheimer’s disease. Psychopharmacol. Bull. 1988, 24, 641–652. [Google Scholar]
- Schmid, N.S.; Ehrensperger, M.M.; Berres, M.; Beck, I.R.; Monsch, A.U. The Extension of the German CERAD Neuropsychological Assessment Battery with Tests Assessing Subcortical, Executive and Frontal Functions Improves Accuracy in Dementia Diagnosis. Dement. Geriatr. Cogn. Dis. Extra 2014, 4, 322–334. [Google Scholar] [CrossRef]
- Maass, F.; Hermann, P.; Varges, D.; Nuhn, S.; van Riesen, C.; Jamous, A.; Focke, N.K.; Hewitt, M.; Leha, A.; Bähr, M.; et al. Prospective CERAD Neuropsychological Assessment in Patients With Multiple System Atrophy. Front. Neurol. 2022, 13, 881369. [Google Scholar] [CrossRef]
- Kaddu-Mulindwa, D.; Heit, M.; Wagenpfeil, G.; Bewarder, M.; Fassbender, K.; Behnke, S.; Yilmaz, U.; Fousse, M. Fewer neurocognitive deficits and less brain atrophy by third ventricle measurement in PLWH treated with modern ART: A prospective analysis. Front. Neurol. 2022, 13, 962535. [Google Scholar] [CrossRef] [PubMed]
- Willmann, C.; Brockmann, K.; Wagner, R.; Kullmann, S.; Preissl, H.; Schnauder, G.; Maetzler, W.; Gasser, T.; Berg, D.; Eschweiler, G.W.; et al. Insulin sensitivity predicts cognitive decline in individuals with prediabetes. BMJ Open Diabetes Res. Care 2020, 8, e001741. [Google Scholar] [CrossRef] [PubMed]
- Von Rennenberg, R.; Liman, T.; Nolte, C.H.; Nave, A.H.; Scheitz, J.F.; Düzel, S.; Regitz-Zagrosek, V.; Gerstorf, D.; Steinhagen-Thiessen, E.; Demuth, I.; et al. High-Sensitivity Cardiac Troponin T and Cognitive Decline in Older Adults: Results of the Berlin Aging Study II. Gerontology 2023, 69, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Berres, M.; Monsch, A.U.; Bernasconi, F.; Thalmann, B.; Stähelin, H.B. Normal ranges of neuropsychological tests for the diagnosis of Alzheimer’s disease. Stud. Health Technol. Inform. 2000, 77, 195–199. [Google Scholar] [PubMed]
- Arbuthnott, K.; Frank, J. Trail making test, part B as a measure of executive control: Validation using a set-switching paradigm. J. Clin. Exp. Neuropsychol. 2000, 22, 518–528. [Google Scholar] [CrossRef]
- Chandler, M.J.; Lacritz, L.H.; Hynan, L.S.; Barnard, H.D.; Allen, G.; Deschner, M.; Weiner, M.F.; Cullum, C.M. A total score for the CERAD neuropsychological battery. Neurology 2005, 65, 102–106. [Google Scholar] [CrossRef]
- Lakhani, M.; Saiful, F.; Parikh, V.; Goyal, N.; Bekheit, S.; Kowalski, M. Recordings of diaphragmatic electromyograms during cryoballoon ablation for atrial fibrillation accurately predict phrenic nerve injury. Heart Rhythm 2014, 11, 369–374. [Google Scholar] [CrossRef]
- Akkaya, E.; Berkowitsch, A.; Zaltsberg, S.; Deubner, N.; Greiss, H.; Hain, A.; Hamm, C.W.; Sperzel, J.; Neumann, T.; Kuniss, M. Safety and feasibility of percutaneous skin closure using purse-string suture compared with compression bandage after pulmonary vein isolation. J. Cardiovasc. Electrophysiol. 2017, 28, 1048–1057. [Google Scholar] [CrossRef]
- Yarlagadda, B.; Deneke, T.; Turagam, M.; Dar, T.; Paleti, S.; Parikh, V.; DiBiase, L.; Halfbass, P.; Santangeli, P.; Mahapatra, S.; et al. Temporal Relationships between Esophageal Injury Type and Progression in Patients Undergoing Atrial Fibrillation Catheter Ablation. Heart Rhythm 2018, 16, 204–212. [Google Scholar] [CrossRef]
- Sarairah, S.Y.; Woodbury, B.; Methachittiphan, N.; Tregoning, D.M.; Sridhar, A.R.; Akoum, N. Esophageal thermal injury following cyroballoon ablation for atrial fibrillation. J. Am. Coll. Cardiol. EP 2020, 6, 262–268. [Google Scholar]
- Deneke, T.; Shin, D.I.; Balta, O.; Bünz, K.; Fassbender, F.; Mügge, A.; Anders, H.; Horlitz, M.; Päsler, M.; Karthikapallil, S.; et al. Post-Ablation Asymptomatic Cerebral Lesions—Long-term Follow-Up Using Magnetic Resonance Imaging. Heart Rhythm 2011, 8, 1705–1711. [Google Scholar] [CrossRef] [PubMed]
- Aryana, A.; Su, W.; Kuniss, M.; Okishige, K.; de Asmundis, C.; Tondo, C.; Chierchia, G.B. Segmental nonocclusive cryoballoon ablation of pulmonary veins and extrapulmonary vein structures: Best practices III. Heart Rhythm 2021, 18, 1435–1444. [Google Scholar] [CrossRef] [PubMed]
- Seidel, G.; Kaps, M.; Gerriets, T. Potential and limitations of transcranial color-coded sonography in stroke patients. Stroke 1995, 26, 2061–2066. [Google Scholar] [CrossRef] [PubMed]
- Postert, T.; Federlein, J.; Przuntek, H.; Büttner, T. Insufficient and absent acoustic temporal bone window: Potential and limitations of transcranial contrast-enhanced color-coded sonography and contrast-enhanced power-based sonography. Ultrasound Med. Biol. 1997, 23, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Wijnhoud, A.D.; Franckena, M.; van der Lugt, A.; Koudstaal, P.J.; Dippel, E.D. Inadequate acoustical temporal bone window in patients with a transient ischemic attack or minor stroke: Role of skull thickness and bone density. Ultrasound Med. Biol. 2008, 34, 923–929. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Age | ≥18 years |
| Atrial fibrillation stage | paroxysmal or persistent |
| Indication for ablation therapy | under current atrial fibrillation guidelines |
| Transcranial bone acoustic window | available unilateral or bilateral |
| Written informed consent | to be provided prior to enrollment |
| Demographics (age, sex, body mass index) |
| Type of atrial fibrillation (paroxysmal vs. persistent) |
| CHA2DS2VASc score |
| Electrocardiography data |
| Echocardiography data |
| Laboratory blood values |
| Comorbidities |
| Current medication |
| Neuropsychological baseline status (1. CERAD Plus test) |
| Available detection site of cerebral microembolic signals |
| Frequency and Characterization of Microembolic Signals over Time: |
|---|
| - Venous access until TSP |
| - TSP |
| - PV/LA Angiography |
| - Cryoballoon introduction into LA |
| - PV occlusion, freeze cycle, and thawing phase for each PV |
| - Left atrial roof ablation (LARA) freeze cycles |
| - Sheath retreat to the RA until inguinal suture |
| EP procedure data: |
| - Procedure time |
| - Fluoroscopic time |
| - Radiation dose |
| - Acute ablation success |
| - Cryoenergy application time |
| - Number of freezes (PV/roofline) |
| - Nadir temperature |
| - Number of isolated PVs |
| - Number of blocked LARA |
| - Amount of contrast agent |
| - Periprocedural complications |
| - Investigator dependency |
| Neuropsychological testing 24 h after PVI |
| Endoscopic esophageal examination 24 to 36 h after PVI, after 2. CERAD Plus test |
| Neuropsychological testing 3 months after PVI |
| Evaluation of mid-term complications |
| Cardiac rhythm evaluation by electrocardiography (resting and 24-hour Holter ECG) |
| Current medication |
| Total (n = 100) | Paroxysmal AF (n = 50) | Persistent AF (n = 50) | p | |
|---|---|---|---|---|
| Age (median, IQR) (years) | 65.5 (58–72) | 66 (57–71) | 65.5 (58.8–74) | 0.564 |
| Sex | ||||
| Male | 69 (69%) | 28 (56%) | 41 (82%) | 0.009 |
| Female | 31 (31%) | 22 (44%) | 9 (18%) | |
| BMI (median, IQR), (Kg/m2) | 28.45 (25.5–33.35) | 27.4 (23.9–31.8) | 30.3 (26.7–34.7) | 0.016 |
| CHA2DS2VASc (median, IQR, range) | 2 (1–3, 0–7) | 2 (1–3) | 2 (1–4) | 0.056 |
| Echocardiography | ||||
| Left atrium diameter (cm) (median, IQR) | 4.17 (3.6–4.6) | 3.8 (3.2–4.2) | 4.6 (4.1–5.0) | <0.001 |
| Left atrium volume (ml) (median, IQR) | 81 (60–102) | 62 (48–83) | 94 (76.5–120.5) | <0.001 |
| Left atrium index (ml/m2) (median, IQR) | 39 (29.9–50.9) | 31.7 (24–38.9) | 48.1 (38.5–56.1) | <0.001 |
| Mitral insufficiency I–II° (median, IQR, range) (n = 77) | I° (I°–I°; I°–II°) | 1 (0–1) | 1 (1–1) | 0.037 |
| Left ejection fraction (median, IQR, range) (%) | 60 (55–60; 40–75) | 60 (60–65) | 55 (50–60) | <0.001 |
| Comorbidities | ||||
| Hypertension | 71 (71%) | 33 (66%) | 38 (76%) | 0.387 |
| Diabetes mellitus | 18 (18%) | 7 (14%) | 11 (22%) | 0.378 |
| LDL (mg/dL) (median, IQR) | 117 (86.5–153.5) | 111 (77–155) | 114 (97–148) | 0.613 |
| Coronary artery disease | 21 (21%) | 10 (20%) | 11 (22%) | 0.999 |
| Sleep apnea | 11 (11%) | 3 (6%) | 8 (16%) | 0.201 |
| Heart insufficiency | ||||
| NT-Pro-BNP (ng/L) (median, IQR) (n = 61) | 417 (86.5–153.5) | 232.5 (138.3–470.5) | 742.0 (206.5–2178.5) | 0.004 |
| Kidney disease | ||||
| eGFR (ml/min/1.73 m2) (median, IQR) | 76 (64.4–88.9) | 77.5 (66.8–89.1) | 75.2 (58.4–89.0) | 0.295 |
| Gastroesophageal reflux disease | 5 (5%) | 3 (6%) | 2 (4%) | 0.999 |
| Previous stroke | 8 (8%) | 2 (4%) | 6 (12%) | 0.269 |
| Severe carotid artery stenosis | 1 (1%) | 0 | 1 (2%) | >0.999 |
| Carotid plaque without hemodynamic relevance | 6 (6%) | 2 (4%) | 4 (8%) | 0.678 |
| Medication prior procedure | ||||
| Intake of oral anticoagulants | 95 (95%) | 45 (90%) | 50 (100%) | 0.056 |
| Intake of platelet inhibitors | 7 (7%) | 1 (2%) | 6 (12%) | 0.112 |
| Intake of proton pump inhibitors | 25 (25%) | 12 (24%) | 13 (26%) | >0.999 |
| Intake of sedative drugs | 14 (14%) | 7 (14%) | 7 (14%) | >0.999 |
| Total (n = 100) | Paroxysmal AF (n = 50) | Persistent AF (n = 50) | p | |
|---|---|---|---|---|
| Procedure time (min) (median, IQR) | 110 (92–128) | 96 (84.5–114.0) | 118.5 (108.8–130.3) | <0.001 |
| Fluoroscopic time (min) (median, IQR) | 26.5 (15.4–26.5) | 18.2 (11.5–23.9) | 23.2 (17.9–30.3) | 0.002 |
| Radiation dose (uGym2) (median, IQR) | 1001 (691.3–1485.3) | 776 (569.7–1516.5) | 1318.5 (970–1613.8) | <0.001 |
| Amount of contrast agent (mL) (median, IQR) | 63 (52–80) | 60 (50–80) | 67 (55–80) | 0.113 |
| Additional right isthmus ablation | 11 (11%) | 7 (14%) | 4 (8%) | 0.525 |
| Pulmonary vein isolation | ||||
| Acute ablation success | 100 (100%) | 50 (100%) | 50 (100%) | 0.999 |
| Total number of freezes (median, IQR) | 5 (4–5) | 5 (4–5) | 5 (4–6) | 0.172 |
| Cryoenergy application time (min) (median, IQR) | 16.16 (15.12–20.0) | 16 (15.2–19.5) | 17.1 (15–22.1) | 0.435 |
| Nadir temperature | ||||
| Nadir temperature RSPV (°C) (median, IQR) | −53 (−56 to −49) | −54 (−56 to −51) | −52 (−56 to −48) | 0.326 |
| Nadir temperature RIPV (°C) (median, IQR) | −51 (−55 to −47) | −52 (−55 to −47) | −50 (−54 to −47) | 0.323 |
| Nadir temperature LSPV (°C) (median, IQR) | −48 (−53 to −45) | −48 (−54 to −44) | −49 (−53 to −46) | 0.218 |
| Nadir temperature LIPV (°C) (median, IQR) | −46 (−51 to −45) | −46 (−48 to −45) | −48 (−54 to −45) | 0.062 |
| Left Atrial Roof Ablation (LARA) | ||||
| Acute ablation success | 91 (91%) | 50 (100%) | 41 (82%) | 0.003 |
| Total number of freezes (median, IQR, range) | 0 (0–4) | 0 (0–0) | 4 (3–4; 3–6) | <0.001 |
| Cryoenergy application time (min) (median, IQR) | 0 (0–720) | 0 (0–0) | 9 (9–18) | <0.001 |
| Nadir temperature (°C) (median, IQR) | 0 (−39 to 0) | 0 (0–0) | −40 (−33 to −46) | <0.001 |
| Acute complications (total) | ||||
| Phrenic nerve injury | 4 (4%) | 3 (6%) | 1 (2%) | 0.617 |
| Pericardial effusion | 0 (0%) | |||
| Stroke/TIA | 0 (0%) | |||
| Vascular groin complication | 0 (0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erkapic, D.; Aleksic, M.; Roussopoulos, K.; Weipert, K.F.; Sözener, K.; Kostev, K.; Allendörfer, J.; Rosenbauer, J.; Guenduez, D.; Tanislav, C. Microembolizations in the Arterial Cerebral Circulation in Patients with Atrial Fibrillation Ablation Using the Cryoballoon Technique—Protocol and Methodology of a Prospective Observational Study. Diagnostics 2023, 13, 1660. https://doi.org/10.3390/diagnostics13091660
Erkapic D, Aleksic M, Roussopoulos K, Weipert KF, Sözener K, Kostev K, Allendörfer J, Rosenbauer J, Guenduez D, Tanislav C. Microembolizations in the Arterial Cerebral Circulation in Patients with Atrial Fibrillation Ablation Using the Cryoballoon Technique—Protocol and Methodology of a Prospective Observational Study. Diagnostics. 2023; 13(9):1660. https://doi.org/10.3390/diagnostics13091660
Chicago/Turabian StyleErkapic, Damir, Marko Aleksic, Konstantinos Roussopoulos, Kay Felix Weipert, Korkut Sözener, Karel Kostev, Jens Allendörfer, Josef Rosenbauer, Dursun Guenduez, and Christian Tanislav. 2023. "Microembolizations in the Arterial Cerebral Circulation in Patients with Atrial Fibrillation Ablation Using the Cryoballoon Technique—Protocol and Methodology of a Prospective Observational Study" Diagnostics 13, no. 9: 1660. https://doi.org/10.3390/diagnostics13091660