
Comparison of Diagnostic Yield and Safety of Serial Pancreatic Juice Aspiration Cytologic Examination (SPACE) with Different Indications
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
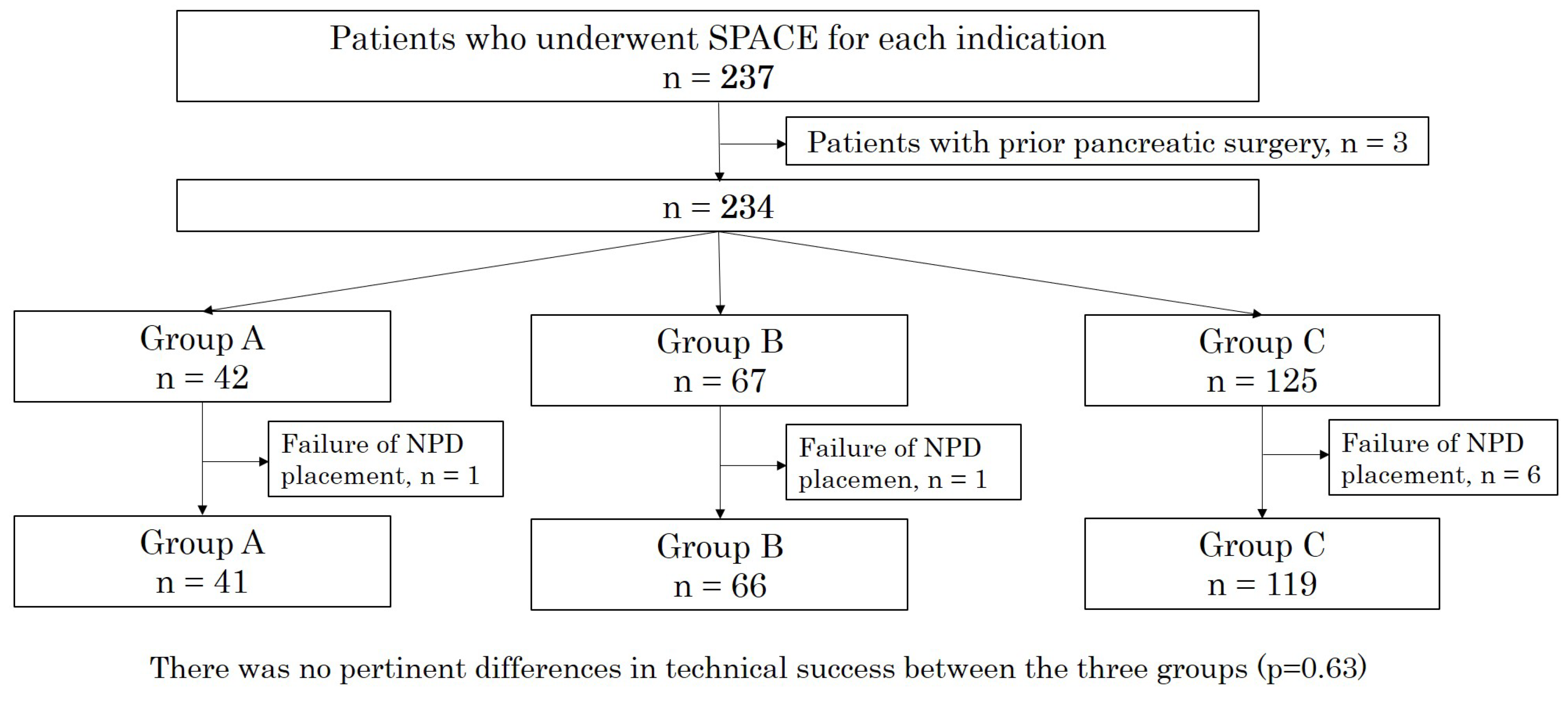
2.1. Study Design
2.2. Placement of Endoscopic NPD Tube and SPACE
2.3. Definitions
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Diagnostic Ability of SPACE
3.3. NPD Tube Related Events and ERCP Related Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Center for Cancer Control and Information Services. Available online: https://ganjoho.jp/reg_stat/statistics/stat/summary (accessed on 12 January 2023).
- Egawa, S.; Toma, H.; Ohigashi, H.; Okusaka, T.; Nakao, A.; Hatori, T.; Maguchi, H.; Yanagisawa, A.; Tanaka, M. Japan pancreatic cancer registry; 30th year anniversary: Japan Pancreas Society. Pancreas 2012, 41, 985–992. [Google Scholar] [CrossRef]
- Amaral, M.J.; Oliveira, R.C.; Donato, P.; Tralhão, J.G. Pancreatic Cancer Biomarkers: Oncogenic Mutations, Tissue and Liquid Biopsies, and Radiomics-A Review. Dig. Dis. Sci. 2023, online ahead of print. [CrossRef]
- Kikuyama, M.; Kamisawa, T.; Kuruma, S.; Chiba, K.; Kawaguchi, S.; Terada, S.; Satoh, T. Early diagnosis to improve the poor prognosis of pancreatic cancer. Cancers 2018, 10, 48. [Google Scholar] [CrossRef] [PubMed]
- Mikata, R.; Ishihara, T.; Tada, M.; Tawada, K.; Saito, M.; Kurosawa, J.; Sugiyama, H.; Sakai, Y.; Tsuyuguchi, T.; Miyazakiet, M.; et al. Clinical usefulness of repeated pancreatic juice cytology via endoscopic naso-pancreatic drainage tube in patients with pancreatic cancer. J. Gastroenterol. 2013, 48, 866–873. [Google Scholar] [CrossRef] [PubMed]
- Iiboshi, T.; Hanada, K.; Fukuda, T.; Yonehara, S.; Sasaki, T.; Chayama, K. Value of cytodiagnosis using endoscopic nasopancreatic drainage for early diagnosis of pancreatic cancer: Establishing a new method for the early detection of pancreatic carcinoma in situ. Pancreas 2012, 41, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Kimura, H.; Furukawa, Y.; Yamasaki, S.; Kagawa, K.; Sakano, A.; Hananoki, M.; Kurushima, H.; Matsumoto, N.; Yamamoto, M.; Tsujita, E.; et al. A study of the usefulness of pancreatic juice cytology obtained via an endoscopic nasal pancreatic drainage (NPD) tube. J. Jpn. Soc. Gastroenterol. 2011, 108, 928–936. [Google Scholar]
- Satoh, T.; Kikuyama, M.; Kawaguch, S.; Kanemoto, H.; Muro, H.; Hanada, K. Acute pancreatitis-onset carcinoma in situ of the pancreas with focal fat replacement diagnosed using serial pancreatic-juice aspiration cytologic examination (SPACE). Clin. J. Gastroenterol. 2017, 10, 541–545. [Google Scholar] [CrossRef]
- Kaneko, J.; Ishiwatari, H.; Sasaki, K.; Yasuda, I.; Takahashi, K.; Imura, J.; Iwashita, T.; Uemura, S.; Hatano, Y.; Miyazaki, T.; et al. Macroscopic visible core length can predict the histological sample quantity in endoscopic ultrasound-guided tissue acquisition: Multicenter prospective study. Dig. Endosc. 2022, 34, 622–631. [Google Scholar] [CrossRef]
- Ishiwatari, H.; Sato, J.; Fujie, S.; Sasaki, K.; Kaneko, J.; Satoh, T.; Matsubayashi, H.; Kishida, Y.; Yoshida, M.; Ito, S.; et al. Gross visual inspection by endosonographers during endoscopic ultrasound-guided fine needle aspiration. Pancreatology 2019, 19, 191–195. [Google Scholar] [CrossRef]
- Kanno, A.; Yasuda, I.; Irisawa, A.; Hara, K.; Ashida, R.; Iwashita, T.; Takenaka, M.; Katanuma, A.; Takikawa, T.; Kubota, K.; et al. Adverse events of endoscopic ultrasound-guided fine-needle aspiration for histologic diagnosis in Japanese tertiary centers: Multicenter retrospective study. Dig. Endosc. 2021, 33, 1146–1157. [Google Scholar] [CrossRef]
- Nakai, Y.; Hamada, T.; Hakuta, R.; Ishigaki, K.; Saito, K.; Saito, T.; Takahara, N.; Mizuno, S.; Kogure, H.; Koike, K.; et al. Endoscopic ultrasonography-guided tissue acquisition for small solid pancreatic lesions: Does the size matter? DEN Open 2021, 2, e52. [Google Scholar] [CrossRef] [PubMed]
- Yamakawa, K.; Masuda, A.; Nakagawa, T.; Shiomi, H.; Toyama, H.; Takenaka, M.; Sakai, A.; Kobayashi, T.; Tsujimae, M.; Ashinaet, S.; et al. Evaluation of efficacy of pancreatic juice cytology for risk classification according to international consensus guidelines in patients with intraductal papillary mucinous neoplasm; a retrospective study. Pancreatology 2019, 19, 424–428. [Google Scholar] [CrossRef]
- Tanaka, M.; Castillo, C.F.; Kamisawa, T.; Jang, J.Y.; Levy, P.; Ohtsuka, T.; Salvia, R.; Shimizu, Y.; Tada, Y.; Wolfgang, C.L. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology 2017, 17, 738–753. [Google Scholar] [CrossRef] [PubMed]
- Cotton, P.B.; Garrow, D.A.; Gallagher, J.; Romagnuolo, J. Risk factors for complications after ERCP: A multivariate analysis of 11,497 procedures over 12 years. Gastrointest. Endosc. 2009, 70, 80–88. [Google Scholar] [CrossRef]
- Cotton, P.B.; Eisen, G.M.; Aabakken, L.; Baron, T.H.; Hutter, M.M.; Jacobson, B.C.; Mergener, K.; Nemcek, A., Jr.; Petersen, B.T.; Petrini, J.L.; et al. A lexicon for endoscopic adverse events: Report of an ASGE workshop. Gastrointest. Endosc. 2010, 71, 446–454. [Google Scholar] [CrossRef]
- Endo, Y.; Morii, T.; Tamura, H.; Okuda, S. Cytodiagnosis of pancreatic malignant tumors by aspiration, under direct vision, using a duodenal fiberscope. Gastroenterology 1974, 67, 944–951. [Google Scholar] [CrossRef]
- Hatfield, A.R.; Smithies, A.; Wilkins, R.; Levi, A.J. Assessment of endoscopic retrograde cholangio-pancreatography (ERCP) and pure pancreatic juice cytology in patients with pancreatic disease. Gut 1976, 17, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Kameya, S.; Kuno, N.; Kasugai, T. The diagnosis of pancreatic cancer by pancreatic juice cytology. Acta Cytol. 1981, 25, 354–360. [Google Scholar]
- Mitchell, M.L.; Carney, C.N. Cytologic criteria for the diagnosis of pancreatic carcinoma. Am. J. Clin. Pathol. 1985, 83, 171–176. [Google Scholar] [CrossRef]
- Nakaizumi, A.; Tatsuta, M.; Uehara, H.; Yamamoto, R.; Takenaka, A.; Kishigami, Y.; Takemura, K.; Kitarnura, T.; Okuda, S. Cytologic examination of pure pancreatic juice in the diagnosis of pancreatic carcinoma. The endoscopic retrograde intraductal catheter aspiration cytologic technique. Cancer 1992, 70, 2610–2614. [Google Scholar] [CrossRef]
- Ikemoto, J.; Serikawa, M.; Hanada, K.; Eguchi, N.; Sasaki, T.; Fujimoto, Y.; Sugiyama, S.; Yamaguchi, A.; Noma, B.; Kamigaki, M.; et al. Clinical Analysis of Early-Stage Pancreatic Cancer and Proposal for a New Diagnostic Algorithm: AMulticenter Observational Study. Diagnostics 2021, 11, 287. [Google Scholar] [CrossRef] [PubMed]
- Rofi, E.; Vivaldi, C.; Del Re, M.; Arrigoni, E.; Crucitta, S.; Funel, N.; Fogli, S.; Vasile, E.; Musettini, G.; Fornaro, L.; et al. The emerging role of liquid biopsy in diagnosis, prognosis and treatment monitoring of pancreatic cancer. Pharmacogenomics 2019, 20, 49–68. [Google Scholar] [CrossRef] [PubMed]
- Loftus, E.V., Jr.; Olivares-Pakzad, B.A.; Batts, K.P.; Adkins, M.C.; Stephens, D.H.; Sarr, M.G.; DiMagno, E.P. Intraductal papillary-mucinous tumors of the pancreas: Clinicopathologic features, outcome, and nomenclature. Members of the pancreas Clinic, and pancreatic Surgeons of Mayo Clinic. Gastroenterology 1996, 110, 1909–1918. [Google Scholar] [CrossRef] [PubMed]
- Uehara, H.; Nakaizumi, A.; Iishi, H.; Lishi, H.; Tatsuta, M.; Kitamra, T.; Okuda, S.; Ohigashi, H.; Ishikawa, O.; Takenaka, A.; et al. Cytologic examination of pancreatic juice for differential diagnosis of benign and malignant mucin-producing tumors of the pancreas. Cancer 1994, 74, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, M.; Hirokawa, M.; Manabe, T.; Mikami, Y.; Kanahara, T.; Miyake, Y.; Iwamoto, S.; Tsunoda, T. Cytologic findings in noninvasive intraductal papillary-mucinous carcinoma of the pancreas. A report of two cases. Acta Cytol. 1999, 43, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Wiesenauer, C.A.; Schmidt, C.M.; Cummings, O.W.; Yiannoutsos, C.T.; Howard, T.J.; Wiebke, E.A.; Goulet, R.J., Jr.; McHenry, L.; Sherman, S.; Lehman, G.A.; et al. Preoperative predictors of malignancy in pancreatic intraductal papillary mucinous neoplasms. Arch. Surg. 2003, 138, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Kawai, M.; Uchiyama, K.; Tani, M.; Onishi, R.; Kinoshita, H.; Ueno, M.; Hama, T.; Yamaue, H. Clinicopathological features of malignant intraductal papillary mucinous tumors of the pancreas: The differential diagnosis from benign entities. Arch. Surg. 2004, 139, 188–192. [Google Scholar] [CrossRef]
- McGuire, D.E.; Venu, R.P.; Brown, R.D.; Etzkorn, K.P.; Glaws, W.R.; Abu-Hammour, A. Brush cytology for pancreatic carcinoma: An analysis of factors influencing results. Gastrointest. Endosc. 1996, 44, 300–304. [Google Scholar] [CrossRef]
- Vandervoort, J.; Soetikno, R.M.; Montes, H.; Lichtenstein, D.R.; Dam, J.V.; Ruymann, F.W.; Cibas, E.S.; Carr-Locke, D.L. Accuracy and complication rate of brush cytology from bile duct versus pancreatic duct. Gastrointest. Endosc. 1999, 49, 322–327. [Google Scholar] [CrossRef]
- Uchida, N.; Kamada, H.; Tsutsui, K.; Ono, M.; Aritomo, Y.; Masaki, T.; Kushida, Y.; Haba, R.; Nakatsu, T.; Kuriyama, S. Utility of pancreatic duct brushing for diagnosis of pancreatic carcinoma. J. Gastroenterol. 2007, 42, 657–662. [Google Scholar] [CrossRef]
- Kawaguchi, S.; Kikuyama, M.; Satoh, T.; Terada, S. Use of nasopancreatic drainage for severe post-endoscopic retrograde cholangiopancreatography pancreatitis: A case series. Intern. Med. 2018, 57, 2657–2662. [Google Scholar] [CrossRef] [PubMed]
- Rocca, R.; De Angelis, C.; Daperno, M.; Carucci, P.; Ravarino, N.; Bruno, M.; Crocellà, L.; Lavagna, A.; Fracchia, M.; Pacchioni, D.; et al. Endoscopic ultrasound-fine needle aspiration (EUS-FNA) for pancreatic lesions: Effectiveness in clinical practice. Dig. Liver Dis. 2007, 39, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Touchefeu, Y.; Le Rhun, M.; Coron, E.; Alamdari, A.; Heymann, M.F.; Mosnier, J.F.; Matysiak, T.; Galmiche, J.P. Endoscopic ultrasound-guided fine-needle aspiration for the diagnosis of solid pancreatic masses: The impact on patient-management strategy. Aliment. Pharmacol. Ther. 2009, 30, 1070–1077. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Group A (n = 41) | Group B (n = 66) | Group C (n = 119) | p-Value | |
|---|---|---|---|---|
| Median age, year (range) | 72 (42–83) | 71.5 (33–84) | 73 (49–87) | 0.16 |
| Sex, male, n (%) | 28 (68) | 38 (58) | 66 (55) | 0.36 |
| Location of the target lesion, head, n (%) | 22 (54) | 17 (26) | 71 (60) | <0.01 |
| Maximum diameter of the MPD, mm (range) | 4 (1–13) | 4 (2–15) | 5 (2–16) | <0.01 |
| History of acute pancreatitis, n (%) | 6 (15) | 21 (32) | 5 (4) | <0.01 |
| Size of pancreatic mass, mm (range) | 17 (7–55) | – | – | – |
| Macroscopic type of IPMN, MD/BD/MX, n (%) | – | – | 12 (10)/62 (52)/45 (38) | – |
| Risk classification, according to ICG 2017, HRS/WF/others, n (%) | – | – | 33 (28)/70 (59)/16 (13) | – |
| The size of NPD tube, 5Fr/6Fr, n (%) | 41(100)/0(0) | 65(98)/1(2) | 106(89)/13(11) | <0.01 |
| The median number of cytology samples, times (range) | 6 (4–7) | 6 (3–7) | 6 (1–7) | 0.23 |
| Final diagnosis, malignant, n (%) | 29 (71) | 14 (21) | 22 (18) | <0.01 |
| Group (n) | Result of SPACE | Malignant | Sp | Se | PPV | NPV | Accuracy | |
|---|---|---|---|---|---|---|---|---|
| Yes | No | [95% CI] | [95% CI] | [95% CI] | [95% CI] | [95% CI] | ||
| (n) | (n) | (%) | (%) | (%) | (%) | (%) | ||
| Group A | Positive | TP = 20 | FP = 9 | 69.0 | 100 | 100 | 57.1 | 78.0 |
| (n = 41) | Negative | FN = 0 | TN = 12 | [49.2–84.7] | [73.5–100] | [83.2–100] | [34.0–78.2] | [62.4–89.4] |
| Group B | Positive | 11 | 3 | 78.6 | 98.1 | 91.7 | 94.4 | 93.9 |
| (n = 66) | Negative | 1 | 51 | [49.2–95.3] | [89.7–100] | [61.5–99.8] | [84.6–98.8] | [85.2–98.3] |
| Group C | Positive | 6 | 16 | 27.3 | 86.6 | 31.6 | 84.0 | 75.6 |
| (n = 119) | Negative | 13 | 84 | [10.7–50.2] | [78.2–92.7] | [12.6–56.6] | [75.3–90.6] | [66.9–83.0] |
| p-value for comparison between groups | p = 0.002 | p = 0.039 | p < 0.001 | p < 0.001 | p = 0.004 | |||
| Size of Detected Mass | Correct Diagnosis | Incorrect Diagnosis | p |
|---|---|---|---|
| 1–10 mm | 6 (18.8%) | 0 (0%) | <0.001 |
| 11–20 mm | 22 (68.8%) | 3 (33.3%) | |
| ≧21 mm | 4 (12.5%) | 6 (66.7%) |
| Group A (n = 41) | Group B (n = 66) | Group C (n = 119) | p-Value | |
|---|---|---|---|---|
| NPD-related events, n (%) | 0 (0) | 1 (1.5) | 5 (4.2) | 0.22 |
| Dislocation, n (%) | 0 (0) | 1 (1.5) | 4 (3.4) | - |
| Occlusion, n (%) | 0 (0) | 0 (0) | 1 (0.8) | - |
| Accidental removal, n (%) | 0 (0) | 0 (0) | 0 (0) | - |
| ERCP-related adverse event, n (%) | ||||
| PEP | 3 (7.3) | 3 (4.5) | 15 (13) | 0.20 |
| Mild, n (%) | 3 (7.3) | 2 (3.0) | 14 (12) | - |
| Moderate, n (%) | 0 (0) | 0 (0) | 1 (0.8) | - |
| Severe, n (%) | 0 (0) | 0 (0) | 0 (0) | - |
| Cholangitis, mild, n (%) | 0 (0) | 1 (1.5) | 1 (0.8) | 1.00 |
| Factors | Univariate | |||
|---|---|---|---|---|
| OR | 95% CI | p | ||
| Age | >75 | 0.77 | 0.27–2.11 | 0.65 |
| ≤74 | 1 | |||
| Sex | Male | 0.76 | 0.28–2.10 | 0.64 |
| Female | 1 | |||
| MPD size | ≥5 mm | 0.58 | 0.18–1.66 | 0.35 |
| <5 mm | 1 | |||
| Indication | IPMN | 2.41 | 0.85–7.92 | 0.11 |
| not IPMN | 1 | |||
| History of | Yes | 1.01 | 0.18–3.80 | 1.00 |
| acute pancreatitis | None | 1 | ||
| Location of target | Pbt | 1.61 | 0.59–4.67 | 0.36 |
| lesion | Ph | 1 | ||
| Size of NPD tube | 6Fr | 0.74 | 0.02–5.44 | 1.00 |
| 5Fr | 1 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Satoh, T.; Kawaguchi, S.; Takeda, S.; Ishiguro, Y.; Asahara, K.; Terada, S.; Endo, S.; Shirane, N.; Kanemoto, H.; Ohno, K. Comparison of Diagnostic Yield and Safety of Serial Pancreatic Juice Aspiration Cytologic Examination (SPACE) with Different Indications. Diagnostics 2023, 13, 1498. https://doi.org/10.3390/diagnostics13081498
Satoh T, Kawaguchi S, Takeda S, Ishiguro Y, Asahara K, Terada S, Endo S, Shirane N, Kanemoto H, Ohno K. Comparison of Diagnostic Yield and Safety of Serial Pancreatic Juice Aspiration Cytologic Examination (SPACE) with Different Indications. Diagnostics. 2023; 13(8):1498. https://doi.org/10.3390/diagnostics13081498
Chicago/Turabian StyleSatoh, Tatsunori, Shinya Kawaguchi, Shodai Takeda, Yuya Ishiguro, Kazuhisa Asahara, Shuzo Terada, Shinya Endo, Naofumi Shirane, Hideyuki Kanemoto, and Kazuya Ohno. 2023. "Comparison of Diagnostic Yield and Safety of Serial Pancreatic Juice Aspiration Cytologic Examination (SPACE) with Different Indications" Diagnostics 13, no. 8: 1498. https://doi.org/10.3390/diagnostics13081498