
Rapid Detection of Mycobacterium Tuberculosis Using a Novel Point-of-Care BZ TB/NTM NALF Assay: Integrating LAMP and LFIA Technologies


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Selection and Study Design
2.2. DNA Extraction and RT-PCR
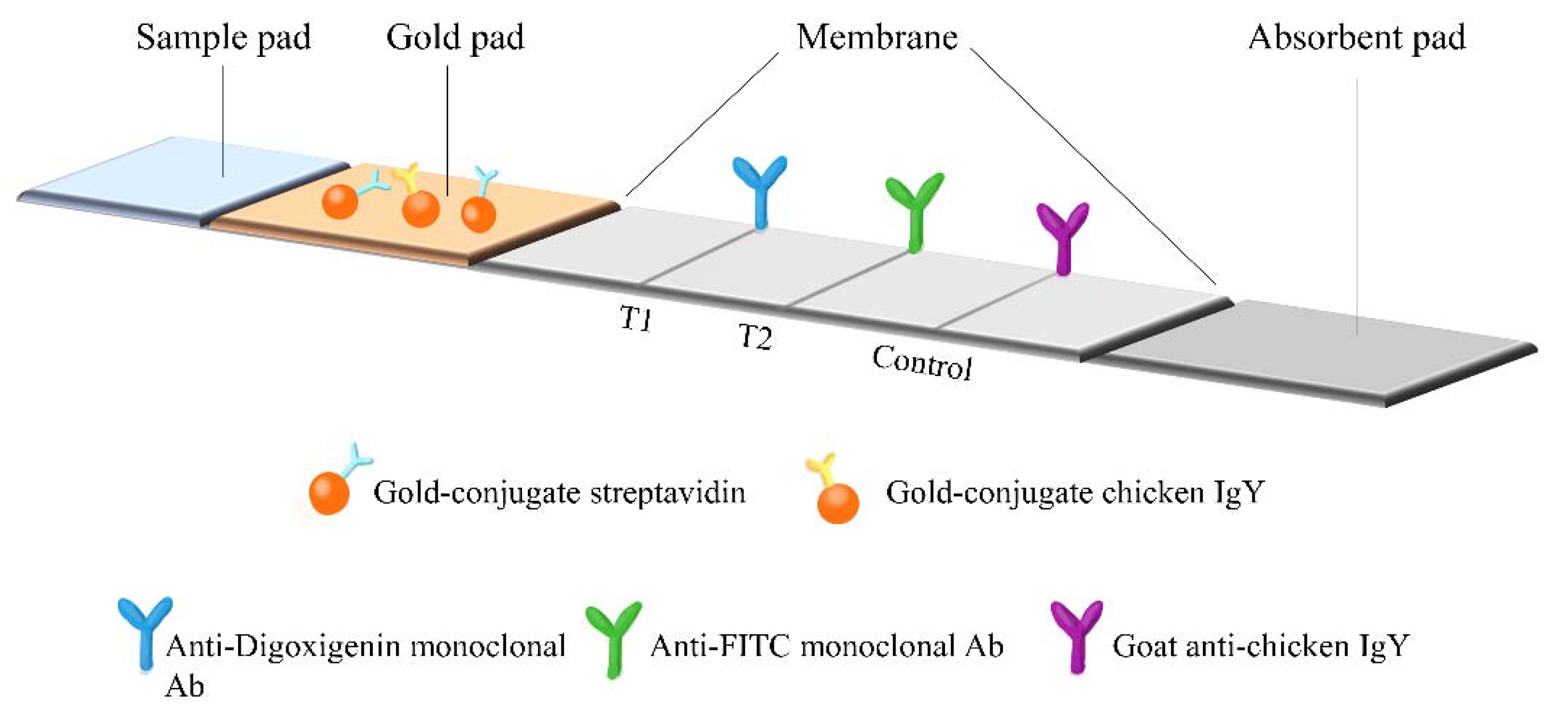
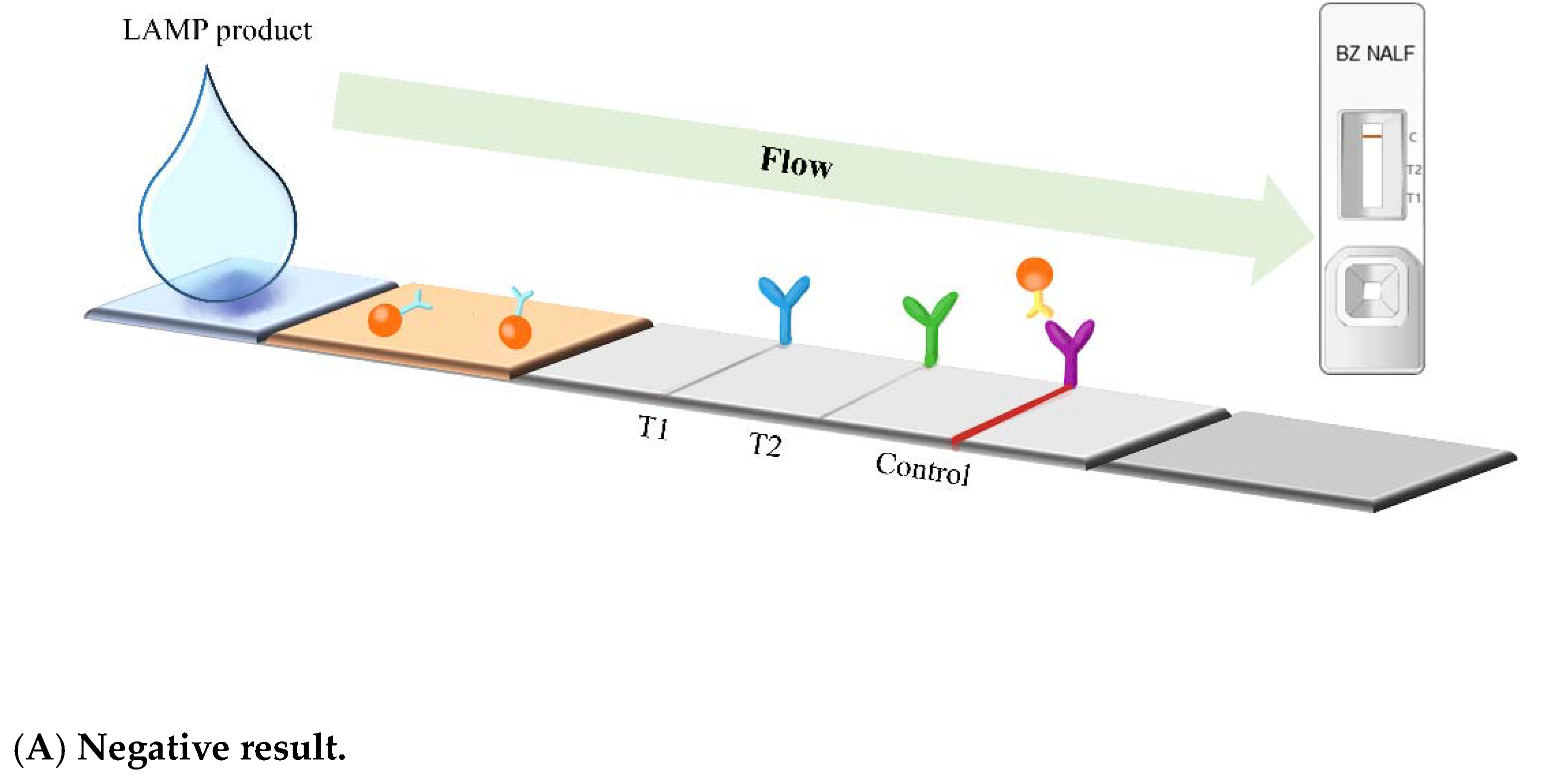
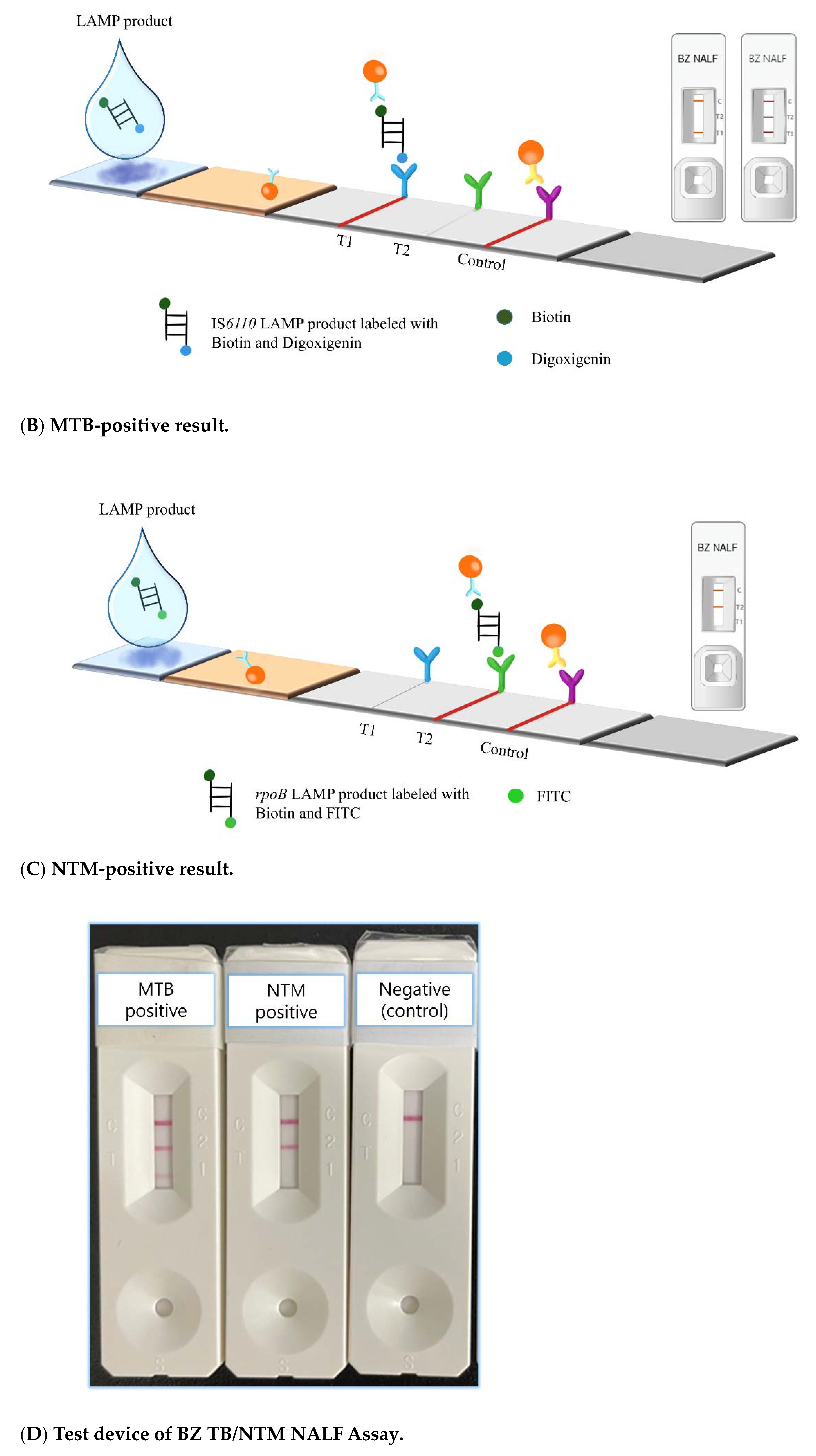
2.3. BZ TB/NTM NALF Assay
2.4. Interpretation of BZ TB/NTM NALF Assay Results
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Global Tuberculosis Report 2022; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- Tiemersma, E.W.; van der Werf, M.J.; Borgdorff, M.W.; Williams, B.; Nagelkerke, N.J.D. Natural History of Tuberculosis: Duration and Fatality of Untreated Pulmonary Tuberculosis in HIV Negative Patients: A Systematic Review. PLoS ONE 2011, 6, e17601. [Google Scholar] [CrossRef] [PubMed]
- Caulfield, A.J.; Wengenack, N.L. Diagnosis of active tuberculosis disease: From microscopy to molecular techniques. J. Clin. Tuberc. Other Mycobact. Dis. 2016, 4, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Lewinsohn, D.M.; Leonard, M.K.; LoBue, P.A.; Cohn, D.L.; Daley, C.L.; Desmond, E.; Keane, J.; Lewinsohn, D.A.; Loeffler, A.M.; Mazurek, G.H. Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention clinical practice guidelines: Diagnosis of tuberculosis in adults and children. Clin. Infect. Dis. 2017, 64, e1–e33. [Google Scholar] [CrossRef] [PubMed]
- Kwak, N.; Choi, S.M.; Lee, J.; Park, Y.S.; Lee, C.-H.; Lee, S.-M.; Yoo, C.-G.; Kim, Y.W.; Han, S.K.; Yim, J.-J. Diagnostic Accuracy and Turnaround Time of the Xpert MTB/RIF Assay in Routine Clinical Practice. PLoS ONE 2013, 8, e77456. [Google Scholar] [CrossRef] [PubMed]
- Dunn, J.J.; Starke, J.R.; Revell, P.A. Laboratory Diagnosis of Mycobacterium tuberculosis Infection and Disease in Children. J. Clin. Microbiol. 2016, 54, 1434–1441. [Google Scholar] [CrossRef] [PubMed]
- WHO. Prerequisites to Country Implementation of Xpert MTB/RIF and Key Action Points at Country Level: Checklist; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Meyer-Rath, G.; Schnippel, K.; Long, L.; MacLeod, W.; Sanne, I.; Stevens, W.; Pillay, S.; Pillay, Y.; Rosen, S. The Impact and Cost of Scaling up GeneXpert MTB/RIF in South Africa. PLoS ONE 2012, 7, e36966. [Google Scholar] [CrossRef]
- WHO. Global Tuberculosis Report 2021; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Wong, Y.P.; Othman, S.; Lau, Y.L.; Radu, S.; Chee, H.-Y. Loop-mediated isothermal amplification (LAMP): A versatile technique for detection of micro-organisms. J. Appl. Microbiol. 2018, 124, 626–643. [Google Scholar] [CrossRef]
- Notomi, T.; Okayama, H.; Masubuchi, H.; Yonekawa, T.; Watanabe, K.; Amino, N.; Hase, T. Loop-mediated isothermal amplification of DNA. Nucleic Acids Res. 2000, 28, E63. [Google Scholar] [CrossRef]
- Mautner, L.; Baillie, C.-K.; Herold, H.M.; Volkwein, W.; Guertler, P.; Eberle, U.; Ackermann, N.; Sing, A.; Pavlovic, M.; Goerlich, O.; et al. Rapid point-of-care detection of SARS-CoV-2 using reverse transcription loop-mediated isothermal amplification (RT-LAMP). Virol. J. 2020, 17, 1–14. [Google Scholar] [CrossRef]
- Jiang, X.; Lillehoj, P.B. Lateral flow immunochromatographic assay on a single piece of paper. Analyst 2020, 146, 1084–1090. [Google Scholar] [CrossRef]
- Chen, A.; Yang, S. Replacing antibodies with aptamers in lateral flow immunoassay. Biosens. Bioelectron. 2015, 71, 230–242. [Google Scholar] [CrossRef]
- Banerjee, R.; Jaiswal, A. Recent advances in nanoparticle-based lateral flow immunoassay as a point-of-care diagnostic tool for infectious agents and diseases. Analyst 2018, 143, 1970–1996. [Google Scholar] [CrossRef] [PubMed]
- Kamphee, H.; Chaiprasert, A.; Prammananan, T.; Wiriyachaiporn, N.; Kanchanatavee, A.; Dharakul, T. Rapid Molecular Detection of Multidrug-Resistant Tuberculosis by PCR-Nucleic Acid Lateral Flow Immunoassay. PLoS ONE 2015, 10, e0137791. [Google Scholar] [CrossRef] [PubMed]
- Amiruddin, M.M.; Ang, G.Y.; Yu, C.Y.; Falero-Diaz, G.; Otero, O.; Reyes, F.; Camacho, F.; Chin, K.; Sarmiento, M.; Norazmi, M.; et al. Development of an immunochromatographic lateral flow dipstick for the detection of Mycobacterium tuberculosis 16 kDa antigen (Mtb-strip). J. Microbiol. Methods 2020, 176, 106003. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Ma, Y.; Liu, R.; Shang, Y.; Ma, L.; Huo, F.; Li, Y.; Shu, W.; Wang, Y.; Gao, M.; et al. Diagnostic Yield of Oral Swab Testing by TB-LAMP for Diagnosis of Pulmonary Tuberculosis. Infect. Drug Resist. 2021, 14, 89–95. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Consolidated Guidelines on Tuberculosis. Module 3: Diagnosis-Rapid Diagnostics for Tuberculosis Detection; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Shete, P.B.; Farr, K.; Strnad, L.; Gray, C.M.; Cattamanchi, A. Diagnostic accuracy of TB-LAMP for pulmonary tuberculosis: A systematic review and meta-analysis. BMC Infect. Dis. 2019, 19, 268. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.; Hanrahan, C.; Wang, Z.Y.; Dendukuri, N.; Lawn, S.D.; Denkinger, C.M.; Steingart, K.R. Lateral flow urine lipoarabinomannan assay for detecting active tuberculosis in HIV-positive adults. Cochrane Database Syst. Rev. 2016, 5, CD011420-108. [Google Scholar] [CrossRef] [PubMed]
- Thierry, D.; Brisson-Noël, A.; Vincent-Lévy-Frébault, V.; Nguyen, S.; Guesdon, J.L.; Gicquel, B. Characterization of a Mycobacterium tuberculosis insertion sequence, IS6110, and its application in diagnosis. J. Clin. Microbiol. 1990, 28, 2668–2673. [Google Scholar] [CrossRef]
- Salah, I.B.; Adékambi, T.; Raoult, D.; Drancourt, M. rpoB sequence-based identification of Mycobacterium avium complex species. Microbiology 2008, 154, 3715–3723. [Google Scholar] [CrossRef]
- Lawn, S.D.; Nicol, M.P. Xpert® MTB/RIF assay: Development, evaluation and implementation of a new rapid molecular diagnostic for tuberculosis and rifampicin resistance. Futur. Microbiol. 2011, 6, 1067–1082. [Google Scholar] [CrossRef]
- Blakemore, R.; Story, E.; Helb, D.; Kop, J.; Banada, P.; Owens, M.R.; Chakravorty, S.; Jones, M.; Alland, D. Evaluation of the analytical performance of the Xpert MTB/RIF assay. J. Clin. Microbiol. 2010, 48, 2495–2501. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Park, B.G.; Lim, D.H.; Jang, W.S.; Nam, J.; Mihn, D.-C.; Lim, C.S. Development and evaluation of a multiplex loop-mediated isothermal amplification (LAMP) assay for differentiation of Mycobacterium tuberculosis and non-tuberculosis mycobacterium in clinical samples. PLoS ONE 2021, 16, e0244753. [Google Scholar] [CrossRef] [PubMed]
- Nagai, K.; Horita, N.; Yamamoto, M.; Tsukahara, T.; Nagakura, H.; Tashiro, K.; Shibata, Y.; Watanabe, H.; Nakashima, K.; Ushio, R.; et al. Diagnostic test accuracy of loop-mediated isothermal amplification assay for Mycobacterium tuberculosis: Systematic review and meta-analysis. Sci. Rep. 2016, 6, 39090. [Google Scholar] [CrossRef] [PubMed]
- Raviglione, M.; Director, G. Global Strategy and Targets for Tuberculosis Prevention, Care and Control after 2015: Report by the Secretariat; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- WHO. Tuberculosis. World Health Organization. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/tuberculosis. (accessed on 24 February 2023).
- Hogan, A.B.; Jewell, B.L.; Sherrard-Smith, E.; Vesga, J.F.; Watson, O.J.; Whittaker, C.; Hamlet, A.; Smith, J.A.; Winskill, P.; Verity, R.; et al. Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: A modelling study. Lancet Glob. Health 2020, 8, e1132–e1141. [Google Scholar] [CrossRef]
- WHO. Automated Real-Time Nucleic Acid Amplification Technology for Rapid and Simultaneous Detection of Tuberculosis and Rifampicin Resistance: Xpert MTB/RIF System: Policy Statement; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Steingart, K.R.; Schiller, I.; Horne, D.J.; Pai, M.; Boehme, C.C.; Dendukuri, N.; Tollefson, D.; Schumacher, S.G.; Ochodo, E.A.; Pai, M.; et al. Xpert® MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults. Cochrane Database Syst. Rev. 2014, 1, CD009593. [Google Scholar] [CrossRef] [PubMed]
- Son, E.; Jang, J.; Kim, T.; Jang, J.H.; Chung, J.H.; Seol, H.Y.; Yeo, H.J.; Yoon, S.H.; Lee, S.E.; Cho, W.H.; et al. Head-to-Head Comparison between Xpert MTB/RIF Assay and Real-Time Polymerase Chain Reaction Assay Using Bronchial Washing Specimens for Tuberculosis Diagnosis. Tuberc. Respir. Dis. 2022, 85, 89–95. [Google Scholar] [CrossRef]
- Ko, Y.; Lee, H.-K.; Lee, Y.S.; Kim, M.-Y.; Shin, J.H.; Shim, E.-J.; Park, S.Y.; Mo, E.K.; Park, Y.B. Accuracy of Xpert® MTB/RIF assay compared with AdvanSure™ TB/NTM real-time PCR using bronchoscopy specimens. Int. J. Tuberc. Lung Dis. 2016, 20, 115–120. [Google Scholar] [CrossRef]
- Hanrahan, C.F.; Haguma, P.; Ochom, E.; Kinera, I.; Cobelens, F.; Cattamanchi, A.; Davis, L.; Katamba, A.; Dowdy, D. Implementation of Xpert MTB/RIF in Uganda: Missed Opportunities to Improve Diagnosis of Tuberculosis. Open Forum Infect. Dis. 2016, 3, ofw068. [Google Scholar] [CrossRef]
- Cowan, J.; Michel, C.; Manhiça, I.; Monivo, C.; Saize, D.; Creswell, J.; Gloyd, S.; Micek, M. Implementing rapid testing for tuberculosis in Mozambique. Bull. World Health Organ. 2014, 93, 125–130. [Google Scholar] [CrossRef]
- Dhama, K.; Karthik, K.; Chakrabort, S.; Tiwari, R.; Kapoor, S.; Kumar, A.; Thomas, P. Loop-mediated Isothermal Amplification of DNA (LAMP): A New Diagnostic Tool Lights the World of Diagnosis of Animal and Human Pathogens: A Review. Pak. J. Biol. Sci. 2014, 17, 151–166. [Google Scholar] [CrossRef]
- Cai, S.; Jung, C.; Bhadra, S.; Ellington, A.D. Phosphorothioated Primers Lead to Loop-Mediated Isothermal Amplification at Low Temperatures. Anal. Chem. 2018, 90, 8290–8294. [Google Scholar] [CrossRef] [PubMed]
- Koczula, K.M.; Gallotta, A. Lateral flow assays. Essays Biochem. 2016, 60, 111–120. [Google Scholar] [PubMed]
- Seki, M.; Kim, C.-K.; Hayakawa, S.; Mitarai, S. Recent advances in tuberculosis diagnostics in resource-limited settings. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1405–1410. [Google Scholar] [CrossRef] [PubMed]
- Cheng, V.C.C.; Yam, W.C.; Hung, I.F.N.; Woo, P.C.Y.; Lau, S.K.P.; Tang, B.S.F.; Yuen, K.Y. Clinical evaluation of the polymerase chain reaction for the rapid diagnosis of tuberculosis. J. Clin. Pathol. 2004, 57, 281–285. [Google Scholar] [CrossRef]
- Rimal, R.; Shrestha, D.; Pyakurel, S.; Poudel, R.; Shrestha, P.; Rai, K.R.; Ghimire, G.R.; Rai, G.; Rai, S.K. Diagnostic performance of GeneXpert MTB/RIF in detecting MTB in smear-negative presumptive TB patients. BMC Infect. Dis. 2022, 22, 321. [Google Scholar] [CrossRef]
- Lee, J.S.; Kim, E.-C.; Joo, S.I.; Lee, S.-M.; Yoo, C.-G.; Kim, Y.W.; Han, S.K.; Shim, Y.-S.; Yim, J.-J. The Incidence and Clinical Implication of Sputum with Positive Acid-Fast Bacilli Smear But Negative in Mycobacterial Culture in a Tertiary Referral Hospital in South Korea. J. Korean Med. Sci. 2008, 23, 767–771. [Google Scholar] [CrossRef]
- Parsons, L.M.; Somoskövi, A.; Gutierrez, C.; Lee, E.; Paramasivan, C.N.; Abimiku, A.; Spector, S.; Roscigno, G.; Nkengasong, J. Laboratory Diagnosis of Tuberculosis in Resource-Poor Countries: Challenges and Opportunities. Clin. Microbiol. Rev. 2011, 24, 314–350. [Google Scholar] [CrossRef]
- Barnard, D.A.; Irusen, E.M.; Bruwer, J.W.; Plekker, D.; Whitelaw, A.C.; Deetlefs, J.D.; Koegelenberg, C.F.N. The utility of Xpert MTB/RIF performed on bronchial washings obtained in patients with suspected pulmonary tuberculosis in a high prevalence setting. BMC Pulm. Med. 2015, 15, 103. [Google Scholar] [CrossRef]
- Lijmer, J.G.; Mol, B.W.; Heisterkamp, S.; Bonsel, G.J.; Prins, M.H.; Van Der Meulen, J.H.P.; Bossuyt, P.M.M. Empirical Evidence of Design-Related Bias in Studies of Diagnostic Tests. JAMA 1999, 282, 1061–1066. [Google Scholar] [CrossRef]
- Ransohoff, D.F.; Feinstein, A.R. Problems of Spectrum and Bias in Evaluating the Efficacy of Diagnostic Tests. N. Engl. J. Med. 1978, 299, 926–930. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Type of Assay | RT-PCR | Performance (95% Confidence Interval, %) | |||||
|---|---|---|---|---|---|---|---|
| Positive | Negative | Sensitivity | Specificity | PPV | NPV | ||
| BZ TB/NTMNALF Assay | Positive | 79 | 1 | 98.7% (93.2–99.9%) | 99.1% (95.2–99.9%) | 98.7% (91.8–99.8%) | 99.1% (94.2–99.8%) |
| Negative | 1 | 114 | |||||
| Culture | Positive | 68 | 0 | 85.0% (75.3–92.0%) | 100% (96.8–100%) | 100% | 90.5% (85.0–94.2%) |
| Negative | 12 | 115 | |||||
| Sex | Age | TB PCR Result | Specimen | Clinical Diagnosis | Anti-TB Treatment | CXR, CT or Biopsy | |
|---|---|---|---|---|---|---|---|
| 1 | M | 82 | AdvanSure | Pleural fluid | TB pleurisy | Performed | CT: diffuse pleural thickening, calcification, and large effusion, r/o TB pleurisy |
| 2 | M | 76 | AdvanSure | Sputum | Pneumonia with TB reactivation | Not performed due to poor condition | CT: multiple small nodules with consolidations, r/o active pulmonary TB |
| 3 | M | 45 | AdvanSure | Sputum | Pulmonary TB | Performed | Biopsy: positive for MTB RT-PCR in lung tissue |
| 4 | M | 74 | Xpert (very low) | Bronchial washing | Non-small cell lung cancer with TB | Not performed due to chemotherapy | CT: pulmonary TB with bronchiectasis |
| 5 | F | 24 | AdvanSure | Neck mass | TB cervical lymphadenopathy | Performed | Biopsy: chronic granulomatous inflammation with caseation necrosis, consistent with TB, in neck tissue |
| 6 | F | 73 | AdvanSure | Sputum | Adenocarcinoma with skull metastasis, r/o Miliary TB | Not performed due to poor condition | CT: patchy opacity and tiny nodular opacities in both lungs, r/o pneumonia and metastasis |
| 7 | F | 88 | AdvanSure | Fine needle aspirate | TB spondylitis | Performed | CT: Subsegmental atelectasis |
| 8 | M | 57 | AdvanSure | Swab | TB epididymitis | Performed | CXR: calcific granulomas in both lungsBiopsy: chronic caseating granulomatous inflammation, consistent with TB in epididymis |
| 9 | M | 46 | Xpert (low) | Bronchial washing | Multi-drug resistant TB | Performed | CXR: cavitary lesion, active pulmonary TB. |
| 10 | M | 37 | Xpert (very low) | Bronchial washing | Pulmonary TB | Performed | CT: peribronchial consolidation and ground-glass opacities (GGO) |
| 11 | M | 27 | AdvanSure | Sputum | TB cervical lymphadenopathy | Performed | CXR: pulmonary TB in lung, activity undetermined Biopsy: positive for MTB RT-PCR in lymph node |
| 12 | F | 74 | AdvanSure | Sputum | TB pleurisy | Performed | CT: patchy GGOs and consolidations |
| TB-LAMP (Eiken) [19,27] | Alere DetermineTM TB LAM Ag (Alere) [19] | BZ TB/NTM NALF Assay | |
|---|---|---|---|
| Test principle | LAMP reaction | Lateral flow technology | Nucleic acid lateral flow (LAMP and lateral flow technology) |
| Readout | Under ultraviolet light with naked eye | Naked eye | Naked eye |
| Turnaround time | ~1 h | ~25 min | ~40 min |
| Sensitivity (95% confidence interval, %) | 80.9% (76.0–85.1%) | Symptomatic participants: 42.0% (31.0–55.0%) Unselected participants: 35.0% (22.0–50.0%) | 98.7% (93.2–99.9%) |
| Specificity (95% confidence interval, %) | 96.5% (94.7–97.7%) | Symptomatic participants: 91.0% (85.0–95.0%) Unselected participants: 95.0% (89.0–98.0%) | 98.7% (91.8–99.8%), |
| Weighted average per-test cost | US$13.78–16.22 | US$3.5 | US$4.0 |
| Recommendation in WHO | Replacement for sputum smear microscopy in adults with signs and symptoms of TB | Assist diagnosis of active TB in HIV-positive adults, adolescents and children: |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.N.; Lee, J.; Yoon, S.-Y.; Jang, W.S.; Lim, C.S. Rapid Detection of Mycobacterium Tuberculosis Using a Novel Point-of-Care BZ TB/NTM NALF Assay: Integrating LAMP and LFIA Technologies. Diagnostics 2023, 13, 1497. https://doi.org/10.3390/diagnostics13081497
Kim HN, Lee J, Yoon S-Y, Jang WS, Lim CS. Rapid Detection of Mycobacterium Tuberculosis Using a Novel Point-of-Care BZ TB/NTM NALF Assay: Integrating LAMP and LFIA Technologies. Diagnostics. 2023; 13(8):1497. https://doi.org/10.3390/diagnostics13081497
Chicago/Turabian StyleKim, Ha Nui, Junmin Lee, Soo-Young Yoon, Woong Sik Jang, and Chae Seung Lim. 2023. "Rapid Detection of Mycobacterium Tuberculosis Using a Novel Point-of-Care BZ TB/NTM NALF Assay: Integrating LAMP and LFIA Technologies" Diagnostics 13, no. 8: 1497. https://doi.org/10.3390/diagnostics13081497