
Effectiveness of Using the FreeStyle Libre® System for Monitoring Blood Glucose during the COVID-19 Pandemic in Diabetic Individuals: Systematic Review
 ,
,  ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Operational Settings
2.3. Search Strategy
2.4. Selection of Studies and Data Extraction
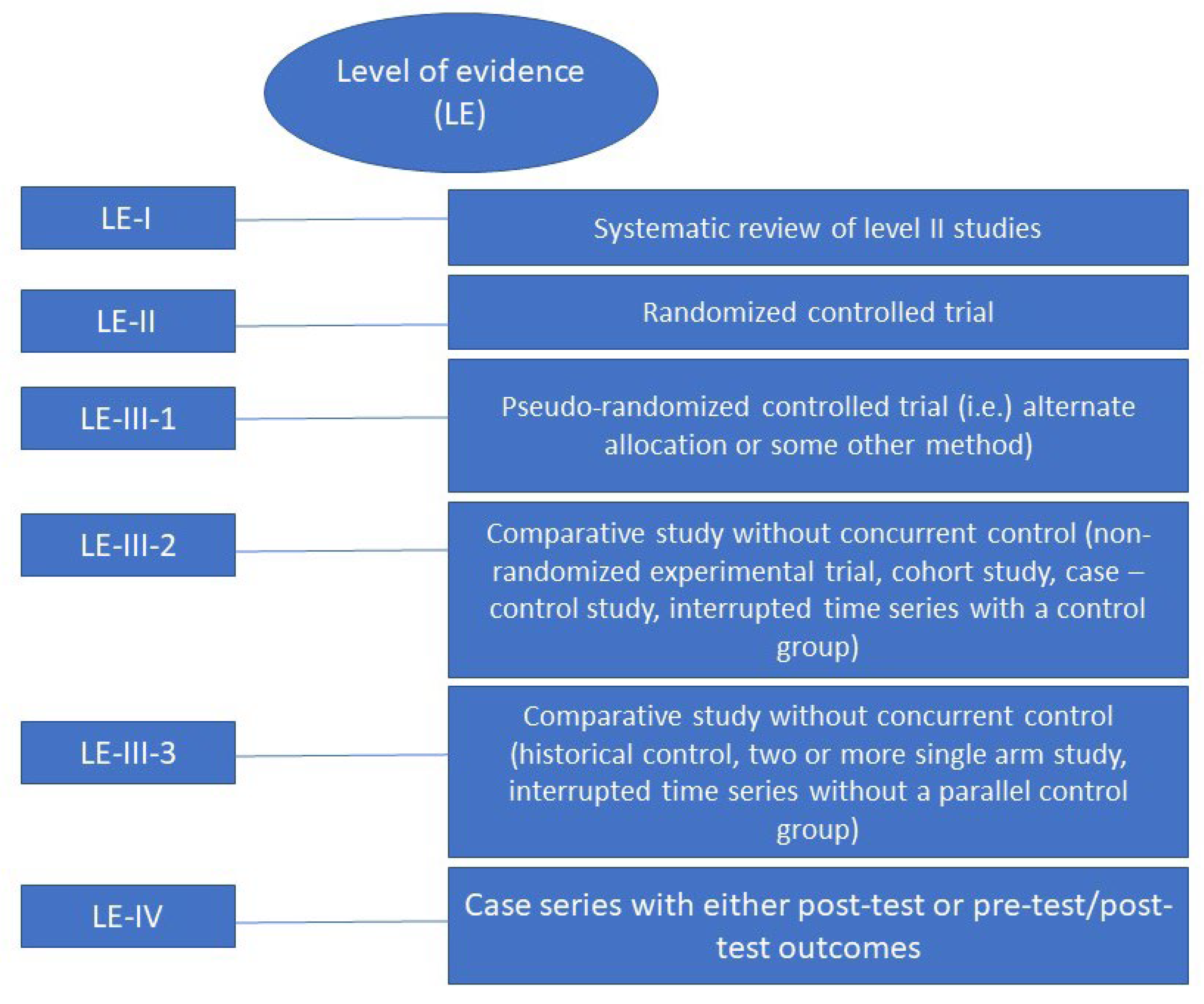
2.5. Level of Evidence
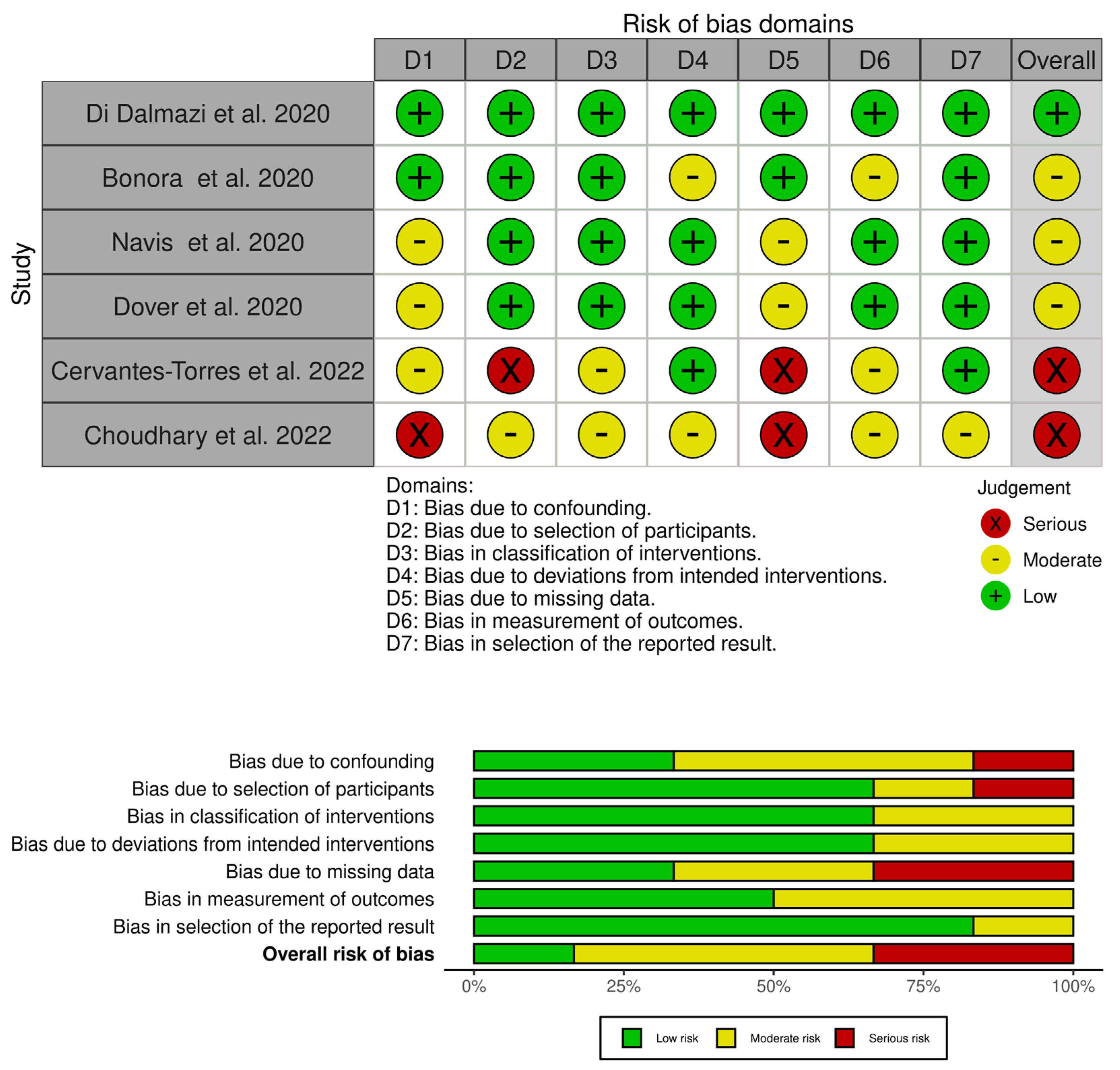
2.6. Methodological Quality of the Studies
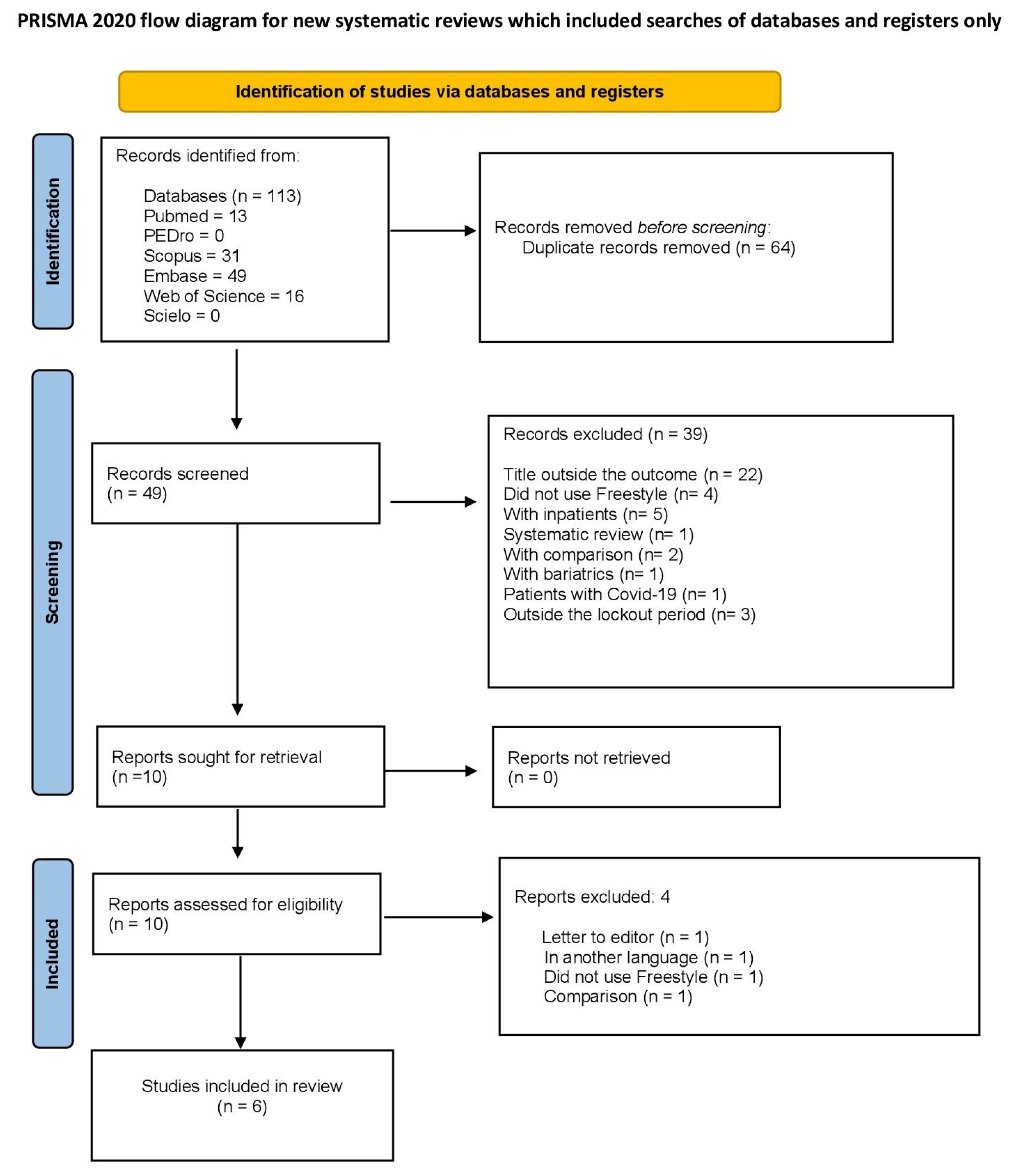
3. Results
4. Discussion
5. Facts and Perspectives
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thimbleby, H. Technology and the future of healthcare. J. Public Health Health Res. 2013, 2, jphr-2013.e28. [Google Scholar] [CrossRef] [PubMed]
- Avila-Tomás, J.F.; Mayer-Pujadas, M.A.; Quesada-Varela, V.J. Artificial intelligence and its applications in medicine I: Introductory background to AI and robotics. Aten. Primaria 2020, 52, 778–784. [Google Scholar] [CrossRef] [PubMed]
- de Freitas Barros, S.R.A.; Cota, A.L.S. Vista do Inteligência Artificial na pandemia da COVID-19. Rev. Thema 2021, 20, 201–214. [Google Scholar] [CrossRef]
- Lim, Y.; Takahashi, H.; Ramadhan, A.A.; Baykara, M. A Novel Approach to Detect COVID-19: Enhanced Deep Learning Models with Convolutional Neural Networks. Appl. Sci. 2022, 12, 9325. [Google Scholar]
- Sonza, A.; de Sá-Caputo, D.D.C.; Sartorio, A.; Tamini, S.; Seixas, A.; Sanudo, B.; Süßenbach, J.; Provenza, M.; Xavier, V.; Taiar, R.; et al. COVID-19 Lockdown and the Behavior Change on Physical Exercise, Pain and Psychological Well-Being: An International Multicentric Study. Int. J. Environ. Res. Public Health 2021, 18, 3810. [Google Scholar] [CrossRef]
- Montenegro, P.; Moral, I.; Puy, A.; Cordero, E.; Chantada, N.; Cuixart, L.; Brontos, C. Prevalence of Post COVID-19 Condition in Primary Care: A Cross Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 1836. [Google Scholar] [CrossRef]
- Fuss, F.K.; Weizman, Y.; Tan, A.M. COVID-19 Pandemic: How Effective Are Preventive Control Measures and Is a Complete Lockdown Justified? A Comparison of Countries and States. COVID 2022, 2, 18–46. [Google Scholar] [CrossRef]
- de Sá-Caputo, D.D.C.; Coelho-Oliveira, A.C.; Sonza, A.; Paineiras-Domingos, L.L.; Taiar, R.; Das, S.; Bello, A.R.; Bernardo-Filho, M. Face masks use to avoid airborne contamination during COVID-19 pandemic and related conditions: A systematic review. Iran J. Public Health. 2021, 50, 2361–2373. [Google Scholar] [CrossRef]
- Dhand, R.; Li, J. Coughs and Sneezes: Their Role in Transmission of Respiratory Viral Infections, Including SARS-CoV-2. Am. J. Respir. Crit. Care Med. 2020, 202, 651–659. [Google Scholar] [CrossRef]
- Yüce, M.; Filiztekin, E.; Özkaya, K.G. COVID-19 diagnosis–A review of current methods. Biosens. Bioelectron. 2021, 172, 112752. [Google Scholar] [CrossRef]
- De Xavier, J.A.D.; Silva, B.L.; Braz, F.L.A.; de Malta, Y.L.S.; Flor, G.B.N.; Alvim, A.L.S. Epidemiologia, Fisiopatologia e Complicações da COVID-19. Uma Revisão Da Lit. 2020. Available online: http://jic-abih.com.br/index.php/jic/article/viewFile/337/pdf (accessed on 22 January 2023).
- Histórico da Pandemia de COVID-19—OPAS/OMS. Organização Pan-Americana da Saúde. Available online: https://www.paho.org/pt/covid19/historico-da-pandemia-covid-19 (accessed on 22 January 2023).
- Marinho, F.P.; de Loyola, I.S.; Monteiro, I.D.O.F.; Castro, T.M.; de Souza Carvalho, M.D.G.; Garcia, J.A.D.; Silvério, A.C.P.; Santos, G.B. Inter-relação entre COVID-19 e diabetes mellitus: Uma revisão sistemática. Soc. Dev. 2021, 10, 1–14. [Google Scholar] [CrossRef]
- Sonza, A.; de Sá-Caputo, D.D.C.; Bachur, J.A.; de Araújo, M.D.G.R.; Trippo, K.V.; da Gama, D.R.N.; Borges, D.L.; Mendonça, V.A.; Bernardo-Filho, M. Brazil before and during COVID-19 pandemic: Impact on the practice and habits of physical exercise. Acta Biomed. 2020, 92, e2021027. [Google Scholar]
- Ting, D.S.W.; Carin, L.; Dzau, V.; Wong, T.Y. Digital technology and COVID-19. Nat. Med. 2020, 26, 459–461. [Google Scholar] [CrossRef] [PubMed]
- Dron, L.; Kalatharan, V.; Gupta, A.; Haggstrom, J.; Zariffa, N.; Morris, A.D.; Arora, P.; Park, J. Data capture and sharing in the COVID-19 pandemic: A cause for concern. Lancet Digit. Health 2022, 4, e748–e756. [Google Scholar] [CrossRef]
- Lam, J.Y.; Shimizu, C.; Tremoulet, A.H.; Bainto, E.; Roberts, S.C.; Sivilay, N.; Gardiner, M.A.; Kanegaye, J.T.; Hogan, A.H.; Salazar, J.C.; et al. A machine-learning algorithm for diagnosis of multisystem inflammatory syndrome in children and Kawasaki disease in the USA: A retrospective model development and validation study. Lancet Digit. Health 2022, 4, e717–e726. [Google Scholar] [CrossRef] [PubMed]
- Taft, J.M.; Weber, C.R.; Gao, B.; Ehling, R.A.; Han, J.; Frei, L.; Metcalfe, S.W.; Overath, M.D.; Yermanos, A.; Kelton, W.; et al. Deep mutational learning predicts ACE2 binding and antibody escape to combinatorial mutations in the SARS-CoV-2 receptor-binding domain. Cell 2022, 185, 4008–4022.e14. [Google Scholar] [CrossRef]
- Elhadd, T.; Mall, R.; Bashir, M.; Palotti, J.; Fernandez-Luque, L.; Farooq, F.; Al Mohanadi, D.; Dabbous, Z.; Malik, R.A.; Abou-Samra, A.B.; et al. Artificial Intelligence (AI) based machine learning models predict glucose variability and hypoglycaemia risk in patients with type 2 diabetes on a multiple drug regimen who fast during ramadan (The PROFAST–IT Ramadan study). Diabetes Res. Clin. Pract. 2020, 169, 108388. [Google Scholar] [CrossRef]
- Bidonde, J.; Fagerlund Charlotte, B.; Fronsdal, K.B.; Lund, U.H.; Robberstard, B. FreeStyle Libre Flash Glucose Self-Monitoring System: A Single-Technology Assessment. 2021. Available online: https://pubmed.ncbi.nlm.nih.gov/29553668/ (accessed on 22 January 2023).
- Alsharif, W.; Qurashi, A. Effectiveness of COVID-19 diagnosis and management tools: A review. Radiography 2021, 27, 682–687. [Google Scholar] [CrossRef]
- Elkin, P.L.; Mullin, S.; Mardekian, J.; Crowner, C.; Sakilay, S.; Sinha, S.; Brady, G.; Wright, M.; Nolen, K.; Trainer, J.; et al. Using Artificial Intelligence with Natural Language Processing to Combine Electronic Health Record’s Structured and Free Text Data to Identify Nonvalvular Atrial Fibrillation to Decrease Strokes and Death: Evaluation and Case-Control Study. J. Med. Internet Res. 2021, 23, e28946. [Google Scholar] [CrossRef]
- Faulds, E.R.; Jones, L.; McNett, M.; Smetana, K.S.; May, C.C.; Sumner, L.; Buschur, E.; Etxline, M.; Ringel, M.D.; Dungaln, K. Facilitators and Barriers to Nursing Implementation of Continuous Glucose Monitoring (CGM) in Critically Ill Patients With COVID-19. Endocr. Pract. 2021, 27, 354–361. [Google Scholar] [CrossRef]
- Tsoukas, M.; Rutkowski, J.; El-Fathi, A.; Yale, J.F.; Bernier-Twardy, S.; Bossy, A.; Pytka, E.; Legault, L.; Haidar, A. Accuracy of FreeStyle Libre in Adults with Type 1 Diabetes: The Effect of Sensor Age. Diabetes Technol. Ther. 2020, 22, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Freckmann, G.; Link, M.; Pleus, S.; Westhoff, A.; Kamecke, U.; Haug, C. Measurement Performance of Two Continuous Tissue Glucose Monitoring Systems Intended for Replacement of Blood Glucose Monitoring. Diabetes Technol. Ther. 2018, 20, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Moraes, H.A.B.D.; Mengue, S.S.; Molina, M.D.C.B.; Cade, N.V. Factors associated with glycemic control in a sample of individuals with Diabetes Mellitus taken from the Longitudinal Study of Adult Health, Brazil, 2008–2010. Epidemiol. E Serviços Saúde 2020, 29, e2018500. [Google Scholar]
- FDA. FDA Approves First Continuous Glucose Monitoring System for Adults Not Requiring Blood Sample Calibration. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-continuous-glucose-monitoring-system-adults-not-requiring-blood-sample (accessed on 22 January 2023).
- Heller, A.; Feldman, B. Electrochemistry in diabetes management. Acc. Chem. Res. 2010, 43, 963–973. [Google Scholar] [CrossRef]
- Blum, A. Freestyle Libre Glucose Monitoring System. Clin. Diabetes 2018, 36, 203–204. [Google Scholar] [CrossRef]
- U. S. Food and Drug Administration. Freestyle Libre Pro Flash Glucose Monitoring System: Summary of Safety and Effectiveness Data (SSED); U.S. Food and Drug Administration: Silver Spring, MD, USA, 2016; pp. 1–34. [Google Scholar]
- Al Hayek, A.A.; Robert, A.A.; Al Dawish, M.A. Effectiveness of the Freestyle Libre Flash Glucose Monitoring System on Diabetes Distress Among Individuals with Type 1 Diabetes: A Prospective Study. Diabetes Ther. 2020, 11, 927–937. [Google Scholar] [CrossRef]
- Al Hayek, A.A.; Robert, A.A.; Al Dawish, M.A. Effectiveness of the freestyle libre 2 flash glucose monitoring system on diabetes-self-management practices and glycemic parameters among patients with type 1 diabetes using insulin pump. Diabetes Metab. Syndr. 2021, 15, 102265. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021, 372, n71. [Google Scholar] [CrossRef]
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Baird, J.; Blazeby, J.M.; Boyd, K.A.; Craig, N.; French, D.P.; McIntosh, E.; et al. A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. BMJ 2021, 374, n2061. [Google Scholar] [CrossRef]
- Thomson, H.; Sterne, J.H.J. ACROBAT-NRSi (A Cochrane Risk of Bias Assessment Tool: For Non-Randomized Studies of Interventions) for Non-Clinical Community Based Studies: A Participatory Workshop Using a Worked Example from Public Health. In Proceedings of the Abstracts of the 23rd Cochrane Colloquium, Vienna, Austria, 3–7 October 2015; Available online: https://abstracts.cochrane.org/2015-vienna/acrobat-nrsi-cochrane-risk-bias-assessment-tool-non-randomized-studies-interventions-non (accessed on 22 January 2023).
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Di Dalmazi, G.; Maltoni, G.; Bongiorno, C.; Tucci, L.; Di Natale, V.; Moscatiello, S.; Laffi, G.; Pession, A.; Zucchini, S.; Pagotto, U. Comparison of the effects of lockdown due to COVID-19 on glucose patterns among children, adolescents, and adults with type 1 diabetes: CGM study. BMJ Open Diabetes Res. Care 2020, 8, e001664. [Google Scholar] [CrossRef] [PubMed]
- Bonora, B.M.; Boscari, F.; Avogaro, A.; Bruttomesso, D.; Fadini, G.P. Glycaemic Control Among People with Type 1 Diabetes During Lockdown for the SARS-CoV-2 Outbreak in Italy. Diabetes Ther. 2020, 11, 1369–1379. [Google Scholar] [CrossRef] [PubMed]
- Prabhu Navis, J.; Leelarathna, L.; Mubita, W.; Urwin, A.; Rutter, M.K.; Schofield, J.; Thabit, H. Impact of COVID-19 lockdown on flash and real-time glucose sensor users with type 1 diabetes in England. Acta Diabetol. 2021, 58, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Dover, A.R.; Ritchie, S.A.; McKnight, J.A.; Strachan, M.W.J.; Zammitt, N.N.; Wake, D.J.; Forbes, S.; Stimson, R.H.; Gibb, F.W. Assessment of the effect of the COVID-19 lockdown on glycaemic control in people with type 1 diabetes using flash glucose monitoring. Diabet. Med. 2021, 38, e14374. [Google Scholar] [CrossRef] [PubMed]
- Cervantes-Torres, L.; Romero-Blanco, C. Longitudinal study of the flash glucose monitoring system in type 1 diabetics: An Health ally in times of COVID-19. J. Clin. Nurs. 2022, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Choudhary, P.; Kao, K.; Dunn, T.C.; Brandner, L.; Rayman, G.; Wilmot, E.G. Glycaemic measures for 8914 adult FreeStyle Libre users during routine care, segmented by age group and observed changes during the COVID-19 pandemic. Diabetes Obes. Metab. 2022, 24, 1976–1982. [Google Scholar] [CrossRef]
- Tuppin, P.; Lesuffleur, T.; Constantinou, P.; Atramont, A.; Coatsaliou, C.; Ferrat, E.; Canouï-Poitrinet, F.; Debeugny, G.; Rachas, A. Underuse of primary healthcare in France during the COVID-19 epidemic in 2020 according to individual characteristics: A national observational study. BMC Prim. Care. 2022, 23, 200. [Google Scholar] [CrossRef]
- Monaghesh, E.; Hajizadeh, A. The role of telehealth during COVID-19 outbreak: A systematic review based on current evidence. BMC Public Health. 2020, 20, 1193. [Google Scholar] [CrossRef]
- Wilms, P.; Schröder, J.; Reer, R.; Scheit, L. The Impact of “Home Office” Work on Physical Activity and Sedentary Behavior during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 12344. [Google Scholar] [CrossRef]
- Pardhan, S.; Islam, M.S.; López-Sánchez, G.F.; Upadhyaya, T.; Sapkota, R.P. Self-isolation negatively impacts self-management of diabetes during the coronavirus (COVID-19) pandemic. Diabetol. Metab. Syndr. 2021, 13, 123. [Google Scholar] [CrossRef]
- Eberle, C.; Stichling, S. Impact of COVID-19 lockdown on glycemic control in patients with type 1 and type 2 diabetes mellitus: A systematic review. Diabetol. Metab. Syndr. 2021, 13, 95. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, L.; Pieralice, S.; Maddaloni, E.; Mignogna, C.; Sterpetti, S.; Coraggio, L.; Luordi, C.; Guarisco, G.; Leto, G.; Leonetti, F.; et al. Effects of the COVID-19 lockdown on glycaemic control in subjects with type 2 diabetes: The glycalock study. Diabetes Obes Metab. 2021, 23, 1624–1630. [Google Scholar] [CrossRef] [PubMed]
- Tinti, D.; Savastio, S.; Grosso, C.; De Donno, V.; Trada, M.; Nugnes, M.; Bertelli, E.; Franceschi, L.; Marchisio, M.; Pozzi, E.; et al. Impact of lockdown during COVID-19 emergency on glucose metrics of children and adolescents with type 1 diabetes in Piedmont, Italy. Acta Diabetol. 2021, 58, 959. [Google Scholar] [CrossRef] [PubMed]
- Tornese, G.; Ceconi, V.; Monasta, L.; Carletti, C.; Faleschini, E.; Barbi, E. Glycemic Control in Type 1 Diabetes Mellitus During COVID-19 Quarantine and the Role of In-Home Physical Activity. Diabetes Technol. Ther. 2020, 22, 462–467. [Google Scholar] [CrossRef]
- Aragona, M.; Barbato, A.; Cavani, A.; Costanzo, G.; Mirisola, C. Negative impacts of COVID-19 lockdown on mental health service access and follow-up adherence for immigrants and individuals in socio-economic difficulties. Public Health 2020, 186, 52–56. [Google Scholar] [CrossRef]
- Ghosal, S.; Sinha, B.; Majumder, M.; Misra, A. Estimation of effects of nationwide lockdown for containing coronavirus infection on worsening of glycosylated haemoglobin and increase in diabetes-related complications: A simulation model using multivariate regression analysis. Diabetes Metab. Syndr. 2020, 14, 319–323. [Google Scholar] [CrossRef]
- Wirtz, B.W.; Weyerer, J.C.; Geyer, C. Artificial Intelligence and the Public Sector—Applications and Challenges. Int. J. Public Adm. 2019, 42, 596–615. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author/Year/Country | Anthropometric Characteristics of the Participants | Location | Period of Data Collection | Objective | Study Design | Level of Evidence |
|---|---|---|---|---|---|---|
| Di Dalmazi et al., 2020/Italy [37] | N = 130 with T1DM Children = 30 Teenagers = 24 Adults = 76 Male = 71 Female = 59 | At home, telephonic contact | 17 February 2020 and 5 April 2020, 20 days before and the 20 days after lockdown | To evaluate CGM metrics in children and adults with T1DM during lockdown and to identify the potentially related factors | Observational (Cohort) | III |
| Bonora et al., 2020/Italy [38] | N = 33 with T1DM Age = 36.9–45.0 years old Male = 12 Female = 21 | DM outpatient clinic of the University Hospital of Padova; data were obtained using the FSL and sharing sensor data with the clinic on a web-based cloud system | At least 3 months | To examine glycemic control during the first week of lockdown against the spread of SARS-CoV-2 in people with T1DM during FGM in Italy in comparison to the pre-lockdown period | Observational (control case) | IV |
| Navis et al., 2020/UK [39] | N = 269 T1DM patients FSL = 190 DG6 = 79 Age = 41.4 ± 12.9 years old Male = 146 Female = 123 | Large teaching hospital in the UK, data were obtained from outpatient electronic records and glucose monitoring web-based platforms on smarthphone device. | Pre-lockdown (1–14 February 2020), early lockdown (1–14 April 2020) and mid-lockdown (1–14 May 2020). | To assess whether sensor-based results before and during lockdown periods were different in a cohort of T1DM glucose sensor users. | Retrospective, observational, single-center cohort. | III |
| Dover et al., 2020/UK [40] | N = 572 T1DM Age = 38–39 years old Male = 301 Female = 271 | Royal Infirmary of Edinburgh and Western General Hospital (Edinburgh) DM clinics; individuals linked their glucose data to these clinics using the LibreView platform. | March and May 2020. | To describe the effect of the lockdown on glycemic control in people with T1DM using flash glucose monitoring | Observational (Cohort). | III |
| Cervantes-Torres and Romero-Blanco, 2022/Spain [41] | N = 206 aged 46.6 ± 15.4 years old Male = 123 Female = 83 | Data of type I diabetic patients were collected from a Spanish health area in the region of Castilla–La Mancha. | The first cut-off point was between February and March 2020 (before the use of FSL), and the second cut-off point was between February and March 2021 (after one year of using FSL). | To assess the effect of FSL device implantation in adult TiDM in the Health Area of Castilla–La Mancha (Spain) during the COVID-19 pandemic | Observational, cross-sectional, pre–post. | III |
| Choudhary et al., 2022/UK [42] | N = 8914 Aged 18 to ≥65 years old | Data were extracted from 8914 de-identified LibreView user accounts for adult users aged 18 years or older. | January to June 2020. | To evaluate the impact of the stay-at-home policy on different glucose metrics for time in range, time below range and time above range for FSL users within four defined age groups and on observed changes during the COVID-19 pandemic. | Observational | III |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaques-Albuquerque, L.T.; dos Anjos-Martins, E.; Torres-Nunes, L.; Valério-Penha, A.G.; Coelho-Oliveira, A.C.; da Silva Sarandy, V.L.; Reis-Silva, A.; Seixas, A.; Bernardo-Filho, M.; Taiar, R.; et al. Effectiveness of Using the FreeStyle Libre® System for Monitoring Blood Glucose during the COVID-19 Pandemic in Diabetic Individuals: Systematic Review. Diagnostics 2023, 13, 1499. https://doi.org/10.3390/diagnostics13081499
Jaques-Albuquerque LT, dos Anjos-Martins E, Torres-Nunes L, Valério-Penha AG, Coelho-Oliveira AC, da Silva Sarandy VL, Reis-Silva A, Seixas A, Bernardo-Filho M, Taiar R, et al. Effectiveness of Using the FreeStyle Libre® System for Monitoring Blood Glucose during the COVID-19 Pandemic in Diabetic Individuals: Systematic Review. Diagnostics. 2023; 13(8):1499. https://doi.org/10.3390/diagnostics13081499
Chicago/Turabian StyleJaques-Albuquerque, Luelia Teles, Elzi dos Anjos-Martins, Luiza Torres-Nunes, Ana Gabriellie Valério-Penha, Ana Carolina Coelho-Oliveira, Viviani Lopes da Silva Sarandy, Aline Reis-Silva, Adérito Seixas, Mario Bernardo-Filho, Redha Taiar, and et al. 2023. "Effectiveness of Using the FreeStyle Libre® System for Monitoring Blood Glucose during the COVID-19 Pandemic in Diabetic Individuals: Systematic Review" Diagnostics 13, no. 8: 1499. https://doi.org/10.3390/diagnostics13081499