
Endocardial Fibroelastosis as an Independent Predictor of Atrioventricular Valve Rupture in Maternal Autoimmune Antibody Exposed Fetus: A Systematic Review with Clinicopathologic Analysis
 ,
,
Abstract
:1. Introduction
2. Case Studies
2.1. Case Description
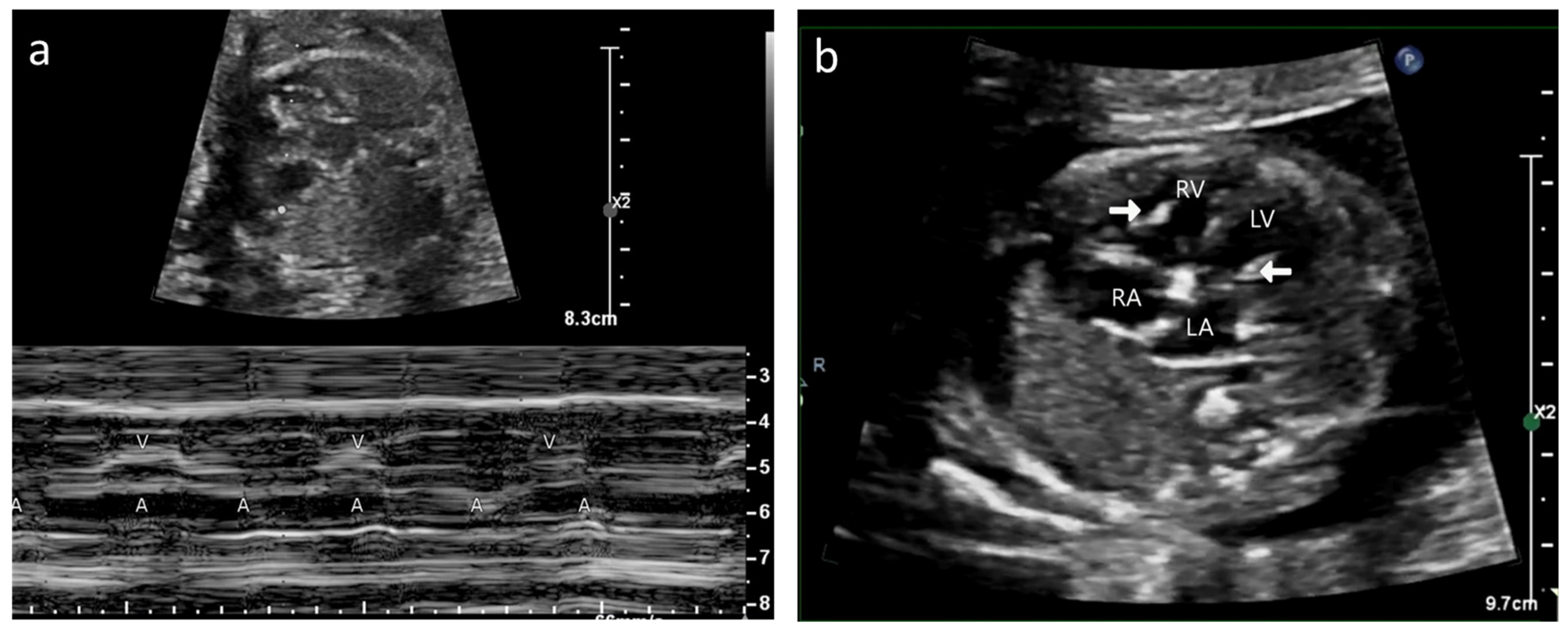
2.1.1. Case A
2.1.2. Case B
2.2. Postmortem Examination
2.2.1. Gross Morphology
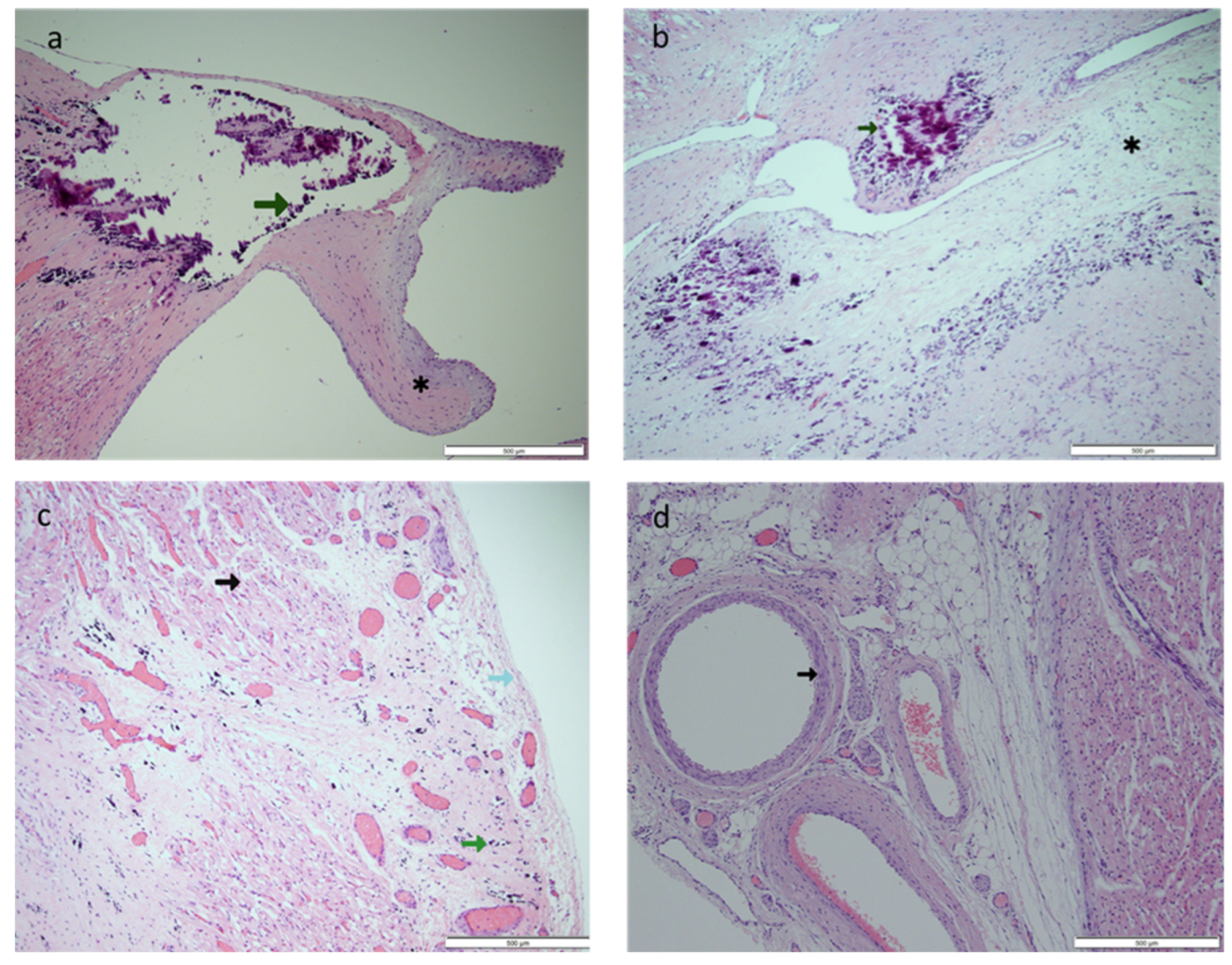
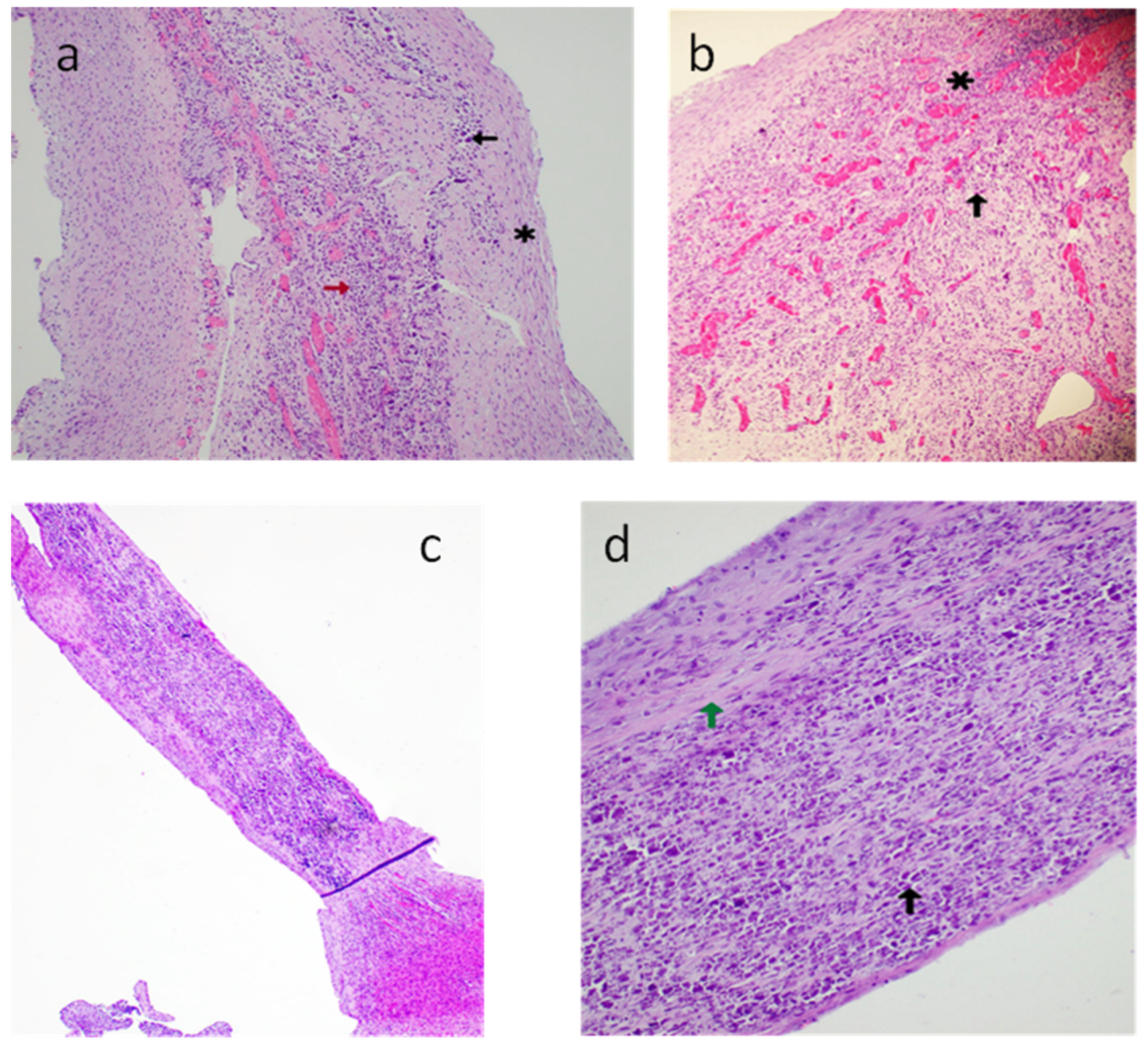
2.2.2. Histopathology
3. Review of the Literature
3.1. Method
3.2. Search Strategy
3.3. Inclusion and Exclusion Criteria
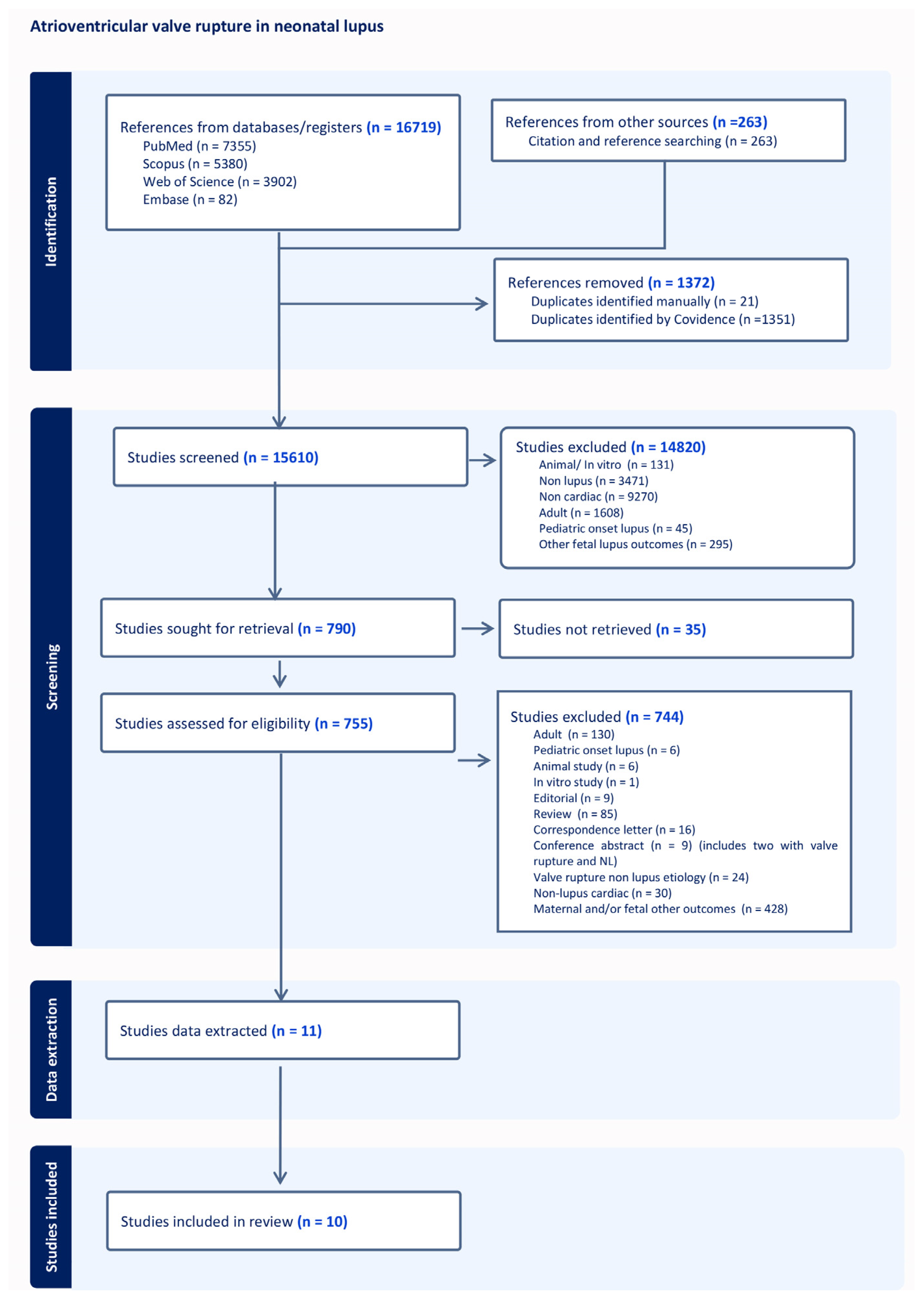
3.4. Study Selection
3.5. Data Extraction
3.6. Quality Assessment
3.7. Data Analysis
4. Results
4.1. Study and Patient Demographics
4.2. Comorbidities and Course
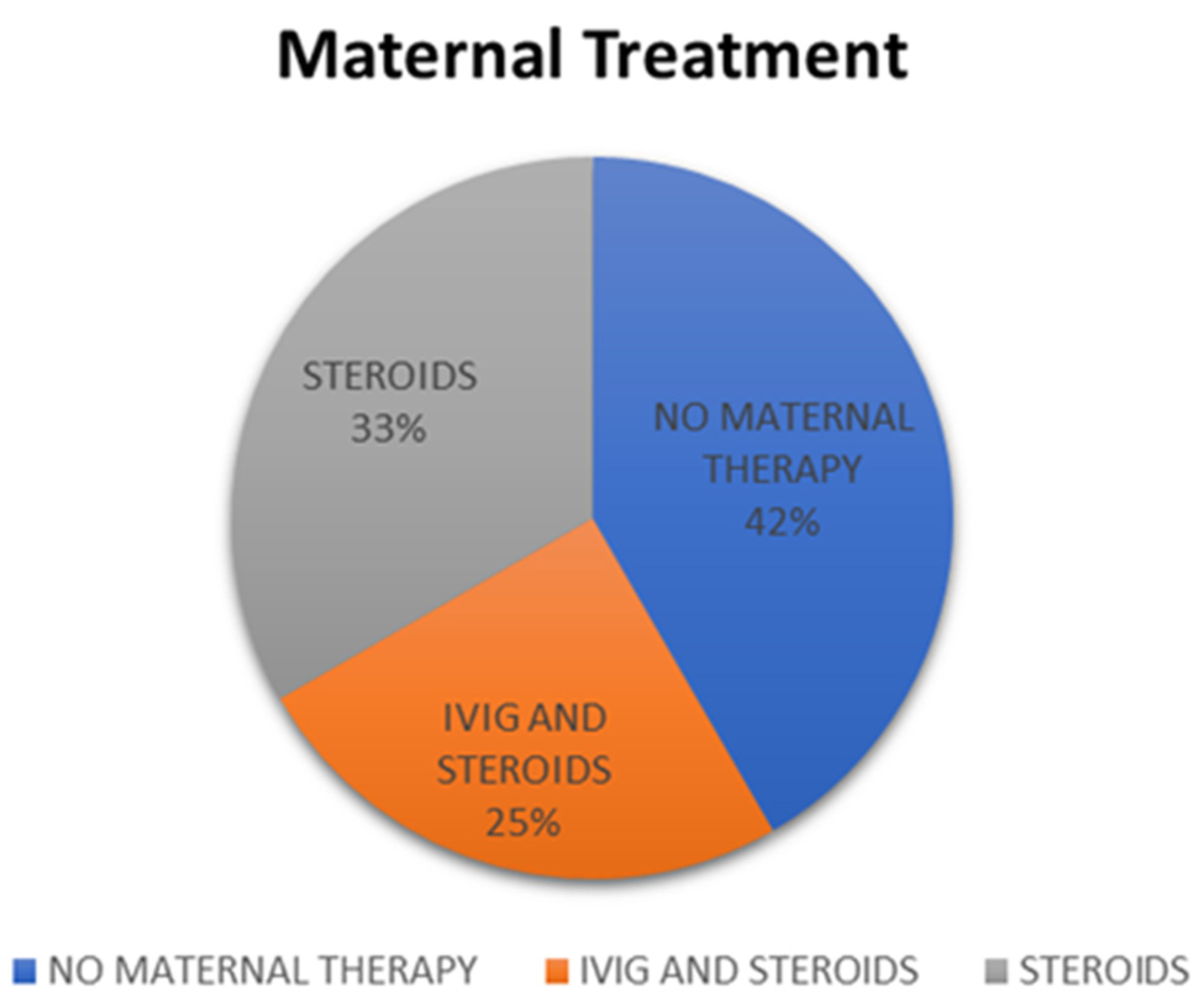
4.3. Maternal Therapy
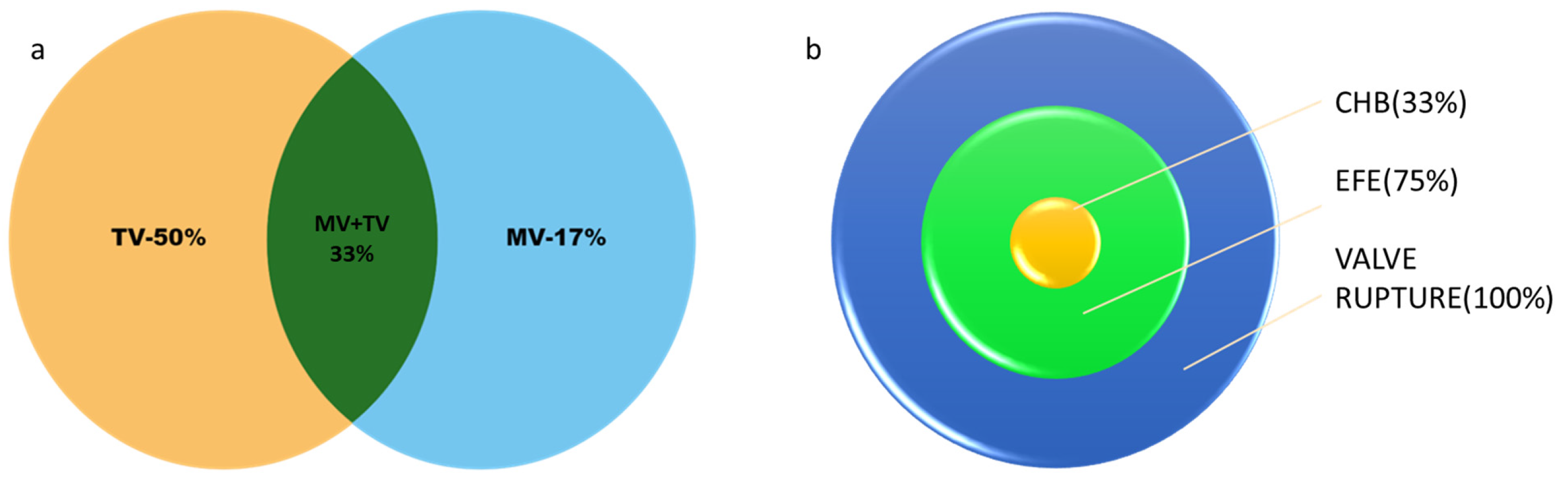
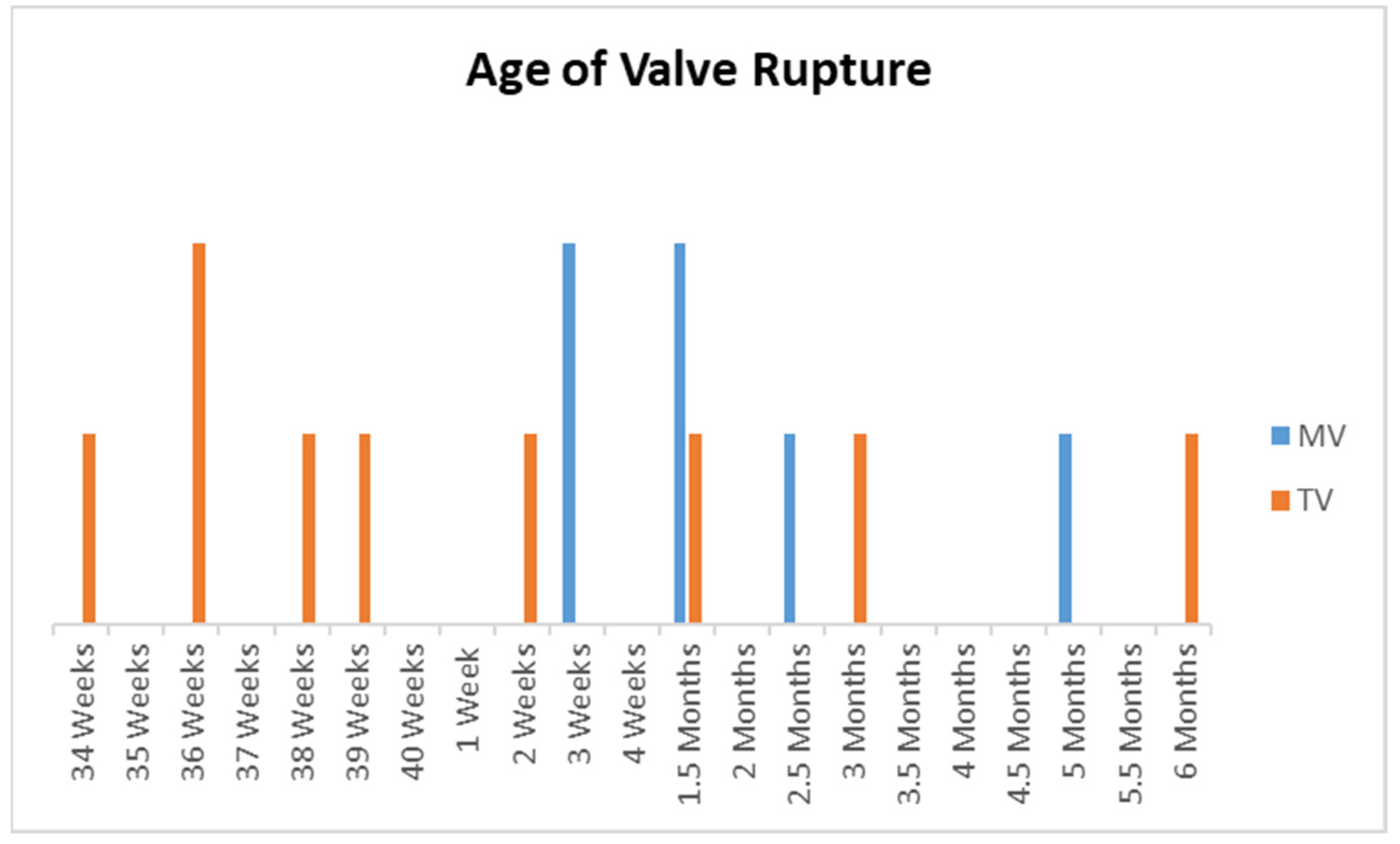
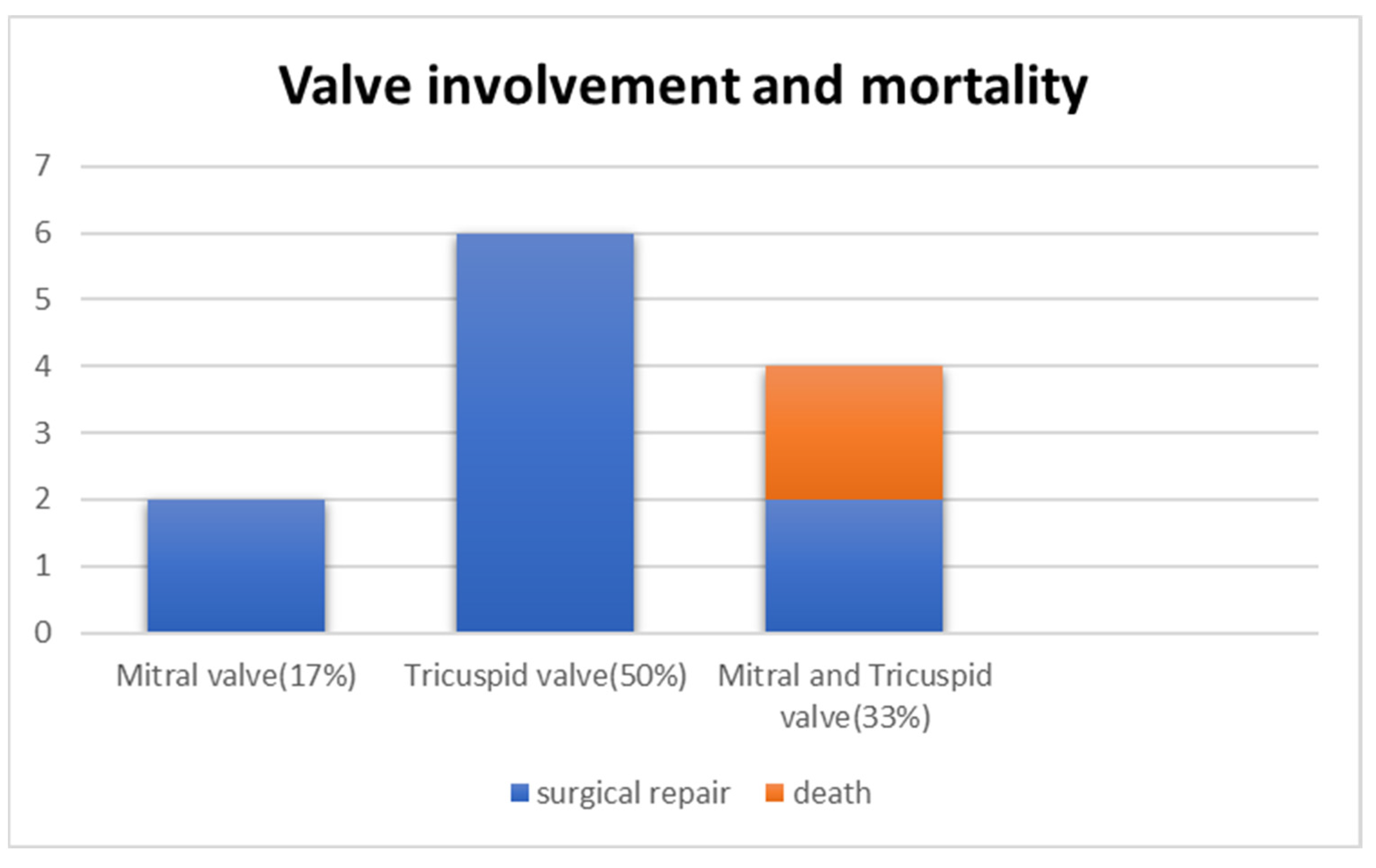
4.4. Age of Valve Rupture and Valves Involved
4.5. Postnatal Management
4.6. Histopathological Findings
5. Discussion
5.1. Causes of Valve Rupture
5.2. Timing of Valve Rupture
5.3. Physiology of Valve Rupture
5.4. Endocardial Fibroelastosis
5.5. Echocardiography Correlation
5.6. Histologic Correlation
5.7. Surgical Repair
5.8. Medical Management and Follow-up
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CHB | Complete heart block |
| EFE | Endocardial fibroelastosis |
| TV | Tricuspid valve |
| TR | Tricuspid valve regurgitation |
| MR | Mitral valve regurgitation |
| MV | Mitral valve |
| AV | Atrioventricular |
| NL | Neonatal lupus |
| RV | Right ventricle |
| LV | Left ventricle |
| RA | Right atrium |
| LA | Left atrium |
| IVIG | Intravenous immunoglobulin |
| bpm | Beats per minute |
References
- Brito-Zerón, P.; Izmirly, P.M.; Ramos-Casals, M.; Buyon, J.P.; Khamashta, M.A. The clinical spectrum of autoimmune congenital heart block. Nat. Rev. Rheumatol. 2015, 11, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Reyes, J.A.; Dipchand, A.I.; Chiasson, D.A. Paediatric dilated cardiomyopathy with and without endocardial fibroelastosis—A pathological analysis of 89 explants. Cardiol. Young 2021, 32, 1041–1047. [Google Scholar] [CrossRef] [PubMed]
- Izmirly, P.M.; Saxena, A.; Kim, M.Y.; Wang, D.; Sahl, S.K.; Llanos, C.; Friedman, D.; Buyon, J.P. Maternal and fetal factors associated with mortality and morbidity in a multi-racial/ethnic registry of anti-SSA/Ro-associated cardiac neonatal lupus. Circulation 2011, 124, 1927–1935. [Google Scholar] [CrossRef] [PubMed]
- Nield, L.E.; Silverman, E.D.; Taylor, G.P.; Smallhorn, J.F.; Mullen, J.B.M.; Silverman, N.H.; Finley, J.P.; Law, Y.M.; Human, D.G.; Seaward, P.G.; et al. Maternal anti-Ro and anti-La antibody—Associated endocardial fibroelastosis. Circulation 2002, 105, 843–848. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K. JBI Critical appraisal checklist for case reports. Joanna Briggs Inst. Rev. Man. Joanna Briggs Inst. 2017, 1–7. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Mawad, W.; Hornberger, L.; Cuneo, B.; Raboisson, M.J.; Moon-Grady, A.J.; Lougheed, J.; Diab, K.; Parkman, J.; Silverman, E.; Jaeggi, E. Outcome of Antibody-Mediated Fetal Heart Disease With Standardized AntiInflammatory Transplacental Treatment. J. Am. Heart Assoc. 2022, 11, e023000. [Google Scholar] [CrossRef]
- Carretero Bellon, J.M.; Brunet-Garcia, L.; Sanchez de Toledo, J.; Congiu, S. Neonatal Rupture of the Tricuspid Valve and Maternal Lupus: Is There a Correlation? World J. Pediatr. Congenit. Heart Surg. 2022, 13, 260–263. [Google Scholar] [CrossRef]
- Cuneo, B.F.; Fruitman, D.; Benson, D.W.; Ngan, B.Y.; Liske, M.R.; Wahren-Herlineus, M.; Ho, S.Y.; Jaeggi, E. Spontaneous rupture of atrioventricular valve tensor apparatus as late manifestation of anti-Ro/SSA antibody-mediated cardiac disease. Am. J. Cardiol. 2011, 107, 761–766. [Google Scholar] [CrossRef]
- Cuneo, B.F.; Strasburger, J.F.; Niksch, A.; Ovadia, M.; Wakai, R.T. An expanded phenotype of maternal SSASSB antibody-associated fetal cardiac disease. J. Matern. Fetal Neonatal Med. 2009, 22, 233–238. [Google Scholar] [CrossRef]
- Fleming, G.A.; Scholl, F.G.; Kavanaugh-McHugh, A.; Liske, M.R. A case of an infant with flail tricuspid valve due to spontaneous papillary muscle rupture: Was neonatal lupus the culprit? Pediatr. Cardiol. 2008, 29, 442–445. [Google Scholar] [CrossRef] [PubMed]
- González-López, M.T.; Pérez-Caballero-Martínez, R.; Gil-Jaurena, J.M. Myocarditis, flail tricuspid valve, and normal rhythm: An exceptional form of neonatal cardiac lupus. Cardiol. Young 2017, 27, 1419–1422. [Google Scholar] [CrossRef] [PubMed]
- Hamaoka, A.; Shiraishi, I.; Yamagishi, M.; Hamaoka, K. A neonate with the rupture of mitral chordae tendinae associated with maternal-derived anti-SSA antibody. Eur. J. Pediatr. 2009, 168, 741–743. [Google Scholar] [CrossRef] [PubMed]
- Brooks, P. Fetal manifestations of maternal anti-Ro and La antibodies—More than complete heart block. Australas. J. Ultrasound Med. 2015, 18, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Shiraishi, I.; Nishimura, K.; Sakaguchi, H.; Abe, T.; Kitano, M.; Kurosaki, K.; Kato, H.; Nakanishi, T.; Yamagishi, H.; Sagawa, K.; et al. Acute rupture of chordae tendineae of the mitral valve in infants a nationwide survey in Japan exploring a new syndrome. Circulation 2014, 130, 1053–1061. [Google Scholar] [CrossRef]
- Tarca, A.J.; Eckersley, L.; Kothari, D. Flail anterior tricuspid valve leaflet in a neonate: Association with maternal antiphospholipid syndrome. Cardiol. Young 2017, 27, 1637–1640. [Google Scholar] [CrossRef] [PubMed]
- Weber, H.S.; Myers, J.L. Maternal collagen vascular disease associated with fetal heart block and degenerative changes of the atrioventricular valves. Pediatr. Cardiol. 1994, 15, 204–206. [Google Scholar] [CrossRef]
- Anagnostopoulos, P.V.; Alphonso, N.; Nölke, L.; Hornberger, L.K.; Raff, G.W.; Azakie, A.; Karl, T.R. Neonatal Mitral and Tricuspid Valve Repair for In Utero Papillary Muscle Rupture. Ann. Thorac. Surg. 2007, 83, 1458–1462. [Google Scholar] [CrossRef]
- Loftus, P.D.; Arrington, C.B.; Kaza, A.K. Neonatal flail tricuspid valve: Diagnosis and management. Ann. Thorac. Surg. 2014, 98, 1098–1101. [Google Scholar] [CrossRef]
- Torigoe, T.; Sakaguchi, H.; Kitano, M.; Kurosaki, K.I.; Shiraishi, I.; Kagizaki, K.; Ichikawa, H.; Yagihara, T. Clinical characteristics of acute mitral regurgitation due to ruptured chordae tendineae in infancy-experience at a single institution. Eur. J. Pediatr. 2012, 171, 259–265. [Google Scholar] [CrossRef]
- Hussain, K.; Gauto-Mariotti, E.; Cattoni, H.M.; Arif, A.W.; Richardson, C.; Manadan, A.; Yadav, N. A Meta-analysis and Systematic Review of Valvular Heart Disease in Systemic Lupus Erythematosus and Its Association with Antiphospholipid Antibodies. JCR J. Clin. Rheumatol. 2020, 27, e525–e532. [Google Scholar] [CrossRef] [PubMed]
- Nield, L.E.; Silverman, E.D.; Smallhorn, J.F.; Taylor, G.P.; Mullen, J.B.; Benson, L.N.; Hornberger, L.K. Endocardial fibroelastosis associated with maternal anti-Ro and anti-La antibodies in the absence of atrioventricular block. J. Am. Coll. Cardiol. 2002, 40, 796–802. [Google Scholar] [CrossRef] [PubMed]
- Saxena, A.; Izmirly, P.M.; Bomar, R.P.; Golpanian, R.S.; Friedman, D.M.; Eisenberg, R.; Kim, M.Y.; Buyon, J.P. Factors associated with long-term cardiac dysfunction in neonatal lupus. Ann. Rheum. Dis. 2019, 79, 217. [Google Scholar] [CrossRef] [PubMed]
- Qu, Y.; Boutjdir, M. Pathophysiology of autoimmune-associated congenital heart block. Appl. Cardiopulm. Pathophysiol. 2012, 16, 96–112. [Google Scholar]
- Jaeggi, E.T.; Hamilton, R.M.; Silverman, E.D.; Zamora, S.A.; Hornberger, L.K. Outcome of children with fetal, neonatal or childhood diagnosis of isolated congenital atrioventricular block: A single institution’s experience of 30 years. J. Am. Coll. Cardiol. 2002, 39, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Guettrot-Imbert, G.; Cohen, L.; Fermont, L.; Villain, E.; Francès, C.; Thiebaugeorges, O.; Foliguet, B.; Leroux, G.; Cacoub, P.; Amoura, Z.; et al. A new presentation of neonatal lupus: 5 Cases of isolated mild endocardial fibroelastosis associated with maternal anti-SSA/Ro and anti-SSB/La antibodies. J. Rheumatol. 2011, 38, 378–386. [Google Scholar] [CrossRef]
- Llanos, C.; Friedman, D.M.; Saxena, A.; Izmirly, P.M.; Tseng, C.E.; Dische, R.; Abellar, R.G.; Halushka, M.; Clancy, R.M.; Buyon, J.P. Anatomical and pathological findings in hearts from fetuses and infants with cardiac manifestations of neonatal lupus. Rheumatology 2012, 51, 1086–1092. [Google Scholar] [CrossRef]
- Li, J. The Role of Autoantibodies in Arrhythmogenesis. Curr. Cardiol. Rep. 2020, 23, 3. [Google Scholar] [CrossRef]
- Popescu, M.R.; Dudu, A.; Jurcut, C.; Ciobanu, A.M.; Zagrean, A.M.; Panaitescu, A.M. A Broader Perspective on Anti-Ro Antibodies and Their Fetal Consequences—A Case Report and Literature Review. Diagnostics 2020, 10, 478. [Google Scholar] [CrossRef]
- Suryawanshi, H.; Clancy, R.; Morozov, P.; Halushka, M.K.; Buyon, J.P.; Tuschl, T. Cell atlas of the foetal human heart and implications for autoimmune-mediated congenital heart block. Cardiovasc. Res. 2020, 116, 1446–1457. [Google Scholar] [CrossRef]
- Hedlund, M.; Thorlacius, G.E.; Ivanchenko, M.; Ottosson, V.; Kyriakidis, N.; Lagnefeldt, L.; Tingström, J.; Sirsjö, A.; Bengtsson, A.A.; Aronsson, E.; et al. Type i IFN system activation in newborns exposed to Ro/SSA and La/SSB autoantibodies in utero. RMD Open 2020, 6, 989. [Google Scholar] [CrossRef] [PubMed]
- Izmirly, P.; Kim, M.; Friedman, D.M.; Costedoat-Chalumeau, N.; Clancy, R.; Copel, J.A.; Phoon, C.K.L.; Cuneo, B.F.; Cohen, R.E.; Robins, K.; et al. Hydroxychloroquine to Prevent Recurrent Congenital Heart Block in Fetuses of Anti-SSA/Ro-Positive Mothers. J. Am. Coll. Cardiol. 2020, 76, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Zuppa, A.A.; Riccardi, R.; Frezza, S.; Gallini, F.; Luciano, R.M.; Alighieri, G.; Romagnoli, C.; De Carolis, S. Neonatal lupus: Follow-up in infants with anti-SSA/Ro antibodies and review of the literature. Autoimmun. Rev. 2017, 16, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid. Based Med. 2018, 23, 60. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Reference Year of Publication | Maternal Age (Years) | Gravida | Prior Affected Pregnancy | Known Case of Auto Immune Disease | Anti-Ro/Anti La |
|---|---|---|---|---|---|---|
| 1 | Case A | 35 | 2 | No | No | +/+ |
| 2 | Cuneo et al. 2011 [9] | 25 | 2 | No | Yes | +/− |
| 3 | Cuneo et al. 2009 [10] | 2 | Yes | Sjogren’s disease | +/− | |
| 4 | Weber et al. 1994 [17] | 31 | 2 | Yes | Sjogren’s disease | +/− |
| 5 | Shiraishi et al. 2014 [15] | - | - | |||
| 6 | Hamaoka et al. 2009 [13] | - | - | +/+ | ||
| 7 | Bellon et al. 2022 [8] | 26 | 1 | - | No | +/− |
| 8 | Tarca et al. 2017 [16] | 31 | 2 | 1 | Antiphospholipid syndrome | +/+ |
| 9 | Gonzalez-Lopez et al. 2017 [12] | 2 | - | No | +/+ | |
| 10 | Brooks et al. 2015 [14] | 1 | No | +/+ | ||
| 11 | Fleming et al. 2008 [11] | No | +/− | |||
| 12 | Cuneo et al. 2011 [9] | 27 | 2 | 0 | Yes | +/− |
| Case | GA (Weeks) for Detection | Valve Involved | Maternal Therapy | Timing of Valve Rupture | GA (Weeks) Delivered | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| EFE | CHB | Effusions | Medication | Initiation | Effect | Antenatal | Perinatal | Postnatal | |||
| 1 | 21 | 21 | 21–29 | MV+TV | D+T | 24 | Pleural effusions resolved, reduction in pericardial effusion to mild | - | - | TV and MV—45 days | 32 + 4 |
| 2 | 19 | - | 19 | MV+TV | D+IVIG | 34 | No change | TV—34–36 weeks | - | MV—23 days | 36 |
| 3 | 19 | - | - | MV+TV | D+IVIG | 17 | Improvement in patchy echogenicity | - | - | TV and MV—7 weeks | 35 |
| 4 | 24 | 24 | - | MV+TV | P+T | 22 | Increased echogenicity along the AV valves without insufficiency, no hydrops fetalis | - | - | TV = 2 weeks MV—2.5 months | 35 |
| 5 | - | MV | - | - | - | - | - | 5 months | |||
| 6 | - | - | MV | - | - | - | - | - | 21 days | 40 | |
| 7 | 20 | - | 39 | TV | - | - | - | 39 weeks | - | - | 39 |
| 8 | 19 | - | - | TV | - | - | - | - | Immediately after delivery | - | 38 + 6 |
| 9 | 21 | 20 | - | TV | D | 21 | Worsening of TR, moderate RV dysfunction | - | Immediately after delivery | - | 34 |
| 10 | - | - | 36 | TV | - | - | - | 36 weeks | - | - | 36 |
| 11 | 20 | 20 | - | TV | D+T | 20 | - | - | 3 months | 34 | |
| 12 | 21 | 21 | - | TV | D+IVIG | 23 | No change | - | - | 6 months | 38 |
| Case | Postnatal Therapy | Age of Rupture | Age of Surgery | Surgery | Outcome |
|---|---|---|---|---|---|
| 1 | - | 45 days | - | Not performed | Died at 55 days of life |
| 2 | - | TV—34–36 weeks MV—23 days | - | Not performed | Died at 32 days |
| 3 | Tapering prednisolone over 4 weeks | 7 weeks | 7 weeks | Repair of mitral and TV chordae with gortex and autologous pericardium | 6 months old—diuretics, ACE inhibitors, first degree AV block, and incomplete RBBB |
| 4 | - | 2 weeks—TV after placing endocardial lead, MV—2.5 months | 2 weeks VVI, 24 h later TV repair and epicardial pacemaker; 2.5 months—MV replacement | 1. Anastomosis of the TV chordae to the papillary muscle and atrial septum was closed 2. MV replacement | Doing well |
| 5 | - | 5 months | - | - | |
| 6 | - | 21 days | 21 days | Annuloplasty and anastomosis of chordae with autologous pericardium | 2 year—1st degree heat block |
| 7 | - | Antenatal | Neonate | Direct attachment of the chordae to neo-papillary muscle and TV annuloplasty | Well at 8 years |
| 8 | - | Delivery | 11 months | Neochordae with gortex attached to septum and annuloplasty | Well at 15 months |
| 9 | Hydrocortisone, IVIG, captopril, sildenafil | Delivery | 2 months | Polytetrafluoroethylene neochordae, No annuloplasty | 20 months |
| 10 | - | 36 weeks | 6 days | TV repair | Normal at 2 years |
| 11 | - | 3 months | Permanent pacemaker: 3 days, BPV: 3 months, TV repair at 3 months | Repair of anterior tricuspid leaflet with PTFE cords, closure of ASD, dilatation of pulmonary valve | Well |
| 12 | Prednisolone for 2 months, IVIG 2 g/kg | 6 months | 6 months | Repair with Gore-Tex chordae | Well at 3 years |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotecha, M.K.; Merchant, K.; Chan, C.J.; Choo, J.T.L.; Gopagondanahalli, K.R.; Zhang, D.Z.; Tan, T.H.; Sundararaghavan, S. Endocardial Fibroelastosis as an Independent Predictor of Atrioventricular Valve Rupture in Maternal Autoimmune Antibody Exposed Fetus: A Systematic Review with Clinicopathologic Analysis. Diagnostics 2023, 13, 1481. https://doi.org/10.3390/diagnostics13081481
Kotecha MK, Merchant K, Chan CJ, Choo JTL, Gopagondanahalli KR, Zhang DZ, Tan TH, Sundararaghavan S. Endocardial Fibroelastosis as an Independent Predictor of Atrioventricular Valve Rupture in Maternal Autoimmune Antibody Exposed Fetus: A Systematic Review with Clinicopathologic Analysis. Diagnostics. 2023; 13(8):1481. https://doi.org/10.3390/diagnostics13081481
Chicago/Turabian StyleKotecha, Monika Kantilal, Khurshid Merchant, Charmaine Jiahui Chan, Jonathan Tze Liang Choo, Krishna Revanna Gopagondanahalli, Dyan Zhewei Zhang, Teng Hong Tan, and Sreekanthan Sundararaghavan. 2023. "Endocardial Fibroelastosis as an Independent Predictor of Atrioventricular Valve Rupture in Maternal Autoimmune Antibody Exposed Fetus: A Systematic Review with Clinicopathologic Analysis" Diagnostics 13, no. 8: 1481. https://doi.org/10.3390/diagnostics13081481