
Nevus Sebaceous of Jadassohn in Adults—Can Reflectance Confocal Microscopy Detect Malignant Transformation?
 ,
, 
{kind=link}
{kind=link}
Abstract
:1. Introduction
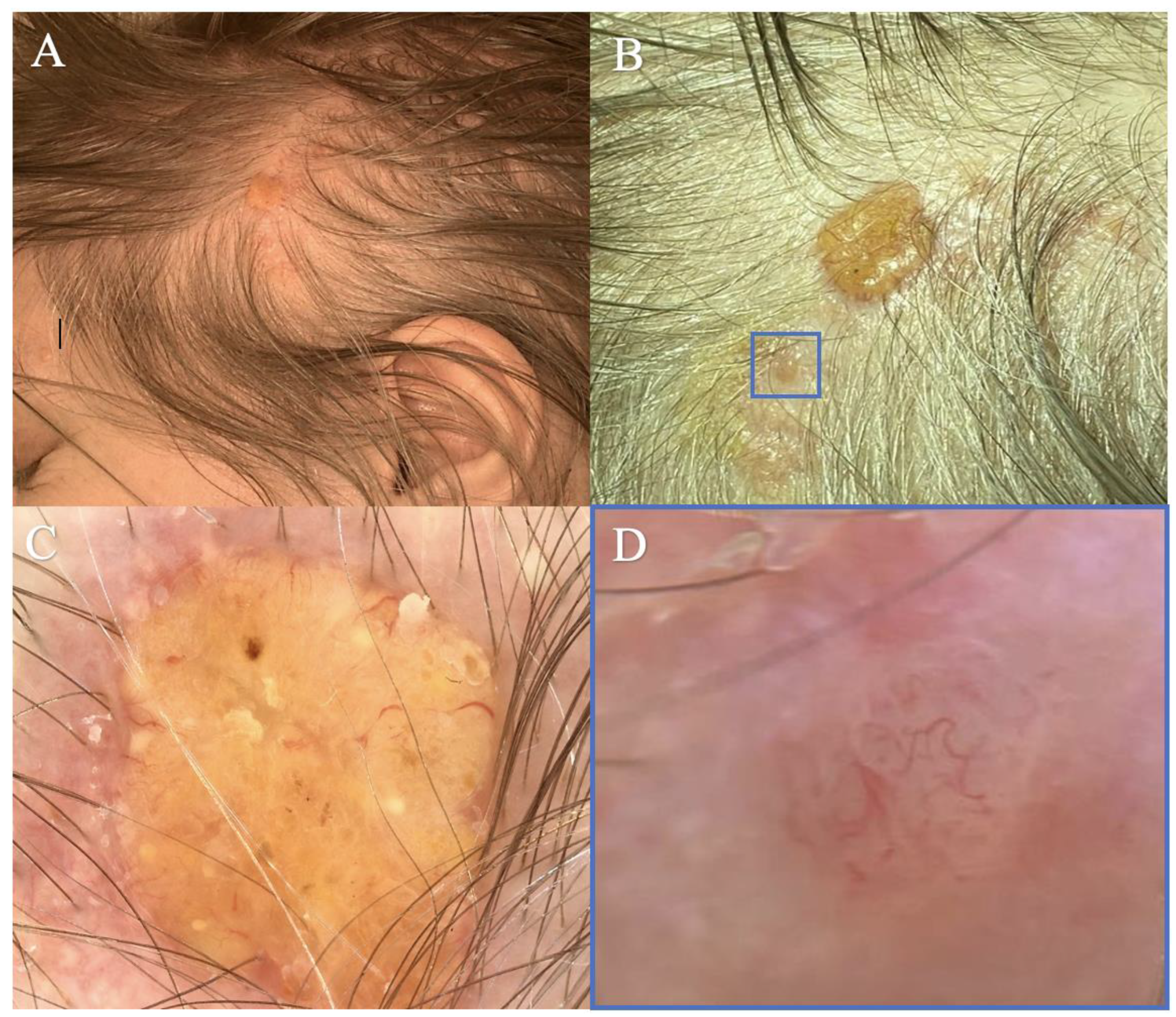
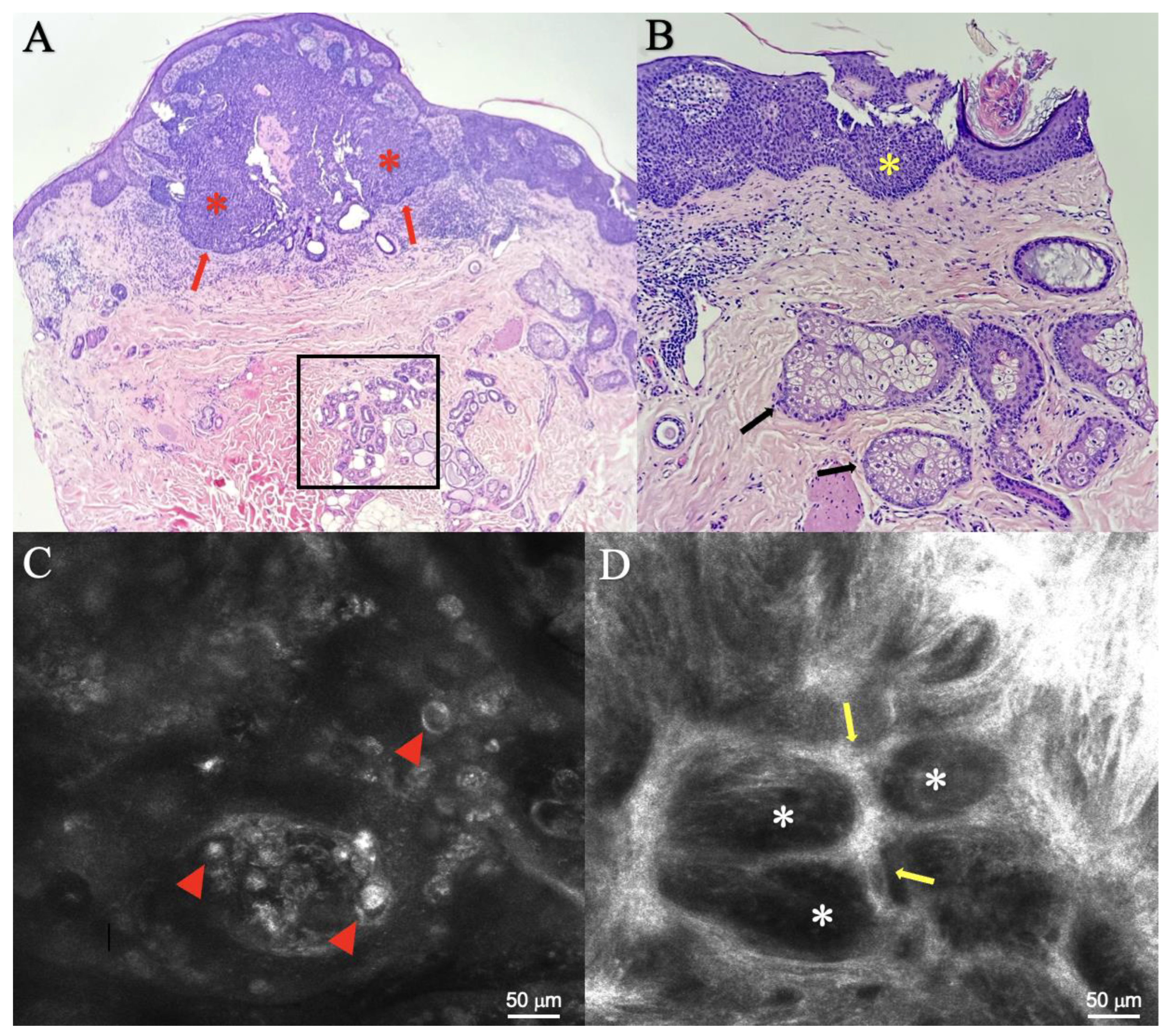
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Terenzi, V.; Indrizzi, E.; Buonaccorsi, S.; Leonardi, A.; Pellacchia, V.; Fini, G. Nevus sebaceus of Jadassohn. J. Craniofacial Surg. 2006, 17, 1234–1239. [Google Scholar] [CrossRef] [PubMed]
- Solomon, L.M.; Esterly, N.B. Epidermal and other congenital organoid nevi. Curr. Probl. Pediatr. 1975, 6, 1–56. [Google Scholar] [CrossRef] [PubMed]
- Serpas de Lopez, R.M.E.; Hernandez-Perez, E. Jadassohn’s sebaceous nevus. J. Dermatol. Surg. Oncol. 1985, 11, 68–72. [Google Scholar] [CrossRef]
- Idriss, M.H.; Elston, D.M. Secondary neoplasms associated with nevus sebaceus of Jadassohn: A study of 707 cases. J. Am. Acad. Dermatol. 2014, 70, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Cribier, B.; Scrivener, Y.; Grosshans, E. Tumors arising in nevus sebaceus: A study of 596 cases. J. Am. Acad. Dermatol. 2000, 42 Pt 1, 263–268. [Google Scholar] [CrossRef]
- Neto, M.P.S.; Assis, B.R.; Andrade, G.R. Sebaceous nevus of Jadassohn: Review and clinical-surgical approach. An. Bras. Dermatol. 2022, 97, 628–636. [Google Scholar] [CrossRef]
- Hsu, M.C.; Liau, J.Y.; Hong, J.L.; Cheng, Y.; Liao, Y.H.; Chen, J.S.; Sheen, Y.; Hong, J. Secondary neoplasms arising from nevus sebaceus: A retrospective study of 450 cases in Taiwan. J. Dermatol. 2016, 43, 175–180. [Google Scholar] [CrossRef]
- Patel, P.; Nawrocki, S.; Hinther, K.; Khachemoune, A. Trichoblastomas Mimicking Basal Cell Carcinoma: The Importance of Identification and Differentiation. Cureus 2020, 12, e8272. [Google Scholar] [CrossRef]
- Sangma, M.M.; Dasiah, S.D.; Bhat, V.R. Syringocystadenoma papilliferum of the scalp in an adult male—A case report. J. Clin. Diagn. Res. 2013, 7, 742–743. [Google Scholar] [CrossRef]
- Hasan, A.; Kandil, A.M.; Al-Ghamdi, H.S.; Alghamdi, M.A.; Nasr, M.; Naeem, S.A.; Abd-Elhay, W.M.; Mohamed, O.K.E.; Ibrahim, H.S.A.; Ahmed, E.M.; et al. Sun-Exposed versus Sun-Protected Cutaneous Basal Cell Carcinoma: Clinico-Pathological Profile and p16 Immunostaining. Diagnostics 2023, 13, 1271. [Google Scholar] [CrossRef]
- Al Mushcab, N.; Husain, R.; Al Subaiei, M.; Al Qarni, A.; Abbas, A.; Al Duhileb, M. Trichoblastoma mimicking basal cell carcinoma and the approach to its management: Case report. Int. J. Surg. Case Rep. 2021, 86, 106318. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, C.; Persechino, F.; Ardigò, M. In Vivo Reflectance Confocal Microscopy in General Dermatology: How to Choose the Right Indication. Dermatol. Pract. Concept. 2020, 10, e2020032. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.; Dohil, M.A.; Eichenfield, L.F.; Cunningham, B.B. SCALP syndrome: Sebaceous nevus syndrome, CNS malformations, aplasia cutis congenita, limbal dermoid, and pigmented nevus (giant congenital melanocytic nevus) with neurocutaneous melanosis: A distinct syndromic entity. J. Am. Acad. Dermatol. 2008, 58, 884–888. [Google Scholar] [CrossRef] [PubMed]
- Mehregan, A.H.; Pinkus, H. Life History of Organoid Nevi: Special Reference to Nevus Sebaceus of Jadassohn. Arch. Dermatol. 1965, 91, 574–588. [Google Scholar] [CrossRef]
- Paninson, B.; Trope, B.M.; Moschini, J.C.; Jeunon-Sousa, M.A.; Ramos-E-Silva, M. Basal Cell Carcinoma on a Nevus Sebaceous of Jadassohn: A Case Report. J. Clin. Aesthet. Dermatol. 2019, 12, 40–43. [Google Scholar]
- Patel, P.; Malik, K.; Khachemoune, A. Sebaceus and Becker’s Nevus: Overview of Their Presentation, Pathogenesis, Associations, and Treatment. Am. J. Clin. Dermatol. 2015, 16, 197–204. [Google Scholar] [CrossRef]
- Xin, H.; Matt, D.; Qin, J.Z.; Burg, G.; Böni, R. The sebaceous nevus: A nevus with deletions of the PTCH gene. Cancer Res. 1999, 59, 1834–1836. [Google Scholar]
- Ghigliotti, G.; De Col, E.; Parodi, A.; Bombonato, C.; Argenziano, G. Trichoblastoma: Is a clinical or dermoscopic diagnosis possible? J. Eur. Acad. Dermatol. Venereol. 2016, 30, 1978–1980. [Google Scholar] [CrossRef]
- Pampena, R.; Peccerillo, F.; Marghoob, N.G.; Piana, S.; Longo, C. Peritumoral clefting as a key feature in differentiating basal cell carcinoma from trichoblastoma through in-vivo reflectance confocal microscopy. J. Eur. Acad. Dermatol. Venereol. 2019, 33, e201–e203. [Google Scholar] [CrossRef]
- Hofmann-Wellenhof, R.; Pellacani, G.; Malvehy, J.; Soyer, H.P. Reflectance Confocal Microscopy for Skin Diseases; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar] [CrossRef]
- Ahlgrimm-Siess, V.; Laimer, M.; Rabinovitz, H.S.; Oliviero, M.; Hofmann-Wellenhof, R.; Marghoob, A.A.; Scope, A. Confocal Microscopy in Skin Cancer. Curr. Dermatol. Rep. 2018, 7, 105–118. [Google Scholar] [CrossRef]
- Vega Memije, M.E.; Luna, E.M.; de Almeida, O.P.; Taylor, A.M.; Cuevas González, J.C. Immunohistochemistry panel for differential diagnosis of Basal cell carcinoma and trichoblastoma. Int. J. Trichology 2014, 6, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Baigrie, D.; Troxell, T.; Cook, C. Nevus Sebaceus. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK482493/ (accessed on 15 February 2023).
- Lupu, M.; Voiculescu, V.M.; Caruntu, A.; Tebeica, T.; Caruntu, C. Preoperative evaluation through dermoscopy and reflectance confocal microscopy of the lateral excision margins for primary basal cell carcinoma. Diagnostics 2021, 11, 120. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Voiculescu, V.M.; Celarel, A.M.; Cozma, E.C.; Banciu, M.L.; Lupu, M. Nevus Sebaceous of Jadassohn in Adults—Can Reflectance Confocal Microscopy Detect Malignant Transformation? Diagnostics 2023, 13, 1480. https://doi.org/10.3390/diagnostics13081480
Voiculescu VM, Celarel AM, Cozma EC, Banciu ML, Lupu M. Nevus Sebaceous of Jadassohn in Adults—Can Reflectance Confocal Microscopy Detect Malignant Transformation? Diagnostics. 2023; 13(8):1480. https://doi.org/10.3390/diagnostics13081480
Chicago/Turabian StyleVoiculescu, Vlad Mihai, Ana Maria Celarel, Elena Codruta Cozma, Madalina Laura Banciu, and Mihai Lupu. 2023. "Nevus Sebaceous of Jadassohn in Adults—Can Reflectance Confocal Microscopy Detect Malignant Transformation?" Diagnostics 13, no. 8: 1480. https://doi.org/10.3390/diagnostics13081480