
A CT-Based Radiomics Model for Prediction of Prognosis in Patients with Novel Coronavirus Disease (COVID-19) Pneumonia: A Preliminary Study
 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Patients
2.2. Imaging Acquisition and Segmentation
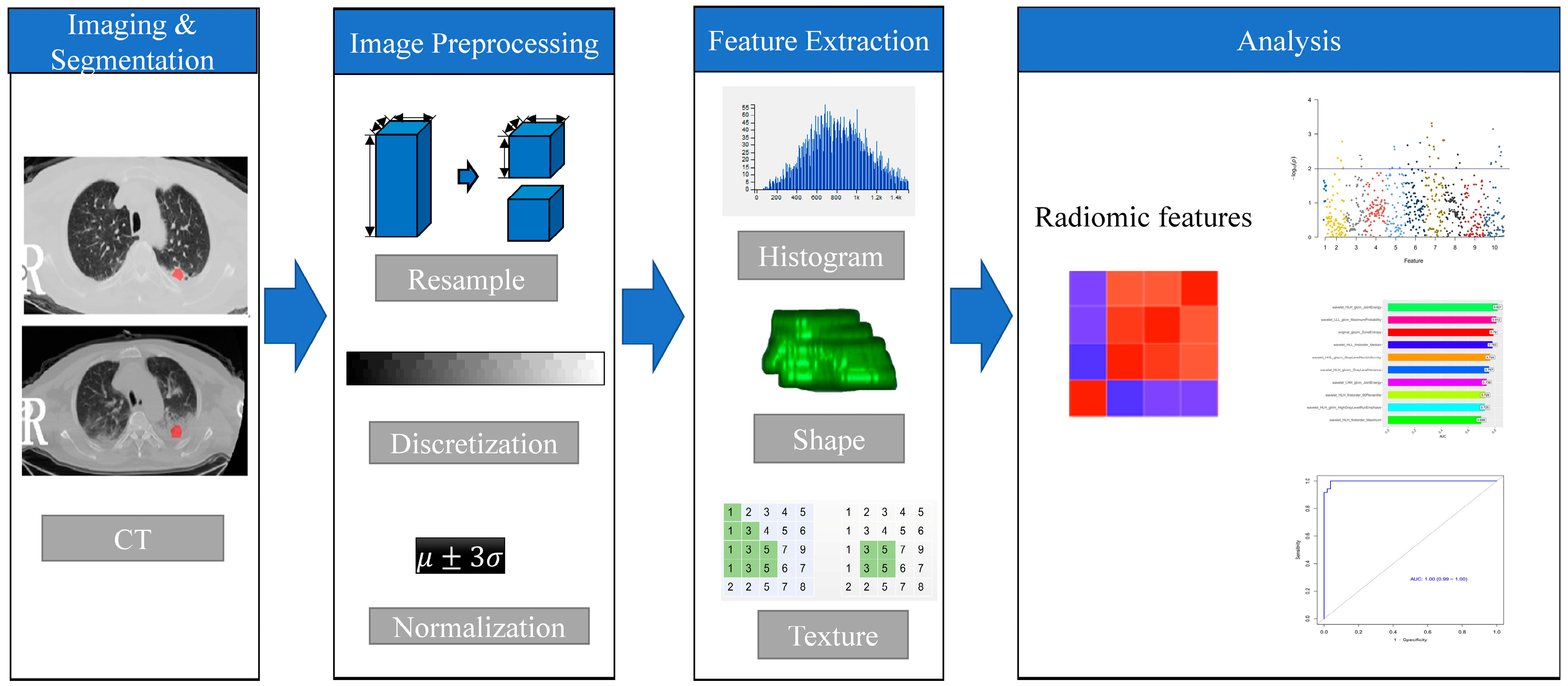
2.3. Radiomics Method
2.4. Radiomics Feature Extraction and Selection
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics
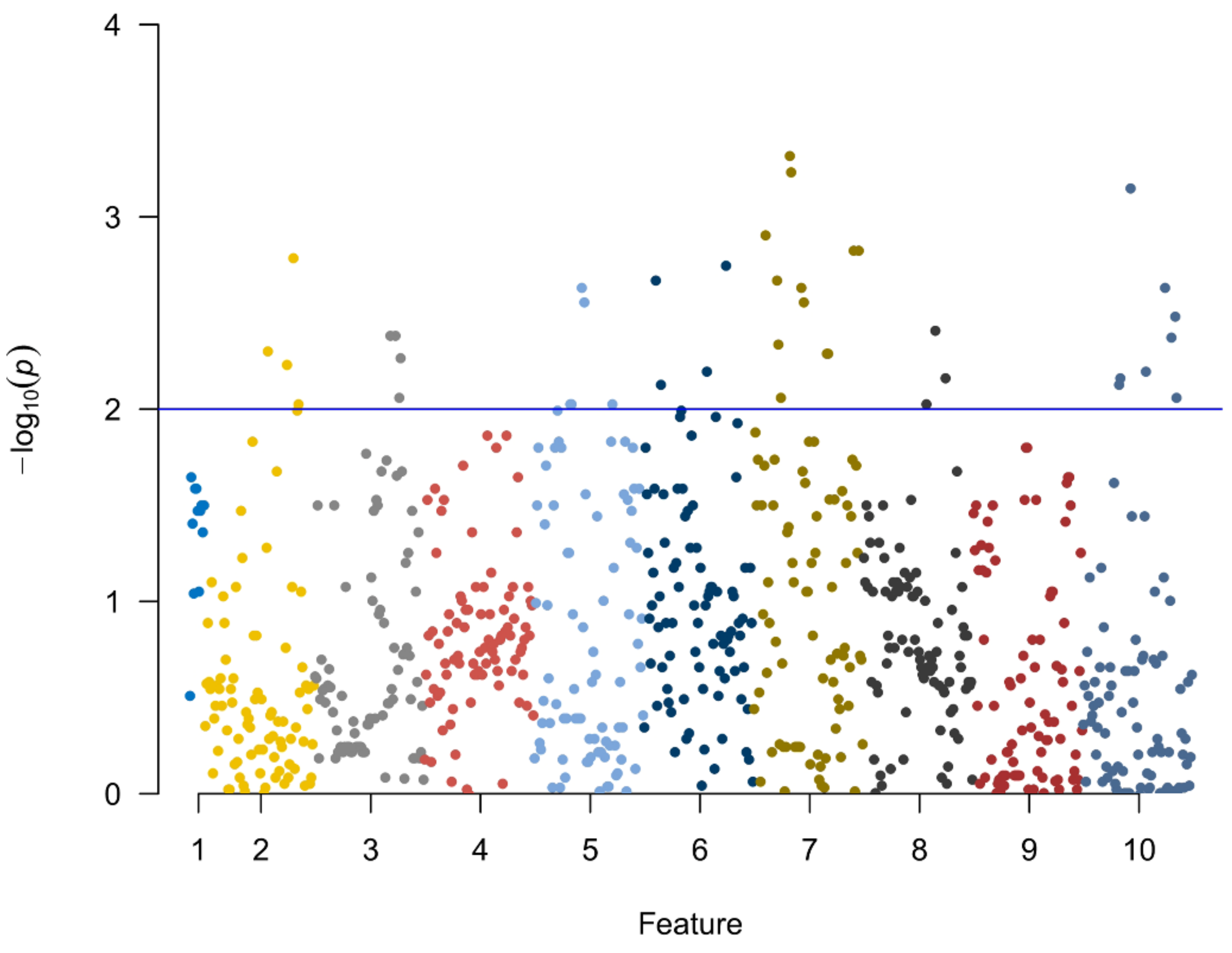
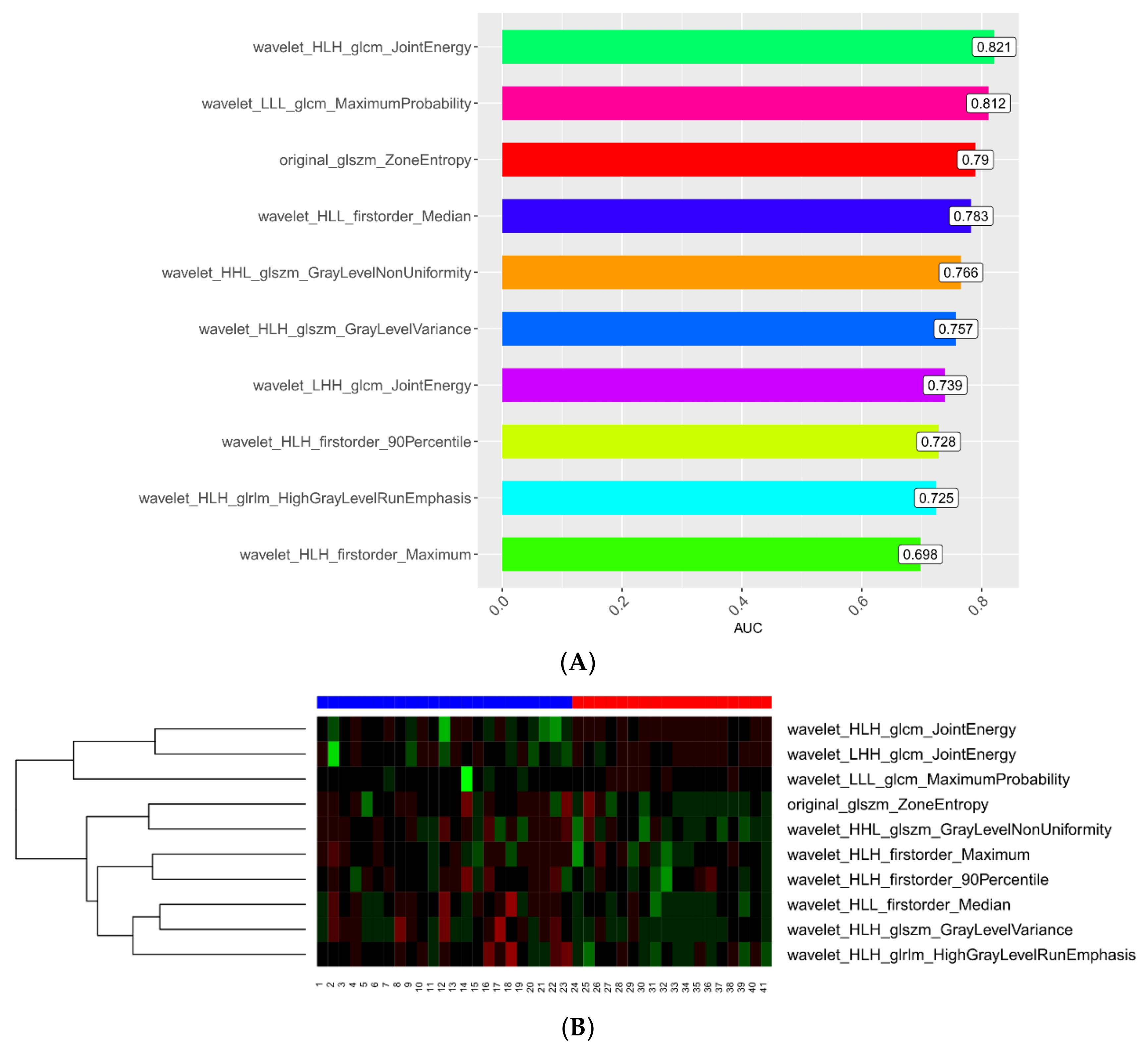
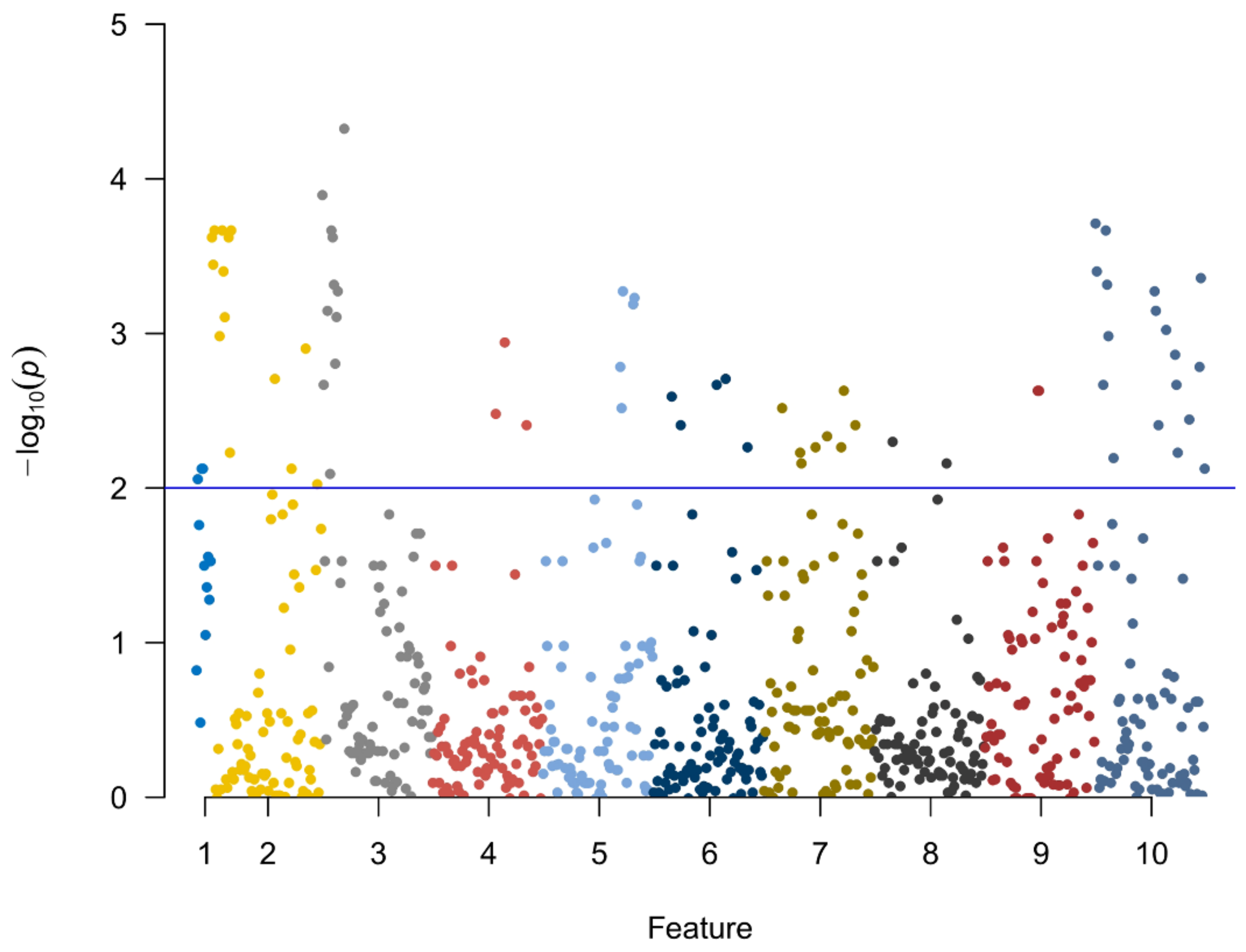
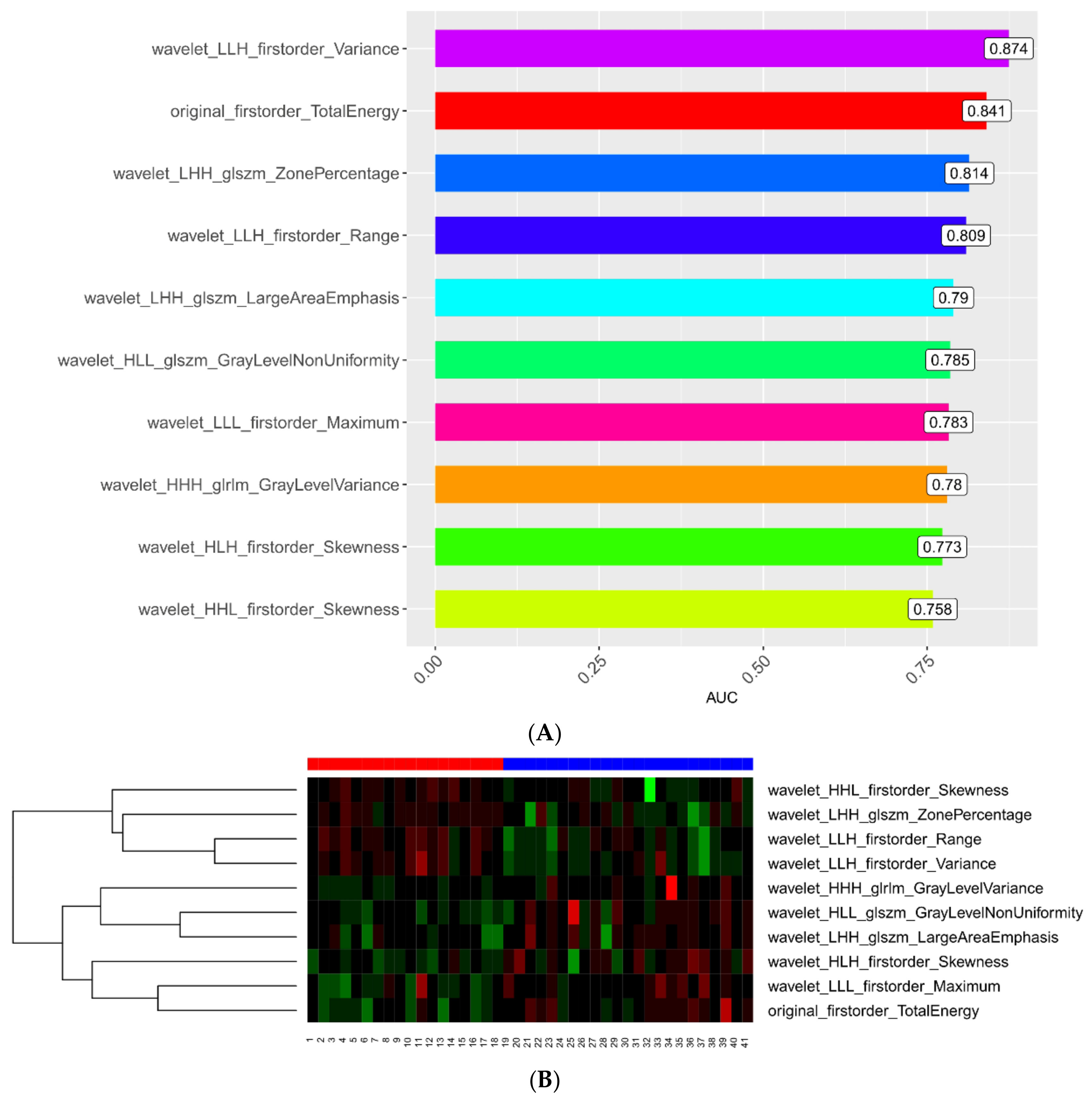
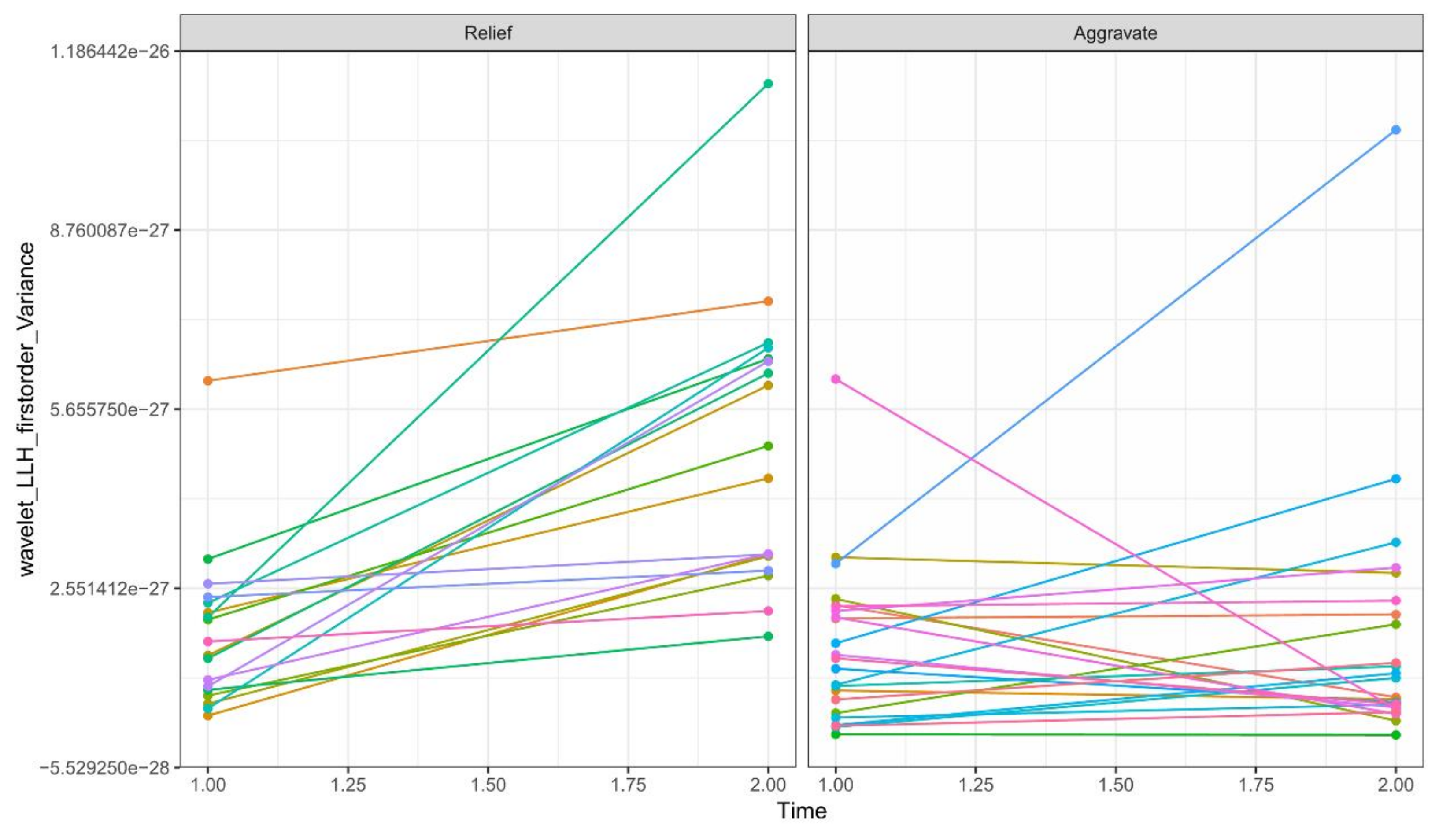
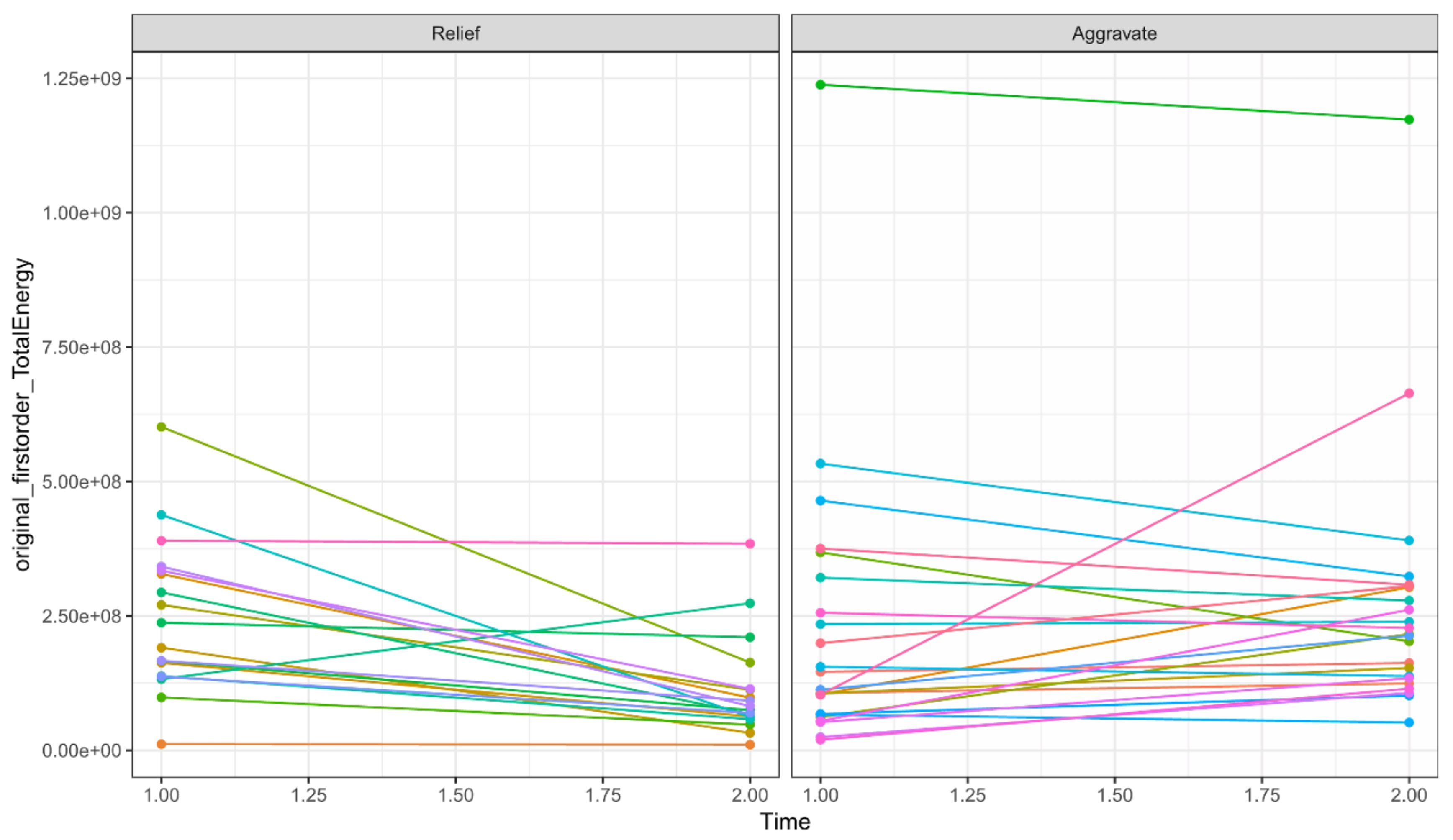
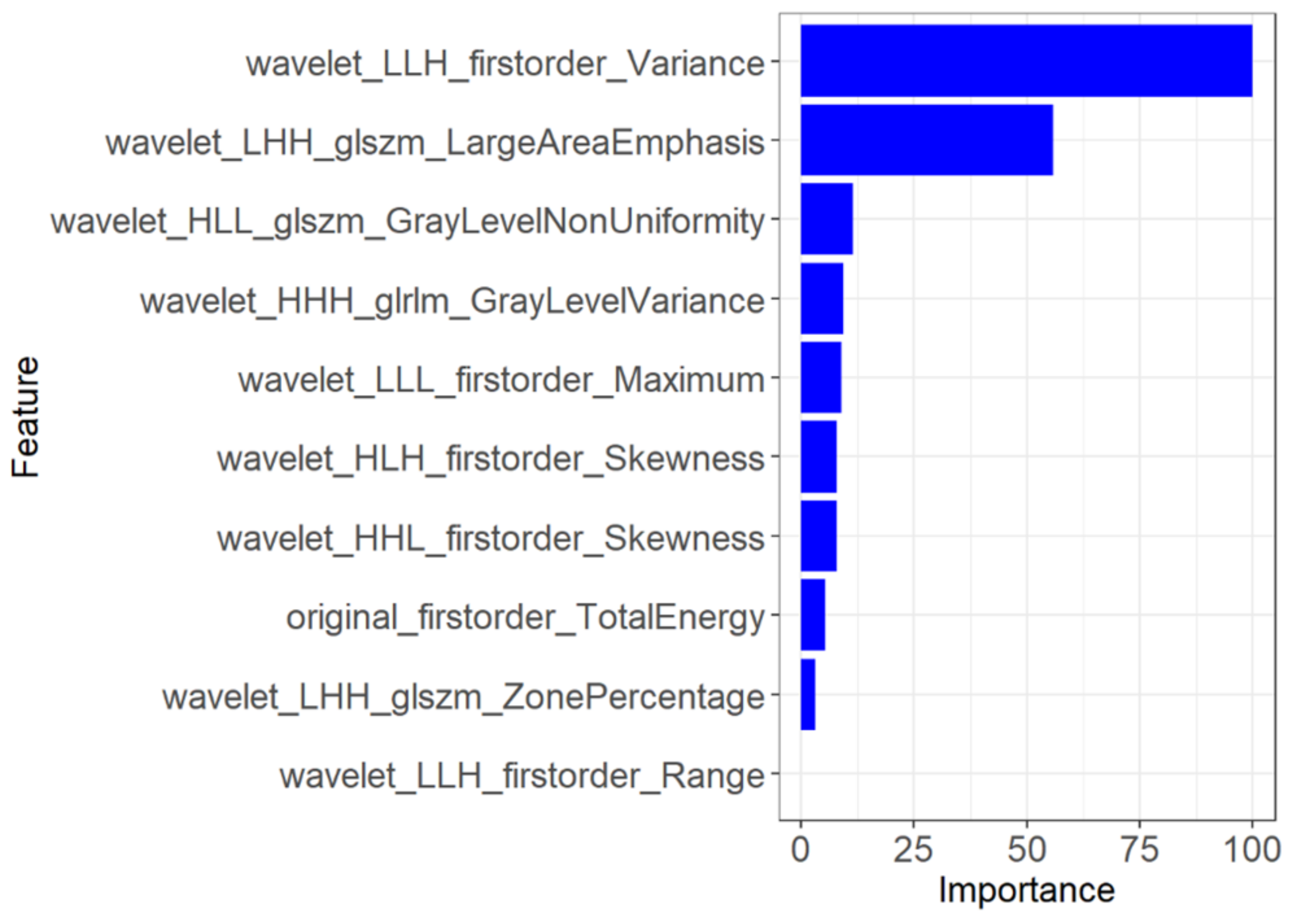
3.2. Feature Extraction and Radiomics Signature Building
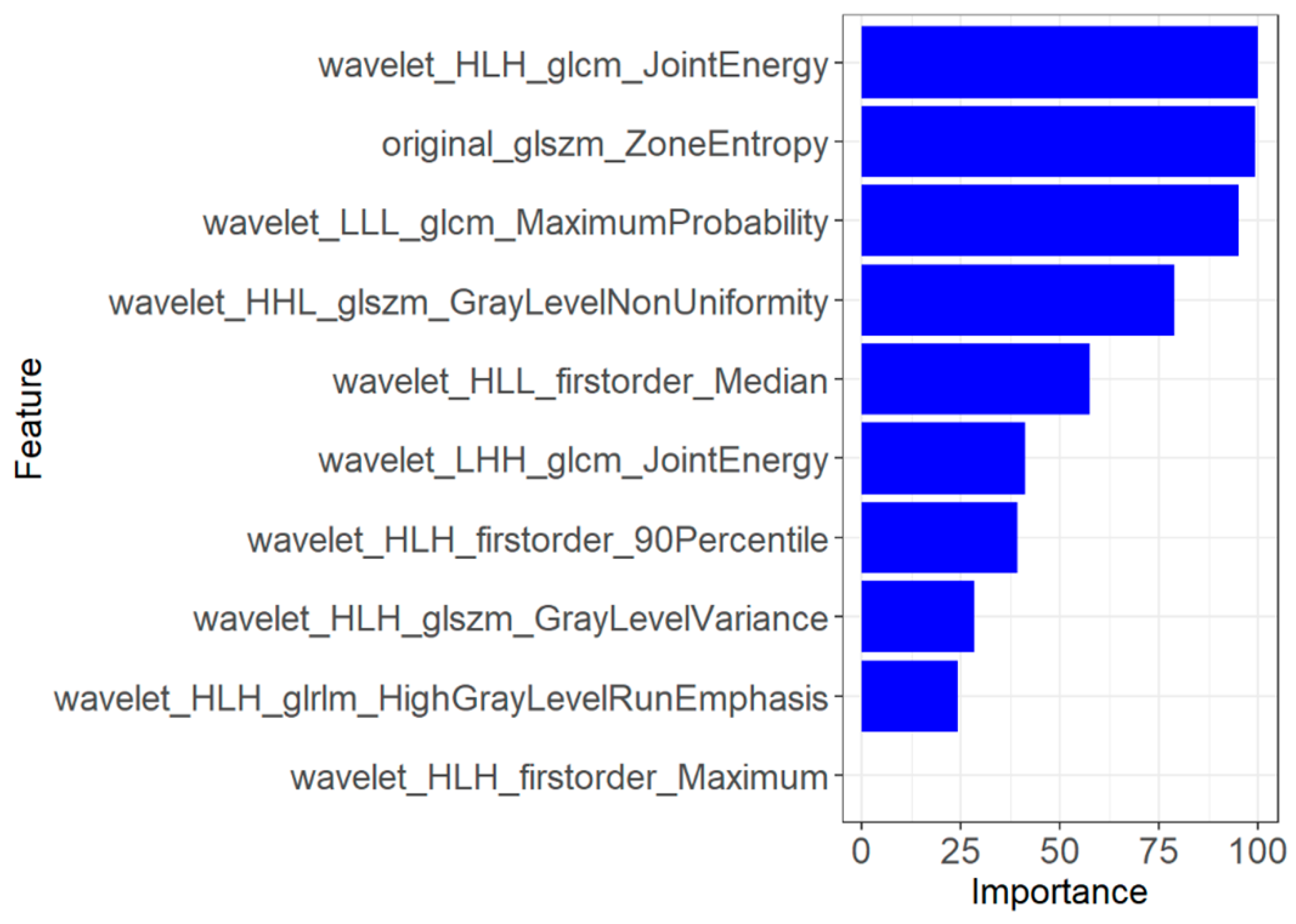
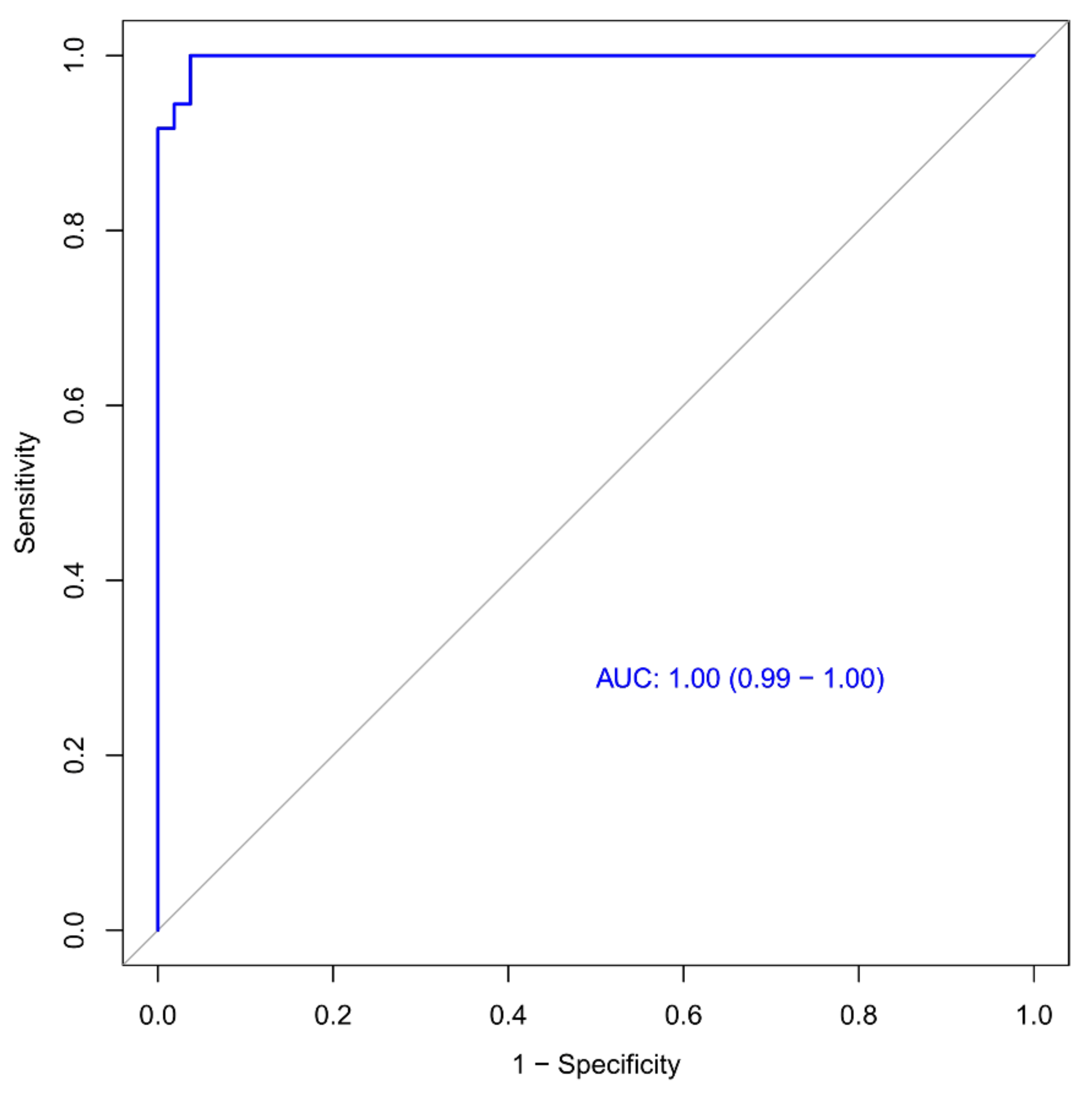
3.3. Building the Prediction Model and ROC Curve Analysis
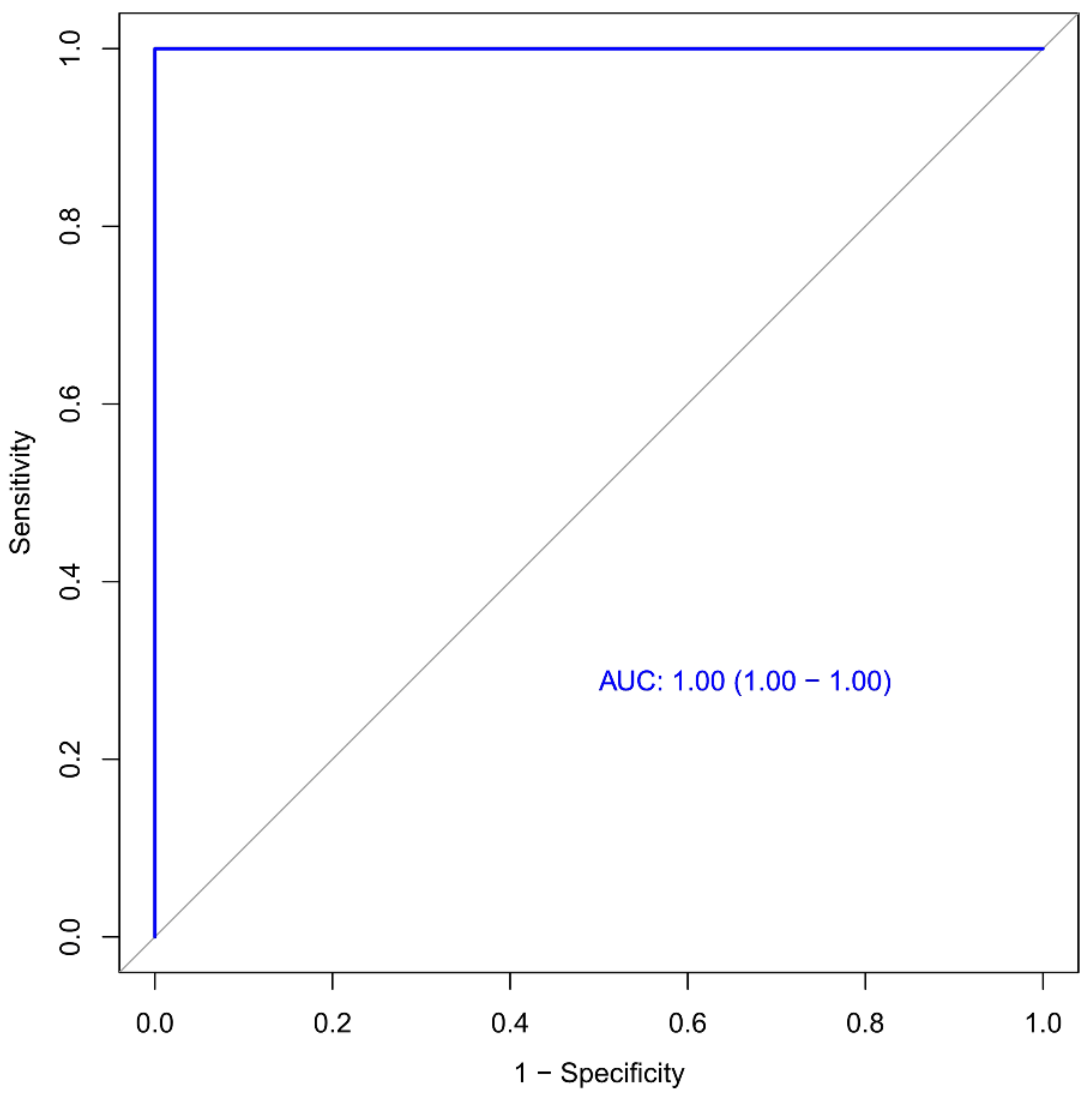
3.4. Validation of the Radiomics Signature
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mo, P.; Xing, Y.; Xiao, Y.U.; Deng, L.; Zhao, Q.; Wang, H.; Zhang, Y. Clinical Characteristics of Refractory Coronavirus Disease 2019 in Wuhan, China. Clin. Infect. Dis. 2021, 73, e4208–e4213. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Tan, W. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease 2019 (COVID-19): Situation Report, 73; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Badraoui, R.; Alrashedi, M.M.; El-May, M.V.; Bardakci, F. Acute respiratory distress syndrome: A life threatening associated complication of SARS-CoV-2 infection inducing COVID-19. J. Biomol. Struct. Dyn. 2021, 39, 6842–6851. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Yang, F.; Liu, F.; Yao, H.; Wu, N.; Wu, H. Development and application of a real-time RT-PCR assay to rapidly detect H2 subtype avian influenza A viruses. J. Vet. Diagn. Investig. 2021, 33, 577–581. [Google Scholar] [CrossRef]
- Wu, J.T.; Leung, K.; Leung, G.M. Nowcasting and Forecasting the Potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: A modelling study. Lancet 2020, 395, 689–697. [Google Scholar] [CrossRef]
- Shatri, J.; Tafilaj, L.; Turkaj, A.; Dedushi, K.; Shatri, M.; Bexheti, S.; Mucaj, S.K. The role of chest computed tomography in asymptomatic patients of positive coronavirus disease 2019: A case and literature review. J. Clin. Imaging Sci. 2020, 10, 35. [Google Scholar] [CrossRef]
- Feng, Z.; Yu, Q.; Yao, S.; Luo, L.; Zhou, W.; Mao, X.; Wang, W. Early prediction of disease progression in COVID-19 pneumonia patients with chest CT and clinical characteristics. Nat. Commun. 2020, 11, 4968. [Google Scholar] [CrossRef]
- Li, M.; Lei, P.; Zeng, B.; Li, Z.; Yu, P.; Fan, B.; Liu, H. Coronavirus disease (COVID-19): Spectrum of CT findings and temporal progression of the disease. Acad. Radiol. 2020, 27, 603–608. [Google Scholar] [CrossRef]
- Dai, W.C.; Zhang, H.W.; Yu, J.; Xu, H.J.; Chen, H.; Luo, S.P.; Lin, F. CT imaging and differential diagnosis of COVID-19. Can. Assoc. Radiol. J. 2020, 71, 195–200. [Google Scholar] [CrossRef]
- Yang, B.; Guo, L.; Lu, G.; Shan, W.; Duan, L.; Duan, S. Radiomic signature: A non-invasive biomarker for discriminating invasive and non-invasive cases of lung adenocarcinoma. Cancer Manag. Res. 2019, 11, 7825. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images are more than pictures, they are data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef]
- Zhang, B.; Ni-Jia-Ti, M.Y.D.L.; Yan, R.; An, N.; Chen, L.; Liu, S.; Zhang, S. CT-based radiomics for predicting the rapid progression of coronavirus disease 2019 (COVID-19) pneumonia lesions. Br. J. Radiol. 2021, 94, 20201007. [Google Scholar] [CrossRef]
- Fu, L.; Li, Y.; Cheng, A.; Pang, P.; Shu, Z. A novel machine learning-derived radiomic signature of the whole lung differentiates stable from progressive COVID-19 infection: A retrospective cohort study. J. Thorac. Imaging 2020, 35, 361. [Google Scholar] [CrossRef]
- Rizzetto, F.; Berta, L.; Zorzi, G.; Cincotta, A.; Travaglini, F.; Artioli, D.; Vanzulli, A. Diagnostic Performance in Differentiating COVID-19 from Other Viral Pneumonias on CT Imaging: Multi-Reader Analysis Compared with an Artificial Intelligence-Based Model. Tomography 2022, 8, 2815–2827. [Google Scholar] [CrossRef]
- Park, C.J.; Park, Y.W.; Ahn, S.S.; Kim, D.; Kim, E.H.; Kang, S.G.; Lee, S.K. Quality of radiomics research on brain metastasis: A roadmap to promote clinical translation. Korean J. Radiol. 2022, 23, 77. [Google Scholar] [CrossRef]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.; Andrearczyk, V.; Apte, A.; Löck, S. The image biomarker standardization initiative: Standardized quantitative radiomics for high-throughput image-based phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef]
- Ashburner, J. Computational anatomy with the SPM software. Magn. Reson. Imaging 2009, 27, 1163–1174. [Google Scholar] [CrossRef]
- Mukaka, M. Statistics corner: A guide to appropriate use of correlation in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar]
- Lv, P.; Peng, F.; Zhang, Y.; Zhang, L.; Li, N.; Sun, L.; Wang, X. COVID-19-associated meningoencephalitis: A care report and literature review. Exp. Ther. Med. 2021, 21, 362. [Google Scholar] [CrossRef]
- Bera, K.; Braman, N.; Gupta, A.; Velcheti, V.; Madabhushi, A. Predicting cancer outcomes with radiomics and artificial intelligence in radiology. Nat. Rev. Clin. Oncol. 2022, 19, 132–146. [Google Scholar] [CrossRef]
- Ferro, M.; de Cobelli, O.; Musi, G.; Del Giudice, F.; Carrieri, G.; Busetto, G.M.; Tătaru, O.S. Radiomics in prostate cancer: An up-to-date review. Ther. Adv. Urol. 2022, 14, 17562872221109020. [Google Scholar] [CrossRef] [PubMed]
- Huang, E.P.; O’Connor, J.P.; McShane, L.M.; Giger, M.L.; Lambin, P.; Kinahan, P.E.; Shankar, L.K. Criteria for the translation of radiomics into clinically useful tests. Nat. Rev. Clin. Oncol. 2023, 20, 69–82. [Google Scholar] [CrossRef] [PubMed]
- Khaniabadi, P.M.; Bouchareb, Y.; Al-Dhuhli, H.; Shiri, I.; Al-Kindi, F.; Khaniabadi, B.M.; Rahmim, A. Two-step machine learning to diagnose and predict involvement of lungs in COVID-19 and pneumonia using CT radiomics. Comput. Biol. Med. 2022, 150, 106165. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Ren, H.; Wu, Z.; Xu, H.; Zhang, S.; Li, J.; Wang, D. CT radiomics facilitates more accurate diagnosis of COVID-19 pneumonia: Compared with CO-RADS. J. Transl. Med. 2021, 19, 29. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Wang, S.; Li, L.; Qian, W.; Hu, Y.; Li, L.; Tian, J. Radiomics analysis of computed tomography helps predict poor prognostic outcome in COVID-19. Theranostics 2020, 10, 7231. [Google Scholar] [CrossRef]
- Homayounieh, F.; Babaei, R.; Mobin, H.K.; Arru, C.D.; Sharifian, M.; Mohseni, I.; Kalra, M.K. Computed tomography radiomics can predict disease severity and outcome in coronavirus disease 2019 pneumonia. J. Comput. Assist. Tomogr. 2020, 44, 640–646. [Google Scholar] [CrossRef]
- Li, K.; Fang, Y.; Li, W.; Pan, C.; Qin, P.; Zhong, Y.; Li, S. CT image visual quantitative evaluation and clinical classification of coronavirus disease (COVID-19). Eur. Radiol. 2020, 30, 4407–4416. [Google Scholar] [CrossRef]
- Li, K.; Wu, J.; Wu, F.; Guo, D.; Chen, L.; Fang, Z.; Li, C. The clinical and chest CT features associated with severe and critical COVID-19 pneumonia. Investig. Radiol. 2020. [Google Scholar] [CrossRef]
- Han, R.; Huang, L.; Jiang, H.; Dong, J.; Peng, H.; Zhang, D. Early clinical and CT manifestations of coronavirus disease 2019 (COVID-19) pneumonia. AJR Am. J. Roentgenol. 2020, 215, 338–343. [Google Scholar] [CrossRef]
- Lee, E.Y.; Ng, M.Y.; Khong, P.L. COVID-19 pneumonia: What has CT taught us? Lancet Infect. Dis. 2020, 20, 384–385. [Google Scholar] [CrossRef]
- Xiong, Y.; Sun, D.; Liu, Y.; Fan, Y.; Zhao, L.; Li, X.; Zhu, W. Clinical and high-resolution CT features of the COVID-19 infection: Comparison of the initial and follow-up changes. Investig. Radiol. 2020, 55, 332–339. [Google Scholar] [CrossRef]
- Deng, Y.; Lei, L.; Chen, Y.; Zhang, W. The potential added value of FDG PET/CT for COVID-19 pneumonia. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1634–1635. [Google Scholar] [CrossRef]
- Ye, Z.; Zhang, Y.; Wang, Y.; Huang, Z.; Song, B. Chest CT manifestations of new coronavirus disease 2019 (COVID-19): A pictorial review. Eur. Radiol. 2020, 30, 4381–4389. [Google Scholar] [CrossRef]
- Yang, W.; Sirajuddin, A.; Zhang, X.; Liu, G.; Teng, Z.; Zhao, S.; Lu, M. The role of imaging in 2019 novel coronavirus pneumonia (COVID-19). Eur. Radiol. 2020, 30, 4874–4882. [Google Scholar] [CrossRef]
- Wu, J.; Pan, J.; Teng, D.; Xu, X.; Feng, J.; Chen, Y.C. Interpretation of CT signs of 2019 novel coronavirus (COVID-19) pneumonia. Eur. Radiol. 2020, 30, 5455–5462. [Google Scholar] [CrossRef]
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, C. Time course of lung changes at chest CT during recovery from coronavirus disease 2019 (COVID-19). Radiology 2020, 295, 715–721. [Google Scholar] [CrossRef]
- Wang, Y.; Dong, C.; Hu, Y.; Li, C.; Ren, Q.; Zhang, X.; Zhou, M. Temporal changes of CT findings in 90 patients with COVID-19 pneumonia: A longitudinal study. Radiology 2020, 296, E55–E64. [Google Scholar] [CrossRef]
- Lyu, P.; Liu, X.; Zhang, R.; Shi, L.; Gao, J. The performance of chest CT in evaluating the clinical severity of COVID-19 pneumonia: Identifying critical cases based on CT characteristics. Investig. Radiol. 2020, 55, 412–421. [Google Scholar] [CrossRef]
- Wu, J.; Wu, X.; Zeng, W.; Guo, D.; Fang, Z.; Chen, L.; Li, C. Chest CT findings in patients with coronavirus disease 2019 and its relationship with clinical features. Investig. Radiol. 2020, 55, 257. [Google Scholar] [CrossRef]
- Song, L.; Zhu, Z.; Mao, L.; Li, X.; Han, W.; Du, H.; Jin, Z. Clinical, conventional CT and radiomic feature-based machine learning models for predicting ALK rearrangement status in lung adenocarcinoma patients. Front. Oncol. 2020, 10, 369. [Google Scholar] [CrossRef]
- Li, L.; Wang, L.; Zeng, F.; Peng, G.; Ke, Z.; Liu, H.; Zha, Y. Development and multicenter validation of a CT-based radiomics signature for predicting severe COVID-19 pneumonia. Eur. Radiol. 2021, 31, 7901–7912. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Aggravate Group (n = 23) | Relief Group (n = 21) | All (n = 44) | p |
|---|---|---|---|---|
| Age, mean ± SD (y) * | 45 ± 15 | 49 ± 13 | 47 ± 14 | 0.448 † |
| Gender (male/female) | 12/11 | 15/6 | 27/44 | 0.190 † |
| Location of lesion, n (%) | 0.947 † | |||
| Subpleural | 22 (95.7) | 20 (95.2) | 42 (95.5) | |
| others | 1 (4.3) | 1 (4.8) | 2 (4.5) | |
| Range (lobes of lung), n (%) | 0.966 # | |||
| 1 | 4 (17.4) | 4 (19.0) | 8 (18.2) | |
| 2 | 4 (17.4) | 2 (9.5) | 6 (13.6) | |
| 3 | 2 (8.7) | 2 (9.5) | 4 (9.1) | |
| 4 | 5 (21.7) | 5 (23.8) | 10 (22.7) | |
| 5 | 8 (34.8) | 8 (38.1) | 16 (36.4) | |
| Density, n (%) | 0.123 # | |||
| Ground-glass opacity | 11 (47.8) | 4 (19.0) | 14 (31.8) | |
| Mix ground glass | 10 (43.5) | 15 (71.4) | 25 (56.8) | |
| solid | 2 (8.7) | 2 (9.5) | 4 (9.1) | |
| Paving stone sign | 9 (39.1) | 12 (57.1) | 21 (47.7) | 0.583 † |
| Air bronchi sign | 14 (60.9) | 13 (61.9) | 27 (61.4) | 0.131 † |
| Vascular thickening | 15 (65.2) | 9 (42.9) | 24 (54.5) | 0.232 † |
| Fiber chords | 11 (47.8) | 13 (61.9) | 24 (54.5) | 0.349 † |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duan, L.; Zhang, L.; Lu, G.; Guo, L.; Duan, S.; Zhou, C. A CT-Based Radiomics Model for Prediction of Prognosis in Patients with Novel Coronavirus Disease (COVID-19) Pneumonia: A Preliminary Study. Diagnostics 2023, 13, 1479. https://doi.org/10.3390/diagnostics13081479
Duan L, Zhang L, Lu G, Guo L, Duan S, Zhou C. A CT-Based Radiomics Model for Prediction of Prognosis in Patients with Novel Coronavirus Disease (COVID-19) Pneumonia: A Preliminary Study. Diagnostics. 2023; 13(8):1479. https://doi.org/10.3390/diagnostics13081479
Chicago/Turabian StyleDuan, Lizhen, Longjiang Zhang, Guangming Lu, Lili Guo, Shaofeng Duan, and Changsheng Zhou. 2023. "A CT-Based Radiomics Model for Prediction of Prognosis in Patients with Novel Coronavirus Disease (COVID-19) Pneumonia: A Preliminary Study" Diagnostics 13, no. 8: 1479. https://doi.org/10.3390/diagnostics13081479