
Prognostic Performance of Bedside Lung Ultrasound Score (LUSS) and ROX Index in Hypoxemic Respiratory Failure Due to COVID-19
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
- Age ≥ 18 years;
- Confirmed COVID-19 pneumonia (positive test result using reverse-transcriptase polymerase chain reaction, RT-PCR, assay of a nasopharyngeal swab); Alert of the hospital Medical Emergency Team for clinical worsening: PaO2/FiO2 ratio < 300 mmHg despite oxygen therapy, respiratory rate > 22 breaths per minute and/or respiratory distress.
2.1. LUS Protocol
- Lung parenchyma score: A score of 0 was assigned for no B-lines in a single intercostal space, a score of 1 was assigned for multiple spaced or isolated B-lines, a score of 2 was assigned for diffuse coalescent B-lines, and a score of 3 was assigned for lung consolidations.
- Pleural line score: A score of 0 was assigned for a normal, continuous, hyperechoic pleural line; a score of 1 was assigned for a discontinuous, irregular pleural line; and a score of 2 was assigned for a broken or a blurred pleural line.
2.2. Clinical Data
2.3. Statistical Analyses
3. Results
3.1. Study Population
3.2. Ventilatory Variables and Outcomes
3.3. Multivariable Analyses
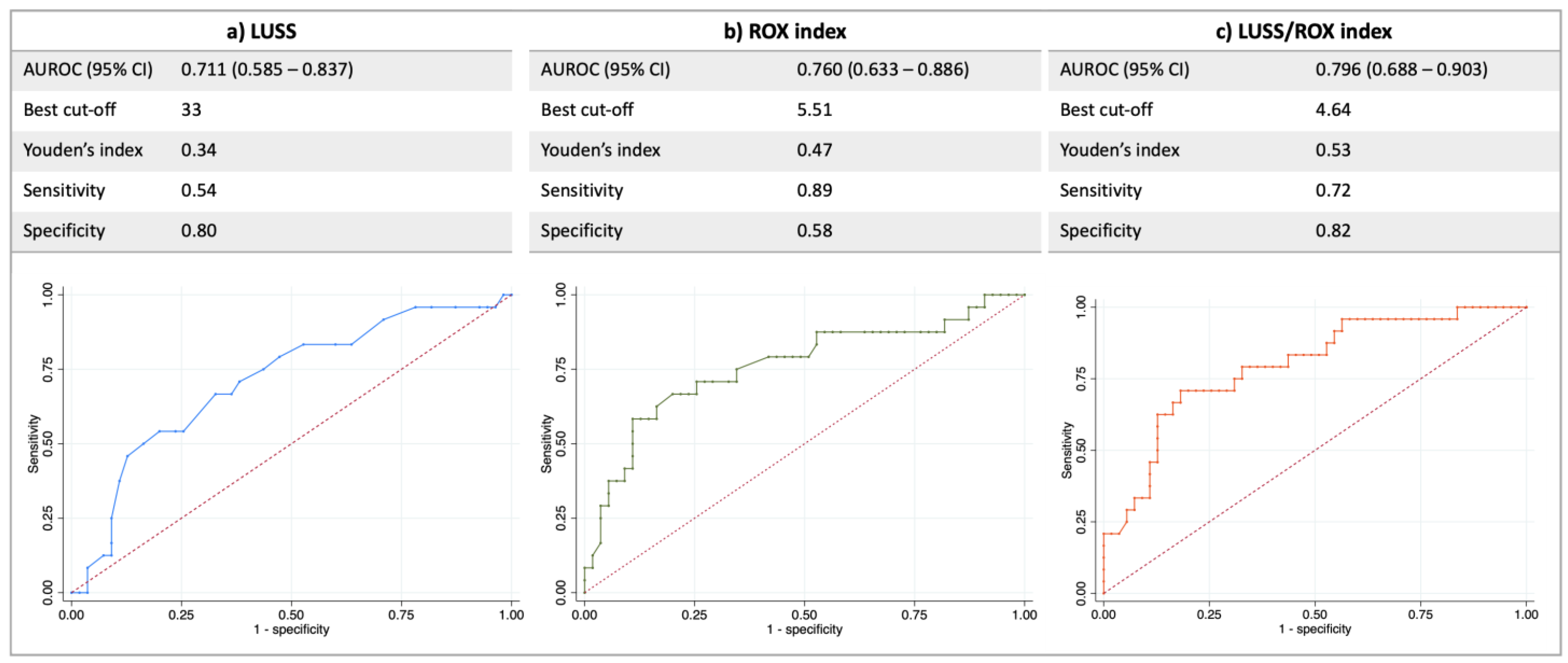
3.4. Prognostic Performance of the 3 Indices
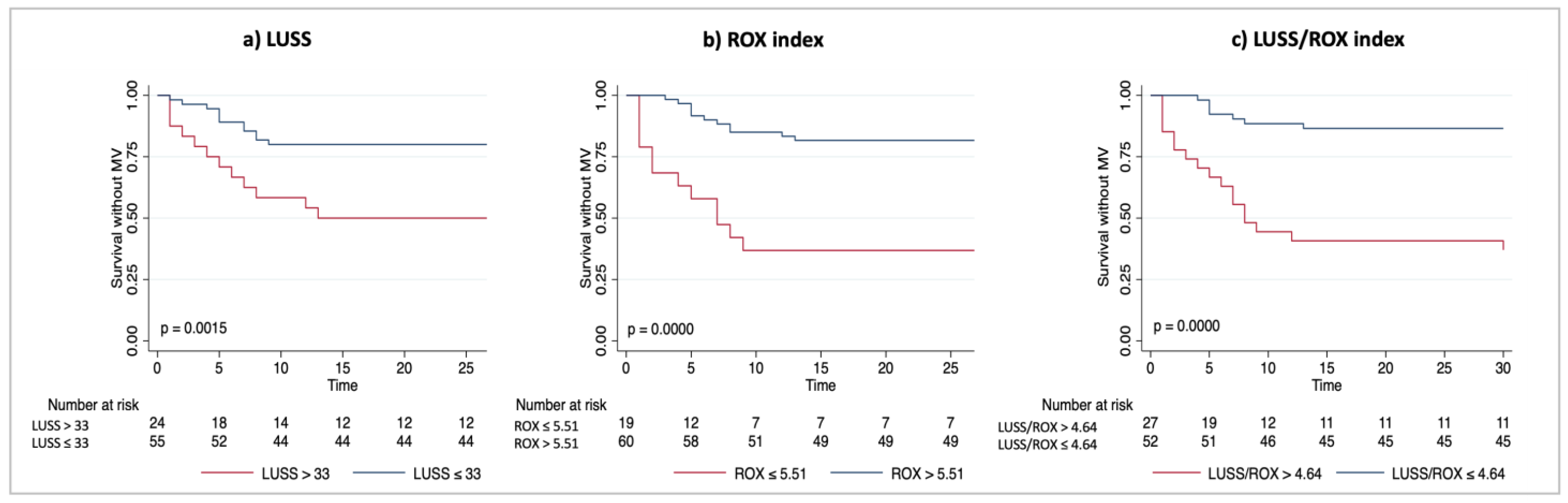
3.5. Unadjusted Survival Analysis at 30-Day Follow-Up
4. Discussion
- −
- All three indices (ROX, LUSS and LUSS/ROX) were independently associated with a negative outcome in the univariable analysis, and this association was confirmed in the multivariable analyses.
- −
- Although the comparison between the AUC of LUSS or ROX versus LUSS/ROX did not reveal a statistically significant difference, we observed a trend toward a better outcome prediction using the LUSS/ROX index as compared to using LUSS; furthermore, the AUROC of the combined LUSS/ROX index improved the low sensitivity of LUSS and the low specificity of the ROX index.
- −
- Using the Kaplan–Meier approach, a statistically significant difference in survival without invasive mechanical ventilation was observed by stratifying the population using all three indices. We observed a higher probability of survival without mechanical ventilation over the 30-day follow-up by using the combined LUSS/ROX best cut-off (p = 0.0000 by log-rank test) (Figure 2c) when compared with LUSS best cut-off (p = 0.0015 by log-rank test) (Figure 2a).
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rezoagli, E.; Magliocca, A.; Bellani, G.; Pesenti, A.; Grasselli, G. Development of a Critical Care Response—Experiences from Italy During the Coronavirus Disease 2019 Pandemic. Anesthesiol. Clin. 2021, 39, 265–284. [Google Scholar] [CrossRef] [PubMed]
- Wendel-Garcia, P.D.; Moser, A.; Jeitziner, M.-M.; Aguirre-Bermeo, H.; Arias-Sanchez, P.; Apolo, J.; Roche-Campo, F.; Franch-Llasat, D.; Kleger, G.-R.; Schrag, C.; et al. Dynamics of disease characteristics and clinical management of critically ill COVID-19 patients over the time course of the pandemic: An analysis of the prospective, international, multicentre RISC-19-ICU registry. Crit. Care 2022, 26, 199. [Google Scholar] [CrossRef] [PubMed]
- Bellani, G.; Grasselli, G.; Cecconi, M.; Antolini, L.; Borelli, M.; De Giacomi, F.; Bosio, G.; Latronico, N.; Filippini, M.; Gemma, M.; et al. Noninvasive Ventilatory Support of Patients with COVID-19 outside the Intensive Care Units (WARd-COVID). Ann. Am. Thorac. Soc. 2021, 18, 1020–1026. [Google Scholar] [CrossRef] [PubMed]
- Garcia, P.D.W.; Aguirre-Bermeo, H.; Buehler, P.K.; Alfaro-Farias, M.; Yuen, B.; David, S.; Tschoellitsch, T.; Wengenmayer, T.; Korsos, A.; Fogagnolo, A.; et al. Implications of early respiratory support strategies on disease progression in critical COVID-19: A matched subanalysis of the prospective RISC-19-ICU cohort. Crit. Care 2021, 25, 175. [Google Scholar] [CrossRef] [PubMed]
- Roca, O.; Caralt, B.; Messika, J.; Samper, M.; Sztrymf, B.; Hernández, G.; García-De-Acilu, M.; Frat, J.-P.; Masclans, J.R.; Ricard, J.-D. An Index Combining Respiratory Rate and Oxygenation to Predict Outcome of Nasal High-Flow Therapy. Am. J. Respir. Crit. Care Med. 2019, 199, 1368–1376. [Google Scholar] [CrossRef] [PubMed]
- Colaianni-Alfonso, N.; Montiel, G.C.; Castro-Sayat, M.; Roca, O.; Grieco, D.L. ROX index to predict CPAP outcome in hypoxemic respiratory failure due to COVID-19. Intensiv. Care Med. 2022, 48, 1818–1819. [Google Scholar] [CrossRef]
- Lichtenstein, D.A. BLUE-protocol and FALLS-protocol: Two applications of lung ultrasound in the critically ill. Chest 2015, 147, 1659–1670. [Google Scholar] [CrossRef] [Green Version]
- Rezoagli, E.; Fumagalli, R.; Bellani, G. Definition and epidemiology of acute respiratory distress syndrome. Ann. Transl. Med. 2017, 5, 282. [Google Scholar] [CrossRef] [Green Version]
- Rezoagli, E.; Laffey, J.G.; Bellani, G. Monitoring Lung Injury Severity and Ventilation Intensity during Mechanical Ventilation. Semin. Respir. Crit. Care Med. 2022, 43, 346–368. [Google Scholar] [CrossRef]
- Smit, M.R.; Hagens, L.A.; Heijnen, N.F.; Pisani, L.; Cherpanath, T.G.; Dongelmans, D.A.; de Grooth, H.-J.S.; Pierrakos, C.; Tuinman, P.R.; Zimatore, C.; et al. Lung Ultrasound Prediction Model for Acute Respiratory Distress Syndrome: A Multicenter Prospective Observational Study. Am. J. Respir. Crit. Care Med. 2023; ahead of print. [Google Scholar] [CrossRef]
- Soldati, G.; Smargiassi, A.; Inchingolo, R.; Buonsenso, D.; Perrone, T.; Briganti, D.F.; Perlini, S.; Torri, E.; Mariani, A.; Mossolani, E.E.; et al. Proposal for International Standardization of the Use of Lung Ultrasound for Patients With COVID-19: A Simple, Quantitative, Reproducible Method. J. Ultrasound Med. 2020, 39, 1413–1439. [Google Scholar] [CrossRef] [Green Version]
- Volpicelli, G.; Lamorte, A.; Villén, T. What’s new in lung ultrasound during the COVID-19 pandemic. Intensiv. Care Med. 2020, 46, 1445–1448. [Google Scholar] [CrossRef] [PubMed]
- Allinovi, M.; Parise, A.; Giacalone, M.; Amerio, A.; Delsante, M.; Odone, A.; Franci, A.; Gigliotti, F.; Amadasi, S.; Delmonte, D.; et al. Lung Ultrasound May Support Diagnosis and Monitoring of COVID-19 Pneumonia. Ultrasound Med. Biol. 2020, 46, 2908–2917. [Google Scholar] [CrossRef] [PubMed]
- de Alencar, J.C.G.; Marchini, J.F.M.; Marino, L.O.; Ribeiro, S.C.D.C.; Bueno, C.G.; da Cunha, V.P.; Neto, F.L.; Neto, R.A.B.; Souza, H.P.; The COVID U. S. P. Registry Team. Lung ultrasound score predicts outcomes in COVID-19 patients admitted to the emergency department. Ann. Intensiv. Care 2021, 11, 6. [Google Scholar] [CrossRef]
- Lichter, Y.; Topilsky, Y.; Taieb, P.; Banai, A.; Hochstadt, A.; Merdler, I.; Oz, A.G.; Vine, J.; Goren, O.; Cohen, B.; et al. Lung ultrasound predicts clinical course and outcomes in COVID-19 patients. Intensiv. Care Med. 2020, 46, 1873–1883. [Google Scholar] [CrossRef] [PubMed]
- Brahier, T.; Meuwly, J.-Y.; Pantet, O.; Vez, M.-J.B.; Donnet, H.G.; Hartley, M.-A.; Hugli, O.; Boillat-Blanco, N. Lung ultrasonography for risk stratification in patients with Coronavirus Disease 2019 (COVID-19): A prospective observational cohort study. Clin. Infect. Dis. 2020, 73, e4189–e4196. [Google Scholar] [CrossRef]
- Deng, Q.; Zhang, Y.; Wang, H.; Chen, L.; Yang, Z.; Peng, Z.; Liu, Y.; Feng, C.; Huang, X.; Jiang, N.; et al. Semiquantitative lung ultrasound scores in the evaluation and follow-up of critically ill patients with COVID-19: A single-center study. Acad. Radiol. 2020, 27, 1363–1372. [Google Scholar] [CrossRef] [PubMed]
- Ji, L.; Cao, C.; Gao, Y.; Zhang, W.; Xie, Y.; Duan, Y.; Kong, S.; You, M.; Ma, R.; Jiang, L.; et al. Prognostic value of bedside lung ultrasound score in patients with COVID-19. Crit. Care 2020, 24, 700. [Google Scholar] [CrossRef] [PubMed]
- Biasucci, D.G.; Buonsenso, D.; Piano, A.; Bonadia, N.; Vargas, J.; Settanni, D.; Bocci, M.G.; Grieco, D.L.; Carnicelli, A.; Scoppettuolo, G.; et al. Lung ultrasound predicts non-invasive ventilation outcome in COVID-19 acute respiratory failure: A pilot study. Minerva Anestesiol. 2021, 87, 1006–1016. [Google Scholar] [CrossRef]
- Zucman, N.; Mullaert, J.; Roux, D.; Roca, O.; Ricard, J.-D.; Longrois, D.; Dreyfuss, D. Contributors Prediction of outcome of nasal high flow use during COVID-19-related acute hypoxemic respiratory failure. Intensiv. Care Med. 2020, 46, 1924–1926. [Google Scholar] [CrossRef]
- Rezoagli, E.; Bellani, G. How I set up positive end-expiratory pressure: Evidence- and physiology-based! Crit. Care 2019, 23, 412. [Google Scholar] [CrossRef] [Green Version]
- Rezoagli, E.; Coppola, G.; Dezza, L.; Galesi, A.; Gallo, G.; Fumagalli, R.; Bellani, G.; Foti, G.; Lucchini, A. High efficiency particulate air filters and heat & moisture exchanger filters increase positive end-expiratory pressure in helmet continuous positive airway pressure: A bench-top study. Pulmonology, 2022; in press. [Google Scholar] [CrossRef]
- Nova, A.; Rezoagli, E.; Eronia, N.; Foti, G.; Bellani, G. Role of PEEP on the prognostic performance of the ROX index in hypoxemic respiratory failure due to COVID-19: Any further gain in outcome prediction? Intensiv. Care Med. 2023, 49, 355–356. [Google Scholar] [CrossRef] [PubMed]
- Bouhemad, B.; Brisson, H.; Le-Guen, M.; Arbelot, C.; Lu, Q.; Rouby, J.-J. Bedside Ultrasound Assessment of Positive End-Expiratory Pressure–induced Lung Recruitment. Am. J. Respir. Crit. Care Med. 2011, 183, 341–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Overall Population n = 79 | Negative Outcome n = 24 (30%) | Positive Outcome n = 55 (70%) | p-Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age, years | 61 [52–71] | 68 [59–75] | 60 [50–70] | 0.067 |
| Sex, female, n | 28 (35%) | 9 (38%) | 19 (35%) | 0.801 |
| BMI, Kg/m2 | 28 [26–33] | 30 [27–34] | 27 [25–32] | 0.052 |
| Comorbidities | ||||
| COPD | 11 (14%) | 3 (13%) | 8 (15%) | 0.809 |
| Diabetes | 7 (9%) | 1 (4%) | 6 (11%) | 0.332 |
| Chronic renal failure | 1 (1%) | 0 (0%) | 1 (2%) | 0.506 |
| Hypertension | 31 (39%) | 11 (46%) | 20 (36%) | 0.428 |
| Ischemic cardiomyopathy | 3 (4%) | 2 (8%) | 1 (2%) | 0.164 |
| Neoplasia | 2 (2%) | 1 (4%) | 1 (2%) | 0.541 |
| Immunosuppression | 2 (2%) | 2 (8%) | 0 (0%) | 0.030 |
| Ventilatory setting | ||||
| Venturi mask | 10 (13%) | 1 (4%) | 9 (16%) | 0.143 |
| HFNO | 3 (4%) | 0 (0%) | 3 (5%) | |
| CPAP | 66 (84%) | 23 (96%) | 43 (78%) | |
| PEEP, cmH2O | 8 [5–10] | 10 [8–10] | 8 [5–10] | 0.014 |
| FiO2 | 60 [50–80] | 75 [65–100] | 50 [50–70] | <0.001 |
| Clinical illness severity | ||||
| SOFA baseline | 2 [2–2] | 2 [2–2] | 2 [1–2] | 0.299 |
| PCR (mg/L) | 6.70 [3.40–12.27] | 5.00 [3.37–12.90] | 7.36 [3.87–11.78] | 0.534 |
| Lymphocytes (cells/mL) | 853 (±316) | 760 (±72) | 889 (±41) | 0.112 |
| D-dimer (μg/mL) | 345 [208–540] | 386 [260–536] | 334 [208–540] | 0.431 |
| PaO2, mmHg | 131 [89–210] | 118 [87–220] | 134 [92–210] | 0.561 |
| PaCO2, mmHg | 36 [33–40] | 37 [33–41] | 36 [33–40] | 0.685 |
| SpO2, % | 99 [97–99] | 98 [97–99] | 99 [98–99] | 0.326 |
| PaO2/FiO2 | 245 (±101) | 197 (±93) | 266 (±98) | 0.005 |
| RR, breaths per minute | 24 [20–28] | 26 [22–31] | 24 [20–26] | 0.028 |
| NIV failure indices | ||||
| ROX index | 7.07 [5.51–9.80] | 5.14 [3.43–7.01] | 7.55 [6.25–10.00] | <0.001 |
| LUSS | 27 (±9) | 31 (±8) | 25 (±9) | <0.001 |
| LUSS/ROX | 3.70 [2.49–5.73] | 6.02 [3.94–8.76] | 3.43 [2.10–4.29] | <0.001 |
| Variable | OR (95% CI) | p-Value | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
|---|---|---|---|---|---|---|
| BMI | 1.077 (0.94–1.23) | 0.277 | 1.07 (0.95–1.22) | 0.260 | 1.08 (0.94–1.23) | 0.280 |
| Age | 1.013 (0.96–1.06) | 0.604 | 1.01 (0.97–1.06) | 0.248 | 1.01 (0.97–1.06) | 0.591 |
| PEEP | 1.289 (1.03–1.62) | 0.029 | 1.22 (0.97–1.53) | 0.093 | 1.23 (0.98–1.54) | 0.073 |
| PaO2/FiO2 | 0.992 (0.99–1.00) | 0.020 | 0.99 (0.99–1.00) | 0.069 | 0.99 (0.99–1.00) | 0.064 |
| RR | 0.974 (0.83–1.14) | 0.749 | 1.13 (1.00–1.27) | 0.047 | 1.02 (0.89–1.17) | 0.775 |
| ROX | 0.706 (0.51–0.98) | 0.039 | ||||
| LUSS | 1.08 (1.00–1.17) | 0.045 | ||||
| LUSS/ROX | 1.35 (1.04–1.76) | 0.023 | ||||
| AIC | 84 | 85 | 84 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nova, A.; Rezoagli, E.; Eronia, N.; Benini, A.; Scognamiglio, A.; Foti, G.; Bellani, G. Prognostic Performance of Bedside Lung Ultrasound Score (LUSS) and ROX Index in Hypoxemic Respiratory Failure Due to COVID-19. Diagnostics 2023, 13, 1361. https://doi.org/10.3390/diagnostics13071361
Nova A, Rezoagli E, Eronia N, Benini A, Scognamiglio A, Foti G, Bellani G. Prognostic Performance of Bedside Lung Ultrasound Score (LUSS) and ROX Index in Hypoxemic Respiratory Failure Due to COVID-19. Diagnostics. 2023; 13(7):1361. https://doi.org/10.3390/diagnostics13071361
Chicago/Turabian StyleNova, Alice, Emanuele Rezoagli, Nilde Eronia, Annalisa Benini, Andrea Scognamiglio, Giuseppe Foti, and Giacomo Bellani. 2023. "Prognostic Performance of Bedside Lung Ultrasound Score (LUSS) and ROX Index in Hypoxemic Respiratory Failure Due to COVID-19" Diagnostics 13, no. 7: 1361. https://doi.org/10.3390/diagnostics13071361