
Is Laser Therapy an Adjuvant in the Treatment of Peri-Implant Mucositis? A Randomized Clinical Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Selection of Patients
- -
- Presence of at least one implant on two different hemiarches;
- -
- Implants must be pillars of fixed prosthetic works;
- -
- Presence of bacterial plaque and signs of inflammation of the peri-implant gingival tissue.
- -
- The exclusion criteria were the following:
- -
- Presence of radiographically detectable bone loss after the initial remodeling of the bone;
- -
- Presence of systemic diseases with an impact on the periodontal tissues (diabetes, immunological diseases, acute articular rheumatism, tuberculosis, etc.);
- -
- Pregnancy or breastfeeding;
- -
- Non-surgical peri-implant treatment performed in the last 6 months;
- -
- Antibiotic treatment in the last 6 months;
2.3. The Periodontal Protocol
- -
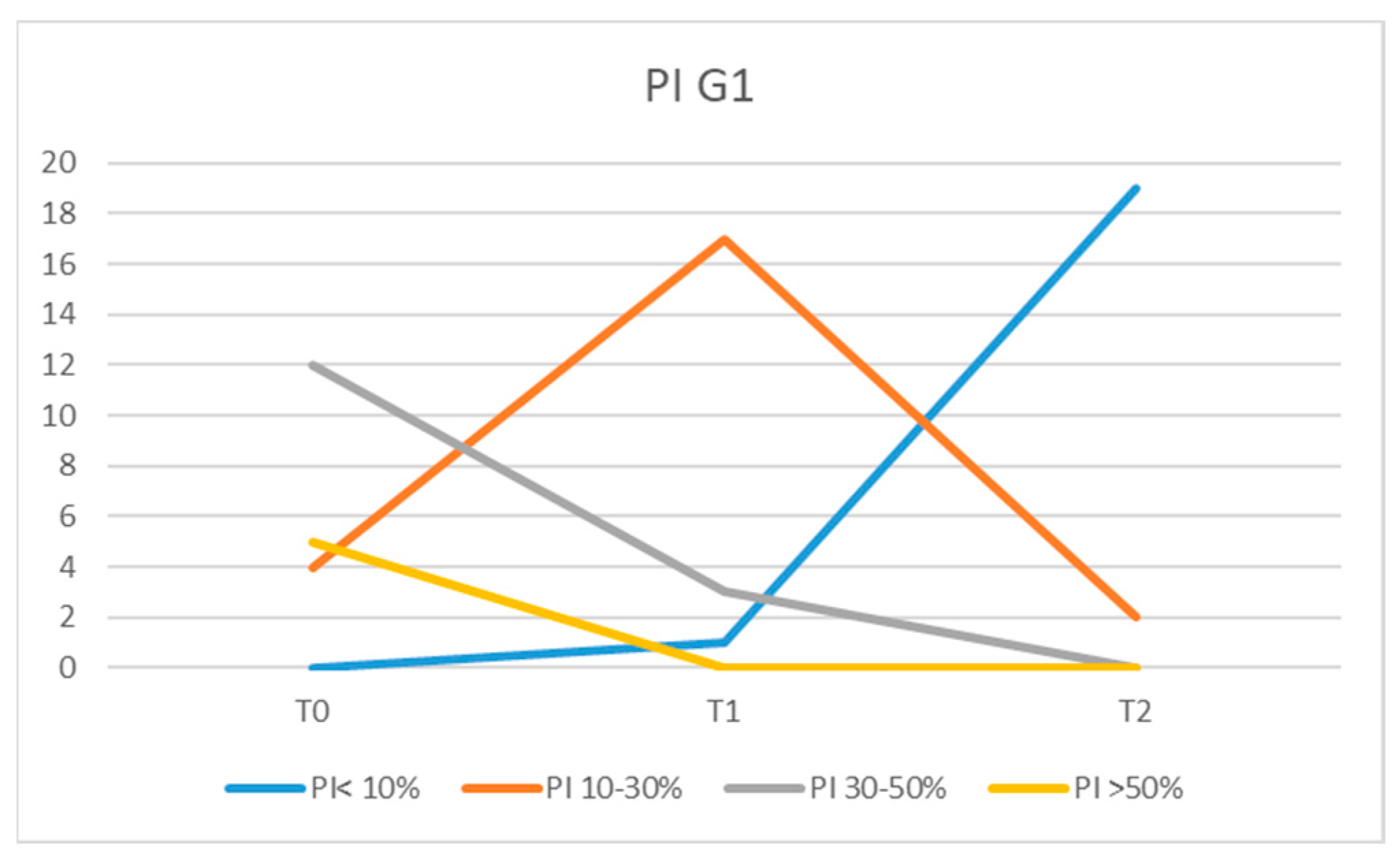
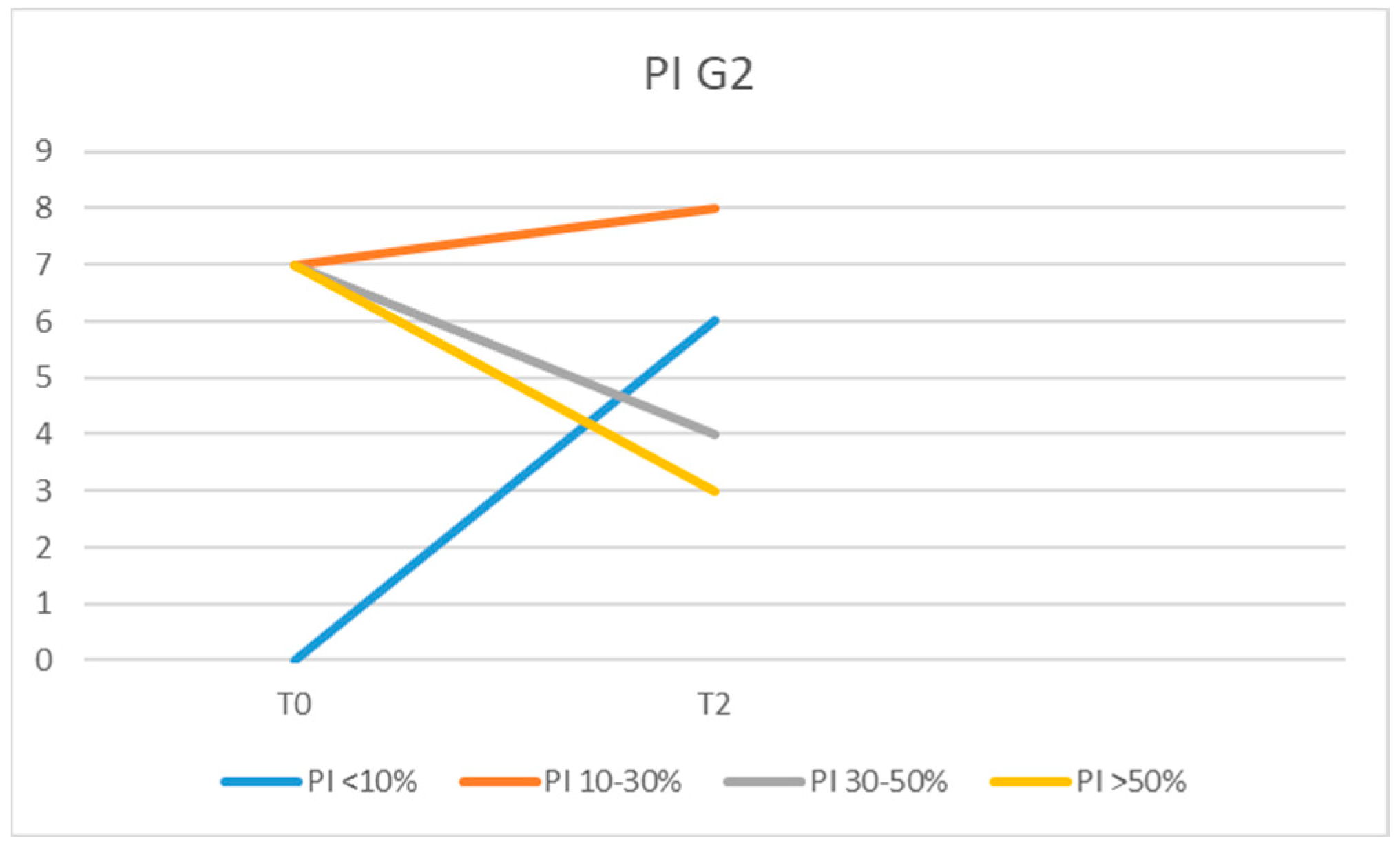
- Plaque index (PI): the presence (+) or absence (−) of bacterial plaque on the buccal, lingual, mesial, and distal surfaces following the application of a plaque disclosing solution. The PI value was calculated by dividing the sum of all surfaces presenting dental plaque by the total number of surfaces examined, multiplied by one hundred;
- -
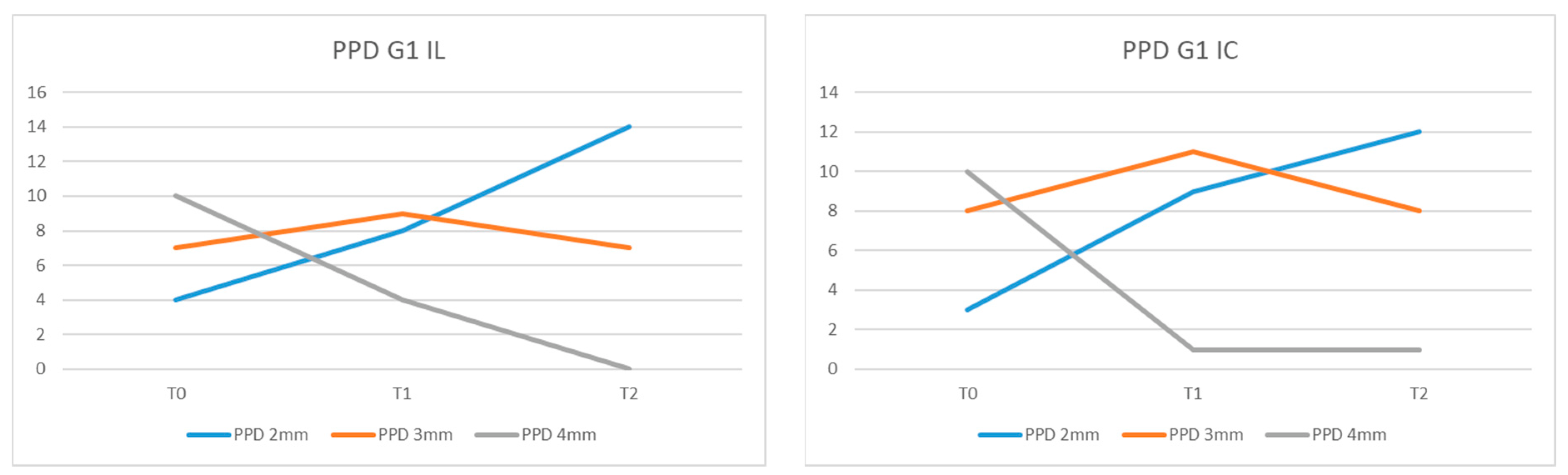
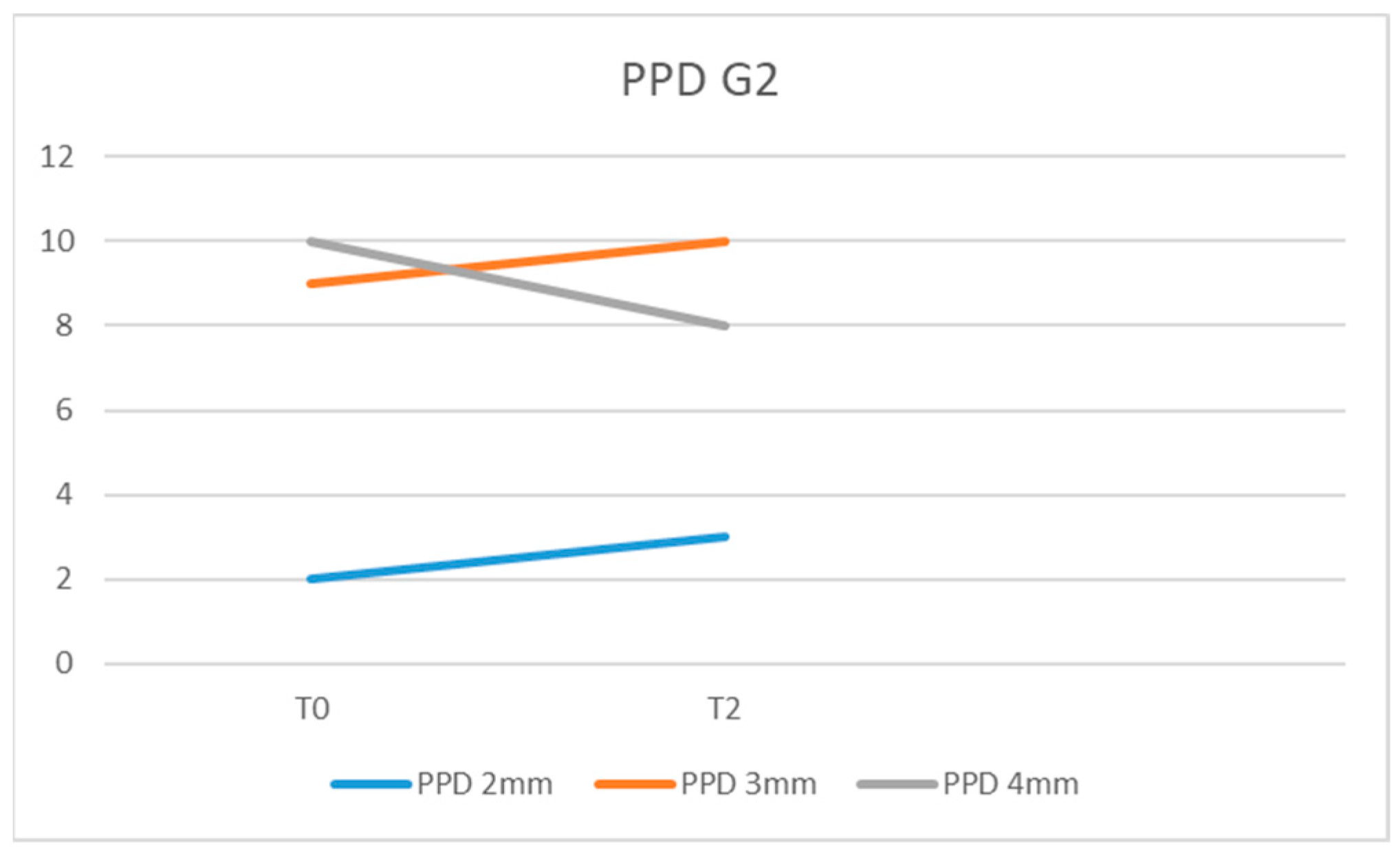
- Probing pocket depth (PPD): the distance from the gingival margin to the apical limit of the peri-implant gingival groove measured in 6 places (mesio-buccal/centro-buccal/disto-buccal/mesio-oral/centro-oral/disto-oral) with a constant force;
- -
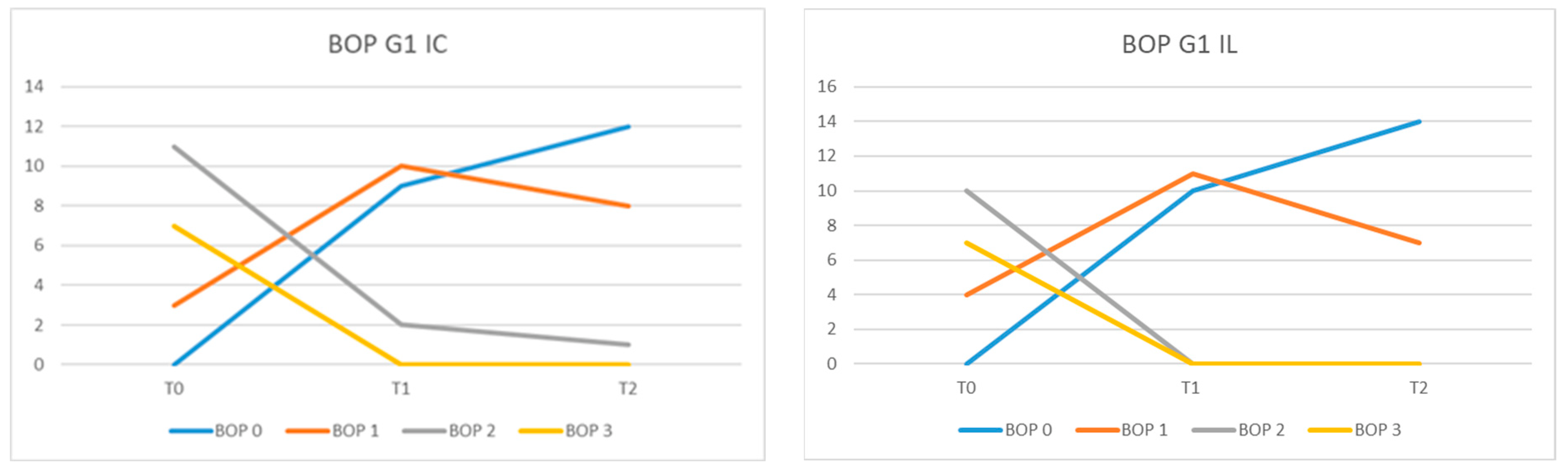
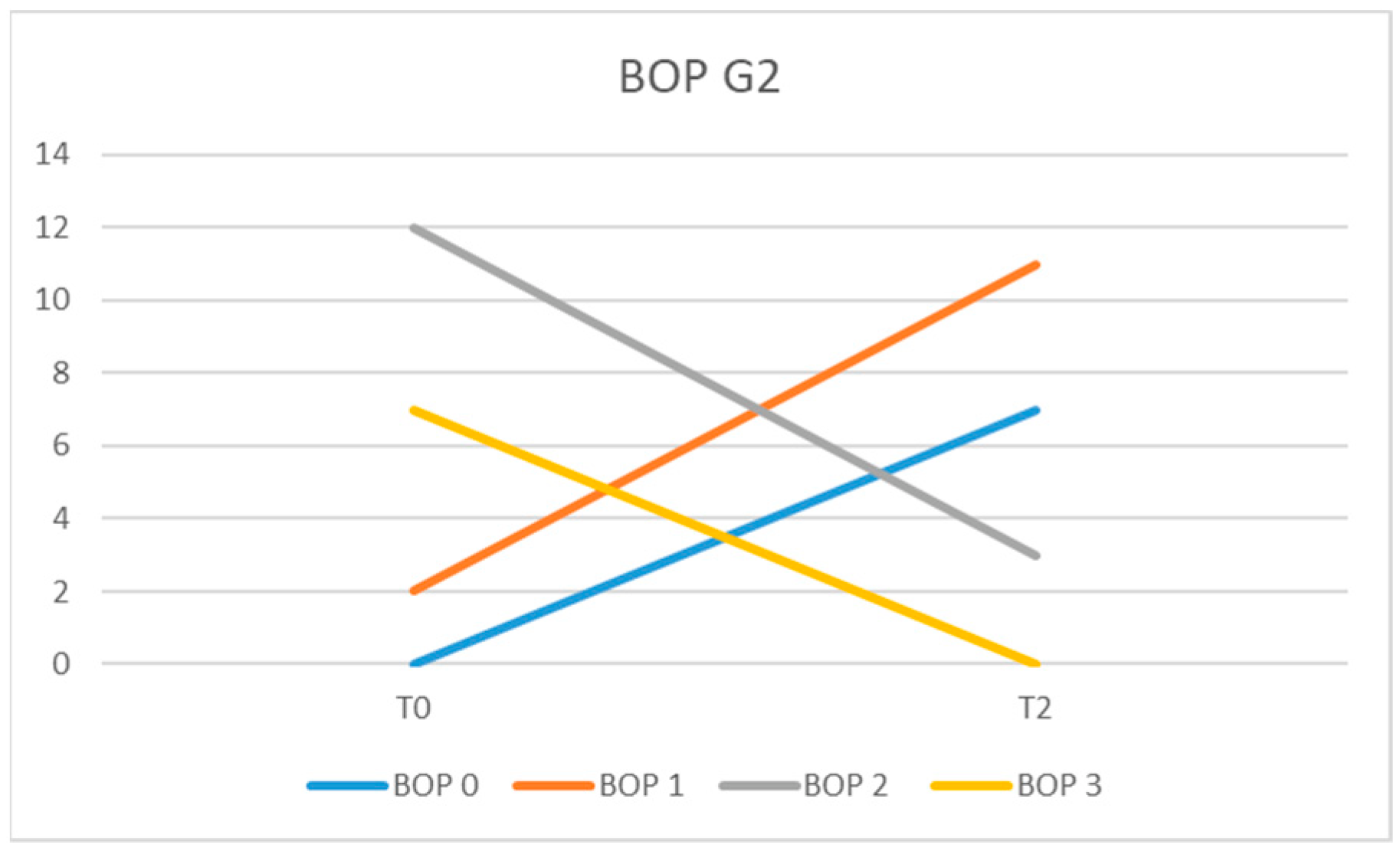
- Bleeding on probing (BOP): by giving the following scores: 1, minimal punctate bleeding; 2, linear bleeding or in drops; 3, spontaneous or profuse bleeding, with or without suppuration [38].
- -
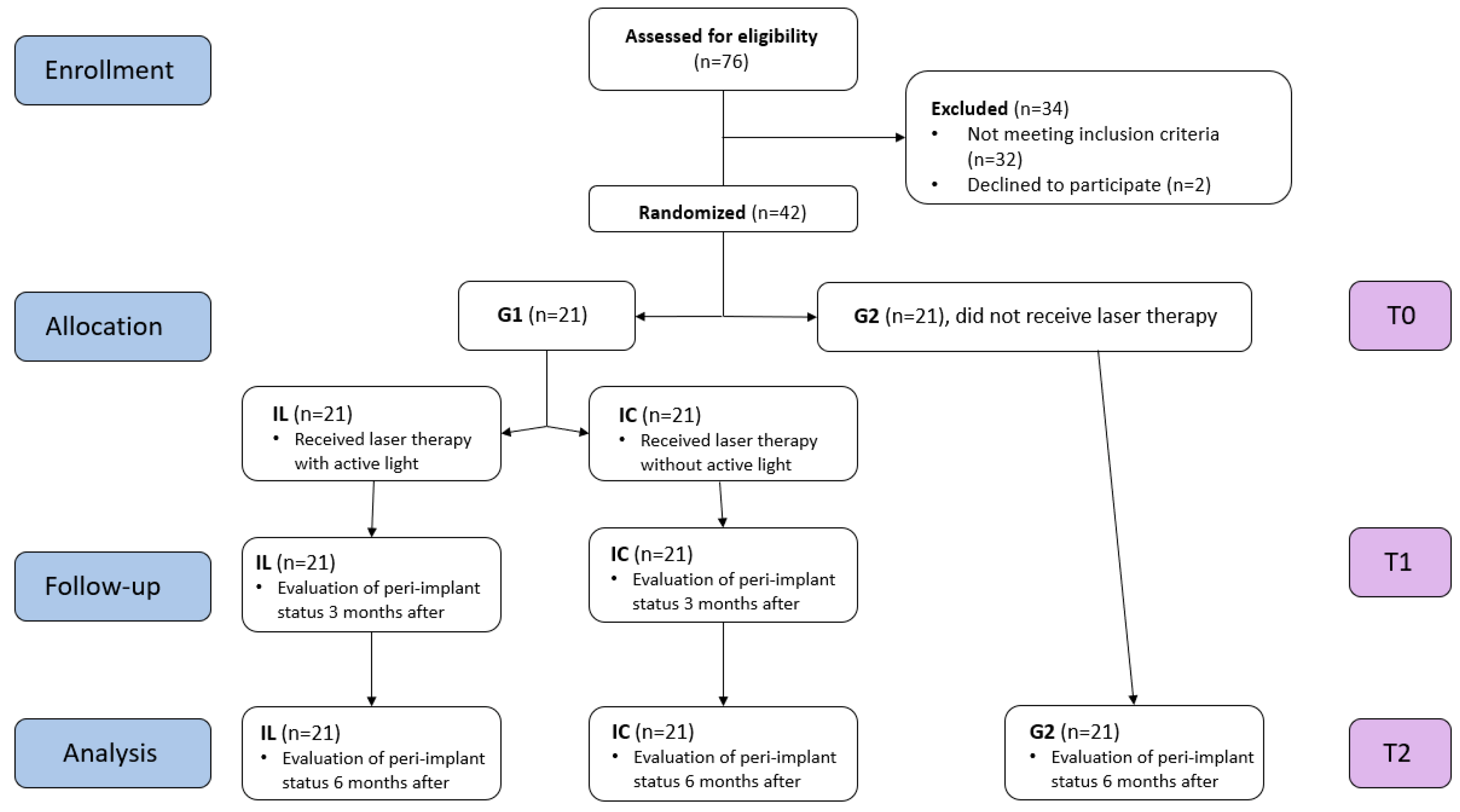
- Group 1: 21 patients who received instructions regarding dental plaque removal and underwent scaling around the implant surface using titanium curettes. Only one out of the two implants each patient had benefited from laser treatment. The peri-implant status was evaluated at the time of the initial examination (T0), three months after (T1), and 6 months after (T2).
- -
- Group 2: 21 patients who received instructions regarding dental plaque removal and underwent scaling around the implant surface using titanium curettes. The peri-implant status was evaluated at the time of the initial examination (T0) and at 6 months (T2).
2.4. The Laser Protocol
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hussain, R.A.; Miloro, M.; Cohen, J.B. An Update on the Treatment of Periimplantitis. Dent. Clin. N. Am. 2021, 65, 43–56. [Google Scholar] [CrossRef] [PubMed]
- Bäumer, A.; Toekan, S.; Saure, D.; Körner, G. Survival and success of implants in a private periodontal practice: A 10 year retrospective study. BMC Oral Health 2020, 20, 92. [Google Scholar] [CrossRef] [PubMed]
- Dalago, H.R.; Schuldt Filho, G.; Rodrigues, M.A.; Renvert, S.; Bianchini, M.A. Risk indicators for peri-implantitis. A cross-sectional study with 916 implants. Clin. Oral Implant. Res. 2017, 28, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Konstantinidis, I.K.; Kotsakis, G.A.; Gerdes, S.; Walter, M.H. Cross-sectional study on the prevalence and risk indicators of peri-implant diseases. Eur. J. Oral Implantol. 2015, 8, 75–88. [Google Scholar] [PubMed]
- Labh, A.K.; Bennis, M.A.; Mani, G. Prevalence of Peri-Implantitis and Peri-Implant Mucositis among Implant Patients: A Dental University Based Study. J. Long Term Eff. Med. Implant. 2021, 31, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Onclin, P.; Slot, W.; Vissink, A.; Raghoebar, G.M.; Meijer, H.J.A. Incidence of peri-implant mucositis and peri-implantitis in patients with a maxillary overdenture: A sub-analysis of two prospective studies with a 10-year follow-up period. Clin. Implant Dent. Relat. Res. 2022, 24, 188–195. [Google Scholar] [CrossRef]
- Romandini, M.; Lima, C.; Pedrinaci, I.; Araoz, A.; Soldini, M.C.; Sanz, M. Prevalence and risk/protective indicators of peri-implant diseases: A university-representative cross-sectional study. Clin. Oral Implant. Res. 2021, 32, 112–122. [Google Scholar] [CrossRef]
- Renvert, S.; Lindahl, C.; Persson, G.R. Occurrence of cases with peri-implant mucositis or peri-implantitis in a 21–26 year follow-up study. J. Clin. Periodontol. 2018, 45, 233–240. [Google Scholar] [CrossRef]
- Schwarz, F.; Becker, K.; Sahm, N.; Horstkemper, T.; Rousi, K.; Becker, J. The prevalence of peri-implant diseases for two-piece implants with an internal tube-in-tube connection: A cross-sectional analysis of 512 implants. Clin. Oral Implant. Res. 2017, 28, 24–28. [Google Scholar] [CrossRef]
- Lee, C.T.; Huang, Y.W.; Zhu, L.; Weltman, R. Prevalences of peri-implantitis and peri-implant mucositis: Systematic review and meta-analysis. J. Dent. 2017, 62, 1–12. [Google Scholar] [CrossRef]
- Testori, T.; Weinstein, T.; Scutellà, F.; Wang, H.L.; Zucchelli, G. Implant placement in the esthetic area: Criteria for positioning single and multiple implants. Periodontol. 2000 2018, 77, 176–196. [Google Scholar] [CrossRef]
- Ahn, D.H.; Kim, H.J.; Joo, J.Y.; Lee, J.Y. Prevalence and risk factors of peri-implant mucositis and peri-implantitis after at least 7 years of loading. J. Periodontal Implant Sci. 2019, 49, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Rameh, S.; Menhall, A.; Younes, R. Key factors influencing short implant success. Oral Maxillofac. Surg. 2020, 24, 263–275. [Google Scholar] [CrossRef]
- Hämmerle, C.H.F.; Tarnow, D. The etiology of hard- and soft-tissue deficiencies at dental implants: A narrative review. J. Periodontol. 2018, 89, S291–S303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S286–S291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45, S1–S8. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Persson, G.R.; Pirih, F.Q.; Camargo, P.M. Peri-implant health, peri-implant mucositis, and peri-implantitis: Case definitions and diagnostic considerations. J. Periodontol. 2018, 89, S304–S312. [Google Scholar] [CrossRef]
- Araujo, M.G.; Lindhe, J. Peri-implant health. J. Clin. Periodontol. 2018, 45, S230–S236. [Google Scholar] [CrossRef] [Green Version]
- Heitz-Mayfield, L.J.A.; Salvi, G.E. Peri-implant mucositis. J. Clin. Periodontol. 2018, 45, S237–S245. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.L. Peri-implantitis. J. Periodontol. 2018, 89, S267–S290. [Google Scholar] [CrossRef]
- Rokaya, D.; Srimaneepong, V.; Wisitrasameewon, W.; Humagain, M.; Thunyakitpisal, P. Peri-implantitis Update: Risk Indicators, Diagnosis, and Treatment. Eur. J. Dent. 2020, 14, 672–682. [Google Scholar] [CrossRef] [PubMed]
- Meyer, S.; Giannopoulou, C.; Courvoisier, D.; Schimmel, M.; Müller, F.; Mombelli, A. Experimental mucositis and experimental gingivitis in persons aged 70 or over. Clinical and biological responses. Clin. Oral Implant. Res. 2017, 28, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A. Maintenance therapy for teeth and implants. Periodontology 2000 2019, 79, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Hirooka, H.; Polyzois, I.; Kelekis-Cholakis, A.; Wang, H.L. Working Group 3. Diagnosis and non-surgical treatment of peri-implant diseases and maintenance care of patients with dental implants—Consensus report of working group 3. Int. Dent. J. 2019, 69, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Bianco, L.L.; Montevecchi, M.; Ostanello, M.; Checchi, V. Recognition and treatment of peri-implant mucositis: Do we have the right perception? A structured review. Dent. Med. Probl. 2021, 58, 545–554. [Google Scholar] [CrossRef]
- Barootchi, S.; Ravidà, A.; Tavelli, L.; Wang, H.L. Nonsurgical treatment for peri-implant mucositis: A systematic review and meta-analysis. Int. J. Oral Implantol. 2020, 13, 123–139. [Google Scholar]
- Wohlfahrt, J.C.; Aass, A.M.; Koldsland, O.C. Treatment of peri-implant mucositis with a chitosan brush-A pilot randomized clinical trial. Int. J. Dent. Hyg. 2019, 17, 170–176. [Google Scholar] [CrossRef]
- Iorio-Siciliano, V.; Blasi, A.; Stratul, S.I.; Ramaglia, L.; Sculean, A.; Salvi, G.E.; Rusu, D. Anti-infective therapy of peri-implant mucositis with adjunctive delivery of a sodium hypochlorite gel: A 6-month randomized triple-blind controlled clinical trial. Clin. Oral Investig. 2020, 24, 1971–1979. [Google Scholar] [CrossRef]
- Hallström, H.; Persson, G.R.; Lindgren, S.; Olofsson, M.; Renvert, S. Systemic antibiotics and debridement of peri-implant mucositis. A randomized clinical trial. J. Clin. Periodontol. 2012, 39, 574–581. [Google Scholar] [CrossRef]
- Peña, M.; Barallat, L.; Vilarrasa, J.; Vicario, M.; Violant, D.; Nart, J. Evaluation of the effect of probiotics in the treatment of peri-implant mucositis: A triple-blind randomized clinical trial. Clin. Oral Investig. 2019, 23, 1673–1683. [Google Scholar] [CrossRef]
- Alzoman, H.; Alojaym, T.G.; Chalikkandy, S.N.; Mehmood, A.; Rashed, F.; Divakar, D.D. Comparison of an Herbal- and a 0.12% Chlorhexidine-based Oral Rinse as Adjuncts to Nonsurgical Mechanical Debridement in the Management of Peri-implant Mucositis: A Randomised Controlled Trial. Oral Health Prev. Dent. 2020, 18, 645–651. [Google Scholar]
- Philip, J.; Laine, M.L.; Wismeijer, D. Adjunctive effect of mouthrinse on treatment of peri-implant mucositis using mechanical debridement: A randomized clinical trial. J. Clin. Periodontol. 2020, 47, 883–891. [Google Scholar] [CrossRef] [PubMed]
- Philip, J.; Buijs, M.J.; Pappalardo, V.Y.; Crielaard, W.; Brandt, B.W.; Zaura, E. The microbiome of dental and peri-implant subgingival plaque during peri-implant mucositis therapy: A randomized clinical trial. J. Clin. Periodontol. 2022, 49, 28–38. [Google Scholar] [CrossRef] [PubMed]
- Aimetti, M.; Mariani, G.M.; Ferrarotti, F.; Ercoli, E.; Liu, C.C.; Romano, F. Adjunctive efficacy of diode laser in the treatment of peri-implant mucositis with mechanical therapy: A randomized clinical trial. Clin. Oral Implant. Res. 2019, 30, 429–438. [Google Scholar] [CrossRef]
- Mariani, G.M.; Ercoli, E.; Guzzi, N.; Bongiovanni, L.; Bianco, L.; Romano, F.; Aimetti, M. One-year clinical outcomes following non-surgical treatment of peri-implant mucositis with adjunctive diode laser application. Minerva Stomatol. 2020, 69, 269–277. [Google Scholar] [CrossRef]
- Lin, G.H.; Suárez López Del Amo, F.; Wang, H.L. Laser therapy for treatment of peri-implant mucositis and peri-implantitis: An American Academy of Periodontology best evidence review. J. Periodontol. 2018, 89, 766–782. [Google Scholar]
- Tenore, G.; Montori, A.; Mohsen, A.; Mattarelli, G.; Palaia, G.; Romeo, U. Evaluation of adjunctive efficacy of diode laser in the treatment of peri-implant mucositis: A randomized clinical trial. Lasers Med. Sci. 2020, 35, 1411–1417. [Google Scholar] [CrossRef] [PubMed]
- Dukka, H.; Saleh, M.H.A.; Ravidà, A.; Greenwell, H.; Wang, H.L. Is bleeding on probing a reliable clinical indicator of peri-implant diseases? J. Periodontol. 2021, 92, 1669–1674. [Google Scholar] [CrossRef]
- Greenstein, G.; Eskow, R. High Prevalence Rates of Peri-implant mucositis and Peri-implantitis Post Dental Implantations Dictate Need for Continuous Peri-implant Maintenance. Compend. Contin. Educ. Dent. 2022, 43, 206–213. [Google Scholar]
- Monje, A.; Wang, H.L.; Nart, J. Association of preventive maintenance therapy compliance and peri-implant diseases: A cross-sectional study. J. Periodontol. 2017, 88, 1030–1041. [Google Scholar] [CrossRef]
- Rokn, A.; Aslroosta, H.; Akbari, S.; Najafi, H.; Zayeri, F.; Hashemi, K. Prevalence of peri-implantitis in patients not participating in well-designed supportive periodontal treatments: A cross-sectional study. Clin. Oral Implant. Res. 2017, 28, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Al Rifaiy, M.Q.; Qutub, O.A.; Alasqah, M.N.; Al-Sowygh, Z.H.; Mokeem, S.A.; Alrahlah, A. Effectiveness of adjunctive antimicrobial photodynamic therapy in reducing peri-implant inflammatory response in individuals vaping electronic cigarettes: A randomized controlled clinical trial. Photodiagnosis Photodyn. Ther. 2018, 22, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Lerario, F.; Roncati, M.; Gariffo, A.; Attorresi, E.; Lucchese, A.; Galanakis, A.; Palaia, G.; Romeo, U. Non-surgical periodontal treatment of peri-implant diseases with the adjunctive use of diode laser: Preliminary clinical study. Lasers Med. Sci. 2016, 31, 1–6. [Google Scholar] [CrossRef]
- Mettraux, G.R.; Sculean, A.; Bürgin, W.B.; Salvi, G.E. Two-year clinical outcomes following non-surgical mechanical therapy of peri-implantitis with adjunctive diode laser application. Clin. Oral Implant. Res. 2016, 27, 845–849. [Google Scholar] [CrossRef]
- Sánchez-Martos, R.; Samman, A.; Bouazza-Juanes, K.; Díaz-Fernández, J.M.; Arias-Herrera, S. Clinical effect of diode laser on peri-implant tissues during non-surgical peri-implant mucositis therapy: Randomized controlled clinical study. J. Clin. Exp. Dent. 2020, 12, e13–e21. [Google Scholar] [CrossRef]
- Arisan, V.; Karabuda, Z.C.; Arici, S.V.; Topçuoğlu, N.; Külekçi, G. A randomized clinical trial of an adjunct diode laser application for the nonsurgical treatment of peri-implantitis. Photomed. Laser Surg. 2015, 33, 547–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atieh, M.A.; Fadhul, I.; Shah, M.; Hannawi, H.; Alsabeeha, N.H.M. Diode Laser as an Adjunctive Treatment for Peri-implant Mucositis: A Systematic Review and Meta-analysis. Int. Dent. J. 2022, 72, 735–745. [Google Scholar] [CrossRef] [PubMed]
- Nicolae, V.D.; Chiscop, I.; Cioranu, V.S.I.; Mârțu, M.-A.; Luchian, A.I.; Mârțu, S.; Solomon, S.M. The use of photoactivated blue-O toluidine for periimplantitis treatment in patients with periodontal disease. Rev. Chim. 2016, 66, 2121–2123. [Google Scholar]
- Zhao, P.; Song, X.; Wang, Q.; Zhang, P.; Nie, L.; Ding, Y.; Wang, Q. Effect of adjunctive diode laser in the non-surgical periodontal treatment in patients with diabetes mellitus: A systematic review and meta-analysis. Lasers Med. Sci. 2021, 36, 939–950. [Google Scholar] [CrossRef]
- Dembowska, E.; Samulak, R.; Jędrzychowska, A.; Dołęgowska, B. Effects of a 980 nm Diode Laser as an Adjunct to Nonsurgical Periodontal Therapy on Periodontal Status and Inflammatory Markers in Patients After Myocardial Infarction: A Randomized Controlled Trial. Photobiomodul. Photomed. Laser Surg. 2022, 40, 532–542. [Google Scholar] [CrossRef]
- Martu, M.-A.; Surlin, P.; Lazar, L.; Maftei, G.A.; Luchian, I.; Gheorghe, D.-N.; Rezus, E.; Toma, V.; Foia, L.-G. Evaluation of Oxidative Stress before and after Using Laser and Photoactivation Therapy as Adjuvant of Non-Surgical Periodontal Treatment in Patients with Rheumatoid Arthritis. Antioxidants 2021, 10, 226. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, S.; Berglundh, T.; Genco, R.; Aass, A.M.; Demirel, K.; Derks, J.; Figuero, E.; Giovannoli, J.L.; Goldstein, M.; Lambert, F.; et al. Primary prevention of peri-implantitis: Managing peri-implant mucositis. J. Clin. Periodontol. 2015, 42, S152–S157. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Index | Group | Moment T0 | Moment T1 | Moment T2 |
|---|---|---|---|---|
| PI (%) | G1 | 41.07 | 19.46 | 5.31 |
| G2 | 42.85 | - | 17.85 | |
| PPD (mm) | G1 IL | 3.28 | 2.80 | 2.33 |
| G1 IC | 3.33 | 2.85 | 2.61 | |
| G2 | 3.38 | - | 3.23 | |
| BOP (score) | G1 IL | 2.14 | 0.52 | 0.33 |
| G1 IC | 2.19 | 0.66 | 0.47 | |
| G2 | 2.23 | - | 0.80 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lazăr, L.; Dakó, T.; Mureșan, I.-É.; Suciu, M.; Maftei, G.-A.; Tatarciuc, M.; Lazăr, A.-P. Is Laser Therapy an Adjuvant in the Treatment of Peri-Implant Mucositis? A Randomized Clinical Trial. Diagnostics 2023, 13, 1192. https://doi.org/10.3390/diagnostics13061192
Lazăr L, Dakó T, Mureșan I-É, Suciu M, Maftei G-A, Tatarciuc M, Lazăr A-P. Is Laser Therapy an Adjuvant in the Treatment of Peri-Implant Mucositis? A Randomized Clinical Trial. Diagnostics. 2023; 13(6):1192. https://doi.org/10.3390/diagnostics13061192
Chicago/Turabian StyleLazăr, Luminița, Timea Dakó, Izabella-Éva Mureșan, Mircea Suciu, George-Alexandru Maftei, Monica Tatarciuc, and Ana-Petra Lazăr. 2023. "Is Laser Therapy an Adjuvant in the Treatment of Peri-Implant Mucositis? A Randomized Clinical Trial" Diagnostics 13, no. 6: 1192. https://doi.org/10.3390/diagnostics13061192