
Association between Sjögren’s Syndrome and Periodontitis: Epidemiological, Fundamental and Clinical Data: A Systematic Review

 ,
, 
 ,
, 
Abstract
:1. Introduction
- Dental caries: xerostomia can increase the risk of dental caries due to the decreased salivary flow, which results in a decreased ability to neutralize acid and wash away bacteria and food particles.
- Oral candidosis: xerostomia can lead to an overgrowth of the fungus Candida, which can cause white, sore patches in the oral cavity, known as oral candidosis.
- Mucositis: Sjögren’s syndrome patients may also have an increased risk of oral mucositis (inflammation and ulceration of the mucous membranes).
- Dysgeusia (distorted sense of taste) and dysphagia (difficulty swallowing).
2. Materials and Methods
2.1. PICO Question
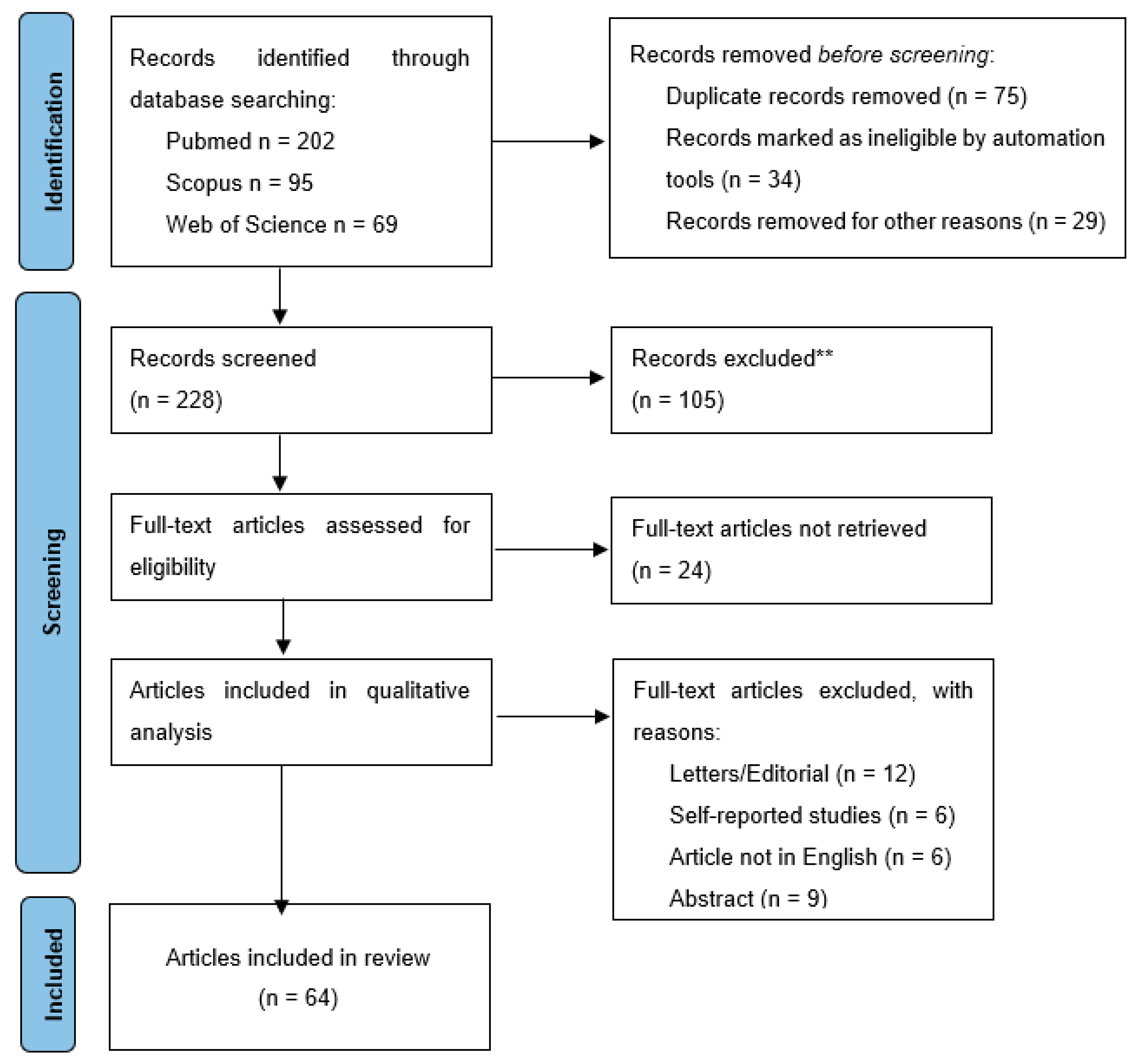
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria for the Selected Studies
2.4. Data Extraction
2.5. Information Structuring and Review Writing
3. Results and Discussion
3.1. Epidemiological Research Data
3.2. Fundamental Research Data
3.3. Clinical Research Data
4. Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AECG | American–European Consensus Group | |
| Anti-SSA | anti-Sjögren’s syndrome-related antigen A autobodies | |
| BAFF | B-cell activating factor | |
| BOP | bleeding on probing index | |
| CAL | Gingival clinical attachment loss | |
| CASP | Caspase | |
| DMFT | Decayed, missing, and filled teeth | |
| EULAR | Sjögren’s syndrome patient reported index | |
| FFA | Free fatty acids | |
| GCF | Gingival crevicular fluid | |
| GI | Gingival index | |
| HLA | Human leukocite antigen | |
| IFN | Interferon | |
| IL | Interleukin | |
| MMP | Matrix-metalloproteinases | |
| NSPT | Non-surgical periodontal therapy | |
| PCNA | Proliferative activity of cell nuclear antigen | |
| PICO | Population Intervention Comparison Outcome | |
| PLQ | Dental plaque index | |
| PPD | Periodontal pocket depth | |
| PRISMA | Preferred Reporting Items for Systematic Review and Meta-Analyses | |
| pSS | Primary Sjögren’s syndrome | |
| RA | Rheumatoid arthritis | |
| SS | Sjögren’s syndrome | |
| sSS | Secondary Sjögren’s syndrome | |
| TGF | Tumor growth factor | |
| TNF | Tumor necrosis factor | |
References
- Kwon, T.H.; Lamster, I.B.; Levin, L. Current concepts in the management of periodontitis. Int. Dent. J. 2021, 71, 462–476. [Google Scholar] [CrossRef] [PubMed]
- Prado, M.M.; Figueiredo, N.; Pimenta, A.D.L.; Miranda, T.S.; Feres, M.; Figueiredo, L.C.; de Almeida, J.; Bueno-Silva, B. Recent updates on microbial biofilms in periodontitis: An analysis of in vitro biofilm models. Periodontitis 2022, 1373, 159–174. [Google Scholar]
- Yucel-Lindberg, T.; Båge, T. Inflammatory mediators in the pathogenesis of periodontitis. Expert Rev. Mol. Med. 2013, 15, e7. [Google Scholar] [CrossRef] [Green Version]
- Herrera, D.; Sanz, M.; Kebschull, M.; Jepsen, S.; Sculean, A.; Berglundh, T.; Papapanou, P.N.; Chapple, I.; Tonetti, M.S.; Kopp, I. Treatment of stage iv periodontitis: The EFP s3 level clinical practice guideline. J. Clin. Periodontol. 2022, 49, 4–71. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.D.; Papapanou, P.N.; Philips, K.H.; Offenbacher, S. Periodontal medicine: 100 years of progress. J. Dent. Res. 2019, 98, 1053–1062. [Google Scholar] [CrossRef]
- Fischer, R.G.; Gomes Filho, I.S.; Cruz, S.S.; Oliveira, V.B.; Lira-Junior, R.; Scannapieco, F.A.; Rego, R.O. What Is the Future of Periodontal Medicine? Braz. Oral Res. 2021, 35, 102. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.C.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 89, S1–S8. [Google Scholar] [CrossRef] [Green Version]
- Loos, B.G. Periodontal medicine: Work in progress! J. Clin. Periodontol. 2016, 43, 470–471. [Google Scholar] [CrossRef]
- Brito-Zerón, P.; Baldini, C.; Bootsma, H.; Bowman, S.J.; Jonsson, R.; Mariette, X.; Sivils, K.; Theander, E.; Tzioufas, A.; Ramos-Casals, M. Sjögren syndrome. Nat. Rev. Dis. Prim. 2016, 2, 16047. [Google Scholar] [CrossRef]
- Baer, A.N.; Walitt, B. Update on Sjögren syndrome and other causes of Sicca in older adults. Rheum. Dis. Clin. N. Am. 2018, 44, 419–436. [Google Scholar] [CrossRef]
- Luppi, F.; Sebastiani, M.; Sverzellati, N.; Cavazza, A.; Salvarani, C.; Manfredi, A. Lung complications of Sjögren syndrome. Eur. Respir. Rev. 2020, 29, 200021. [Google Scholar] [CrossRef] [PubMed]
- Margaretten, M. Neurologic manifestations of primary sjögren syndrome. Rheum. Dis. Clin. N. Am. 2017, 43, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Theander, E.; Jacobsson, L.T.H. Relationship of sjögren’s syndrome to other connective tissue and autoimmune disorders. Rheum. Dis. Clin. N. Am. 2008, 34, 935–947. [Google Scholar] [CrossRef] [PubMed]
- Seror, R.; Nocturne, G.; Mariette, X. Current and future therapies for primary Sjögren syndrome. Nat. Rev. Rheumatol. 2021, 17, 475–486. [Google Scholar] [CrossRef]
- Akpek, E.K.; Bunya, V.Y.; Saldanha, I.J. Sjögren’s syndrome: More than just dry eye. Cornea 2019, 38, 658–661. [Google Scholar] [CrossRef]
- Stefanski, A.-L.; Tomiak, C.; Pleyer, U.; Dietrich, T.; Burmester, G.R.; Dörner, T. The diagnosis and treatment of Sjögren’s syndrome. Dtsch. Ärzteblatt Int. 2017, 114, 354. [Google Scholar] [CrossRef] [Green Version]
- Jonsson, R.; Brokstad, K.A.; Jonsson, M.V.; Delaleu, N.; Skarstein, K. Current concepts on Sjögren’s syndrome—Classification criteria and biomarkers. Eur. J. Oral Sci. 2018, 126, 37–48. [Google Scholar] [CrossRef]
- Weerasinghe, W.S.; Jayasinghe, C. Overlapping rheumatoid arthritis and antisynthetase syndrome with Secondary Sjögren’s syndrome: A case report and review of the literature. J. Med. Case Rep. 2022, 16, 132. [Google Scholar] [CrossRef]
- Popov, Y.; Salomon-Escoto, K. Gastrointestinal and hepatic disease in Sjögren syndrome. Rheum. Dis. Clin. N. Am. 2018, 44, 143–151. [Google Scholar] [CrossRef] [PubMed]
- González, S.; Sung, H.; Sepúlveda, D.; González, M.J.; Molina, C. Oral manifestations and their treatment in sjögren′s syndrome. Oral Dis. 2013, 20, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Choudhry, H.S.; Hosseini, S.; Choudhry, H.S.; Fatahzadeh, M.; Khianey, R.; Dastjerdi, M.H. Updates in diagnostics, treatments, and correlations between oral and ocular manifestations of Sjögren’s syndrome. Ocul. Surf. 2022, 26, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Mathews, S.A.; Kurien, B.T.; Scofield, R.H. Oral manifestations of Sjögren’s syndrome. J. Dent. Res. 2008, 87, 308–318. [Google Scholar] [CrossRef] [PubMed]
- López-Pintor, R.M.; Fernández Castro, M.; Hernández, G. Afectación oral en el paciente con síndrome de Sjögren Primario. Manejo multidisciplinar entre odontólogos Y reumatólogos. Reumatol. Clínica 2015, 11, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Pinto, A. Management of xerostomia and other complications of Sjögren’s syndrome. Oral Maxillofac. Surg. Clin. N. Am. 2014, 26, 63–73. [Google Scholar] [CrossRef]
- Najera, M.P.; Al-Hashimi, I.; Plemons, J.M.; Rivera-Hidalgo, F.; Rees, T.D.; Haghighat, N.; Wright, J.M. Prevalence of periodontal disease in patients with Sjögren’s syndrome. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 1997, 83, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Soto-Rojas, A.E.; Kraus, A. The oral side of Sjögren syndrome. diagnosis and treatment. A Review. Arch. Med. Res. 2002, 33, 95–106. [Google Scholar] [CrossRef]
- Chuang, C.-J.; Hsu, C.-W.; Lu, M.-C.; Koo, M. Increased risk of developing dental diseases in patients with primary Sjögren’s syndrome—A secondary cohort analysis of population-based claims data. PLoS ONE 2020, 15, e0239442. [Google Scholar] [CrossRef]
- Leung, K.C.M.; McMillan, A.S.; Leung, W.K.; Wong, M.C.M.; Lau, C.S.; Mok, T.M.Y. Oral health condition and saliva flow in southern Chinese with Sjögren’s syndrome. Int. Dent. J. 2004, 54, 159–165. [Google Scholar] [CrossRef]
- Schiødt, M.; Christensen, L.B.; Petersen, P.E.; Thorn, J.J. Periodontal disease in primary Sjögren’s syndrome. Oral Dis. 2001, 7, 106–108. [Google Scholar]
- Condé, K.; Guelngar, C.O.; Barry, M.C.; Atakla, H.G.; Mohamed, A.; Cissé, F. Sjögren’s syndrome in children: About 15 cases in Guinea conakry. Eur. J. Med. Res. 2021, 26, 66. [Google Scholar] [CrossRef]
- Olate, S.; Muñoz, D.; Neumann, S.; Pozzer, L.; Cavalieri-Pereira, L.; de Moraes, M. A descriptive study of the oral status in subjects with Sjögren’s syndrome. Int. J. Clin. Exp. Med. 2014, 7, 1140–1144. [Google Scholar] [PubMed]
- Boutsi, E.A.; Paikos, S.; Dafni, U.G.; Moutsopoulos, H.M.; Skopouli, F.N. Dental and periodontal status of Sjögren’s syndrome. J. Clin. Periodontol. 2000, 27, 231–235. [Google Scholar] [CrossRef]
- Lin, C.-Y.; Tseng, C.-F.; Liu, J.-M.; Chuang, H.-C.; Lei, W.-T.; Liu, L.; Yu, Y.-C.; Hsu, R.-J. Association between periodontal disease and subsequent Sjögren’s syndrome: A nationwide population-based Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 771. [Google Scholar] [CrossRef] [Green Version]
- Lu, M.-C.; Jheng, C.-H.; Tsai, T.-Y.; Koo, M.; Lai, N.-S. Increased dental visits in patients prior to diagnosis of primary sjögren’s syndrome: A population-based study in Taiwan. Rheumatol. Int. 2014, 34, 1555–1561. [Google Scholar] [CrossRef] [PubMed]
- Al-Hashimi, I. Oral and periodontal status in Sjögren’s syndrome. Tex. Dent. J. 2001, 118, 932–939. [Google Scholar] [PubMed]
- Melguizo-Rodríguez, L.; Costela-Ruiz, V.J.; Manzano-Moreno, F.J.; Ruiz, C.; Illescas-Montes, R. Salivary biomarkers and their application in the diagnosis and monitoring of the most common oral pathologies. Int. J. Mol. Sci. 2020, 21, 5173. [Google Scholar] [CrossRef]
- Moreno-Quispe, L.A.; Serrano, J.; Virto, L.; Sanz, M.; Ramírez, L.; Fernández-Castro, M.; Hernández, G.; López-Pintor, R.M. Association of salivary inflammatory biomarkers with primary Sjögren’s syndrome. J. Oral Pathol. Med. 2020, 49, 940–947. [Google Scholar] [CrossRef]
- Bunte, K.; Beikler, T. Th17 cells and the il-23/il-17 axis in the pathogenesis of periodontitis and immune-mediated inflammatory diseases. Int. J. Mol. Sci. 2019, 20, 3394. [Google Scholar] [CrossRef] [Green Version]
- Nibali, L.; Fedele, S.; D’Aiuto, F.; Donos, N. Interleukin-6 in oral diseases: A Review. Oral Dis. 2011, 18, 236–243. [Google Scholar] [CrossRef]
- Maciejczyk, M.; Pietrzykowska, A.; Zalewska, A.; Knaś, M.; Daniszewska, I. The significance of matrix metalloproteinases in oral diseases. Adv. Clin. Exp. Med. 2016, 25, 383–390. [Google Scholar] [CrossRef] [Green Version]
- Özçaka, Ö.; Alpöz, E.; Nalbantsoy, A.; Karabulut, G.; Kabasakal, Y. Clinical periodontal status and inflammatory cytokines in primary SJÖGREN syndrome and rheumatoid arthritis. J. Periodontol. 2018, 89, 959–965. [Google Scholar] [CrossRef]
- Marotte, H. The association between periodontal disease and joint destruction in rheumatoid arthritis extends the link between the HLA-DR shared epitope and severity of Bone Destruction. Ann. Rheum. Dis. 2005, 65, 905–909. [Google Scholar] [CrossRef] [Green Version]
- Marton, K.; Boros, I.; Varga, G.; Zelles, T.; Fejerdy, P.; Zeher, M.; Nagy, G. Evaluation of palatal saliva flow rate and oral manifestations in patients with Sjögren’s syndrome. Oral Dis. 2006, 12, 480–486. [Google Scholar] [CrossRef] [PubMed]
- Tervahartiala, T.; Ingman, T.; Sorsa, T.; Ding, Y.; Kangaspunta, P.; Konttinen, Y.T. Proteolytic enzymes as indicators of periodontal health in Gingival crevicular fluid of patients with Sjögren’s syndrome. Eur. J. Oral Sci. 1995, 103, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Sommakia, S.; Baker, O.J. Regulation of inflammation by lipid mediators in oral diseases. Oral Dis. 2016, 23, 576–597. [Google Scholar] [CrossRef]
- Shikama, Y.; Kudo, Y.; Ishimaru, N.; Funaki, M. Potential role of free fatty acids in the pathogenesis of periodontitis and Primary Sjögren’s syndrome. Int. J. Mol. Sci. 2017, 18, 836. [Google Scholar] [CrossRef]
- Pers, J.-O.; d’Arbonneau, F.; Devauchelle-Pensec, V.; Saraux, A.; Pennec, Y.-L.; Youinou, P. Is periodontal disease mediated by salivary BAFF in Sjögren’s syndrome? Arthritis Rheum. 2005, 52, 2411–2414. [Google Scholar] [CrossRef] [PubMed]
- De Luca, F.; Shoenfeld, Y. The microbiome in autoimmune diseases. Clin. Exp. Immunol. 2018, 195, 74–85. [Google Scholar] [CrossRef] [Green Version]
- Lugonja, B.; Yeo, L.; Milward, M.R.; Smith, D.; Dietrich, T.; Chapple, I.L.; Rauz, S.; Williams, G.P.; Barone, F.; de Pablo, P.; et al. Periodontitis prevalence and serum antibody reactivity to periodontal bacteria in primary Sjögren’s syndrome: A pilot study. J. Clin. Periodontol. 2016, 43, 26–33. [Google Scholar] [CrossRef]
- Çelenligil, H.; Eratalay, K.; Kansu, E.; Ebersole, J.L. Periodontal status and serum antibody responses to oral microorganisms in Sjögren’s syndrome. J. Periodontol. 1998, 69, 571–577. [Google Scholar] [CrossRef]
- Çelenligil-Nazlıel, H.; Palalı, A.; Ayhan, A.; Ruacan, Ş. Analysis of in situ proliferative activity in oral gingival epithelium in patients with xerostomia. J. Periodontol. 2003, 74, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Nayar, G.; Gauna, A.; Chukkapalli, S.; Velsko, I.; Kesavalu, L.; Cha, S. Polymicrobial infection alter inflammatory microrna in rat salivary glands during periodontal disease. Anaerobe 2016, 38, 70–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scardina, G.A.; Ruggieri, A.; Messina, P. Periodontal disease and Sjögren Syndrome: A possible correlation? Angiology 2009, 61, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Martins, V.A.O.; Floriano, T.F.; Leon, E.P.; Villamarín, L.E.B.; Deveza, G.B.H.; Aikawa, N.E.; Silva, C.A.A.; Kupa, L.V.K.; Peres, M.P.; Braz-Silva, P.H.; et al. Primary dental care treatment in primary Sjögren’s syndrome: A possible role in improving salivary flow rate. Clin. Exp. Rheumatol. 2022, 40, 2258–2267. [Google Scholar] [CrossRef]
- Singh, M.; Teles, F.; Uzel, N.G.; Papas, A. Characterizing microbiota from Sjögren’s syndrome patients. JDR Clin. Transl. Res. 2020, 6, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Depinoy, T.; Saraux, A.; Pers, J.-O.; Boisramé, S.; Cornec, D.; Marhadour, T.; Guellec, D.; Devauchelle-Pensec, V.; Bressollette, L.; Jousse-Joulin, S. Salivary glands and periodontal changes in a population of Sjögren’s and Sicca syndrome treated by pilocarpine: A pilot study. Rheumatol. Ther. 2020, 8, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.-Y.; Hung, K.-C.; Lin, M.-S.; Ko, C.-H.; Lin, Y.-S.; Chen, T.-H.; Lin, C.-Y.; Chen, Y.-C. The effect of Pilocarpine on dental caries in patients with primary Sjögren’s syndrome: A database prospective cohort study. Arthritis Res. Ther. 2019, 21, 251. [Google Scholar] [CrossRef] [Green Version]
- De Goés Soares, L.; Rocha, R.L.; Bagordakis, E.; Galvão, E.L.; Douglas-de-Oliveira, D.W.; Falci, S.G. Relationship between Sjögren syndrome and periodontal status: A systematic review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Lucchese, A.; Portelli, M.; Marcolina, M.; Nocini, P.F.; Caldara, G.; Bertossi, D.; Lucchese, C.; Tacchino, U.; Manuelli, M. Effect of dental care on the oral health of Sjögrens syndrome patients. J. Biol. Regul. Homeost. Agents 2018, 32 (Suppl. 2), 37–43. [Google Scholar]
- Antoniazzi, R.P.; Miranda, L.A.; Zanatta, F.B.; Islabão, A.G.; Gustafsson, A.; Chiapinotto, G.A.; Oppermann, R.V. Periodontal conditions of individuals with Sjögren’s syndrome. J. Periodontol. 2009, 80, 429–435. [Google Scholar] [CrossRef]
- Márton, K.; Madléna, M.; Bánóczy, J.; Varga, G.; Fejérdy, P.; Sreebny, L.M.; Nagy, G. Unstimulated whole saliva flow rate in relation to sicca symptoms in Hungary. Oral Dis. 2008, 14, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-Y.; Wu, C.-Y.; Chen, M.-H.; Huang, H.-Y.; Chen, Y.-h.; Tsao, Y.-P.; Lai, Y.-L.; Lee, S.-Y. Periodontal conditions in patients with Sjögren’s syndrome: A meta-analysis. J. Dent. Sci. 2021, 16, 1222–1232. [Google Scholar] [CrossRef]
- Le Gall, M.; Cornec, D.; Pers, J.-O.; Saraux, A.; Jousse-Joulin, S.; Cochener, B.; Roguedas-Contios, A.-M.; Devauchelle-Pensec, V.; Boisramé, S. A prospective evaluation of dental and periodontal status in patients with suspected Sjögren’s syndrome. Jt. Bone Spine 2016, 83, 235–236. [Google Scholar] [CrossRef]
- Ergun, S.; Cekici, A.; Topcuoglu, N.; Migliari, D.A.; Kulekci, G.; Tanyeri, H.; Isik, G. Oral status and candida colonization in patients with Sjögren’s syndrome. Med. Oral Patol. Oral Y Cir. Bucal 2010, 15, e310–e315. [Google Scholar] [CrossRef] [PubMed]
- Fox, R.; Howell, F. Oral problems in patients with Sjögren’s syndrome. Scand. J. Rheumatol. 1961, 61, 194–200. [Google Scholar]
- Napeñas, J.J.; Rouleau, T.S. Oral complications of Sjögren’s syndrome. Oral Maxillofac. Surg. Clin. N. Am. 2014, 26, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, A.M.; Bardow, A.; Nauntofte, B. Salivary changes and dental caries as potential oral markers of autoimmune salivary gland dysfunction in primary Sjögren’s syndrome. BMC Clin. Pathol. 2005, 5, 4. [Google Scholar] [CrossRef] [Green Version]
- Rhodus, N.L.; Michalowicz, B.S. Periodontal status and sulcular Candida albicans colonization in patients with primary Sjögren’s Syndrome. Quintessence Int. 2005, 36, 228–233. [Google Scholar] [PubMed]
- Jorkjend, L.; Johansson, A.; Johansson, A.-K.; Bergenholtz, A. Periodontitis, caries and salivary factors in Sjögren’s syndrome patients compared to sex- and age-matched controls. J. Oral Rehabil. 2003, 30, 369–378. [Google Scholar] [CrossRef]
- Kuru, B.; McCullough, M.J.; Yilmaz, S.; Porter, S.R. Clinical and microbiological studies of periodontal disease in Sjögren’s syndrome patients. J. Clin. Periodontol. 2002, 29, 92-91. [Google Scholar] [CrossRef]
- Ravald, N.; List, T. Caries and periodontal conditions in patients with primary Sjögren’s syndrome. Swed. Dent. J. 1998, 22, 97–103. [Google Scholar]
- Pedersen, A.; Andersen Torpet, L.; Reibel, J.; Holmstrup, P.; Nauntofte, B. Oral findings in patients with primary Sjögren’s syndrome and oral lichen planus—A preliminary study on the effects of bovine colostrum-containing oral hygiene products. Clin. Oral Investig. 2002, 6, 11–20. [Google Scholar] [PubMed]
- Pedersen, A.M.; Reibel, J.; Nordgarden, H.; Bergem, H.O.; Jensen, J.L.; Nauntofte, B. Primary sjögren’s syndrome: Salivary gland function and clinical oral findings. Oral Dis. 2008, 5, 128–138. [Google Scholar] [CrossRef] [PubMed]
- Maarse, F.; Jager, D.H.J.; Alterch, S.; Korfage, A.; Forouzanfar, T.; Vissink, A.; Brand, H.S. Sjögren’s syndrome is not a risk factor for periodontal disease: A systematic review. Clin. Exp. Rheumatol. 2019, 37 (Suppl. 118), 225–233. [Google Scholar] [PubMed]
- Tseng, C.C. Periodontal status of patients with Sjögren’s syndrome: A cross-sectional study. J. Formos. Med. Assoc. Taiwan Yi Zhi 1990, 90, 109–111. [Google Scholar]
- Bolstad, A.I.; Skarstein, K. Epidemiology of sjögren’s syndrome—From an oral perspective. Curr. Oral Health Rep. 2016, 3, 328–336. [Google Scholar] [CrossRef] [Green Version]
- Chatzistavrianou, D.; Shahdad, S. Implant Treatment in Patients with Sjögren’s Syndrome: A Review of the Literature and Two Clinical Case Reports. Eur. J. Prosthodont. Restor. Dent. 2016, 24, 40–46. [Google Scholar]
- Guobis, Z.; Pacauskiene, I.; Astramskaite, I. General diseases influence on Peri-Implantitis Development: A Systematic Review. J. Oral Maxillofac. Res. 2016, 7, e5. [Google Scholar] [CrossRef]
- Weinlander, M.; Krennmair, G.; Piehslinger, E. Implant prosthodontic rehabilitation of patients with rheumatic disorders: A case series report. Int. J. Prosthodont. 2010, 23, 22–28. [Google Scholar]
- Albrecht, K.; Callhoff, J.; Westhoff, G.; Dietrich, T.; Dörner, T.; Zink, A. The prevalence of dental implants and related factors in patients with Sjögren Syndrome: Results from a cohort study. J. Rheumatol. 2016, 43, 1380–1385. [Google Scholar] [CrossRef]
- Ambrósio, L.M.; Rovai, E.D.S.; França, B.N.; Balzarini, D.A.; Abreu, I.S.; Lopes, S.B.; Nunes, T.B.; Lourenço, S.V.; Pasoto, S.G.; Saraiva, L.; et al. Effects of periodontal treatment on primary SJȪGREN’s syndrome symptoms. Braz. Oral Res. 2017, 31, 8. [Google Scholar] [CrossRef] [Green Version]
- Gambino, A.; Broccoletti, R.; Cafaro, A.; Cabras, M.; Carcieri, P.; Arduino, P.G. Impact of a sodium carbonate spray combined with professional oral hygiene procedures in patients with Sjögren’s syndrome: An explorative study. Gerodontology 2016, 34, 208–214. [Google Scholar] [CrossRef]
- Jadhav, S.; Jadhav, A.; Thopte, S.; Marathe, S.; Vhathakar, P.; Chivte, P.; Jamkhande, A. Sjögren’s Syndrome: A Case Study. J. Int. Oral Health JIOH 2015, 7, 72–74. [Google Scholar]
- Lins, L.; Paraná, R.; Reis, S.R.; Pereira Falcão, A.F. Primary biliary cirrhosis and primary Sjögren’s syndrome: Insights for the stomatologist. Case Rep. Gastroenterol. 2014, 8, 251–256. [Google Scholar] [CrossRef]
- Johansson, G.; Andersson, G.; Edwardsson, S.; Bjorn, A.-L.; Manthorpe, R.; Attstrom, R. Effects of mouthrinses with linseed extract salinumr without/with chlorhexidine on oral conditions in patients with Sjögren’s syndrome. A double-blind crossover investigation. Gerodontology 2001, 18, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Leung, W.K.; Chu, C.H.; Mok, M.Y.; Yeung, K.W.S.; Ng, S.K.S. Periodontal status of adults with systemic sclerosis: Case-control study. J. Periodontol. 2011, 82, 1140–1145. [Google Scholar] [CrossRef]
- Chen, H.-H.; Huang, N.; Chen, Y.-M.; Chen, T.-J.; Chou, P.; Lee, Y.-L.; Chou, Y.-J.; Lan, J.-L.; Lai, K.-L.; Lin, C.-H.; et al. Association between a history of periodontitis and the risk of rheumatoid arthritis: A nationwide, population-based, Case–Control Study. Ann. Rheum. Dis. 2012, 72, 1206–1211. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Pang, X.; Guan, J.; Liu, X.; Li, X.; Wang, Y.; Chen, Z.; Cheng, B. The Association of Periodontal Diseases and Sjögren’s syndrome: A systematic review and meta-analysis. Front. Med. 2023, 9, 904638. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Database | Keyword Search |
|---|---|
| PUBMED | (“Sjögren, syndrome”[Mesh]) AND “Periodontitis”[Mesh]; (“Sjögren, syndrome”[Mesh]) AND “Periodontal Diseases”[Mesh]; (“Sjögren, syndrome”[Mesh]) AND “Periodontal Status”[Mesh]; (“Sicca, syndrome”[Mesh]) AND “Periodontitis”[Mesh]; (“dry, mouth”[Mesh]) AND “Periodontitis”[Mesh]; |
| Web of Science | TS = (“Sjögren syndrome”) AND TS = (“Periodontal Diseases”); TS = (“Sjögren syndrome”) AND TS = (“Periodontitis”); TS = (“dry mouth”) AND TS = (“Periodontitis”). |
| SCOPUS | ALL(“Sjögren syndrome”) AND ALL(“Periodontal Diseases”); ALL(“Sjögren syndrome”) AND ALL(“Periodontitis”); TITLE-ABS-KEY(“Sjögren syndrome”) AND TITLE-ABS-KEY(“Periodontal Diseases”); TITLE-ABS-KEY(“Sjögren syndrome”) AND TITLE-ABS-KEY(“Periodontitis”). |
| Reference | Type of Study | SS Group (No.) | Findings |
|---|---|---|---|
| Highlighted link between periodontitis and SS | |||
| Al-Hashimi et al., 2001 [35] | Review | / | Dentists and dental hygienists can help identify early signs and symptoms of SS |
| Lin et al., 2019 [33] | Retrospective cohort analysis | 3292 | Patients with periodontitis had a significantly more elevated risk of subsequent SS onset; dental practitioners should be aware of SS risk |
| Lu et al., 2014 [34] | Retrospective cohort analysis | 389 | Dental and periodontal care is essential in early recognition of SS signs and symptoms |
| Chuang et al., 2020 [27] | Retrospective cohort analysis | 709 | Increased risk for periodontal disease onset in SS patients; rheumatologists should be vigilant for oral health of SS patients |
| Najera et al., 1997 [25] | Transversal | 25 | SS patients have a 2.2 times increased risk for developing periodontitis than controls |
| Olate et al., 2014 [31] | Transversal | 35 | Increased prevalence of periodontal inflammation (gingival bleeding) in SS patients |
| Conde et al., 2021 [30] | Retrospective | 15 | Increased prevalence of periodontitis in children with SS |
| No link between periodontitis and SS | |||
| Soto-Rojas et al., 2002 [26] | Review | / | No significant difference in periodontal status of SS patients and controls |
| Leung et al., 2004 [28] | Transversal | 51 | SS patients appear not to be at increased risk for periodontal disease than controls; periodontal parameters cannot be used for SS detection |
| Schiødt et al., 2001 [29] | Transversal | 57 | Periodontal disease has similar prevalence among SS and control participants |
| Boutsi et al., 2000 [32] | Transversal | 24 | No significant difference in periodontal status in SS patients compared to control group |
| Reference | Type of Study | SS Group (No.) | Findings |
|---|---|---|---|
| Highlighted link between periodontitis and SS | |||
| Maciejczyk et al., 2016 [40] | Review | / | MMP-2 and MMP-9 involvement in SS pathogenesis |
| Bunte et al., 2019 [38] | Review | / | IL-17 has important role in the pathogenesis of SS and periodontitis |
| Sommakia et al., 2016 [45] | Review | / | Lipid mediators’ saliva levels could be an additional tool for study of SS and periodontitis etiology, development, and treatment |
| Shikama et al., 2017 [46] | Review | / | Common involvement of free fatty acids in the pathogenesis of periodontitis and SS |
| Nibali et al., 2012 [39] | Review | / | Association between SS and periodontitis, mediated by IL-6, end-stage effector cytokine in the inflammatory reaction |
| De Luca et al., 2019 [48] | Review | / | Increased levels of Streptococcus spp. and Veillonella spp. in SS patients |
| M. Rodriguez et al., 2020 [36] | Review | / | Increased levels of relevant pro-inflammatory mediators in saliva of SS patients |
| Martins et al., 2022 [54] | Prospective | 52 | Primary dental care promoted improvement in salivary flow rates in SS patients |
| Pers et al., 2005 [47] | Transversal | 15 | B-cells could contribute to periodontal complications through up-regulation of BAFF in saliva of SS patients |
| Lungoja et al., 2016 [49] | Transversal | 39 | Increased P. denticola antibody levels in SS patients, identification of potential bacterial triggers |
| Marton et al., 2006 [43] | Case–control | 49 | Oral health status of SS patients may be associated with the general autoimmune process (anti-SSA/SSB antibodies) |
| Moreno et al., 2020 [37] | Case–control | 36 | IL-6 expressed elevated levels in saliva of SS patients; this cytokine could be useful in the diagnosis and follow-up of SS patients |
| Celenligil et al., 1998 [50] | Case–control | 17 | SS may affect bacterial colonization in dental biofilm and contribute to elevation of periodontitis risk |
| Celenligil et al., 2003 [51] | Case–control | 18 | Inflammation causes increased proliferative activity, but this positive effect is downregulated by the reduced saliva flow in SS |
| Scardina et al., 2010 [53] | Case–control | 25 | Evident alterations to the capillaries and typical conformation of the interdental papilla microcirculation in SS patients |
| Singh et al., 2021 [55] | Case–control | 57 | Saliva is a major controlling factor for oral biofilm (impact of V. parvula in SS patients) |
| Nayar et al., 2016 [52] | Experimental | / | The role of micro-RNA in modulating the development of SS offers plausible mechanisms for association with periodontitis |
| No link between periodontitis and SS | |||
| Ozcaka et al., 2018 [41] | Case–control | 44 | No significant difference in periodontal status and GCF levels of TNF-alpha and IFN-gamma between SS patients and controls |
| Tervahartiala et al., 1995 [44] | Comparative | 8 | Periodontal pockets development is not affected by involvement of glandular tissue (lower collagenase and elastase activity in SS) |
| Depinoy et al., 2021 [56] | Prospective cohort | 19 | Treatment with pilocarpine showed no improvement in periodontal parameters in SS patients |
| Hsu et al., 2019 [57] | Prospective cohort | 487 | Pilocarpine may have no protective effect on dental caries and periodontitis in SS patients |
| Reference | Type of Study | SS Group (No.) | Findings |
|---|---|---|---|
| Highlighted link between periodontitis and SS | |||
| Chatzistavrianou et al., 2016 [77] | Review | / | The clinical advantages proved by implant prosthodontics outpace the slightly lower overall implant success rate in SS patients |
| Fox et al., 1986 [65] | Review | / | Patients with SS present specific therapeutic problems: increased oral infections and periodontitis |
| Albrecht et al., 2016 [80] | Observational cohort | 205 | Majority of SS patients were satisfied with dental implants and would recommend them to others |
| Rhodus et al., 2005 [68] | Case–control | 10 | SS patients have significantly more gingival recession and GCF flow than healthy controls |
| Ergun et al., 2010 [64] | Case–control | 37 | SS patients could have a higher risk for periodontitis |
| Gambino et al., 2017 [82] | Randomized control trial | 22 | Gingival status of SS patients improved after non-surgical periodontal therapy, as well as salivary flow |
| Lucchese et al., 2018 [59] | Clinical Trial | 52 | Significant decrease in biofilm deposits and gingival inflammation before and after dental care of SS patients |
| Johansson et al., 2001 [85] | Clinical trial | 22 | Observed positive effects on symptoms in patients with SS after use of chlorhexidine |
| Antoniazzi et al., 2009 [60] | Comparative | 19 | SS negatively affects the periodontal status and increased gingival inflammation in patients with SS |
| Pedersen et al., 2002 [72] | Comparative | 20 | SS predisposes to more systemic disease, increased medication intake, and poor general health, risk factors for periodontitis |
| Le Gall et al., 2016 [63] | Prospective | 31 | More severe periodontal conditions in SS patients than non-SS due to impaired salivary gland function and reduced buffer capacity |
| Marton et al., 2008 [61] | Transversal | / | Increased biofilm deposits and gingival bleeding in a hyposalivation scenario |
| Weinlander et al., 2010 [79] | Retrospective | 5 | Major peri-implant soft tissue alterations in patients with SS |
| Jadhav et al., 2015 [83] | Case report | / | Need for symptomatic treatment in SS patients to prevent periodontal disease |
| Lins et al., 2014 [84] | Case report | / | Appropriate dental care in SS patients may prevent periodontitis, improving the patient’s quality of life |
| No link between periodontitis and SS | |||
| Wu et al., 2021 [62] | Meta-analysis | 198 | Clinical attachment loss and pocket depth were similar in SS patients and healthy controls; need for well-designed observational studies |
| Maarse et al., 2019 [74] | Meta-analysis | / | No evidence of a higher periodontitis risk in patients with SS |
| Bolstad et al., 2016 [76] | Review | / | SS does not seem to contribute to more periodontal disease than in healthy persons |
| Goubis et al., 2016 [78] | Review | / | Implant therapy is advisable and offers acceptable success rates in SS patients |
| Napenas et al., 2014 [66] | Review | / | No increase in incidence and severity of periodontitis in SS patients; no consistent relationship between saliva flow and periodontitis |
| De Goes-Soares et al., 2018 [58] | Review | 518 | No strong evidence that the periodontal status is influenced by SS |
| Ambrosio et al., 2017 [81] | Longitudinal prospective | 28 | SS patients have similar periodontal status to controls at baseline and after non-surgical periodontal therapy |
| Pedersen et al., 2005 [73] | Case–control | 20 | Presence of periodontal disease is not substantially increased in SS patients |
| Ravald et al., 1998 [71] | Case–control | 21 | The periodontal conditions are similar in SS patients to those found in the general population |
| Tseng et al., 1991 [75] | Comparative | 14 | SS has no observable influence on the assessed periodontal indexes |
| Kuru et al., 2002 [70] | Comparative | 18 | Periodontal status does not differ significantly between SS patients and age–gender-matched controls |
| Jorkjund et al., 2003 [69] | Case–control | 33 | SS patients are not specifically at risk of periodontitis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gheorghe, D.N.; Popescu, D.M.; Dinescu, S.C.; Silaghi, M.; Surlin, P.; Ciurea, P.L. Association between Sjögren’s Syndrome and Periodontitis: Epidemiological, Fundamental and Clinical Data: A Systematic Review. Diagnostics 2023, 13, 1401. https://doi.org/10.3390/diagnostics13081401
Gheorghe DN, Popescu DM, Dinescu SC, Silaghi M, Surlin P, Ciurea PL. Association between Sjögren’s Syndrome and Periodontitis: Epidemiological, Fundamental and Clinical Data: A Systematic Review. Diagnostics. 2023; 13(8):1401. https://doi.org/10.3390/diagnostics13081401
Chicago/Turabian StyleGheorghe, Dorin Nicolae, Dora Maria Popescu, Stefan Cristian Dinescu, Margarita Silaghi, Petra Surlin, and Paulina Lucia Ciurea. 2023. "Association between Sjögren’s Syndrome and Periodontitis: Epidemiological, Fundamental and Clinical Data: A Systematic Review" Diagnostics 13, no. 8: 1401. https://doi.org/10.3390/diagnostics13081401