
The Malignant Gastrointestinal Neuroectodermal Tumor (GNET): A Distinct Entity and the Challenging Differential Diagnosis with Mesenchymal, Lymphoid, and Melanic Tumors: A Case Report and Brief Review of the Literature
 ,
, 
Abstract
:1. Introduction
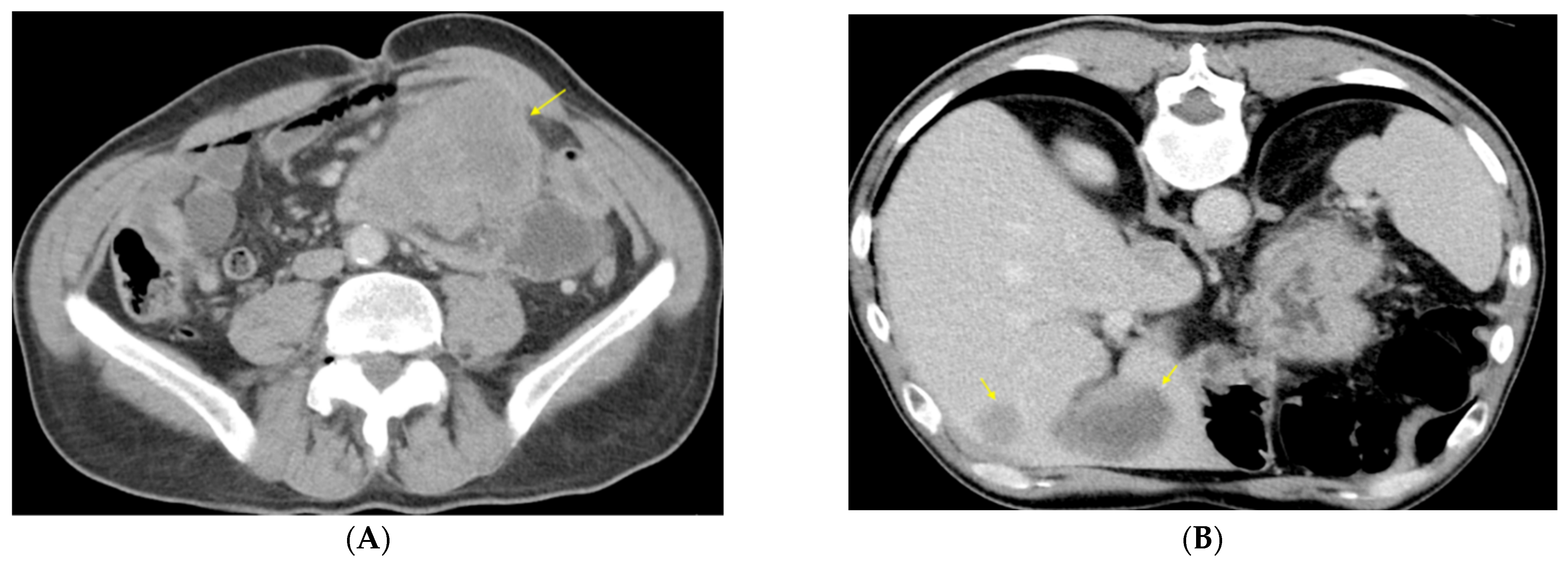
2. Case Presentation
Clinical Findings
3. Results
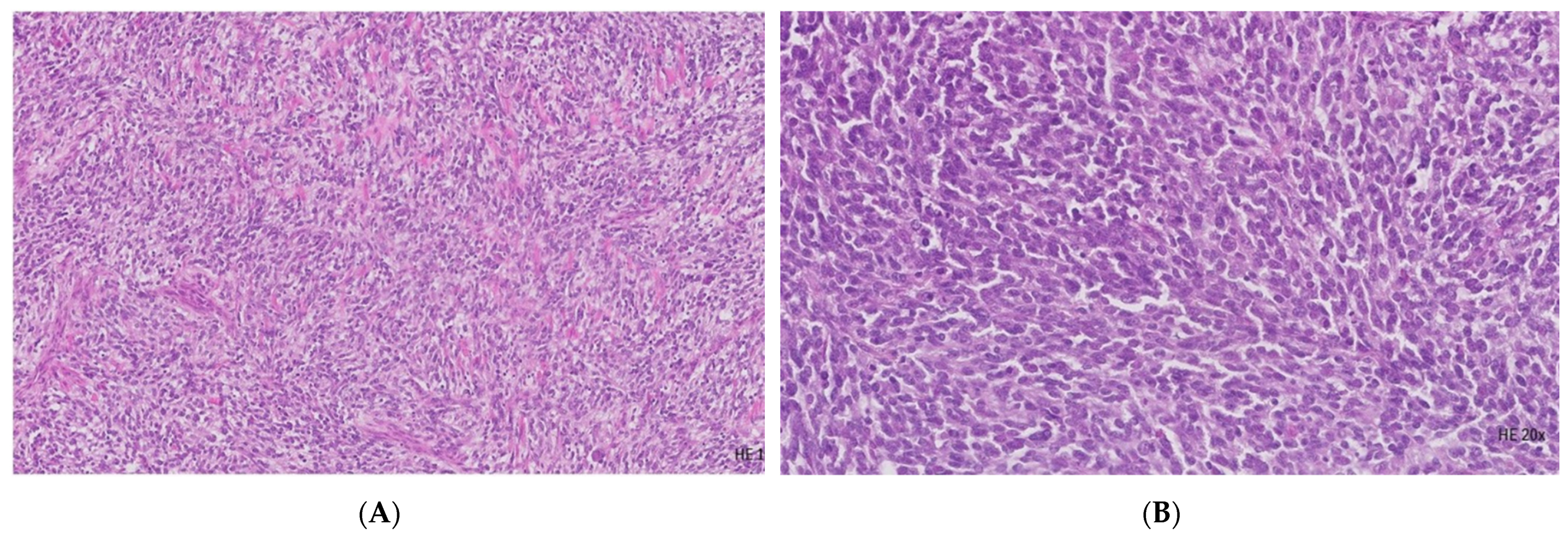
3.1. Histopathological Examination
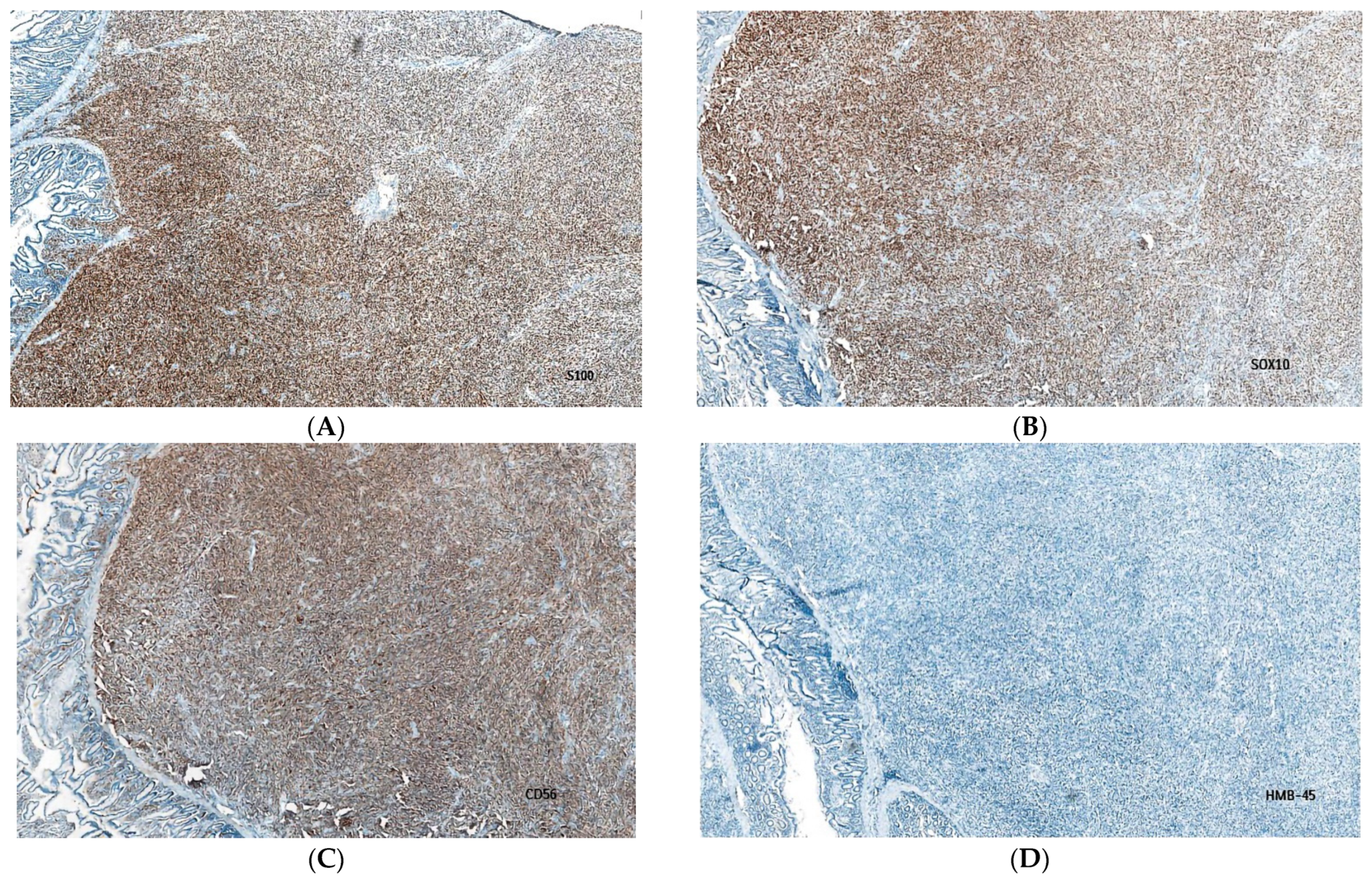
3.2. Immunohistochemical Evaluation
3.3. Final Diagnosis
4. Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Source | Year | Number of Cases | Comment |
|---|---|---|---|
| Fukuda et al. [20] | 2000 | 1 | Case report of a CCS arising in the transverse colon |
| Pauwels et al. [22] | 2002 | 1 | Case report of a CSS with morphological features resembling malignant melanoma. |
| Zambrano et al. [7] | 2003 | 6 | First described as an idiosyncratic type of gastrointestinal neoplasm that shared certain features with clear cell sarcoma of soft parts (melanoma of soft parts) |
| Rosai J [6] | 2005 | 1 | First descriptive evolution of clear cell sarcoma and osteoclast-rich clear cell sarcoma-like tumor of the gastrointestinal tract |
| Covinsky et al. [21] | 2005 | 20 | A report of a subset of GI tumors diagnosed as malignant melanoma by routine histopathologic evaluation represents CCS. |
| Antonescu et al. [16] | 2006 | 3 | A report of a subset of CCS that occurs preferentially in the gastrointestinal tract and shows little or no melanocytic differentiation, with a t(12;22) translocation resulting in the fusion of EWS (EWSR1) with ATF1 |
| Lyle et al. [19] | 2008 | 7 | Molecular evaluation of 7 cases of CSS previously diagnosed as malignant melanoma |
| Stockman et al. [10] | 2012 | 16 | First introduction of term “GNET” |
| Alyousef et al. [4] | 2017 | 1 | - |
| Chang et al. [12] | 2020 | 19 | - |
| Damle et al. [13] | 2021 | 1 | - |
| Kandler et al. [11] | 2022 | 23 | - |
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CCS | clear cell sarcoma |
| CCS-like tumour of GI tract | Clear cell sarcoma-like tumor of the gastrointestinal tract |
| CCSTA | clear cell sarcoma of tendons and aponeuroses |
| CG-A | chromogranin A |
| CD56 | cluster designation 56 |
| CT | computed tomography |
| GNET | Malignant gastrointestinal neuroectodermal tumor |
| GI | Gastrointestinal |
| EMA | epithelial membrane antigen |
| FISH | fluorescence in situ hybridization |
| HPFs | high power fields |
| HMB45 | human melanoma black 45 |
| IHC | Immunohistochemistry |
| LCA | leukocyte common antigen |
| LVI | Lymphovascular invasion |
| Melan A | melanoma antigen |
| MITF | microphthalmia transcription factor |
| NF | Neurofilament |
| OLGC | osteoclast-like giant cells |
| PNI | perineural infiltration |
| SYN | synaptophysin |
| SOX10—SRY | related HMG—box 10 protein |
References
- Green, C.; Spagnolo, D.V.; Robbins, P.D.; Fermoyle, S.; Wong, D.D. Clear cell sarcoma of the gastrointestinal tract and malignant gastrointestinal neuroectodermal tumor: Distinct or related entities? A review. Pathology 2018, 50, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Goldblum, J.R.; Lazar, A.J.; Miettinen, M.; Tsui, W.M.W. Raf Sciot: Chapter 12: Mesenchymal tumours of the digestive system—Tumours of uncertain differentiation. In WHO Classification of Tumours Editorial Board. Digestive System Tumours, 5th ed.; WHO Classification of Tumours Series; International Agency for Research on Cancer: Lyon, France, 2019; Volume 1, Available online: https://publications.iarc.fr/579 (accessed on 28 December 2022).
- Insabato, L.; Guadagno, E.; Natella, V.; Somma, A.; Bihl, M.; Pizzolorusso, A.; Mainenti, P.P.; Apice, G.; Tornillo, L. An unusual association of malignant gastrointestinal neuroectodermal tumor (clear cell sarcoma-like) and Ewing sarcoma. Pathol. Res. Pract. 2015, 211, 688–692. [Google Scholar] [CrossRef] [PubMed]
- Alyousef, M.J.; Alratroot, J.A.; ElSharkawy, T.; Shawarby, M.A.; Al Hamad, M.A.; Hashem, T.M.; Alsayyah, A. Malignant gastrointestinal neuroectodermal tumor: A case report and review of the literature. Diagn. Pathol. 2017, 12, 29. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Thway, K. Clear cell sarcoma-like tumor of the gastrointestinal tract: An evolving entity. Arch. Pathol. Lab. Med. 2015, 139, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Rosai, J. Clear Cell Sarcoma and Osteoclast-Rich Clear Cell Sarcoma-Like Tumor of the Gastrointestinal Tract: One Tumor Type or Two? Melanoma or Sarcoma? Int. J. Surg. Pathol. 2005, 13, 309–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zambrano, E.; Reyes-Mugica, M.; Franchi, A.; Rosai, J. An osteoclast-rich tumor of the gastrointestinal tract with features resembling clear cell sarcoma of soft parts: Reports of 6 cases of a GIST simulator. Int. J. Surg. Pathol. 2003, 11, 75–82. [Google Scholar] [CrossRef]
- Friedrichs, N.; Testi, M.A.; Moiraghi, L.; Modena, P.; Paggen, E.; Plotner, A.; Wiechmann, V.; Mantovani-Löffler, L.; Merkelbach-Bruse, S.; Buettner, R.; et al. Clear cell sarcoma-like tumor with osteoclast-like giant cells in the small bowel. Further evidence for a new tumor entity. Int. J. Surg. Pathol. 2005, 13, 313–318. [Google Scholar] [CrossRef]
- Sandberg, A.A.; Bridge, J.A. Updates on the cytogenetics and molecular genetics of bone and soft tissue tumors: Clear cell sarcoma (malignant melanoma of soft parts). Cancer Genet. Cytogenet. 2001, 130, 1–7. [Google Scholar] [CrossRef]
- Stockman, D.L.; Miettinen, M.; Suster, S.; Spagnolo, D.; Dominguez-Malagon, H.; Hornick, J.L.; Adsay, V.; Chou, P.M.; Amanuel, B.; Vantuinen, P.; et al. Malignant gastrointestinal neuroectodermal tumor: Clinicopathologic, immunohistochemical, ultrastructural, and molecular analysis of 16 cases with a reappraisal of clear cell sarcoma-like tumors of the gastrointestinal tract. Am. J. Surg. Pathol. 2012, 36, 857–868. [Google Scholar] [CrossRef]
- Kandler, T.; Cortez, E.; Clinton, L.; Hemmerich, A.; Ahmed, O.; Wong, R.; Forns, T.; MacNeill, A.J.; Hamilton, T.D.; Khorasani, M.; et al. A Case Series of Metastatic Malignant Gastrointestinal Neuroectodermal Tumors and Comprehensive Genomic Profiling Analysis of 20 Cases. Curr. Oncol. 2022, 29, 20109. [Google Scholar] [CrossRef]
- Chang, B.; Yu, L.; Guo, W.W.; Sheng, W.Q.; Wang, L.; Lao, I.; Huang, D.; Bai, Q.M.; Wang, J. Malignant Gastrointestinal Neuroectodermal Tumor: Clinicopathologic, Immunohistochemical, and Molecular Analysis of 19 Cases. Am. J. Surg. Pathol. 2020, 44, 456–466. [Google Scholar] [CrossRef] [PubMed]
- Damle, A.; Sreenija, Y.; Mathews, N.R.; Nair, K.; Philp, A.; Pavithran, K.; Paulose, R.R. Malignant Gastrointestinal Neuroectodermal Tumour-Case Report with Review of Literature. J. Gastrointest. Cancer 2021, 52, 1125–1130. [Google Scholar] [CrossRef]
- Oye, M.; Kandah, F.; Mikulic, S.; Patel, B.; Villabon, D.C.; Gopinath, A. Malignant gastrointestinal neuroectodermal tumor presenting with recurrent ascites. Curr. Probl. Cancer Case Rep. 2020, 1, 100017. [Google Scholar] [CrossRef]
- Huang, G.; Chen, Q.; Zhong, L.; Chen, H.; Zhang, H.; Liu, X.; Tang, F. Primary malignant gastrointestinal neuroectodermal tumor occurring in the ileum with intra abdominal granulomatous nodules: A case report and review of the literature. Oncol. Lett. 2019, 17, 3899–3909. [Google Scholar] [CrossRef]
- Antonescu, C.R.; Nafa, K.; Segal, N.H.; Dal Cin, P.; Ladanyi, M. EWS-CREB1: A recurrent variant fusion in clear cell sarcoma—Association with gastrointestinal location and absence of melanocytic differentiation. Clin. Cancer Res. 2006, 12, 5356–5362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, W.; Zhang, X.; Li, D.; Chen, J.; Meng, K.; Wang, Y.; Lu, Z.; Zhou, X. Osteoclast-rich tumor of the gastrointestinal tract with features resembling those of clear cell sarcoma of soft parts. Virchows Arch. 2006, 448, 200–203. [Google Scholar] [CrossRef]
- Comin, C.E.; Novelli, L.; Tornaboni, D.; Messerini, L. Clear cell sarcoma of the ileum: Report of a case and review of literature. Virchows Arch. 2007, 451, 839–845. [Google Scholar] [CrossRef]
- Lyle, P.L.; Amato, C.M.; Fitzpatrick, J.E.; Robinson, W.A. Gastrointestinal melanoma or clear cell sarcoma?: Molecular evaluation of 7 cases previously diagnosed as malignant melanoma. Am. J. Surg. Pathol. 2008, 32, 858–866. [Google Scholar] [CrossRef]
- Fukuda, T.; Kakihara, T.; Baba, K.; Yamaki, T.; Yamaguchi, T.; Suzuki, T. Clear cell sarcoma arising in the transverse colon. Pathol. Int. 2000, 50, 412–416. [Google Scholar] [CrossRef]
- Covinsky, M.; Gong, S.; Rajaram, V.; Perry, A.; Pfeifer, J. EWS-ATF1 fusion transcripts in gastrointestinal tumors previously diagnosed as malignant melanoma. Hum. Pathol. 2005, 36, 74–81. [Google Scholar] [CrossRef]
- Pauwels, P.; Debiec-Rychter, M.; Sciot, R.; Vlasveld, T.; Butter, B.D.; Hagemeijer, A.; Hogendoorn, P.C.W. Clear cell sarcoma of the stomach. Histopathology 2002, 41, 526–530. [Google Scholar] [CrossRef] [PubMed]
- West, R.B.; Corless, C.L.; Chen, X.; Rubin, B.P.; Subramanian, S.; Montgomery, K.; Zhu, S.; Ball, C.A.; Nielsen, T.O.; Patel, R. The novel marker, DOG1, is expressed ubiquitously in gastrointestinal stromal tumors irrespective of KIT or PDGFRA mutation status. Am. J. Pathol. 2004, 165, 107–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]




| Antibody | Isotype | Clone | Controls | Manufacturer |
|---|---|---|---|---|
| S100 | IgG2a | 4C4.9 | Melanoma | Ventana Roche |
| SOX10 | IgG | SP267 | Melanoma, Skin Melanocytes | Cell Marque |
| CD56 | - | MRQ-42 | Pancreatic Islet Cells, Pancreatic Endocrine Cells, Neuroblastoma | Cell Marque |
| CD99 | IgG1 | O13 | Pancreatic Islet Cells, Sertoli Cells of the Testis | Ventana Roche |
| Confirm anti-Melanosome | IgG1/K | HMB45 | Melanoma, Skin | Ventana Roche |
| Confirm anti-MART-1/Melan-A | IgG1 | A103 | Melanoma, Normal Skin | Ventana Roche |
| Confirm anti-MITF | IgG1 | C5/D5 | Melanoma | Ventana Roche |
| Confirm anti-Tyrosinase | IgG2a | T311 | Lung, Melanoma | Ventana Roche |
| Confirm anti-Desmin | IgG1/K | DE-R-11 | Intestine | Ventana Roche |
| DOG-1 | Rabbit Ig | SP31 | Gastrointestinal stromal tumor | Cell Marque |
| C-kit (CD117) | - | 9.7 | Gastrointestinal stromal tumor | Ventana Roche |
| Confirm anti-CD34 | IgG1 | QBEnd/10 | Appendix, Placenta, Tonsil | Ventana Roche |
| CD57 | IgM/K | NK-1 | Lymph Node, Tonsil | Cell Marque |
| CD45 (LCA) | IgG1/K | 2B11 & PD7/26 | Lymph Node, Tonsil | Ventana Roche |
| anti-Pan Keratin (AE1/AE3) | IgG1 | AE1/AE3/PCK26 | Intestine, Liver | Ventana Roche |
| Confirm anti-EMA | IgG2a | E29 | Normal Pancreas | Ventana Roche |
| Neurofilament NF | IgG1/K | 2F11 | Brain | Cell Marque |
| Synaptophysin | IgG1 | MRQ-40 | Pancreatic Islet Cells | Cell Marque |
| anti-Chromogranin A (CG-A) | IgG1/K | LK2H10 | Pancreas | Ventana Roche |
| Ki-67 | - | 30-9 | Lymph Node, Tonsil | Ventana Roche |
| Antibody | Immunohistochemistry Evaluation |
|---|---|
| S100 | Diffuse positive cytoplasmic and nuclear reactions |
| SOX10 | High diffuse positive nuclear reaction |
| CD56 | Positive cytoplasmic and cell membrane reactions |
| CD99 | Low positive cell membrane reaction |
| Confirm anti-Melanosome | Absent reaction |
| Confirm anti-MART-1/Melan-A | Absent reaction |
| Confirm anti-MITF | Absent reaction |
| Confirm anti-Tyrosinase | Absent reaction |
| Confirm anti-Desmin | Absent reaction (Positive control) |
| DOG-1 | Absent reaction |
| C-kit (CD117) | Absent reaction (Positive control) |
| Confirm anti-CD34 | Absent reaction (Positive control) |
| CD57 | Absent reaction |
| CD45 (LCA) | Absent reaction (Positive control) |
| anti-Pan Keratin (AE1/AE3) | Absent reaction (Positive control) |
| Confirm anti-EMA | Absent reaction (Positive control) |
| Neurofilament NF | Absent reaction |
| Synaptophysin | Absent reaction (Positive control) |
| anti-Chromogranin A (CG-A) | Absent reaction (Positive control) |
| Ki-67 | A high positive nuclear reaction in about 40% of malignant cells. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boșoteanu, M.; Cristian, M.; Așchie, M.; Baz, R.A.; Zielonka, A.M.; Cozaru, G.C.; Boșoteanu, L.A. The Malignant Gastrointestinal Neuroectodermal Tumor (GNET): A Distinct Entity and the Challenging Differential Diagnosis with Mesenchymal, Lymphoid, and Melanic Tumors: A Case Report and Brief Review of the Literature. Diagnostics 2023, 13, 1131. https://doi.org/10.3390/diagnostics13061131
Boșoteanu M, Cristian M, Așchie M, Baz RA, Zielonka AM, Cozaru GC, Boșoteanu LA. The Malignant Gastrointestinal Neuroectodermal Tumor (GNET): A Distinct Entity and the Challenging Differential Diagnosis with Mesenchymal, Lymphoid, and Melanic Tumors: A Case Report and Brief Review of the Literature. Diagnostics. 2023; 13(6):1131. https://doi.org/10.3390/diagnostics13061131
Chicago/Turabian StyleBoșoteanu, Mădălina, Miruna Cristian, Mariana Așchie, Radu Andrei Baz, Alina Marta Zielonka, Georgeta Camelia Cozaru, and Luana Andreea Boșoteanu. 2023. "The Malignant Gastrointestinal Neuroectodermal Tumor (GNET): A Distinct Entity and the Challenging Differential Diagnosis with Mesenchymal, Lymphoid, and Melanic Tumors: A Case Report and Brief Review of the Literature" Diagnostics 13, no. 6: 1131. https://doi.org/10.3390/diagnostics13061131