
Applications of Artificial Intelligence in Philadelphia-Negative Myeloproliferative Neoplasms
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
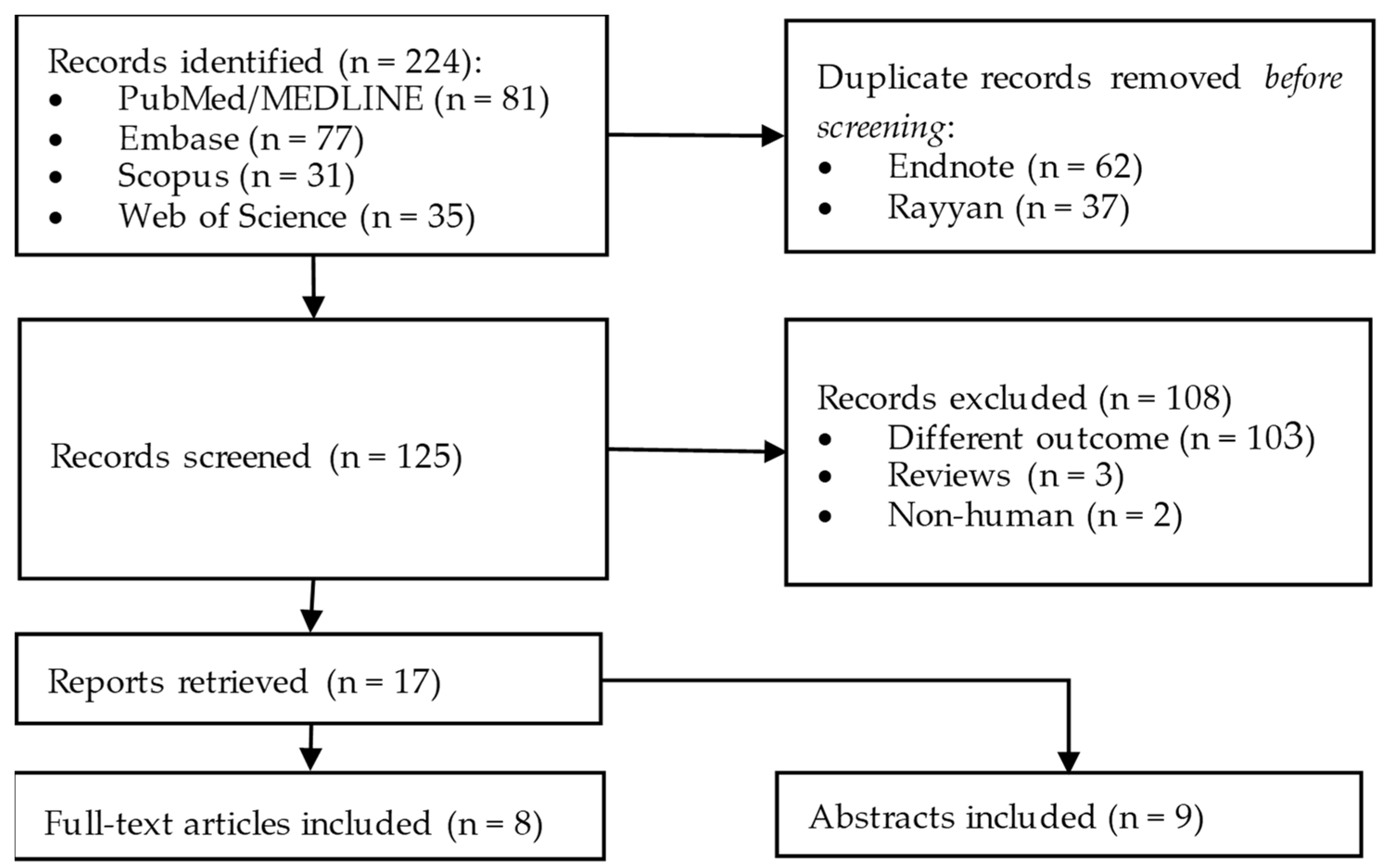
2. Methods
3. Results
3.1. Diagnosis
3.1.1. Diagnosis of MPNs Using Bone Marrow and Peripheral Blood Specimens
3.1.2. Differential Diagnosis of PMF and ET Using Megakaryocytic Lineage
3.1.3. Reduced and Optimized PV Diagnosis Rules
3.1.4. Diagnosis of JAK2 V617F Negative Patients with WHO-Defined ET
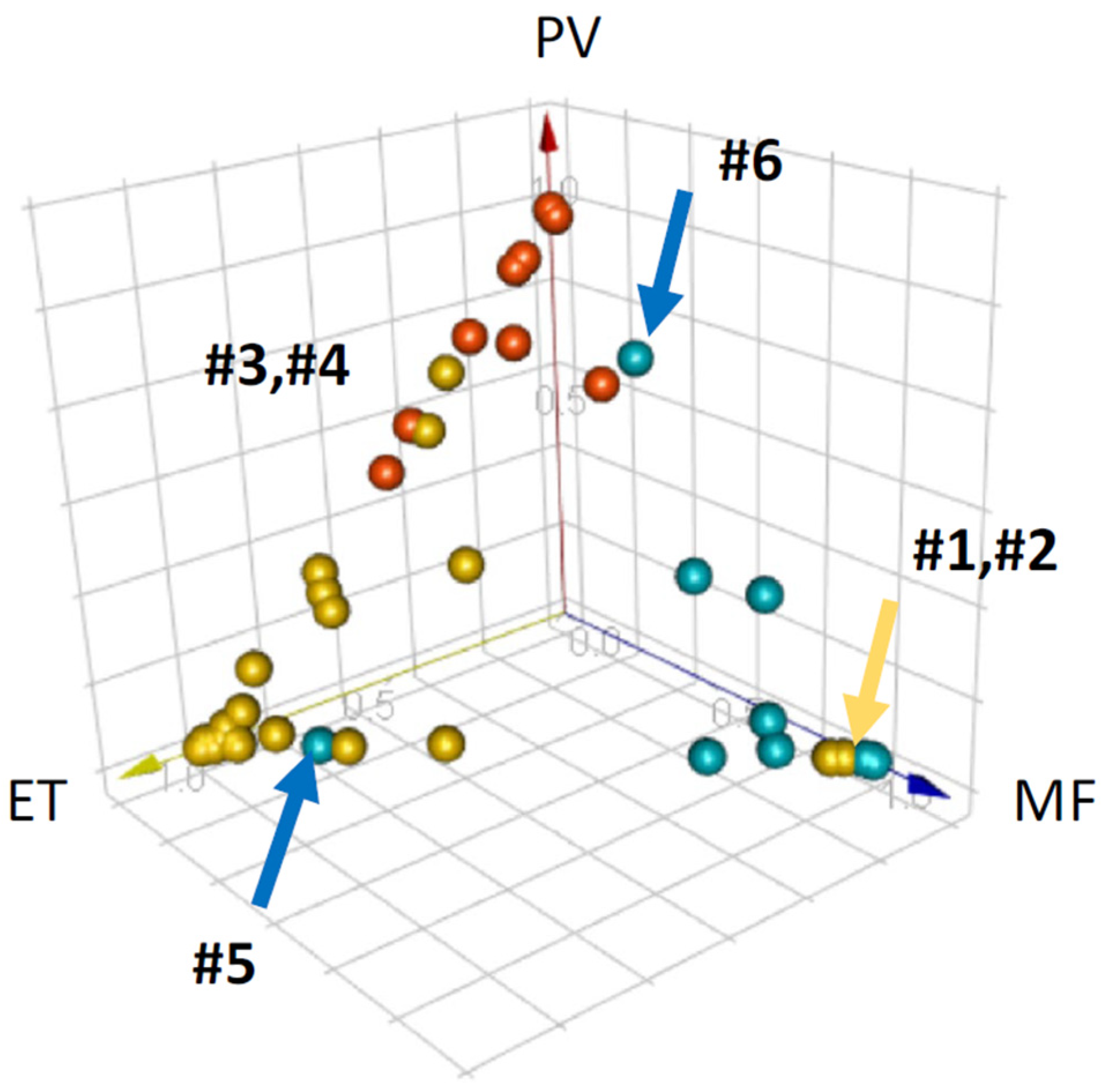
3.1.5. Supervised Classification of MPNs
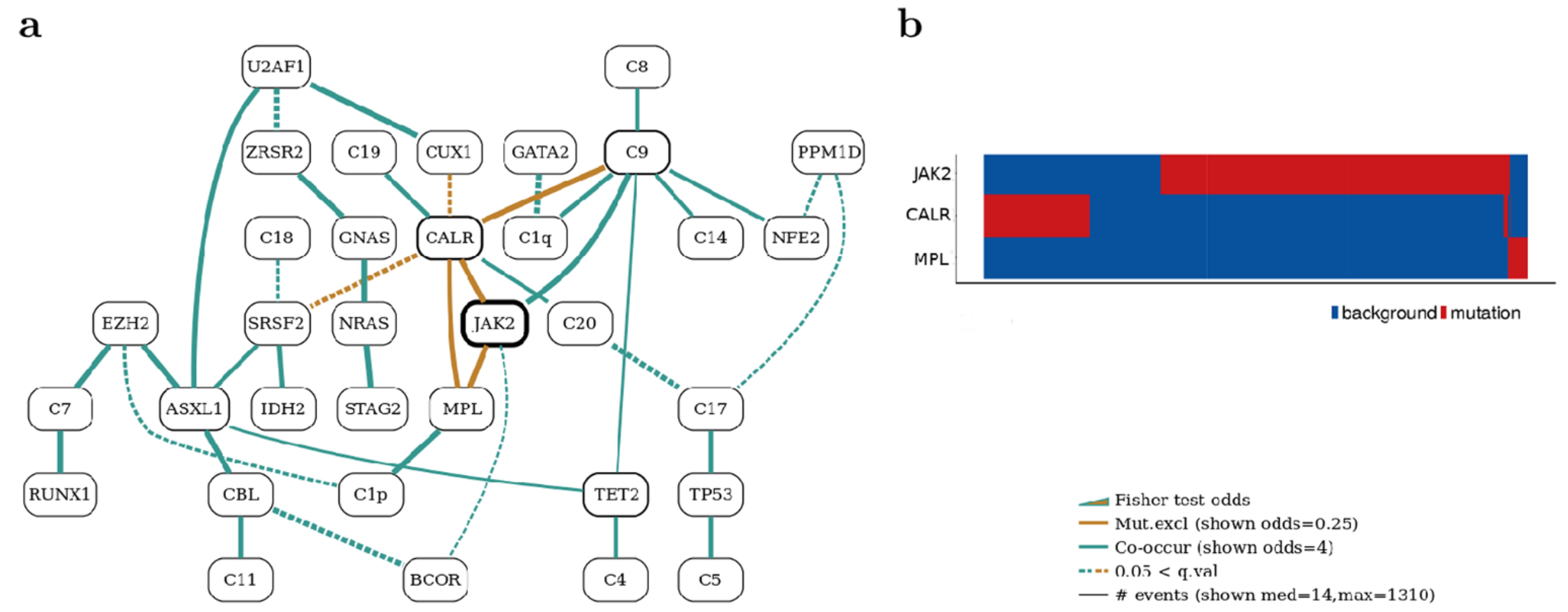
3.1.6. Bayesian Networks Elucidate Complex Genomic Landscapes in MPNs
3.1.7. Distinction of MPNs Using Genetic Markers
3.1.8. Random Forest Classifier for Predicting MPN Subtype Using Genomics
3.2. Prognosis
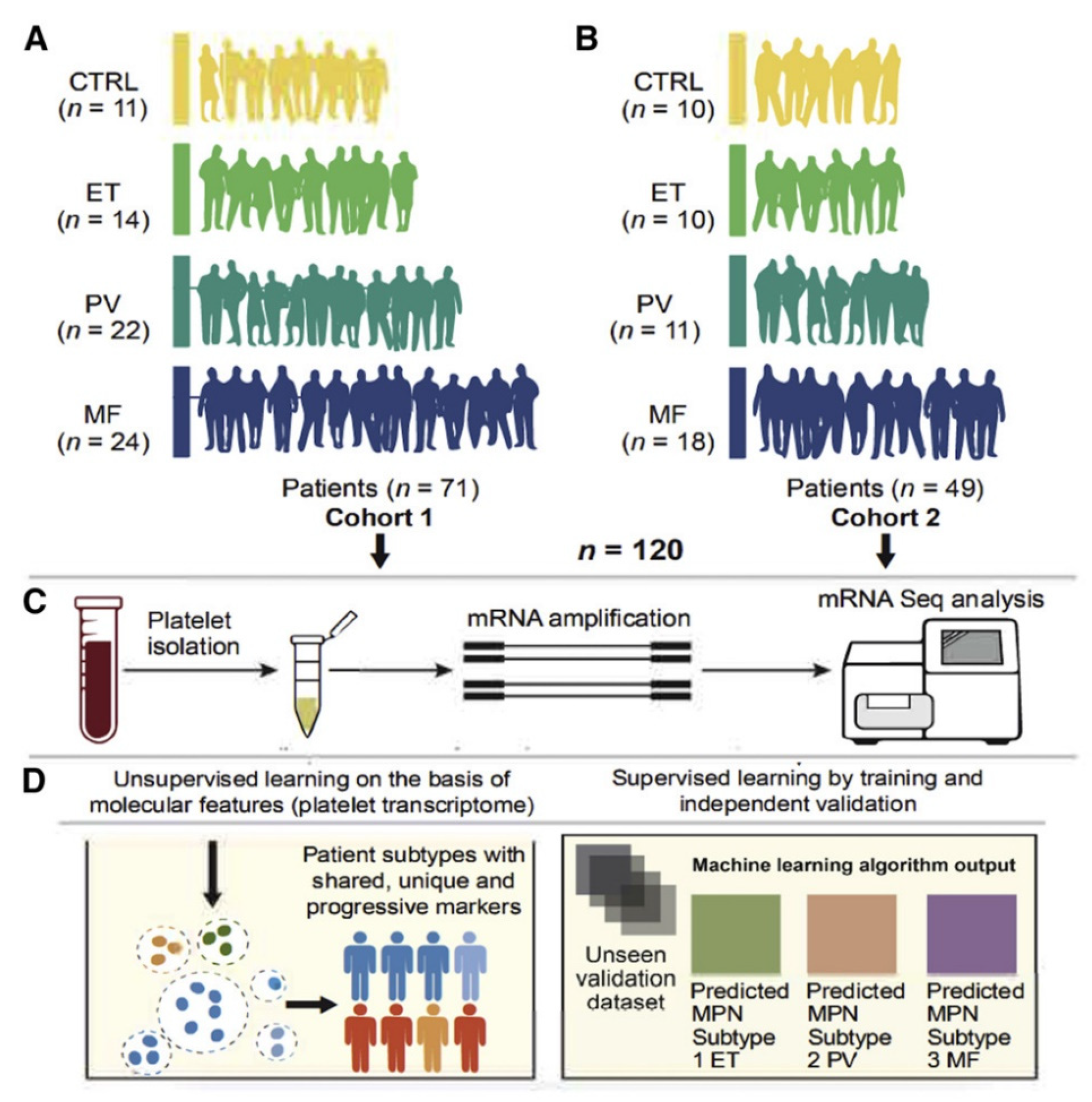
3.2.1. Myelofibrosis Prediction Using Platelet Transcriptome of MPNs
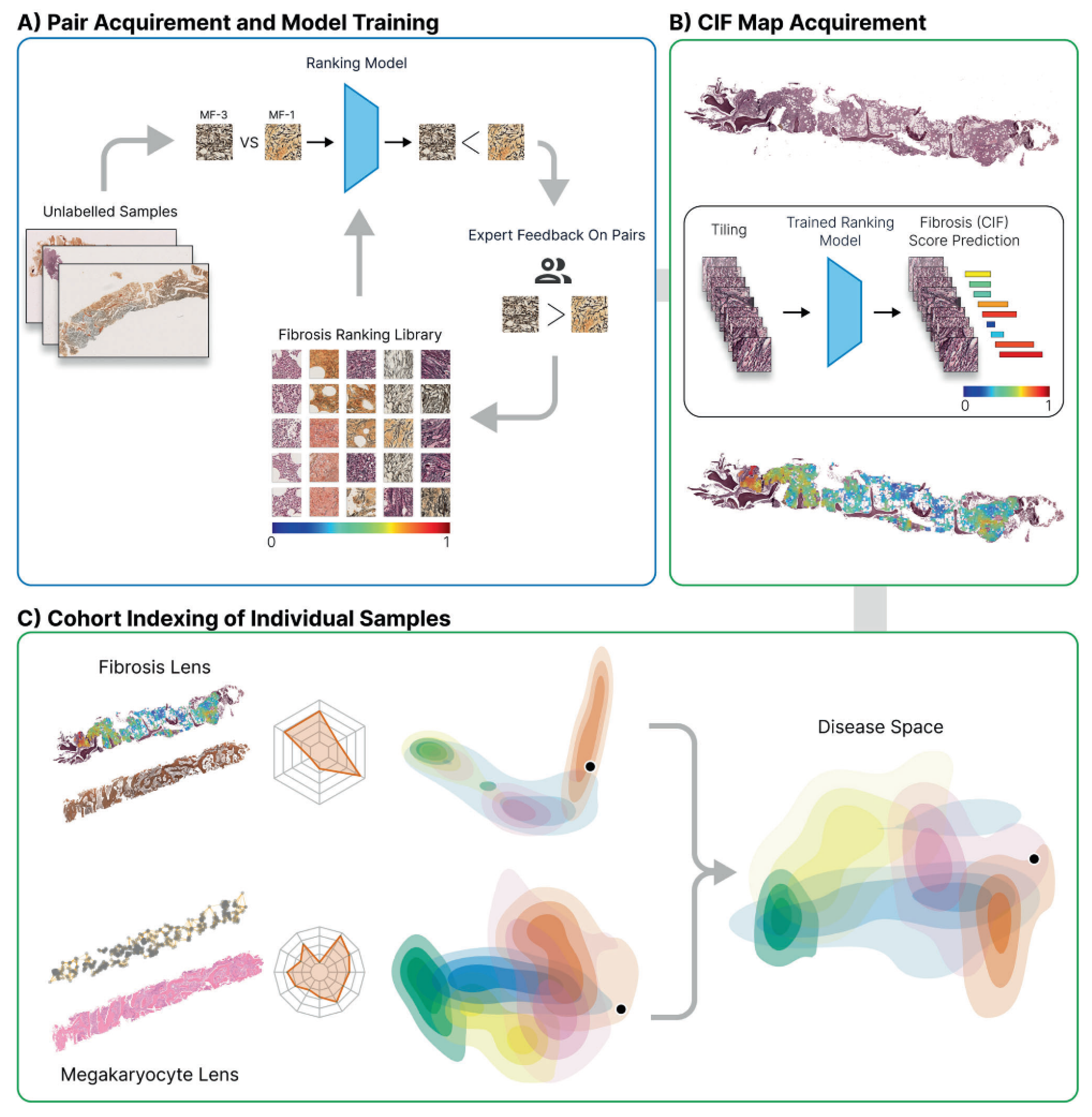
3.2.2. Continuous Index of Fibrosis in MPNs
3.2.3. Predicting Risk of Thrombosis in PV Using Clinicopathologic Features
3.2.4. Predicting Fibrosis in PV Using Accessible Baseline Characteristics
3.2.5. Predicting Hydroxyurea Failure and Thromboembolism in PV
3.2.6. Predicting Thrombosis Risk in Secondary Myelofibrosis
3.2.7. Prediction of Primary Myelofibrosis Using Gene Expression
3.2.8. Prediction of Myelofibrosis Progression in Health Records
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rampal, R.; Al-Shahrour, F.; Abdel-Wahab, O.; Patel, J.P.; Brunel, J.P.; Mermel, C.H.; Bass, A.J.; Pretz, J.; Ahn, J.; Hricik, T.; et al. Integrated genomic analysis illustrates the central role of JAK-STAT pathway activation in myeloproliferative neoplasm pathogenesis. Blood 2014, 123, e123–e133. [Google Scholar] [CrossRef]
- O’Sullivan, J.; Mead, A.J. Heterogeneity in myeloproliferative neoplasms: Causes and consequences. Adv. Biol. Regul. 2019, 71, 55–68. [Google Scholar] [CrossRef]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef] [PubMed]
- Barbui, T.; Thiele, J.; Gisslinger, H.; Kvasnicka, H.M.; Vannucchi, A.M.; Guglielmelli, P.; Orazi, A.; Tefferi, A. The 2016 WHO classification and diagnostic criteria for myeloproliferative neoplasms: Document summary and in-depth discussion. Blood Cancer J. 2018, 8, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, C.N.; McMullin, M.F.; Green, A.R.; Mead, A.J. Equivalence of BCSH and WHO diagnostic criteria for ET. Leukemia 2017, 31, 1660. [Google Scholar] [CrossRef] [Green Version]
- Xie, J.; Chen, X.; Gao, F.; Hou, R.; Tian, T.; Zhang, Y.; Fan, L.; Hu, J.; Zhu, G.; Yang, W.; et al. Two activating mutations of MPL in triple-negative myeloproliferative neoplasms. Cancer Med. 2019, 8, 5254–5263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabagnols, X.; Favale, F.; Pasquier, F.; Messaoudi, K.; Defour, J.P.; Ianotto, J.C.; Marzac, C.; Le Couedic, J.P.; Droin, N.; Chachoua, I.; et al. Presence of atypical thrombopoietin receptor (MPL) mutations in triple-negative essential thrombocythemia patients. Blood 2016, 127, 333–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rumi, E.; Pietra, D.; Pascutto, C.; Guglielmelli, P.; Martinez-Trillos, A.; Casetti, I.; Colomer, D.; Pieri, L.; Pratcorona, M.; Rotunno, G.; et al. Clinical effect of driver mutations of JAK2, CALR, or MPL in primary myelofibrosis. Blood 2014, 124, 1062–1069. [Google Scholar] [CrossRef] [Green Version]
- Verger, E.; Cassinat, B.; Chauveau, A.; Dosquet, C.; Giraudier, S.; Schlageter, M.H.; Ianotto, J.C.; Yassin, M.A.; Al-Dewik, N.; Carillo, S.; et al. Clinical and molecular response to interferon-alpha therapy in essential thrombocythemia patients with CALR mutations. Blood 2015, 126, 2585–2591. [Google Scholar] [CrossRef] [Green Version]
- Yassin, M.A.; Taher, A.; Mathews, V.; Hou, H.A.; Shamsi, T.; Tuglular, T.F.; Xiao, Z.; Kim, S.J.; Depei, W.; Li, J.; et al. MERGE: A Multinational, Multicenter Observational Registry for Myeloproliferative Neoplasms in Asia, including Middle East, Turkey, and Algeria. Cancer Med. 2020, 9, 4512–4526. [Google Scholar] [CrossRef]
- Allahverdi, N.; Yassin, M.; Ibrahim, M. Environmental Factors, Lifestyle Risk Factors, and Host Characteristics Associated With Philadelphia Negative Myeloproliferative Neoplasm: A Systematic Review. Cancer Control 2021, 28, 10732748211046802. [Google Scholar] [CrossRef] [PubMed]
- Hultcrantz, M.; Bjorkholm, M.; Dickman, P.W.; Landgren, O.; Derolf, A.R.; Kristinsson, S.Y.; Andersson, T.M.L. Risk for Arterial and Venous Thrombosis in Patients With Myeloproliferative Neoplasms: A Population-Based Cohort Study. Ann. Intern. Med. 2018, 168, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Marchioli, R.; Finazzi, G.; Landolfi, R.; Kutti, J.; Gisslinger, H.; Patrono, C.; Marilus, R.; Villegas, A.; Tognoni, G.; Barbui, T. Vascular and neoplastic risk in a large cohort of patients with polycythemia vera. J. Clin. Oncol. 2005, 23, 2224–2232. [Google Scholar] [CrossRef] [PubMed]
- Dunbar, A.J.; Rampal, R.K.; Levine, R. Leukemia secondary to myeloproliferative neoplasms. Blood 2020, 136, 61–70. [Google Scholar] [CrossRef]
- Baumeister, J.; Chatain, N.; Sofias, A.M.; Lammers, T.; Koschmieder, S. Progression of Myeloproliferative Neoplasms (MPN): Diagnostic and Therapeutic Perspectives. Cells 2021, 10, 3551. [Google Scholar] [CrossRef]
- Topol, E.J. High-performance medicine: The convergence of human and artificial intelligence. Nat. Med. 2019, 25, 44–56. [Google Scholar] [CrossRef]
- Beam, A.L.; Kohane, I.S. Big Data and Machine Learning in Health Care. JAMA 2018, 319, 1317–1318. [Google Scholar] [CrossRef]
- Jordan, M.I.; Mitchell, T.M. Machine learning: Trends, perspectives, and prospects. Science 2015, 349, 255–260. [Google Scholar] [CrossRef]
- Shamshirband, S.; Fathi, M.; Dehzangi, A.; Chronopoulos, A.T.; Alinejad-Rokny, H. A review on deep learning approaches in healthcare systems: Taxonomies, challenges, and open issues. J. Biomed. Inform. 2021, 113, 103627. [Google Scholar] [CrossRef]
- Rajkomar, A.; Dean, J.; Kohane, I. Machine Learning in Medicine. N. Engl. J. Med. 2019, 380, 1347–1358. [Google Scholar] [CrossRef]
- Khosravi, P.; Kazemi, E.; Imielinski, M.; Elemento, O.; Hajirasouliha, I. Deep Convolutional Neural Networks Enable Discrimination of Heterogeneous Digital Pathology Images. EBioMedicine 2018, 27, 317–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulten, W.; Bandi, P.; Hoven, J.; Loo, R.V.; Lotz, J.; Weiss, N.; Laak, J.V.; Ginneken, B.V.; Hulsbergen-van de Kaa, C.; Litjens, G. Epithelium segmentation using deep learning in H&E-stained prostate specimens with immunohistochemistry as reference standard. Sci. Rep. 2019, 9, 864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, J.M.; Sanders, S.; Carter, M.; Honeyman, D.; Cleo, G.; Auld, Y.; Booth, D.; Condron, P.; Dalais, C.; Bateup, S.; et al. Improving the translation of search strategies using the Polyglot Search Translator: A randomized controlled trial. J. Med. Libr. Assoc. 2020, 108, 195–207. [Google Scholar] [CrossRef] [Green Version]
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote. J. Med. Libr. Assoc. 2016, 104, 240–243. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sirinukunwattana, K.; Aberdeen, A.; Theissen, H.; Sousos, N.; Psaila, B.; Mead, A.J.; Turner, G.D.H.; Rees, G.; Rittscher, J.; Royston, D. Artificial intelligence-based morphological fingerprinting of megakaryocytes: A new tool for assessing disease in MPN patients. Blood Adv. 2020, 4, 3284–3294. [Google Scholar] [CrossRef]
- Kimura, K.; Ai, T.; Horiuchi, Y.; Matsuzaki, A.; Nishibe, K.; Marutani, S.; Saito, K.; Kaniyu, K.; Takehara, I.; Uchihashi, K.; et al. Automated diagnostic support system with deep learning algorithms for distinction of Philadelphia chromosome-negative myeloproliferative neoplasms using peripheral blood specimen. Sci. Rep. 2021, 11, 3367. [Google Scholar] [CrossRef]
- Asaulenko, Z.P.; Polushkina, L.B.; Lepsky, A.I.; Krivolapov, Y.A. Morphological Differential Diagnosis of Primary Myelofibrosis and Essential Thrombocythemia with Computer Cluster Analysis of a Megakaryocytic Lineage in Myeloid Tissue. Biophysics 2020, 65, 676–680. [Google Scholar] [CrossRef]
- Kantardzic, M.; Djulbegovic, B.; Hamdan, H. A data-mining approach to improving Polycythemia Vera diagnosis. Comput. Ind. Eng. 2002, 43, 765–773. [Google Scholar] [CrossRef]
- Shen, Z.; Du, W.; Perkins, C.; Fechter, L.; Natu, V.; Maecker, H.; Rowley, J.; Gotlib, J.; Zehnder, J.; Krishnan, A. Platelet transcriptome identifies progressive markers and potential therapeutic targets in chronic myeloproliferative neoplasms. Cell Rep. Med. 2021, 2, 100425. [Google Scholar] [CrossRef]
- Ryou, H.; Sirinukunwattana, K.; Aberdeen, A.; Grindstaff, G.; Stolz, B.J.; Byrne, H.; Harrington, H.A.; Sousos, N.; Godfrey, A.L.; Harrison, C.N.; et al. Continuous Indexing of Fibrosis (CIF): Improving the assessment and classification of MPN patients. Leukemia 2022, 37, 348–358. [Google Scholar] [CrossRef] [PubMed]
- Angelopoulos, N.; Chatzipli, A.; Nangalia, J.; Maura, F.; Campbell, P.J. Bayesian networks elucidate complex genomic landscapes in cancer. Commun. Biol. 2022, 5, 306. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Zhao, Y.; Wang, D.; Ding, Z.; Li, C.; Wang, B.; Xue, X.; Ma, J.; Deng, Y.; Liu, Q.; et al. Transcriptome research identifies four hub genes related to primary myelofibrosis: A holistic research by weighted gene co-expression network analysis. Aging 2021, 13, 23284–23307. [Google Scholar] [CrossRef] [PubMed]
- Kimura, K.; Tabe, Y.; Ai, T.; Takehara, I.; Fukuda, H.; Takahashi, H.; Naito, T.; Komatsu, N.; Uchihashi, K.; Ohsaka, A. A novel automated image analysis system using deep convolutional neural networks can assist to differentiate MDS and AA. Sci. Rep. 2019, 9, 13385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briggs, C.; Longair, I.; Kumar, P.; Singh, D.; Machin, S.J. Performance evaluation of the Sysmex haematology XN modular system. J. Clin. Pathol. 2012, 65, 1024–1030. [Google Scholar] [CrossRef]
- Salah, H.T.; Muhsen, I.N.; Salama, M.E.; Owaidah, T.; Hashmi, S.K. Machine learning applications in the diagnosis of leukemia: Current trends and future directions. Int. J. Lab. Hematol. 2019, 41, 717–725. [Google Scholar] [CrossRef]
- Wu, Y.Y.; Huang, T.C.; Ye, R.H.; Fang, W.H.; Lai, S.W.; Chang, P.Y.; Liu, W.N.; Kuo, T.Y.; Lee, C.H.; Tsai, W.C.; et al. A Hematologist-Level Deep Learning Algorithm (BMSNet) for Assessing the Morphologies of Single Nuclear Balls in Bone Marrow Smears: Algorithm Development. JMIR Med. Inform. 2020, 8, e15963. [Google Scholar] [CrossRef]
- Wang, Q.; Bi, S.; Sun, M.; Wang, Y.; Wang, D.; Yang, S. Deep learning approach to peripheral leukocyte recognition. PLoS ONE 2019, 14, e0218808. [Google Scholar] [CrossRef] [Green Version]
- Yassin, M.A.; Nehmeh, S.A.; Nashwan, A.J.; Kohla, S.A.; Mohamed, S.F.; Ismail, O.M.; Al Sabbagh, A.; Soliman, D.S.; Szabados, L.; Fayad, H. Assessing Bone Marrow Activity with [18F]FLT PET in Patients with Essential Thrombocythemia and Prefibrotic Myelofibrosis: A Proof of Concept. Technol. Cancer Res. Treat. 2022, 21, 15330338221086396. [Google Scholar] [CrossRef]
- Stuart, B.J.; Viera, A.J. Polycythemia vera. Am. Fam. Physician 2004, 69, 2139–2144. [Google Scholar]
- Djulbegovic, B.; Hadley, T.; Joseph, G. A new algorithm for the diagnosis of polycythemia. Am. Fam. Physician 1991, 44, 113–120. [Google Scholar]
- Djulbegovic, B.; Hozo, I. Computer program for the diagnosis and treatment of polycythemia rubra vera. MD Comput. 1999, 16, 83–89. [Google Scholar]
- Guncar, G.; Kukar, M.; Notar, M.; Brvar, M.; Cernelc, P.; Notar, M.; Notar, M. An application of machine learning to haematological diagnosis. Sci. Rep. 2018, 8, 411. [Google Scholar] [CrossRef] [Green Version]
- Belcic, T.; Cernelc, P.; Sever, M. Artificial intelligence aiding in diagnosis of JAK2 V617F negative patients with who defined essential thrombocythemia. HemaSphere 2019, 3, 998. [Google Scholar] [CrossRef]
- Skov, V.; Burton, M.; Thomassen, M.; Stauffer Larsen, T.; Kjær, L.; Hasselbalch Riley, C.; Jensen, M.K.; Bjerrum, O.W.; Kruse, T.A.; Hasselbalch, H.C. Supervised multi-classifier separation of the Ph-negative myeloproliferative neoplasms. Haematologica 2015, 100, 522–523. [Google Scholar]
- Al-Dewik, N.; Ben-Omran, T.; Zayed, H.; Trujillano, D.; Kishore, S.; Rolfs, A.; Yassin, M.A. Clinical Exome Sequencing unravels new disease-causing mutations in the myeloproliferative neoplasms: A pilot study in patients from the state of Qatar. Gene 2019, 689, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Al-Dewik, N.I.; Cassinat, B.; Kiladjian, J.-J.; Knuth, A.; Yassin, M.A. Targeted Exome Sequencing Identifies Novel Mutations in Familial Myeloproliferative Neoplasms Patients in the State of Qatar. Blood 2014, 124, 5570. [Google Scholar] [CrossRef]
- Meggendorfer, M.; Walter, W.; Haferlach, C.; Kern, W.; Haferlach, T. Deep learning algorithms support distinction of PV, PMF, and ET based on clinical and genetic markers. Blood 2017, 130, 4223. [Google Scholar]
- Jabalameli, M.R.; Ennis, S.; Collins, A.; Cross, N.C.P.; Tapper, W.J. Ensemble Random Forest Classifier for predicting myeloproliferative neoplasms subtype using patient’s genomic profile. Eur. J. Hum. Genet. 2019, 26, 690. [Google Scholar] [CrossRef] [Green Version]
- Spivak, J.L. Myeloproliferative Neoplasms. N. Engl. J. Med. 2017, 377, 895–896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spivak, J.L.; Considine, M.; Williams, D.M.; Talbot, C.C., Jr.; Rogers, O.; Moliterno, A.R.; Jie, C.; Ochs, M.F. Two clinical phenotypes in polycythemia vera. N. Engl. J. Med. 2014, 371, 808–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tibshirani, R. Regression Shrinkage and Selection via the Lasso. J. R. Stat. Society Ser. B 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Moons, K.G.; Kengne, A.P.; Grobbee, D.E.; Royston, P.; Vergouwe, Y.; Altman, D.G.; Woodward, M. Risk prediction models: II. External validation, model updating, and impact assessment. Heart 2012, 98, 691–698. [Google Scholar] [CrossRef]
- Guo, B.B.; Linden, M.D.; Fuller, K.A.; Phillips, M.; Mirzai, B.; Wilson, L.; Chuah, H.; Liang, J.; Howman, R.; Grove, C.S.; et al. Platelets in myeloproliferative neoplasms have a distinct transcript signature in the presence of marrow fibrosis. Br. J. Haematol. 2020, 188, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Rondina, M.T.; Voora, D.; Simon, L.M.; Schwertz, H.; Harper, J.F.; Lee, O.; Bhatlekar, S.C.; Li, Q.; Eustes, A.S.; Montenont, E.; et al. Longitudinal RNA-Seq Analysis of the Repeatability of Gene Expression and Splicing in Human Platelets Identifies a Platelet SELP Splice QTL. Circ. Res. 2020, 126, 501–516. [Google Scholar] [CrossRef]
- Campbell, P.J.; MacLean, C.; Beer, P.A.; Buck, G.; Wheatley, K.; Kiladjian, J.J.; Forsyth, C.; Harrison, C.N.; Green, A.R. Correlation of blood counts with vascular complications in essential thrombocythemia: Analysis of the prospective PT1 cohort. Blood 2012, 120, 1409–1411. [Google Scholar] [CrossRef] [Green Version]
- Abu-Zeinah, G.; Krichevsky, S.; Silver, R.T.; Taylor, E.; Tremblay, D.; Srisuwananukorn, A.; Mascarenhas, J.; Scandura, J. A Novel Machine Learning-Derived Dynamic Scoring System Predicts Risk of Thrombosis in Polycythemia Vera (PV) Patients. Blood 2021, 138, 3619. [Google Scholar] [CrossRef]
- Srisuwananukorn, A.; Percha, B.; Abu-Zeinah, G.; Scandura, J.; Krichevsky, S.; Taylor, E.; Silver, R.T.; Thibaud, S.; Ronner, L.; Podoltsev, N.; et al. Novel Machine Learning Algorithm Predicts Disease Progression in Polycythemia Vera (PV) with Readily-Available Baseline Characteristics. Blood 2021, 138, 2583. [Google Scholar] [CrossRef]
- Verstovsek, S.; De Stefano, V.; Heidel, F.H.; Zuurman, M.; Zaiac, M.; Bigan, E.; Ruhl, M.; Meier, C.; Beffy, M.; Kiladjian, J.J. Machine-learning to predict hydroxyurea (HU) failure and incidence of thromboembolic events (TES) with hu vs ruxolitinib switch therapy in polycythemia vera patients. HemaSphere 2020, 4, 517–518. [Google Scholar] [CrossRef]
- Mora, B.; Kuykendall, A.; Guglielmelli, P.; Rumi, E.; Maffioli, M.; Komrokji, R.; Barraco, D.; Rambaldi, A.; Caramella, M.; Kiladjian, J.J.; et al. MYSEC-prognostic model and previous thrombotic events predict the risk of thrombosis in post polycythemia vera and post essential thrombocythemia myelofibrosis: A study of the MYSEC group. Leukemia 2022, 36, 2453–2460. [Google Scholar] [CrossRef]
- Bejan, C.A.; Sochacki, A.; Zhao, S.; Xu, Y.; Savona, M. Identification of myelofibrosis from electronic health records with novel algorithms and JAKextractor. Cancer Res. 2018, 78, 5303. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Outcome | Advantages | Limitations | Model(s) | Model(s) Uses |
|---|---|---|---|---|---|
| Sirinukunwattana et al. [26] | Automated analysis of megakaryocytes can categorize MPNs and differentiate them from reactive BM samples | Fast assessment of sequential BM samples Comprehensive summary of megakaryocytic cells | Marrow cellularity, lineage maturation, degree of fibrosis, and blast cell estimation are required for MPNs WHO classification | Unsupervised Learning: Principal Component Analysis (PCA) | Reduction of high dimensional data Exploratory data analysis and visualization of complex datasets |
| Kimura et al. [27] | Automated diagnostic support system for MPNs using peripheral blood (PB) specimen | Fast assessment of PB specimens Accurate differentiation of PV, ET, and MF | Single-center study Small number of cases | Deep Learning: Convolutional Neural Network (CNN) | Image recognition and classification Learns features automatically from raw data |
| Asaulenko et al. [28] | Histotopographical features of megakaryocytes allowed correct differentiation between ET and PMF in 71.6% of cases | Patterns of megakaryocyte distribution in BM of ET and prePMF patients with JAK2/CALR mutations can be revealed only using ML | The percentage of correct diagnostic predictions for PMF was only 40% | Unsupervised Learning: Density-Based Spatial Clustering of Applications with Noise (DBSCAN) | Clustering and anomaly detection in high-dimensional data Automatically detect clusters of arbitrary shape and size |
| Kantardzic et al. [29] | Extraction of new decision rules for PV diagnosis, based on a reduced and optimized set of lab parameters | Reducing the original parameters of diagnosis to only four while still obtaining good classification results | Not diagnostic by its own Only complements the standard PVSG criteria | Supervised Learning: Artificial neural networks (ANNs) and Support vector machines (SVMs) | Classification and regression tasks Both require large amounts of labeled data for training |
| Shen et al. [30] | Progressive platelet transcriptomic markers, enable an externally validated prediction for advanced MPNs | Comprehensive catalog of platelet transcriptome in chronic MPNs Accurate prediction of MF using <5 candidate markers | Only analyzed platelet-derived molecular alterations Biological and computational validations are needed for decision making | Supervised Learning: Multiple LASSO (Least Absolute Shrinkage and Selection Operator) penalized regression classifiers | Classification and prediction tasks, especially when there are more features than observations |
| Ryou et al. [31] | Continuous Indexing of Fibrosis (CIF) enhances the detection and monitoring of fibrosis within BMTs and aids MPN subtyping | Accurate discrimination between ET and Pre-PMF Identification of MPN patients at risk of progression | Invasive technique Requires BM trephines | Ranking-CNN: Learning to Rank (LTR) and Convolutional Neural Network (CNN) | Ranking and recommendation tasks LTR models rank items based on relevance, while CNNs extract features from raw data |
| Angelopoulos et al. [32] | Discovered genomic sets and their relationships in MPNs using Bayesian networks (BNs) | BNs allow correlations among driver events in large genomic cohorts Graphical illustrations | Robustness of the networks is important for BN learning Not suitable for small datasets | Probabilistic Graphical: Bayesian networks | Probabilistic inference and decision-making under uncertainty Models’ complex relationships between variables |
| Li et al. [33] | EPB42, CALR, SLC4A1 and MPL are candidate prognostic biomarkers and potential therapeutic targets for early PMF | WGCNA, a powerful global research tool for data mining from multiple genes in large-scale datasets was used | Molecular biological studies and larger samples are needed to further validate these hub genes | Supervised Learning: Support vector machines (SVMs) | Classification and prediction tasks, especially when there are more features than observations |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elsayed, B.; Elshoeibi, A.M.; Elhadary, M.; Ferih, K.; Elsabagh, A.A.; Rahhal, A.; Abu-Tineh, M.; Afana, M.S.; Abdulgayoom, M.; Yassin, M. Applications of Artificial Intelligence in Philadelphia-Negative Myeloproliferative Neoplasms. Diagnostics 2023, 13, 1123. https://doi.org/10.3390/diagnostics13061123
Elsayed B, Elshoeibi AM, Elhadary M, Ferih K, Elsabagh AA, Rahhal A, Abu-Tineh M, Afana MS, Abdulgayoom M, Yassin M. Applications of Artificial Intelligence in Philadelphia-Negative Myeloproliferative Neoplasms. Diagnostics. 2023; 13(6):1123. https://doi.org/10.3390/diagnostics13061123
Chicago/Turabian StyleElsayed, Basel, Amgad M. Elshoeibi, Mohamed Elhadary, Khaled Ferih, Ahmed Adel Elsabagh, Alaa Rahhal, Mohammad Abu-Tineh, Mohammad S. Afana, Mohammed Abdulgayoom, and Mohamed Yassin. 2023. "Applications of Artificial Intelligence in Philadelphia-Negative Myeloproliferative Neoplasms" Diagnostics 13, no. 6: 1123. https://doi.org/10.3390/diagnostics13061123