
Diagnostic Performance of Electromagnetic Navigation versus Virtual Navigation Bronchoscopy-Guided Biopsy for Pulmonary Lesions in a Single Institution: Potential Role of Artificial Intelligence for Navigation Planning


Abstract
:1. Introduction
2. Materials and Methods
2.1. Veran ENB Procedure
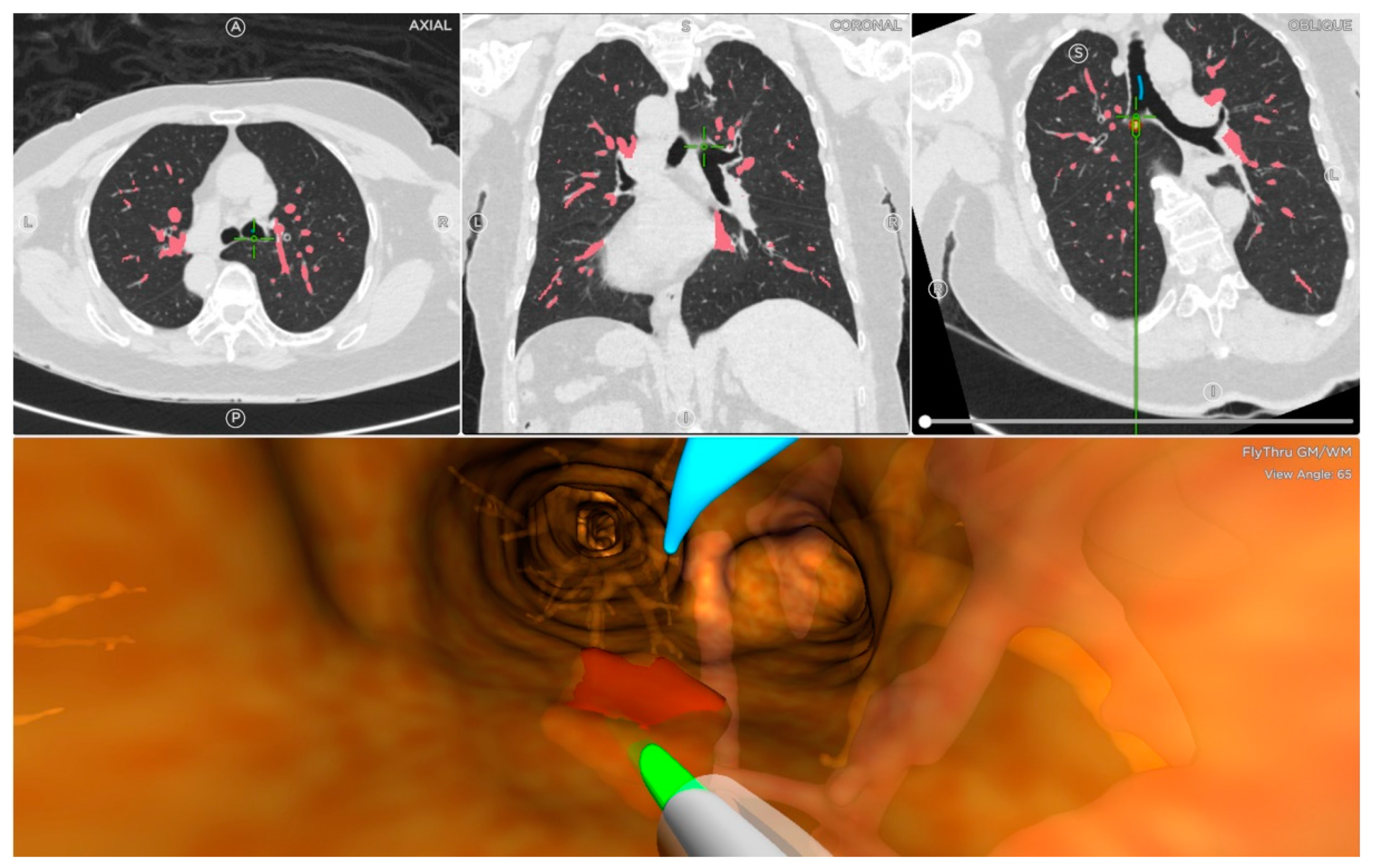
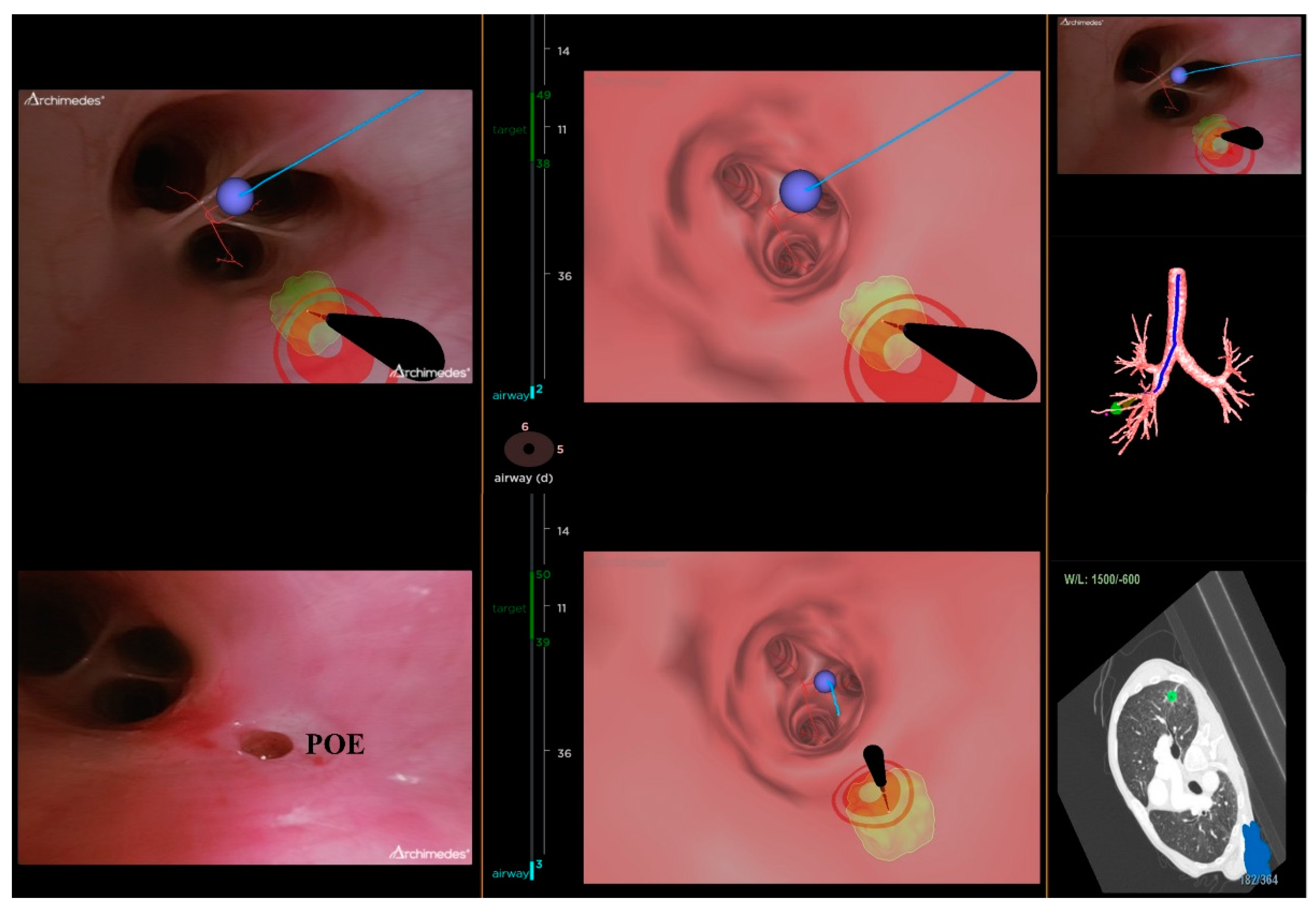
2.2. Archimedes VNB Procedure
2.3. Statical Analysis
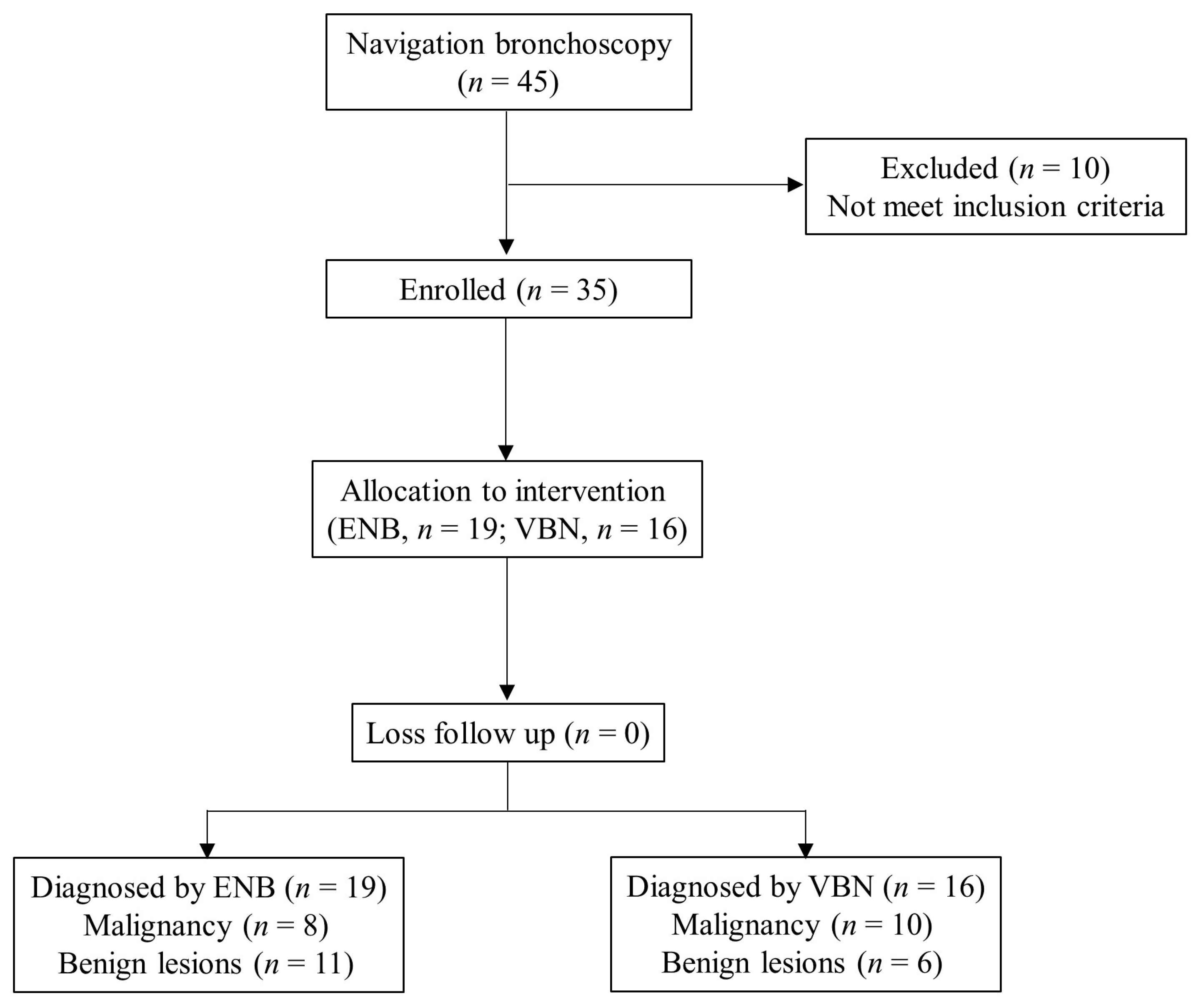
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Koning, H.J.; van der Aalst, C.M.; de Jong, P.A.; Scholten, E.T.; Nackaerts, K.; Heuvelmans, M.A.; Lammers, J.J.; Weenink, C.; Yousaf-Khan, U.; Horeweg, N.; et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N. Engl. J. Med. 2020, 382, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Gierada, D.S.; Pinsky, P.F. Survival Following Detection of Stage I Lung Cancer by Screening in the National Lung Screening Trial. Chest 2021, 159, 862–869. [Google Scholar] [CrossRef]
- Larscheid, R.C.; Thorpe, P.E.; Scott, W.J. Percutaneous transthoracic needle aspiration biopsy: A comprehensive review of its current role in the diagnosis and treatment of lung tumors. Chest 1998, 114, 704–709. [Google Scholar] [CrossRef] [PubMed]
- Popovich, J.; Jr Kvale, P.A.; Eichenhorn, M.S.; Radke, J.R.; Ohorodnik, J.M.; Fine, G. Diagnostic accuracy of multiple biopsies from flexible fiberoptic bronchoscopy. A comparison of central versus peripheral carcinoma. Am. Rev. Respir. Dis. 1982, 125, 521–523. [Google Scholar] [CrossRef] [PubMed]
- Baaklini, W.A.; Reinoso, M.A.; Gorin, A.B.; Sharafkaneh, A.; Manian, P. Diagnostic yield of fiberoptic bronchoscopy in evaluating solitary pulmonary nodules. Chest 2000, 117, 1049–1054. [Google Scholar] [CrossRef] [Green Version]
- Rickets, W.; Lau, K.K.W.; Pollit, V.; Mealing, S.; Leonard, C.; Mallender, P.; Chaudhuri, N.; Shah, P.L.; Naidu, U.B. Exploratory cost-effectiveness model of electromagnetic navigation bronchoscopy (ENB) compared with CT-guided biopsy (TTNA) for diagnosis of malignant indeterminate peripheral pulmonary nodules. BMJ Open. Respir. Res. 2020, 7, e000595. [Google Scholar] [CrossRef]
- DiBardino, D.M.; Yarmus, L.B.; Semaan, R.W. Transthoracic needle biopsy of the lung. J. Thorac. Dis. 2015, 7 (Suppl. S4), S304–S316. [Google Scholar]
- Heerink, W.J.; de Bock, G.H.; de Jonge, G.J.; Groen, H.J.; Vliegenthart, R.; Oudkerk, M. Complication rates of CT-guided transthoracic lung biopsy: Meta-analysis. Eur. Radiol. 2017, 27, 138–148. [Google Scholar] [CrossRef] [Green Version]
- Gex, G.; Pralong, J.A.; Combescure, C.; Seijo, L.; Rochat, T.; Soccal, P.M. Diagnostic yield and safety of electromagnetic navigation bronchoscopy for lung nodules: A systematic review and meta-analysis. Respiration 2014, 87, 165–176. [Google Scholar] [CrossRef]
- Mehta, A.C.; Hood, K.L.; Schwarz, Y.; Solomon, S.B. The Evolutional History of Electromagnetic Navigation Bronchoscopy: State of the Art. Chest 2018, 154, 935–947. [Google Scholar] [CrossRef]
- Wilson, D.S.; Bartlett, R.J. Improved Diagnostic Yield of Bronchoscopy in a Community Practice: Combination of Electromagnetic Navigation System and Rapid On-site Evaluation. J. Bronchol. Interv. Pulmonol. 2007, 14, 227–232. [Google Scholar] [CrossRef]
- Yutaka, Y.; Sato, T.; Isowa, M.; Murata, Y.; Tanaka, S.; Yamada, Y.; Ohsumi, A.; Nakajima, D.; Hamaji, M.; Menju, T.; et al. Electromagnetic navigation bronchoscopy versus virtual bronchoscopy navigation for improving the diagnosis of peripheral lung lesions: Analysis of the predictors of successful diagnosis. Surg. Today 2022, 52, 923–930. [Google Scholar] [CrossRef]
- Herth, F.J.; Eberhardt, R.; Sterman, D.; Silvestri, G.A.; Hoffmann, H.; Shah, P.L. Bronchoscopic transparenchymal nodule access (BTPNA): First in human trial of a novel procedure for sampling solitary pulmonary nodules. Thorax 2015, 70, 326–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang Memoli, J.S.; Nietert, P.J.; Silvestri, G.A. Meta-analysis of guided bronchoscopy for the evaluation of the pulmonary nodule. Chest 2012, 142, 385–393. [Google Scholar] [CrossRef] [Green Version]
- Sun, J.; Criner, G.J.; Dibardino, D.; Li, S.; Nader, D.; Lam, B.; Kopas, L.; Wahidi, M.M.; Majid, A.; Marron, R.; et al. Efficacy and safety of virtual bronchoscopic navigation with fused fluoroscopy and vessel mapping for access of pulmonary lesions. Respirology 2022, 27, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Tam, T.C.C.; Poon, H.M.; Yu, K.-C.; Lee, W.-N. NaviAirway: A bronchiole-sensitive deep learning-based airway segmentation pipeline for planning of navigation bronchoscopy. arXiv 2022, arXiv:2203.04294. [Google Scholar]
- Yoo, J.Y.; Kang, S.Y.; Park, J.S.; Cho, Y.-J.; Park, S.Y.; Yoon, H.I.; Park, S.J.; Jeong, H.-G.; Kim, T. Deep learning for anatomical interpretation of video bronchoscopy images. Sci. Rep. 2021, 11, 23765. [Google Scholar] [CrossRef]
- Chien, J.C.; Lee, J.D.; Su, E.; Li, S.H. A Bronchoscope Localization Method Using an Augmented Reality Co-Display of Real Bronchoscopy Images with a Virtual 3D Bronchial Tree Model. Sensors 2020, 20, 6997. [Google Scholar] [CrossRef]
- Ernst, A.; Wahidi, M.M.; Read, C.A.; Buckley, J.D.; Addrizzo-Harris, D.J.; Shah, P.L.; Herth, F.J.F.; de Hoyos Parra, A.; Ornelas, J.; Yarmus, L.; et al. Adult Bronchoscopy Training: Current State and Suggestions for the Future: CHEST Expert Panel Report. Chest 2015, 148, 321–332. [Google Scholar] [CrossRef] [Green Version]
- Stather, D.R.; Maceachern, P.; Chee, A.; Dumoulin, E.; Tremblay, A. Trainee impact on advanced diagnostic bronchoscopy: An analysis of 607 consecutive procedures in an interventional pulmonary practice. Respirology 2013, 18, 179–184. [Google Scholar] [CrossRef]
- Semaan, R.W.; Lee, H.J.; Feller-Kopman, D.; Lerner, A.D.; Mallow, C.M.; Thiboutot, J.; Arias, S.A.; Yarmus, L.B. Same-Day Computed Tomographic Chest Imaging for Pulmonary Nodule Targeting with Electromagnetic Navigation Bronchoscopy May Decrease Unnecessary Procedures. Ann. Am. Thorac. Soc. 2016, 13, 2223–2228. [Google Scholar] [CrossRef]
- Schwarz, Y.; Greif, J.; Becker, H.D.; Ernst, A.; Mehta, A. Real-time electromagnetic navigation bronchoscopy to peripheral lung lesions using overlaid CT images: The first human study. Chest 2006, 129, 988–994. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.W.; Kim, H.-J.; Song, M.J.; Kwon, B.S.; Lim, S.Y.; Lee, Y.J.; Park, J.S.; Cho, Y.-J.; Yoon, H.I.; Lee, J.H.; et al. Utility and safety of sole electromagnetic navigation bronchoscopy under moderate sedation for lung cancer diagnosis. Transl. Lung Cancer Res. 2022, 11, 462–471. [Google Scholar] [CrossRef]
- Ost, D.E.; Ernst, A.; Lei, X.; Kovitz, K.L.; Benzaquen, S.; Diaz-Mendoza, J.; Greenhill, S.; Toth, J.; Feller-Kopman, D.; Puchalski, J.; et al. Diagnostic Yield and Complications of Bronchoscopy for Peripheral Lung Lesions. Results of the AQuIRE Registry. Am. J. Respir. Crit. Care Med. 2016, 193, 68–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Folch, E.E.; Pritchett, M.A.; Nead, M.A.; Bowling, M.R.; Murgu, S.D.; Krimsky, W.S.; Murillo, B.A.; LeMense, G.P.; Minnich, D.J.; Bansal, S.; et al. Electromagnetic Navigation Bronchoscopy for Peripheral Pulmonary Lesions: One-Year Results of the Prospective, Multicenter NAVIGATE Study. J. Thorac. Oncol. 2019, 14, 445–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Criner, G.J.; Eberhardt, R.; Fernandez-Bussy, S.; Gompelmann, D.; Maldonado, F.; Patel, N.; Shah, P.L.; Slebos, D.J.; Valipour, A.; Wahidi, M.M.; et al. Interventional Bronchoscopy. Am. J. Respir. Crit. Care Med. 2020, 202, 29–50. [Google Scholar] [CrossRef]
- Oki, M.; Saka, H.; Asano, F.; Kitagawa, C.; Kogure, Y.; Tsuzuku, A.; Ando, M. Use of an Ultrathin vs Thin Bronchoscope for Peripheral Pulmonary Lesions: A Randomized Trial. Chest 2019, 156, 954–964. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.M.; Yu, K.L.; Lin, K.H.; Liu, Y.L.; Sun, S.E.; Meng, L.H.; Ko, H.J. Localization of Small Pulmonary Nodules Using Augmented Fluoroscopic Bronchoscopy: Experience from 100 Consecutive Cases. World J. Surg. 2020, 44, 2418–2425. [Google Scholar] [CrossRef]
- Mariolo, A.V.; Vieira, T.; Stern, J.B.; Perrot, L.; Caliandro, R.; Escande, R.; Brian, E.; Grigoroiu, M.; Boddaert, G.; Gossot, D.; et al. Electromagnetic navigation bronchoscopy localization of lung nodules for thoracoscopic resection. J. Thorac. Dis. 2021, 13, 4371–4377. [Google Scholar] [CrossRef]
- Ali, M.S.; Sethi, J.; Taneja, A.; Musani, A.; Maldonado, F. Computed Tomography Bronchus Sign and the Diagnostic Yield of Guided Bronchoscopy for Peripheral Pulmonary Lesions. A Systematic Review and Meta-Analysis. Ann. Am. Thorac. Soc. 2018, 15, 978–987. [Google Scholar] [CrossRef]
- Wang, C.W.; Khalil, M.A.; Lin, Y.J.; Lee, Y.C.; Huang, T.W.; Chao, T.K. Deep Learning Using Endobronchial-Ultrasound-Guided Transbronchial Needle Aspiration Image to Improve the Overall Diagnostic Yield of Sampling Mediastinal Lymphadenopathy. Diagnostics 2022, 12, 2234. [Google Scholar] [CrossRef] [PubMed]
- Bhadra, K. Artificial Intelligence Improves Patient Outcomes for Diagnostics of Pulmonary Nodules During Navigational Bronchoscopy. Am. J. Respir. Crit. Care Med. 2019, 199, A2360. [Google Scholar]
- Zhang, Y.; Jheon, S.; Li, H.; Zhang, H.; Xie, Y.; Qian, B.; Lin, K.; Wang, S.; Fu, C.; Hu, H.; et al. Results of low-dose computed tomography as a regular health examination among Chinese hospital employees. J. Thorac. Cardiovasc. Surg. 2020, 160, 824–831.e4. [Google Scholar] [CrossRef] [PubMed]
- Banach, A.; King, F.; Masaki, F.; Tsukada, H.; Hata, N. Visually Navigated Bronchoscopy using three cycle-Consistent generative adversarial network for depth estimation. Med. Image Anal. 2021, 73, 102164. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Total | 35 |
| Age (years) mean (range) | 67.6 ± 9.9 (48–85) |
| Sex (n, %) | |
| Male | 18 (51.4%) |
| Female | 17 (48.6%) |
| Body mass index | 23.2 ± 3.6 (16.6–31.6) |
| Smoking history | 13 (37.1%) |
| Pack-years mean (range) | 32.2 ± 19.5 (10–75) |
| Procedure time (min) | 54.8 ± 30.4 (13–127) |
| Lesion size (mm) mean (range) | 36.3 ± 21.9 (11–128) |
| Location (n, %) | |
| Right upper lobe | 11 (31.4%) |
| Right middle lobe | 4 (11.4%) |
| Right lower lobe | 12 (34.3%) |
| Left upper lobe | 6 (17.1%) |
| Left lower lobe | 2 (5.7%) |
| Distance from pleura (mm) mean (range) | 16.1 ± 11.7 (1–41) |
| Radiographic characteristics (n, %) | |
| Ground glass opacity | 0 (0.0%) |
| Part-solid | 2 (5.7%) |
| Solid | 33 (94.3%) |
| Air-bronchus present | 32 (91.4%) |
| Histopathology | |
| Benign diagnosis | 17 (48.6%) |
| Cancer diagnosis | 18 (51.4%) |
| Variable | ENB (n = 19) | VBN (n = 16) | p-Value |
|---|---|---|---|
| Age | 69.6 ± 10.1 | 61.5 ± 9.7 | 0.194 |
| Sex (Male) | 12 (63.2%) | 6 (37.5%) | 0.130 |
| Body mass index | 23.5 ± 3.7 | 22.8 ± 3.5 | 0.575 |
| Smoking history | 7 (36.8%) | 6 (37.5%) | 0.968 |
| Pack-years | 30.7 ± 20.1 | 33.8 ± 20.6 | 0.788 |
| Size (mm) | 36.6 ± 16.5 (11–80) | 27.6 ± 8.7 (14–41) | 0.049 |
| Procedure time (min) | 45.2 ± 17.6 (13–83) | 38.33 ± 13.8 (16–56) a | 0.313 |
| 66.8 ± 38.7 (16–127) b | 0.037 | ||
| Location (n, %) | 0.301 | ||
| Right upper lobe | 5 (26.3%) | 6 (37.5%) | |
| Right middle lobe | 2 (10.5%) | 2 (12.5%) | |
| Right lower lobe | 7 (36.8%) | 5 (31.3%) | |
| Left upper lobe | 5 (26.3%) | 1 (6.3%) | |
| Left lower lobe | 0 (0.0%) | 2 (12.5%) | |
| Distance from pleura (mm) | 14.3 ± 12.4 | 18.3 ± 10.9 | 0.322 |
| Radiographic characteristics (n, %) | 0.181 | ||
| Ground glass opacity | 0 (0.0%) | 0 (0.0%) | |
| Part-solid | 2 (10.5%) | 0 (0.0%) | |
| Solid | 17 (89.5%) | 16 (100.0%) | |
| Air-bronchus present | 17 (89.5%) | 15 (93.8%) | 0.653 |
| Histopathology | 0.154 | ||
| Benign diagnosis | 11 (57.9%) | 6 (37.5%) | |
| Cancer diagnosis | 8 (42.1%) | 10 (62.5%) |
| Variable | Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value |
|---|---|---|---|---|
| ENB | 80.0% (8/10) | 77.8% (7/9) | 80.0% (8/10) | 77.8% (7/9) |
| VBN | 90.0% (9/10) | 100.0% (6/6) | 90.0% (9/10) | 85.7% (6/7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, Y.-M.; Kuo, Y.-S.; Lin, K.-H.; Chen, Y.-Y.; Huang, T.-W. Diagnostic Performance of Electromagnetic Navigation versus Virtual Navigation Bronchoscopy-Guided Biopsy for Pulmonary Lesions in a Single Institution: Potential Role of Artificial Intelligence for Navigation Planning. Diagnostics 2023, 13, 1124. https://doi.org/10.3390/diagnostics13061124
Tsai Y-M, Kuo Y-S, Lin K-H, Chen Y-Y, Huang T-W. Diagnostic Performance of Electromagnetic Navigation versus Virtual Navigation Bronchoscopy-Guided Biopsy for Pulmonary Lesions in a Single Institution: Potential Role of Artificial Intelligence for Navigation Planning. Diagnostics. 2023; 13(6):1124. https://doi.org/10.3390/diagnostics13061124
Chicago/Turabian StyleTsai, Yuan-Ming, Yen-Shou Kuo, Kuan-Hsun Lin, Ying-Yi Chen, and Tsai-Wang Huang. 2023. "Diagnostic Performance of Electromagnetic Navigation versus Virtual Navigation Bronchoscopy-Guided Biopsy for Pulmonary Lesions in a Single Institution: Potential Role of Artificial Intelligence for Navigation Planning" Diagnostics 13, no. 6: 1124. https://doi.org/10.3390/diagnostics13061124