
Classification of Breast Lesions on DCE-MRI Data Using a Fine-Tuned MobileNet
Abstract
:1. Introduction
2. Materials and Methods
2.1. Dataset
2.2. MRI Techniques
2.3. Proposed Model
2.4. Data Augmentation
2.5. Network Structure of MobileNetV1
2.6. Network Structure of MobileNetV2
2.7. Fine-Tuning Strategies
2.8. Hyperparameter Settings
2.9. Evaluation Metrics
3. Results
3.1. Intergroup Age and Lesion Diameter Comparisons
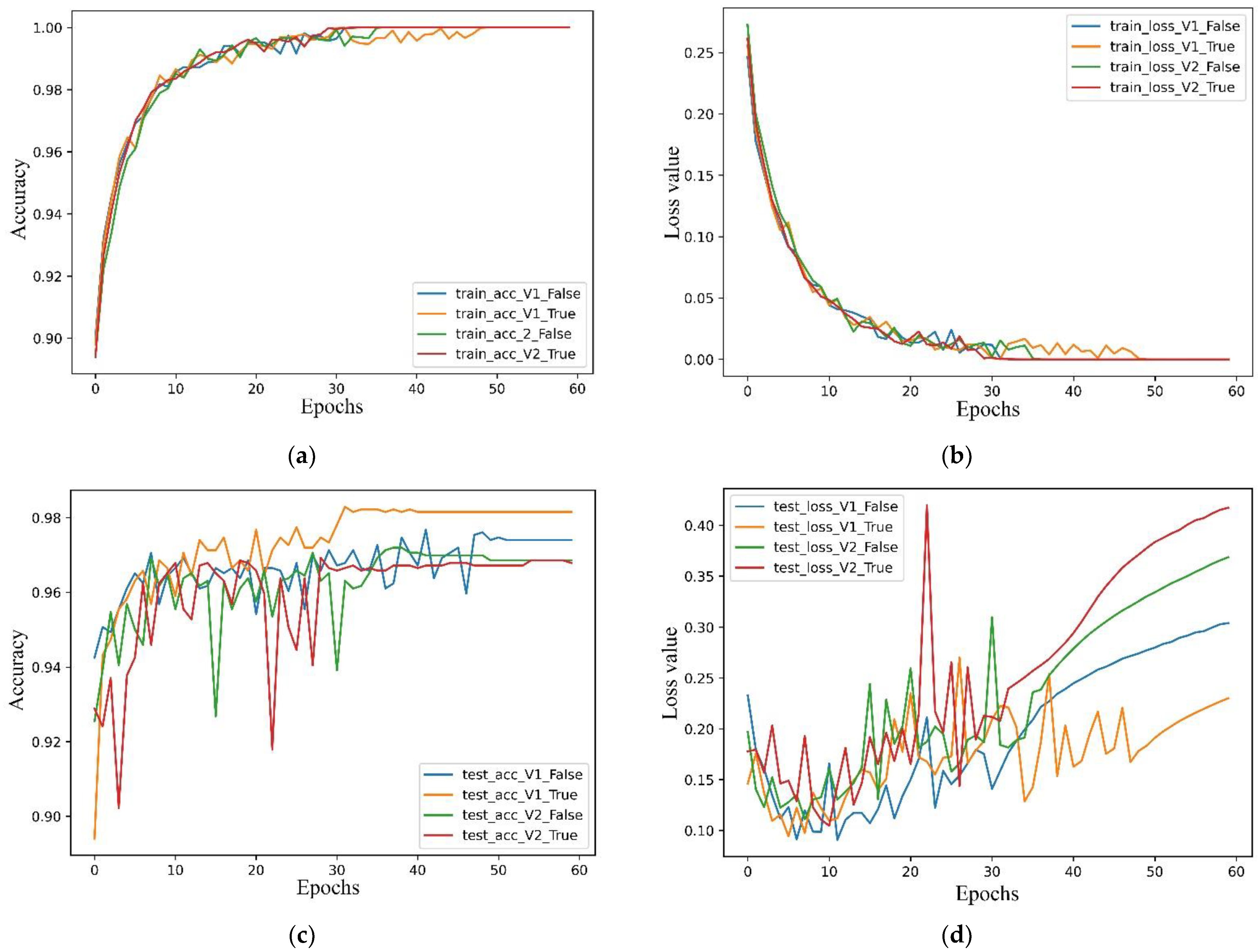
3.2. Learning Curves
3.3. Training Time and Model Size
3.4. Cross-Validation
3.5. Classification Report
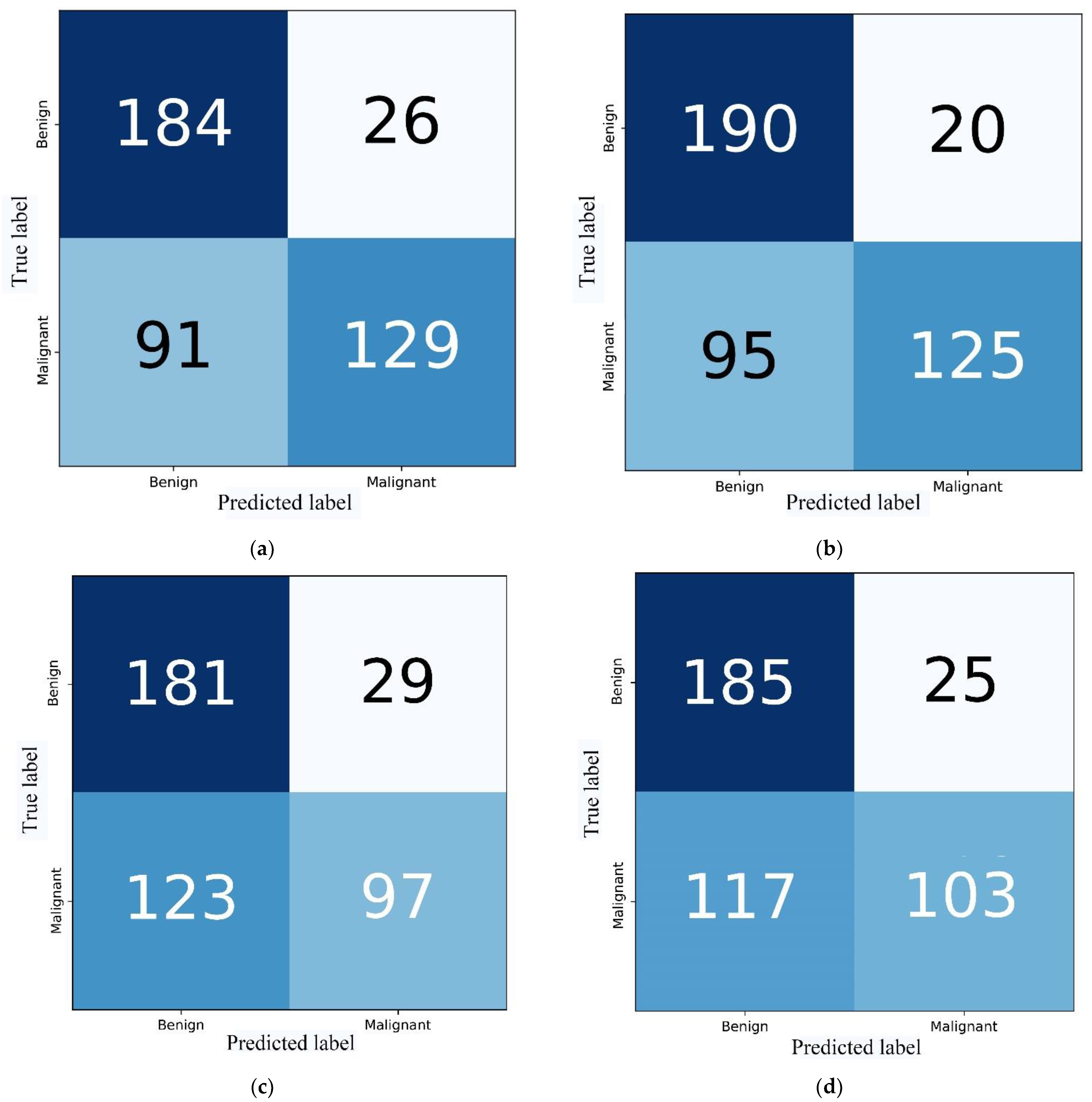
3.6. Visualization of Confusion Matrices
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Fujioka, T.; Mori, M.; Kubota, K.; Oyama, J.; Yamaga, E.; Yashima, Y.; Katsuta, L.; Nomura, K.; Nara, M.; Oda, G.; et al. The Utility of Deep Learning in Breast Ultrasonic Imaging: A Review. Diagnostics 2020, 10, 1055. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.M.; Khan, R.A.; Arif, S.; Sajid, U. Artificial intelligence for breast cancer analysis: Trends & directions. Comput. Biol. Med. 2022, 142, 105221. [Google Scholar] [PubMed]
- Zerouaoui, H.; Idri, A. Reviewing Machine Learning and Image Processing Based Decision-Making Systems for Breast Cancer Imaging. J. Med. Syst. 2021, 45, 8. [Google Scholar] [CrossRef]
- Gubern-Mérida, A.; Martí, R.; Melendez, J.; Hauth, J.L.; Mann, R.M.; Karssemeijer, N.; Platel, B. Automated localization of breast cancer in DCE-MRI. Med. Image Anal. 2015, 20, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Xie, Y.; Wu, Q.; Xia, Y. Medical image classification using synergic deep learning. Med. Image Anal. 2019, 54, 10–19. [Google Scholar] [CrossRef]
- Ayana, G.; Park, J.; Jeong, J.-W.; Choe, S.-W. A Novel Multistage Transfer Learning for Ultrasound Breast Cancer Image Classification. Diagnostics 2022, 12, 135. [Google Scholar] [CrossRef] [PubMed]
- Saffari, N.; Rashwan, H.; Abdel-Nasser, M.; Singh, V.K.; Arenas, M.; Mangina, E.; Herrera, B.; Puig, D. Fully Automated Breast Density Segmentation and Classification Using Deep Learning. Diagnostics 2020, 10, 988. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Edwards, A.V.; Newstead, G.M. Artificial Intelligence Applied to Breast MRI for Improved Diagnosis. Radiology 2021, 298, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Das, A.; Nair, M.S.; Peter, S.D. Computer-Aided Histopathological Image Analysis Techniques for Automated Nuclear Atypia Scoring of Breast Cancer: A Review. J. Digit. Imaging 2020, 33, 1091–1121. [Google Scholar] [CrossRef]
- Dong, F.; She, R.; Cui, C.; Shi, S.; Hu, X.; Zeng, J.; Wu, H.; Xu, J.; Zhang, Y. One step further into the blackbox: A pilot study of how to build more confidence around an AI-based decision system of breast nodule assessment in 2D ultrasound. Eur. Radiol. 2021, 31, 4991–5000. [Google Scholar] [CrossRef]
- Yang, Y.; Hu, Y.; Shen, S.; Jiang, X.; Gu, R.; Wang, H.; Liu, F.; Mei, J.; Liang, J.; Jia, H.; et al. A new nomogram for predicting the malignant diagnosis of Breast Imaging Reporting and Data System (BI-RADS) ultrasonography category 4A lesions in women with dense breast tissue in the diagnostic setting. Quant Imaging Med. Surg. 2021, 11, 3005–3017. [Google Scholar] [CrossRef]
- Tripathi, S.; Singh, S.K.; Lee, H.K. An end-to-end breast tumour classification model using context-based patch modelling—A BiLSTM approach for image classification. Comput. Med. Imaging Graph. 2021, 87, 101838. [Google Scholar] [CrossRef]
- Barsha, N.A.; Rahman, A.; Mahdy, M.R.C. Automated detection and grading of Invasive Ductal Carcinoma breast cancer using ensemble of deep learning models. Comput. Biol. Med. 2021, 139, 104931. [Google Scholar] [CrossRef]
- Avanzo, M.; Wei, L.; Stancanello, J.; Vallières, M.; Rao, A.; Morin, O.; Mattonen, S.A.; El Naqa, I. Machine and deep learning methods for radiomics. Med. Phys. 2020, 47, e185–e202. [Google Scholar] [CrossRef]
- Chan, H.P.; Hadjiiski, L.M.; Samala, R.K. Computer-aided diagnosis in the era of deep learning. Med. Phys. 2020, 47, e218–e227. [Google Scholar] [CrossRef] [PubMed]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; van der Laak, J.A.W.M.; van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L.C. MobileNetV2: Inverted Residuals and Linear Bottlenecks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Salt Lake City, UT, USA, 18–22 June 2018; pp. 4510–4520. [Google Scholar] [CrossRef]
- Taresh, M.M.; Zhu, N.; Ali, T.A.A.; Hameed, A.S.; Mutar, M.L. Transfer Learning to Detect COVID-19 Automatically from X-ray Images Using Convolutional Neural Networks. Int. J. Biomed. Imaging 2021, 2021, 8828404. [Google Scholar] [CrossRef] [PubMed]
- Koward, A.G.; Zhu, M.; Chen, B.; Kalenichenko, D.; Wang, W.; Weyand, T.; Adam, H. MobileNets: Efficient Convolutional Neural Networks for Mobile Vision Applications. arXiv 2017, arXiv:170404861. [Google Scholar] [CrossRef]
- Wang, Z.; Li, X.; Yao, M.; Li, J.; Jiang, Q.; Yan, B. A new detection model of microaneurysms based on improved FC-DenseNet. Sci. Rep. 2022, 12, 950. [Google Scholar] [CrossRef]
- Mahmood, T.; Li, J.; Pei, Y.; Akhtar, F. An Automated In-Depth Feature Learning Algorithm for Breast Abnormality Prognosis and Robust Characterization from Mammography Images Using Deep Transfer Learning. Biology 2021, 10, 859. [Google Scholar] [CrossRef]
- Gomez-Flores, W.; Coelho de Albuquerque Pereira, W. A Comparative Study of Pre-trained Convolutional Neural Networks for Semantic Segmentation of Breast Tumors in Ultrasound. Comput. Biol. Med. 2020, 126, 104036. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Hu, Y.; Zou, T.; Liu, H.; Wang, J.; Wang, X. A New Image Classification Approach via Improved MobileNet Models with Local Receptive Field Expansion in Shallow Layers. Comput. Intell. Neurosci. 2020, 2020, 8817849. [Google Scholar] [CrossRef] [PubMed]
- Arora, V.; Ng, E.Y.-K.; Leekha, R.S.; Darshan, M.; Singh, A. Transfer learning-based approach for detecting COVID-19 ailment in lung CT scan. Comput. Biol. Med. 2021, 135, 104575. [Google Scholar] [CrossRef] [PubMed]
- Bolcato, M.; Fassina, G.; Rodriguez, D.; Russo, M.; Aprile, A. The contribution of legal medicine in clinical risk management. BMC Health Serv. Res. 2019, 19, 85. [Google Scholar] [CrossRef] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pathological Diagnosis | Cases | Percent (%) | Age (Years) | Lesion Diameter (mm) |
|---|---|---|---|---|
| Malignant lesions | 48.2 ± 11.4 | 24.00 ± 11.09 | ||
| Invasive ductal carcinoma | 124 | 80.52 | ||
| Intraductal carcinoma | 19 | 12.34 | ||
| Invasive lobular carcinoma | 4 | 2.60 | ||
| Mucinous carcinoma | 4 | 2.60 | ||
| Lymphoma | 1 | 0.65 | ||
| Papillary carcinoma | 2 | 1.30 | ||
| Total | 154 | 100.00 | ||
| Benign lesions | 45.0 ± 10.5 | 32.89 ± 16.45 | ||
| Cyst | 17 | 9.83 | ||
| Adenosis | 26 | 15.03 | ||
| Fibroadenoma | 111 | 64.16 | ||
| Chronic inflammation | 4 | 2.31 | ||
| Intraductal papilloma | 13 | 7.51 | ||
| Lobular tumour | 2 | 1.16 | ||
| Total | 173 | 100.00 |
| Parameters. | Philips Achieva | GE Healthcare |
|---|---|---|
| Field strength | 3.0 T | 3.0 T |
| No. of coil channels | 8 | 8 |
| Acquisition plane | Axial | Axial |
| Pulse sequence | 3D gradient echo (Thrive) | Enhanced fast gradient echo 3D |
| Repetition time (ms) | 5.5 | 9.6 |
| Echo time (ms) | 2.7 | 2.1 |
| Flip angle | 10° | 10° |
| No. of postcontrast phases | 5 | 5 |
| Fat suppression | Yes | Yes |
| Scan time | 570 s | 500 s |
| Parameter | Value |
|---|---|
| Rotation range | 60° |
| Shear range | 0.2 |
| Zoom range | 0.2 |
| Horizontal flip | True |
| Vertical flip | True |
| Fill mode | Nearest |
| Models | Params1 | Params2 | Params3 | Time (min) | Size (MB) |
|---|---|---|---|---|---|
| V1_False | 3,228,864 | 0 | 3,228,864 | 19.23 | 19.4 |
| V1_True | 3,228,864 | 3,206,976 | 21,888 | 20.67 | 19.4 |
| V2_False | 2,257,984 | 0 | 2,257,984 | 27.55 | 16.7 |
| V2_True | 2,257,984 | 2,223,872 | 34,112 | 25.99 | 16.7 |
| Folds | Ac1 | Loss1 | Ac2 | Loss2 |
|---|---|---|---|---|
| Fold1 | 1.00 | ˂0.01 | 0.9815 | 0.2322 |
| Fold2 | 1.00 | ˂0.01 | 0.9803 | 0.2225 |
| Fold3 | 1.00 | ˂0.01 | 0.9812 | 0.2175 |
| Fold4 | 1.00 | ˂0.01 | 0.9805 | 0.2402 |
| Fold5 | 1.00 | ˂0.01 | 0.9814 | 0.2156 |
| DTL Models | Pr | Rc | F1 | AUC | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Group1 | Group2 | Avg | Group1 | Group2 | Avg | Group1 | Group2 | Avg | ||
| V1_False | 0.88 | 0.59 | 0.77 | 0.67 | 0.83 | 0.73 | 0.76 | 0.69 | 0.73 | 0.73 |
| V1_True | 0.90 | 0.57 | 0.79 | 0.67 | 0.86 | 0.73 | 0.77 | 0.68 | 0.74 | 0.74 |
| V2_False | 0.86 | 0.44 | 0.74 | 0.60 | 0.77 | 0.65 | 0.70 | 0.56 | 0.66 | 0.65 |
| V2_True | 0.88 | 0.47 | 0.76 | 0.61 | 0.80 | 0.67 | 0.72 | 0.59 | 0.68 | 0.67 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.; Zhang, M.; He, G.; Shen, D.; Meng, M. Classification of Breast Lesions on DCE-MRI Data Using a Fine-Tuned MobileNet. Diagnostics 2023, 13, 1067. https://doi.org/10.3390/diagnostics13061067
Wang L, Zhang M, He G, Shen D, Meng M. Classification of Breast Lesions on DCE-MRI Data Using a Fine-Tuned MobileNet. Diagnostics. 2023; 13(6):1067. https://doi.org/10.3390/diagnostics13061067
Chicago/Turabian StyleWang, Long, Ming Zhang, Guangyuan He, Dong Shen, and Mingzhu Meng. 2023. "Classification of Breast Lesions on DCE-MRI Data Using a Fine-Tuned MobileNet" Diagnostics 13, no. 6: 1067. https://doi.org/10.3390/diagnostics13061067