
Prognostic Scores in Acute Liver Failure Due to Viral Hepatitis

Abstract
:1. Introduction
2. Viral Etiologies of ALF
3. Epidemiology
4. Importance of Prognostic Systems
- (i)
- Dynamicity
- (ii)
- Applicability
- (iii)
- Accuracy
- (iv)
- Ease of use
5. Clinical Presentation of Viral ALF
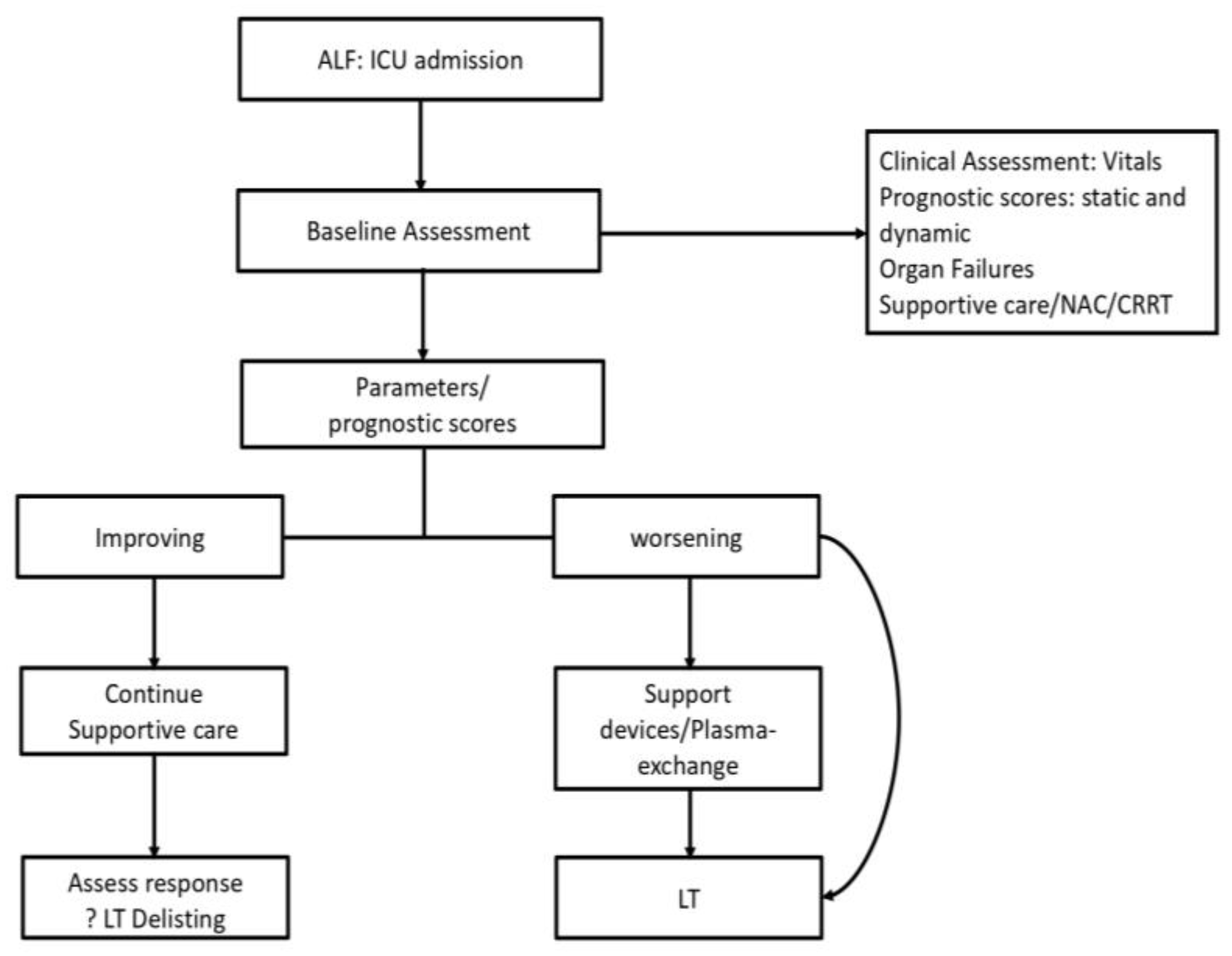
6. Approach to Management
7. Prognostic Scoring Systems in Viral ALF
8. Management of Viral ALF
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Acharya, S.K. Acute Liver Failure: Indian Perspective. Clin. Liver Dis. 2021, 18, 143–149. [Google Scholar] [CrossRef]
- Shalimar; Acharya, S.K.; Lee, W.M. Worldwide Differences in Acute Liver Failure. In Critical Care in Acute Liver Failure; Future Medicine Ltd.: London, UK, 2013; pp. 32–46. [Google Scholar]
- Anand, A.C.; Nandi, B.; Acharya, S.K.; Arora, A.; Babu, S.; Batra, Y.; Chawla, Y.K.; Chowdhury, A.; Chaoudhuri, A.; Eapen, E.C.; et al. Indian National Association for the Study of the Liver Consensus Statement on Acute Liver Failure (Part 1): Epidemiology, Pathogenesis, Presentation and Prognosis. J. Clin. Exp. Hepatol. 2020, 10, 339–376. [Google Scholar] [CrossRef]
- Kumar, R.; Anand, U.; Priyadarshi, R.N. Liver Transplantation in Acute Liver Failure: Dilemmas and Challenges. World J. Transplant. 2021, 11, 187–202. [Google Scholar] [CrossRef]
- Bretherick, A.D.; Craig, D.G.N.; Masterton, G.; Bates, C.; Davidson, J.; Martin, K.; Iredale, J.P.; Simpson, K.J. Acute Liver Failure in Scotland between 1992 and 2009; Incidence, Aetiology and Outcome. QJM Int. J. Med. 2011, 104, 945–956. [Google Scholar] [CrossRef] [Green Version]
- Nephew, L.D.; Zia, Z.; Ghabril, M.; Orman, E.; Lammert, C.; Kubal, C.; Chalasani, N. Sex Disparities in Waitlisting and Liver Transplant for Acute Liver Failure. JHEP Rep. 2020, 3, 100200. [Google Scholar] [CrossRef]
- Mehrotra, S.; Mehta, N.; Rao, P.S.; Lalwani, S.; Mangla, V.; Nundy, S. Live Donor Liver Transplantation for Acute Liver Failure: A Single Center Experience. Indian J. Gastroenterol. 2018, 37, 25–30. [Google Scholar] [CrossRef]
- Koch, D.G.; Tillman, H.; Durkalski, V.; Lee, W.M.; Reuben, A. Development of a Model to Predict Transplant-Free Survival of Patients with Acute Liver Failure. Clin. Gastroenterol. Hepatol. 2016, 14, 1199–1206.e2. [Google Scholar] [CrossRef]
- Shalimar; Sonika, U.; Kedia, S.; Mahapatra, S.J.; Nayak, B.; Yadav, D.P.; Gunjan, D.; Thakur, B.; Kaur, H.; Acharya, S.K. Comparison of Dynamic Changes among Various Prognostic Scores in Viral Hepatitis-Related Acute Liver Failure. Ann. Hepatol. 2018, 17, 403–412. [Google Scholar] [CrossRef]
- Bernal, W.; Lee, W.M.; Wendon, J.; Larsen, F.S.; Williams, R. Acute Liver Failure: A Curable Disease by 2024? J. Hepatol. 2015, 62, S112–S120. [Google Scholar] [CrossRef] [Green Version]
- Patterson, J.; Hussey, H.S.; Abdullahi, L.H.; Silal, S.; Goddard, L.; Setshedi, M.; Spearman, W.; Hussey, G.D.; Kagina, B.; Muloiwa, R. The Global Epidemiology of Viral-Induced Acute Liver Failure: A Systematic Review Protocol. BMJ Open 2019, 9, e029819. [Google Scholar] [CrossRef] [Green Version]
- Patterson, J.; Hussey, H.S.; Silal, S.; Goddard, L.; Setshedi, M.; Spearman, W.; Hussey, G.D.; Kagina, B.M.; Muloiwa, R. Systematic Review of the Global Epidemiology of Viral-Induced Acute Liver Failure. BMJ Open 2020, 10, e037473. [Google Scholar] [CrossRef]
- Ciglenecki, I.; Rumunu, J.; Wamala, J.F.; Nkemenang, P.; Duncker, J.; Nesbitt, R.; Gignoux, E.; Newport, T.; Heile, M.; Jamet, C.; et al. The First Reactive Vaccination Campaign against Hepatitis E. Lancet Infect. Dis. 2022, 22, 1110–1111. [Google Scholar] [CrossRef]
- Shalimar; Acharya, S.K.; Kumar, R.; Bharath, G.; Rout, G.; Gunjan, D.; Nayak, B. Acute Liver Failure of Non–A-E Viral Hepatitis Etiology—Profile, Prognosis, and Predictors of Outcome. J. Clin. Exp. Hepatol. 2020, 10, 453–461. [Google Scholar] [CrossRef]
- Thanapirom, K.; Treeprasertsuk, S.; Soonthornworasiri, N.; Poovorawan, K.; Chaiteerakij, R.; Komolmit, P.; Phaosawasdi, K.; Pinzani, M. The Incidence, Etiologies, Outcomes, and Predictors of Mortality of Acute Liver Failure in Thailand: A Population-Base Study. BMC Gastroenterol. 2019, 19, 18. [Google Scholar] [CrossRef]
- Simões, C.; Santos, S.; Vicente, M.; Sousa Cardoso, F. Epidemiology of Acute Liver Failure from a Regional Liver Transplant Center in Portugal. GE-Port. J. Gastroenterol. 2019, 26, 33–39. [Google Scholar] [CrossRef]
- Polson, J.; Lee, W.M. AASLD Position Paper: The Management of Acute Liver Failure. Hepatology 2005, 41, 1179–1197. [Google Scholar] [CrossRef]
- Wendon, J.; Cordoba, J.; Dhawan, A.; Larsen, F.S.; Manns, M.; Nevens, F.; Samuel, D.; Simpson, K.J.; Yaron, I.; Bernardi, M. EASL Clinical Practical Guidelines on the Management of Acute (Fulminant) Liver Failure. J. Hepatol. 2017, 66, 1047–1081. [Google Scholar] [CrossRef]
- Donnelly, M.C.; Davidson, J.S.; Martin, K.; Baird, A.; Hayes, P.C.; Simpson, K.J. Acute Liver Failure in Scotland: Changes in Aetiology and Outcomes over Time (the Scottish Look-Back Study). Aliment. Pharmacol. Ther. 2017, 45, 833–843. [Google Scholar] [CrossRef] [Green Version]
- Ordys, B.B.; Robinson, O. Acute Liver Failure. Anaesth. Intensive Care Med. 2021, 22, 113–120. [Google Scholar] [CrossRef]
- Matar, A.J.; Subramanian, R. Extracorporeal Liver Support: A Bridge to Somewhere. Clin. Liver Dis. 2021, 18, 274–279. [Google Scholar] [CrossRef]
- Larsen, F.S.; Schmidt, L.E.; Bernsmeier, C.; Rasmussen, A.; Isoniemi, H.; Patel, V.C.; Triantafyllou, E.; Bernal, W.; Auzinger, G.; Shawcross, D.; et al. High-Volume Plasma Exchange in Patients with Acute Liver Failure: An Open Randomised Controlled Trial. J. Hepatol. 2016, 64, 69–78. [Google Scholar] [CrossRef]
- Jain, V.; Dhawan, A. Prognostic Modeling in Pediatric Acute Liver Failure. Liver Transpl. 2016, 22, 1418–1430. [Google Scholar] [CrossRef]
- Kumar, R.; Shalimar; Sharma, H.; Goyal, R.; Kumar, A.; Khanal, S.; Prakash, S.; Gupta, S.D.; Panda, S.K.; Acharya, S.K. Prospective Derivation and Validation of Early Dynamic Model for Predicting Outcome in Patients with Acute Liver Failure. Gut 2012, 61, 1068–1075. [Google Scholar] [CrossRef]
- Kumar, R.; Shalimar; Bhatia, V.; Khanal, S.; Sreenivas, V.; Gupta, S.D.; Panda, S.K.; Acharya, S.K. Antituberculosis Therapy–Induced Acute Liver Failure: Magnitude, Profile, Prognosis, and Predictors of Outcome. Hepatology 2010, 51, 1665–1674. [Google Scholar] [CrossRef]
- Sanders, S.; Flaws, D.; Than, M.; Pickering, J.W.; Doust, J.; Glasziou, P. Simplification of a Scoring System Maintained Overall Accuracy but Decreased the Proportion Classified as Low Risk. J. Clin. Epidemiol. 2016, 69, 32–39. [Google Scholar] [CrossRef]
- Gomez, D.; Cameron, I.C. Prognostic Scores for Colorectal Liver Metastasis: Clinically Important or an Academic Exercise? HPB 2010, 12, 227–238. [Google Scholar] [CrossRef] [Green Version]
- Cao, Z.; Li, F.; Xiang, X.; Liu, K.; Liu, Y.; Tang, W.; Lin, L.; Guo, Q.; Bao, S.; Xie, Q.; et al. Circulating Cell Death Biomarker: Good Candidates of Prognostic Indicator for Patients with Hepatitis B Virus Related Acute-on-Chronic Liver Failure. Sci. Rep. 2015, 5, 14240. [Google Scholar] [CrossRef] [Green Version]
- Castaneda, D.; Gonzalez, A.J.; Alomari, M.; Tandon, K.; Zervos, X.B. From Hepatitis A to E: A Critical Review of Viral Hepatitis. World J. Gastroenterol. 2021, 27, 1691–1715. [Google Scholar] [CrossRef]
- Blackmore, L.; Bernal, W. Acute Liver Failure. Clin. Med. 2015, 15, 468–472. [Google Scholar] [CrossRef] [Green Version]
- Jung, D.-H.; Hwang, S.; Lim, Y.-S.; Kim, K.-H.; Ahn, C.-S.; Moon, D.-B.; Ha, T.-Y.; Song, G.-W.; Park, G.-C.; Lee, S.-G. Outcome Comparison of Liver Transplantation for Hepatitis A-Related versus Hepatitis B-Related Acute Liver Failure in Adult Recipients. Clin. Transplant. 2018, 32, e13140. [Google Scholar] [CrossRef]
- Taylor, R.M.; Davern, T.; Munoz, S.; Han, S.-H.; McGuire, B.; Larson, A.M.; Hynan, L.; Lee, W.M.; Fontana, R.J.; US Acute Liver Failure Study Group. Fulminant Hepatitis A Virus Infection in the United States: Incidence, Prognosis, and Outcomes. Hepatology 2006, 44, 1589–1597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, Q.-F.; Xiong, T.; Huang, P.; Zhong, Y.-D.; Wang, H.-L.; Yang, Y.-F. Early Predictors of Acute Hepatitis B Progression to Liver Failure. PLoS ONE 2018, 13, e0201049. [Google Scholar] [CrossRef] [PubMed]
- Ichai, P.; Samuel, D. Management of Fulminant Hepatitis B. Curr. Infect. Dis. Rep. 2019, 21, 25. [Google Scholar] [CrossRef]
- Urban, S.; Neumann-Haefelin, C.; Lampertico, P. Hepatitis D Virus in 2021: Virology, Immunology and New Treatment Approaches for a Difficult-to-Treat Disease. Gut 2021, 70, 1782–1794. [Google Scholar] [CrossRef] [PubMed]
- Kar, P.; Karna, R. A Review of the Diagnosis and Management of Hepatitis E. Curr. Treat. Options Infect. Dis. 2020, 12, 310–320. [Google Scholar] [CrossRef]
- Shalimar; Kedia, S.; Gunjan, D.; Sonika, U.; Mahapatra, S.J.; Nayak, B.; Kaur, H.; Acharya, S.K. Acute Liver Failure Due to Hepatitis E Virus Infection Is Associated with Better Survival than Other Etiologies in Indian Patients. Dig. Dis. Sci. 2017, 62, 1058–1066. [Google Scholar] [CrossRef]
- Jensen, K.O.; Angst, E.; Hetzer, F.H.; Gingert, C. Acute Cytomegalovirus Hepatitis in an Immunocompetent Host as a Reason for Upper Right Abdominal Pain. Case Rep. Gastroenterol. 2016, 10, 36–43. [Google Scholar] [CrossRef] [Green Version]
- Chávez, S.M.; Poniachik, J.M.; Urzua, Á.M.; Roblero, J.P.; Cattaneo, M.J.; Jimenez, A.P.; Carreño, L.E.; Cornejo, R.A. Acute Liver Failure Due to Herpes Simplex Virus: Diagnostic Clues and Potential Role of Plasmapheresis. Medicine 2021, 100, e27139. [Google Scholar] [CrossRef]
- Mellinger, J.L.; Rossaro, L.; Naugler, W.E.; Nadig, S.N.; Appelman, H.; Lee, W.M.; Fontana, R.J. Epstein–Barr Virus (EBV) Related Acute Liver Failure: A Case Series from the US Acute Liver Failure Study Group. Dig. Dis. Sci. 2014, 59, 1630–1637. [Google Scholar] [CrossRef]
- Kye Mon, K.; Nontprasert, A.; Kittitrakul, C.; Tangkijvanich, P.; Leowattana, W.; Poovorawan, K. Incidence and Clinical Outcome of Acute Liver Failure Caused by Dengue in a Hospital for Tropical Diseases, Thailand. Am. J. Trop. Med. Hyg. 2016, 95, 1338–1344. [Google Scholar] [CrossRef] [Green Version]
- Rovegno, M.; Vera, M.; Ruiz, A.; Benítez, C. Current Concepts in Acute Liver Failure. Ann. Hepatol. 2019, 18, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Aziz, R.; Price, J.; Agarwal, B. Management of Acute Liver Failure in Intensive Care. BJA Educ. 2021, 21, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Scott, T.R.; Kronsten, V.T.; Hughes, R.D.; Shawcross, D.L. Pathophysiology of Cerebral Oedema in Acute Liver Failure. World J. Gastroenterol. WJG 2013, 19, 9240–9255. [Google Scholar] [CrossRef] [PubMed]
- Tandon, R.; Froghi, S. Artificial Liver Support Systems. J. Gastroenterol. Hepatol. 2021, 36, 1164–1179. [Google Scholar] [CrossRef]
- Li, J.; Liang, X.; You, S.; Feng, T.; Zhou, X.; Zhu, B.; Luo, J.; Xin, J.; Jiang, J.; Shi, D.; et al. Development and Validation of a New Prognostic Score for Hepatitis B Virus-Related Acute-on-Chronic Liver Failure. J. Hepatol. 2021, 75, 1104–1115. [Google Scholar] [CrossRef]
- Wu, T.; Li, J.; Shao, L.; Xin, J.; Jiang, L.; Zhou, Q.; Shi, D.; Jiang, J.; Sun, S.; Jin, L.; et al. Development of Diagnostic Criteria and a Prognostic Score for Hepatitis B Virus-Related Acute-on-Chronic Liver Failure. Gut 2018, 67, 2181–2191. [Google Scholar] [CrossRef]
- Yantorno, S.E.; Kremers, W.K.; Ruf, A.E.; Trentadue, J.J.; Podestá, L.G.; Villamil, F.G. MELD Is Superior to King’s College and Clichy’s Criteria to Assess Prognosis in Fulminant Hepatic Failure. Liver Transplant. Off. Publ. Am. Assoc. Study Liver Dis. Int. Liver Transplant. Soc. 2007, 13, 822–828. [Google Scholar] [CrossRef]
- Dhiman, R.K.; Jain, S.; Maheshwari, U.; Bhalla, A.; Sharma, N.; Ahluwalia, J.; Duseja, A.; Chawla, Y. Early Indicators of Prognosis in Fulminant Hepatic Failure: An Assessment of the Model for End-Stage Liver Disease (MELD) and King’s College Hospital Criteria. Liver Transpl. 2007, 13, 814–821. [Google Scholar] [CrossRef]
- Katoonizadeh, A.; Decaestecker, J.; Wilmer, A.; Aerts, R.; Verslype, C.; Vansteenbergen, W.; Yap, P.; Fevery, J.; Roskams, T.; Pirenne, J.; et al. MELD Score to Predict Outcome in Adult Patients with Non-Acetaminophen-Induced Acute Liver Failure. Liver Int. Off. J. Int. Assoc. Study Liver 2007, 27, 329–334. [Google Scholar] [CrossRef]
- Bismuth, H.; Samuel, D.; Castaing, D.; Adam, R.; Saliba, F.; Johann, M.; Azoulay, D.; Ducot, B.; Chiche, L. Orthotopic Liver Transplantation in Fulminant and Subfulminant Hepatitis The Paul Brousse Experience. Ann. Surg. 1995, 222, 109. [Google Scholar] [CrossRef]
- Ichai, P.; Legeai, C.; Francoz, C.; Boudjema, K.; Boillot, O.; Ducerf, C.; Mathurin, P.; Pruvot, F.-R.; Suc, B.; Wolf, P.; et al. Patients with Acute Liver Failure Listed for Superurgent Liver Transplantation in France: Reevaluation of the Clichy-Villejuif Criteria. Liver Transpl. 2015, 21, 512–523. [Google Scholar] [CrossRef] [PubMed]
- Hadem, J.; Stiefel, P.; Bahr, M.J.; Tillmann, H.L.; Rifai, K.; Klempnauer, J.; Wedemeyer, H.; Manns, M.P.; Schneider, A.S. Prognostic Implications of Lactate, Bilirubin, and Etiology in German Patients With Acute Liver Failure. Clin. Gastroenterol. Hepatol. 2008, 6, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, A.; King, L.Y.; Hynan, L.S.; Vedvyas, C.; Lin, W.; Lee, W.M.; Chung, R.T. Development of an Accurate Index for Predicting Outcomes of Patients with Acute Liver Failure. Gastroenterology 2012, 143, 1237–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figorilli, F.; Putignano, A.; Roux, O.; Houssel-Debry, P.; Francoz, C.; Paugam-Burtz, C.; Soubrane, O.; Agarwal, B.; Durand, F.; Jalan, R. Development of an Organ Failure Score in Acute Liver Failure for Transplant Selection and Identification of Patients at High Risk of Futility. PLoS ONE 2017, 12, e0188151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McPhail, M.J.W.; Wendon, J.A.; Bernal, W. Meta-Analysis of Performance of Kings’s College Hospital Criteria in Prediction of Outcome in Non-Paracetamol-Induced Acute Liver Failure. J. Hepatol. 2010, 53, 492–499. [Google Scholar] [CrossRef]
- Kim, J.D.; Cho, E.J.; Ahn, C.; Park, S.K.; Choi, J.Y.; Lee, H.C.; Kim, D.Y.; Choi, M.S.; Wang, H.J.; Kim, I.H.; et al. A Model to Predict 1-Month Risk of Transplant or Death in Hepatitis A-Related Acute Liver Failure: Hepatology. Hepatology 2019, 70, 621–629. [Google Scholar] [CrossRef]
- Wu, J.; Shi, C.; Sheng, X.; Xu, Y.; Zhang, J.; Zhao, X.; Yu, J.; Shi, X.; Li, G.; Cao, H.; et al. Prognostic Nomogram for Patients with Hepatitis E Virus-Related Acute Liver Failure: A Multicenter Study in China. J. Clin. Transl. Hepatol. 2021, 9, 828–837. [Google Scholar] [CrossRef]
- Zhou, L.; Dong, P.-L.; Ding, H.-G. Comparison Scoring Model of Severe Viral Hepatitis and Model of End Stage Liver Disease for the Prognosis of Patients with Liver Failure in China. World J. Gastroenterol. WJG 2007, 13, 2999–3002. [Google Scholar] [CrossRef]
- Craig, D.G.N.; Reid, T.W.D.J.; Wright, E.C.; Martin, K.G.; Davidson, J.S.; Hayes, P.C.; Simpson, K.J. The Sequential Organ Failure Assessment (SOFA) Score Is Prognostically Superior to the Model for End-Stage Liver Disease (MELD) and MELD Variants Following Paracetamol (Acetaminophen) Overdose. Aliment. Pharmacol. Ther. 2012, 35, 705–713. [Google Scholar] [CrossRef]
- Cholongitas, E.; Theocharidou, E.; Vasianopoulou, P.; Betrosian, A.; Shaw, S.; Patch, D.; O’Beirne, J.; Agarwal, B.; Burroughs, A.K. Comparison of the Sequential Organ Failure Assessment Score with the King’s College Hospital Criteria and the Model for End-Stage Liver Disease Score for the Prognosis of Acetaminophen-Induced Acute Liver Failure. Liver Transplant. Off. Publ. Am. Assoc. Study Liver Dis. Int. Liver Transplant. Soc. 2012, 18, 405–412. [Google Scholar] [CrossRef]
- Mitchell, I.; Bihari, D.; Chang, R.; Wendon, J.; Williams, R. Earlier Identification of Patients at Risk from Acetaminophen-Induced Acute Liver Failure. Crit. Care Med. 1998, 26, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, V.; Singh, R.; Acharya, S.K. Predictive Value of Arterial Ammonia for Complications and Outcome in Acute Liver Failure. Gut 2006, 55, 98–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, R.; Shalimar; Sharma, H.; Prakash, S.; Panda, S.K.; Khanal, S.; Acharya, S.K. Persistent Hyperammonemia Is Associated With Complications and Poor Outcomes in Patients With Acute Liver Failure. Clin. Gastroenterol. Hepatol. 2012, 10, 925–931. [Google Scholar] [CrossRef]
- Bernal, W.; Wendon, J. More on Serum Phosphate and Prognosis of Acute Liver Failure. Hepatology 2003, 38, 533–534. [Google Scholar] [CrossRef] [PubMed]
- Chung, P.Y.; Sitrin, M.D.; Te, H.S. Serum Phosphorus Levels Predict Clinical Outcome in Fulminant Hepatic Failure. Liver Transpl. 2003, 9, 248–253. [Google Scholar] [CrossRef]
- Bernal, W. Lactate Is Important in Determining Prognosis in Acute Liver Failure. J. Hepatol. 2010, 53, 209–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taurá, P.; Martinez-Palli, G.; Martinez-Ocon, J.; Beltran, J.; Sanchez-Etayo, G.; Balust, J.; Anglada, T.; Mas, A.; Garcia-Valdecasas, J.-C. Hyperlactatemia in Patients with Non-Acetaminophen-Related Acute Liver Failure. World J. Gastroenterol. WJG 2006, 12, 1949–1953. [Google Scholar] [CrossRef]
- Schiødt, F.V.; Ostapowicz, G.; Murray, N.; Satyanarana, R.; Zaman, A.; Munoz, S.; Lee, W.M. Alpha-Fetoprotein and Prognosis in Acute Liver Failure. Liver Transpl. 2006, 12, 1776–1781. [Google Scholar] [CrossRef] [PubMed]
- Antoniades, C.G.; Berry, P.A.; Davies, E.T.; Hussain, M.; Bernal, W.; Vergani, D.; Wendon, J. Reduced Monocyte HLA-DR Expression: A Novel Biomarker of Disease Severity and Outcome in Acetaminophen-Induced Acute Liver Failure. Hepatology 2006, 44, 34–43. [Google Scholar] [CrossRef]
- Bernsmeier, C.; Triantafyllou, E.; Brenig, R.; Lebosse, F.J.; Singanayagam, A.; Patel, V.C.; Pop, O.T.; Khamri, W.; Nathwani, R.; Tidswell, R.; et al. CD14+ CD15− HLA-DR− Myeloid-Derived Suppressor Cells Impair Antimicrobial Responses in Patients with Acute-on-Chronic Liver Failure. Gut 2018, 67, 1155–1167. [Google Scholar] [CrossRef] [Green Version]
- Grama, A.; Burac, L.; Aldea, C.O.; Bulata, B.; Delean, D.; Samasca, G.; Abrudan, C.; Sirbe, C.; Pop, T.L. Vitamin D-Binding Protein (Gc-Globulin) in Acute Liver Failure in Children. Diagnostics 2020, 10, 278. [Google Scholar] [CrossRef] [PubMed]
- Schiødt, F.V.; Rossaro, L.; Stravitz, R.T.; Shakil, A.O.; Chung, R.T.; Lee, W.M.; Group, A.L.F.S. Gc-Globulin and Prognosis in Acute Liver Failure. Liver Transpl. 2005, 11, 1223–1227. [Google Scholar] [CrossRef] [PubMed]
- Oketani, M.; Uto, H.; Ido, A.; Tsubouchi, H. Management of Hepatitis B Virus-Related Acute Liver Failure. Clin. J. Gastroenterol. 2014, 7, 19–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norvell, J.P.; Blei, A.T.; Jovanovic, B.D.; Levitsky, J. Herpes Simplex Virus Hepatitis: An Analysis of the Published Literature and Institutional Cases. Liver Transpl. 2007, 13, 1428–1434. [Google Scholar] [CrossRef]
- Nakase, H.; Herfarth, H. Cytomegalovirus Colitis, Cytomegalovirus Hepatitis and Systemic Cytomegalovirus Infection: Common Features and Differences. Inflamm. Intest. Dis. 2016, 1, 15–23. [Google Scholar] [CrossRef]
- Zhang, F.; Sodroski, C.; Cha, H.; Li, Q.; Liang, T.J. Infection of Hepatocytes with HCV Increases Cell Surface Levels of Heparan Sulfate Proteoglycans, Uptake of Cholesterol and Lipoprotein, and Virus Entry by Up-Regulating SMAD6 and SMAD7. Gastroenterology 2017, 152, 257–270.e7. [Google Scholar] [CrossRef] [Green Version]
- Cosset, F.-L.; Mialon, C.; Boson, B.; Granier, C.; Denolly, S. HCV Interplay with Lipoproteins: Inside or Outside the Cells? Viruses 2020, 12, 434. [Google Scholar] [CrossRef] [Green Version]
- Sasaki-Tanaka, R.; Masuzaki, R.; Okamoto, H.; Shibata, T.; Moriyama, M.; Kogure, H.; Kanda, T. Drug Screening for Hepatitis A Virus (HAV): Nicotinamide Inhibits c-Jun Expression and HAV Replication. J. Virol. 2023, 97, e01987-22. [Google Scholar] [CrossRef]
- Primadharsini, P.P.; Nagashima, S.; Nishiyama, T.; Takahashi, M.; Murata, K.; Okamoto, H. Development of Recombinant Infectious Hepatitis E Virus Harboring the NanoKAZ Gene and Its Application in Drug Screening. J. Virol. 2022, 96, e01906-21. [Google Scholar] [CrossRef]
- Yuen, M.-F.; Lim, S.-G.; Plesniak, R.; Tsuji, K.; Janssen, H.L.A.; Pojoga, C.; Gadano, A.; Popescu, C.P.; Stepanova, T.; Asselah, T.; et al. Efficacy and Safety of Bepirovirsen in Chronic Hepatitis B Infection. N. Engl. J. Med. 2022, 387, 1957–1968. [Google Scholar] [CrossRef]
- Yang, X.; Chen, Y.; Zhang, J.; Tang, T.; Kong, Y.; Ye, F.; Zhang, X.; Liu, X.; Lin, S. Thymosin A1 Treatment Reduces Hepatic Inflammation and Inhibits Hepatocyte Apoptosis in Rats with Acute Liver Failure. Exp. Ther. Med. 2018, 15, 3231–3238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shokravi, S.; Borisov, V.; Zaman, B.A.; Niazvand, F.; Hazrati, R.; Khah, M.M.; Thangavelu, L.; Marzban, S.; Sohrabi, A.; Zamani, A. Mesenchymal Stromal Cells (MSCs) and Their Exosome in Acute Liver Failure (ALF): A Comprehensive Review. Stem Cell Res. Ther. 2022, 13, 192. [Google Scholar] [CrossRef] [PubMed]
- Paulsen, G.C.; Danziger-Isakov, L. Respiratory Viral Infections in Solid Organ and Hematopoietic Stem Cell Transplantation. Clin. Chest Med. 2017, 38, 707–726. [Google Scholar] [CrossRef] [PubMed]
- Seetharam, A. Intensive Care Management of Acute Liver Failure: Considerations While Awaiting Liver Transplantation. J. Clin. Transl. Hepatol. 2019, 7, 384–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saluja, V.; Sharma, A.; Pasupuleti, S.S.; Mitra, L.G.; Kumar, G.; Agarwal, P.M. Comparison of Prognostic Models in Acute Liver Failure: Decision Is to Be Dynamic. Indian J. Crit. Care Med. Peer-Rev. Off. Publ. Indian Soc. Crit. Care Med. 2019, 23, 574–581. [Google Scholar] [CrossRef]
- Stahl, K.; Hadem, J.; Schneider, A.; Manns, M.P.; Wiesner, O.; Schmidt, B.M.W.; Hoeper, M.M.; Busch, M.; David, S. Therapeutic Plasma Exchange in Acute Liver Failure. J. Clin. Apheresis 2019, 34, 589–597. [Google Scholar] [CrossRef] [Green Version]
- Saliba, F.; Camus, C.; Durand, F.; Mathurin, P.; Letierce, A.; Delafosse, B.; Barange, K.; Perrigault, P.F.; Belnard, M.; Ichaï, P.; et al. Albumin Dialysis with a Noncell Artificial Liver Support Device in Patients with Acute Liver Failure: A Randomized, Controlled Trial. Ann. Intern. Med. 2013, 159, 522–531. [Google Scholar] [CrossRef]
- Sponholz, C.; Matthes, K.; Rupp, D.; Backaus, W.; Klammt, S.; Karailieva, D.; Bauschke, A.; Settmacher, U.; Kohl, M.; Clemens, M.G.; et al. Molecular Adsorbent Recirculating System and Single-Pass Albumin Dialysis in Liver Failure—A Prospective, Randomised Crossover Study. Crit. Care 2016, 20, 2. [Google Scholar] [CrossRef] [Green Version]
- Ogura, Y.; Kabacam, G.; Singhal, A.; Moon, D.-B. The Role of Living Donor Liver Transplantation for Acute Liver Failure. Int. J. Surg. 2020, 82, 145–148. [Google Scholar] [CrossRef]
- Lee, C.A.; Sinha, S.; Fitzpatrick, E.; Dhawan, A. Hepatocyte Transplantation and Advancements in Alternative Cell Sources for Liver-Based Regenerative Medicine. J. Mol. Med. Berl. Ger. 2018, 96, 469–481. [Google Scholar] [CrossRef] [Green Version]
- Campsen, J.; Blei, A.T.; Emond, J.C.; Everhart, J.E.; Freise, C.E.; Lok, A.S.; Saab, S.; Wisniewski, K.A.; Trotter, J.F. Outcomes of Living Donor Liver Transplantation for Acute Liver Failure: The Adult-to-Adult Living Donor Liver Transplantation Cohort Study. Liver Transplant. 2008, 14, 1273–1280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narasimhan, G. Living Donor Liver Transplantation in India. Hepatobiliary Surg. Nutr. 2016, 5, 127–132. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Etiologies | Examples |
|---|---|
| Viral Hepatitis | Hepatitis A, B, C, D, E, cytomegalovirus, Epstein–Barr virus, herpes simplex, varicella zoster, adenovirus, dengue virus |
| Drug-induced | Acetaminophen (APAP), isoniazid, ketoconazole, nitrofurantoin, rifampin, herbal medications |
| Autoimmune Hepatitis | - |
| Metabolic Disease | Wilson’s Disease |
| Vascular Diseases of Liver | Budd-Chiari Syndrome, veno-occlusive disease of the liver |
| Pregnancy-related liver failure | Acute fatty liver of pregnancy, pre-eclampsia |
| Malignant infiltration | Breast carcinoma, hematologic malignancies |
| Toxin exposure | Mushroom, rat poison, yellow phosphorus and other toxic agents |
| Miscellaneous | Partial hepatectomy, sepsis, hemophagocytic lymphohistiocytosis, hepatic ischemia |
| (I) Based on the Availability of Effective Vaccine |
|---|
| Vaccine-preventable viruses |
| Hepatitis A |
| Hepatitis B |
| Viruses with no available vaccine |
| Hepatitis C |
| Hepatitis D |
| Hepatitis E |
| (II) Based on the immune status of the patient |
| Immune competent (although these may also occur in the immunocompromised) |
| Hepatitis A, B, C, D, E |
| Dengue virus |
| Immunocompromised |
| Herpes simplex virus (HSV-1 and HSV-2) |
| Cytomegalovirus (CMV) |
| Epstein–Barr Virus (EBV) |
| Viral Agent | Mode of Infection | Incubation Period | Factors Leading to Progression to ALF | Transplant-Free Survival (TFS) | Post-Transplant Survival | |
|---|---|---|---|---|---|---|
| 1-year | 5-years | |||||
| Hepatitis A virus [29,31,32] | Feco-oral route | 2–8 days | Old age, chronic viral hepatitis, underlying liver pathology | 57–69% | 69% | 69% |
| Hepatitis B virus [29,31,33,34] | Parenteral route | 4–26 weeks | Total bilirubin >5x upper limit of normal, HBe antigen negative status, concomitant alcohol use | 25% | 88% | 85% |
| Hepatitis C virus [29] | Parenteral route | 2–26 weeks | Uncommon | - | - | - |
| Hepatitis D [35] | Parenteral route | 2–8 weeks | Unknown Possible HBV coinfection | - | - | - |
| Hepatitis E virus [36,37] | Feco-oral route | 2–9 weeks | Poorly known causes | 55.1% | - | - |
| CMV [38] | Contact through infected body fluids: blood, urine, saliva etc. Can be transmitted parenterally | 3–12 weeks | Poorly known causes | - | - | - |
| HSV [39] | Contact with sores, saliva, surfaces in and around the mouth | 2–12 days | Poorly known causes | 20% | - | - |
| EBV [40] | Contact through infected body fluids: blood, urine, saliva etc. Can be transmitted parenterally | 4–6 weeks | Primary or secondary immunosuppression | 50% | 100% | - |
| Dengue Virus [41] | Bite of the infected Aedes Aegypti mosquito | 3–10 days | Young age ≤40 years, atypical lymphocytes >10%, platelets <50,000 per mm3 | 33.3% | - | - |
| O’Grady System [42] | Weeks from Jaundice to Encephalopathy |
|---|---|
| Hyperacute | 0–1 |
| Acute | 1–4 |
| Subacute | 4–12 |
| Bernuau System [42] | |
| Fulminant | 0–2 |
| Subfulminant | 2–12 |
| Japanese Classification (Mochida) [42] | |
| Fulminant | 0–8 days |
| Acute | Within 10 days |
| Subacute | 11 days to 8 weeks |
| Late-onset | 8–12 weeks |
| Name | Component | Limitations |
|---|---|---|
| Based on the Severity of Liver Dysfunction | ||
| MELD Score [48,49,50] | Serum Creatinine, Bilirubin, INR | -Predominantly retrospective analyses. -The use of MELD as a dynamic index has not been explored in large prospective studies. -Variable ideal discriminatory cut-off values -INR is subject to interlaboratory variation |
| Clichy Score [51,52] | Factor V levels with respect to age | -The etiology of viral ALF was predominantly hepatitis B. -Factor V is not a routinely available parameter |
| BiLE Score [53] | Bilirubin, lactate and etiology | -It is a retrospectively developed criteria. -The performance of the same was not validated prospectively. -The derivation cohort predominantly comprised of patients with ALF of indeterminate etiology |
| ALFED Score [24] | Arterial Ammonia, bilirubin, HE greater than Grade II, INR | Waiting time of 48 h may delay the selection of patients and referral for transplant. |
| ALFSG Score [54] | Coma grade, INR, bilirubin, phosphorus, and M30 levels | Major limiting factor is the use of cytokeratin-18 cleavage fragments, which are not routinely available at all centers. |
| ALF-OF score [55] | CLIF-C OF score Norepinephrine dose | Developed for patients with acetaminophen-induced ALF. Validation for viral ALF awaited. |
| Clinical Prognostic Indicator (CPI) score [49] | Age ≥ 50 years, JEI > 7 days, Grade 3 or 4 HE, cerebral edema, PT ≥ 35 s, and creatinine ≥ 1.5 mg/dL | Retrospective analysis No patient received an LT |
| Etiology-Specific Scoring Systems | ||
| King’s College Criteria [49,56] (For non-APAP) | INR, age, etiology, duration of jaundice to encephalopathy, bilirubin | Low sensitivity implies that a large number of patients who require LT would be missed by the scoring system. Static score hence does not reflect the evolving nature of ALF clinically |
| Hepatitis A related ALF [57] (ALFA) score | Age, bilirubin, INR, ammonia, creatinine and hemoglobin | Model-based on retrospectively collected data. Single-time assessment based on values on the day of diagnosis of ALF (static score) |
| ALFSG Index for Hepatitis A [32] | Serum ALT < 2600 IU/L, creatinine > 2.0 mg/dL, need for mechanical ventilation and need for vasopressors | Limited numbers for derivation cohort |
| Prognostic Nomogram for Hepatitis E [58] | Gamma-glutamyl transpeptidase, albumin, total bilirubin, urea nitrogen, creatinine, international normalized ratio, and neutrophil-to-lymphocyte ratio | Prospective validation required in larger population samples |
| Scoring model of severe viral hepatitis (SMSVH) score [59] | Clinical type, hepatic encephalopathy, serum sodium and prothrombin activity | Chronic liver failure patients were included in the derivation cohort. No details on LT available. Needs validation |
| Non-Liver related scores of organ dysfunction | ||
| Sequential Organ Failure (SOFA) Score [60,61] | P/F ratio, MAP/inotrope use, bilirubin, creatinine, platelets, GCS | Limitation of the derivation cohort to APAP-ALF Difficult to assess CNS involvement in intubated patients Not prospectively validated in viral ALF |
| Acute Physiology and Chronic Health Evaluation (APACHE) Score [61,62] | Multiple serologic and clinical markers | Limitations: score is cumbersome to calculate and is not validated for use. No additional benefit as compared to the MELD score or KCC. |
| Stand-alone serological markers | ||
| Serum arterial ammonia [63,64] | - | Waiting for 72 h to assess persistent hyperammonemia may result in delayed referral of patients for LT. Ammonia levels can be influenced by non-hepatic factors |
| Serum phosphate levels [65,66] | - | Performs poorly compared to other markers, such as lactate, in predicting the outcome Limited assessment of outcomes specifically in viral ALF patients in prior studies |
| Blood lactate [67,68] | - | Lactate shows mixed results in non-acetaminophen related ALF, with studies advocating both for and against lactate’s utility as a prognostic tool. Needs further validation in viral ALF |
| Serum alpha-fetoprotein [69] | - | Needs further validation in viral ALF |
| Research-based scores not commonly used clinically | ||
| Monocyte HLA-DR expression [70,71] | - | It is yet to be validated and is unavailable at most centers. |
| Serum Gc globulin [72,73] | - | The test is not readily available and needs validation in a larger cohort prior to use. |
| Prognostic Score | Cut-Offs | Sensitivity | Specificity | PPV | NPV | DA |
|---|---|---|---|---|---|---|
| Based on severity of liver dysfunction | ||||||
| MELD score | ≥35 | 86% | 75% | 88% | 73% | 83% |
| Clichy score | factor V level <20% in patients who were <30 years old Factor V level <30% in patients >30 years old | 69% | 50% | 64% | 55% | - |
| BiLE score | ≥6.9 | 79% | 84% | 89% | 71% | - |
| ALFED score | ≥3 | 94% | 59% | 74% | 90% | 78% |
| ≥4 | 90% | 80% | 85% | 87% | 86% | |
| ≥5 | 70% | 93% | 93% | 71% | 80% | |
| ALFSG score | 84.7% | 59.2% | - | - | 74.6% | |
| ALF Organ Failure (ALF-OF) score | 5.58 | 82.6% | 89.5% | 82.6% | 89.5% | - |
| Clinical Prognostic Indicator (CPI) score | 1 | 100% | 9.6% | 66.2% | 100% | 67.4% |
| 2 | 97.8% | 42.3% | 75% | 91.7% | 77.8% | |
| 3 | 73.9% | 86.5% | 90.7% | 65.2% | 78.5% | |
| 4 | 30.4% | 100% | 100% | 44.8% | 55.6% | |
| Etiology-specific scoring systems | ||||||
| King’s college criteria (KCC) | - | 58.2% | 100% | - | - | 27.7% |
| ALFSG Index for Hepatitis A | ≥1 Factor | 100% | 56% | 65% | 100% | - |
| ≥2 Factor | 92% | 88% | 86% | 93% | - | |
| ≥3 Factor | 62% | 94% | 89% | 75% | - | |
| ≥4 Factor | 8% | 100% | 100% | 57% | - | |
| Scoring model of severe viral hepatitis (SMSVH) | 5 | 77.7% | 88.0% | - | - | - |
| Non-liver related scores of organ dysfunction | ||||||
| Sequential Organ Failure (SOFA) Score | >6 by 72 h or >7 by 96 h | 90% | 69% | 96.9% | 98.8% | - |
| Acute Physiology and Chronic Health Evaluation (APACHE) Score | >15 | 82% | 98% | - | - | - |
| Standalone serological markers | ||||||
| Serum arterial ammonia | Baseline arterial ammonia > 124 mol/L | 78.6% | 76.3% | - | - | 77.5% |
| Serum phosphate levels | Level of 1.2 mmol/L at 48 to 96 h after acetamenophen overdose | 89% | 100% | 100% | 98% | - |
| Blood lactate | Post-resuscitation arterial lactate cut-off 3.0 mmol/L | 76% | 97% | - | - | - |
| Serum alpha-fetoprotein | The ratio of AFP level on day 3 as compared to day 1 was >1 in 71% of survivors as compared to <1 in 80% of non-survivors. | - | - | - | - | - |
| Research based scores which are not commonly used clinically | ||||||
| Monocyte HLA-DR expression | Monocyte HLA-DR expression 15% or less | 96% | 98% | - | - | 100% |
| Serum Gc globulin | Cut-off level of 80 mg/L | 49% | 90% | 85% | 43% | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biswas, S.; Kumar, R.; Acharya, S.K.; Shalimar. Prognostic Scores in Acute Liver Failure Due to Viral Hepatitis. Diagnostics 2023, 13, 1035. https://doi.org/10.3390/diagnostics13061035
Biswas S, Kumar R, Acharya SK, Shalimar. Prognostic Scores in Acute Liver Failure Due to Viral Hepatitis. Diagnostics. 2023; 13(6):1035. https://doi.org/10.3390/diagnostics13061035
Chicago/Turabian StyleBiswas, Sagnik, Ramesh Kumar, Subrat Kumar Acharya, and Shalimar. 2023. "Prognostic Scores in Acute Liver Failure Due to Viral Hepatitis" Diagnostics 13, no. 6: 1035. https://doi.org/10.3390/diagnostics13061035