
The Importance of Immunohistochemistry in the Evaluation of Tumor Depth of Primary Cutaneous Melanoma


Abstract
:1. Introduction
2. Materials and Methods
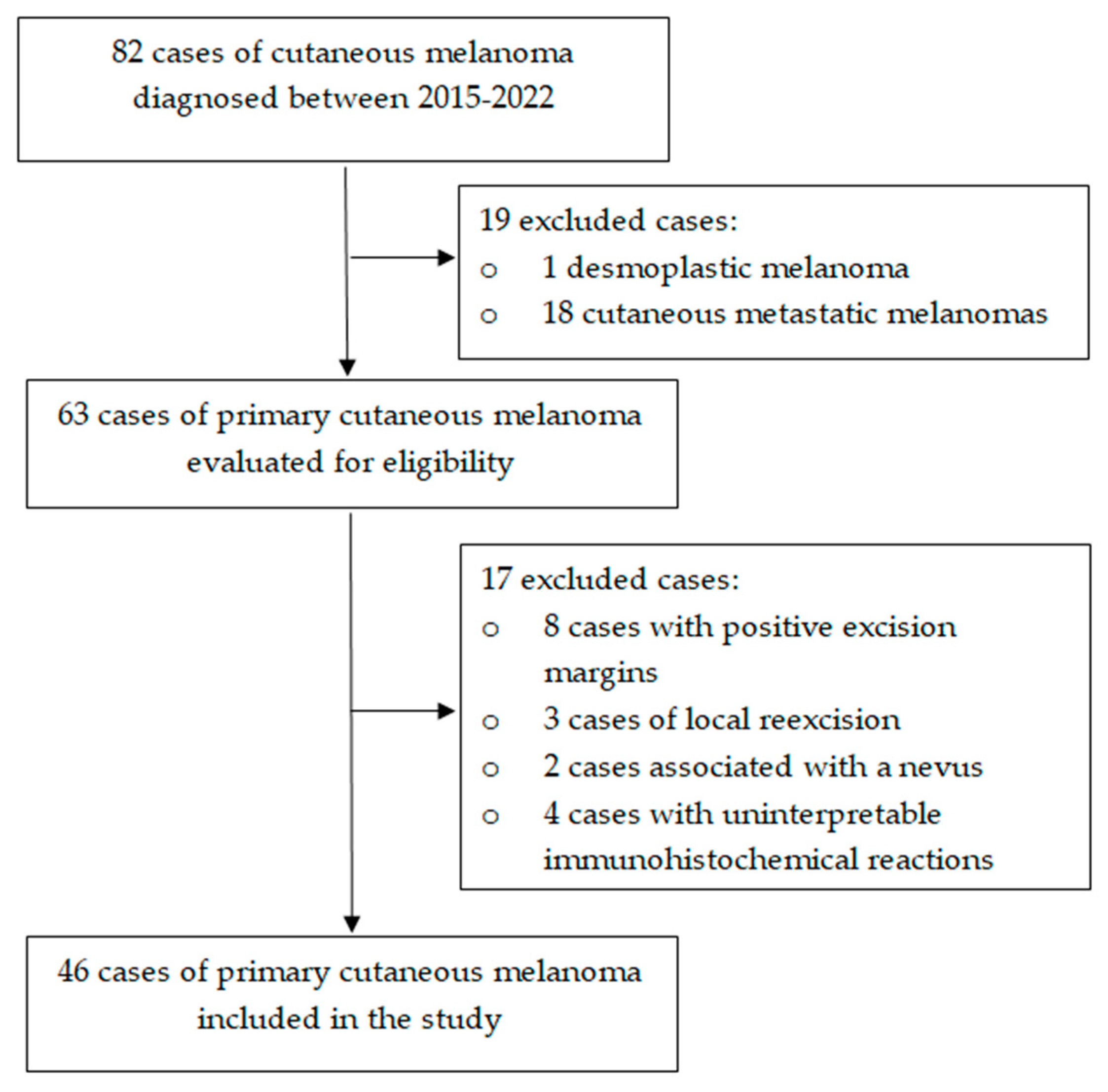
2.1. Study Design and Case Selection
2.2. Histopathologic Evaluation of the Specimens
2.3. Statistical Analysis
3. Results
4. Discussion
Strenghts, Limitations, and Future Research Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Davey, M.G.; Miller, N.; McInerney, N.M. A Review of Epidemiology and Cancer Biology of Malignant Melanoma. Cureus 2021, 13, e15087. [Google Scholar] [CrossRef] [PubMed]
- Hessler, M.; Jalilian, E.; Xu, Q.; Reddy, S.; Horton, L.; Elkin, K.; Manwar, R.; Tsoukas, M.; Mehregan, D.; Avanaki, K. Melanoma Biomarkers and Their Potential Application for In Vivo Diagnostic Imaging Modalities. Int. J. Mol. Sci. 2020, 21, 9583. [Google Scholar] [CrossRef]
- Lideikaitė, A.; Mozūraitienė, J.; Letautienė, S. Analysis of prognostic factors for melanoma patients. Acta Med. Litu. 2017, 24, 25–34. [Google Scholar] [CrossRef]
- Conforti, C.; Zalaudek, I. Epidemiology and Risk Factors of Melanoma: A Review. Dermatol. Pract. Concept. 2021, 11, e2021161S. [Google Scholar] [CrossRef]
- Hartman, R.I.; Lin, J.Y. Cutaneous Melanoma-A Review in Detection, Staging, and Management. Hematol. Oncol. Clin. N. Am. 2019, 33, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Eddy, K.; Chen, S. Overcoming Immune Evasion in Melanoma. Int. J. Mol. Sci. 2020, 21, 8984. [Google Scholar] [CrossRef] [PubMed]
- Damsky, W.E.; Bosenberg, M. Melanocytic nevi and melanoma: Unraveling a complex relationship. Oncogene 2017, 36, 5771–5792. [Google Scholar] [CrossRef] [Green Version]
- Strashilov, S.; Yordanov, A. Aetiology and Pathogenesis of Cutaneous Melanoma: Current Concepts and Advances. Int. J. Mol. Sci. 2021, 22, 6395. [Google Scholar] [CrossRef] [PubMed]
- Cherobin, A.C.F.P.; Wainstein, A.J.A.; Colosimo, E.A.; Goulart, E.M.A.; Bittencourt, F.V. Prognostic factors for metastasis in cutaneous melanoma. An. Bras. Dermatol. 2018, 93, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Lee, T.L.; Liao, Y.H.; Liau, J.Y.; Sheen, Y.S. Risk factors of recurrence and distant metastasis in primary cutaneous melanoma in Taiwan. Sci. Rep. 2021, 11, 21012. [Google Scholar] [CrossRef]
- Bax, M.J.; Johnson, T.M.; Harms, P.W.; Schwartz, J.L.; Zhao, L.; Fullen, D.R.; Chan, M.P. Detection of Occult Invasion in Melanoma In Situ. JAMA Dermatol. 2016, 152, 1201–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brochez, L.; Verhaeghe, E.; Grosshans, E.; Haneke, E.; Piérard, G.; Ruiter, D.; Naeyaert, J.M. Inter-observer variation in the histopathological diagnosis of clinically suspicious pigmented skin lesions. J. Pathol. 2002, 196, 459–466. [Google Scholar] [CrossRef]
- Eriksson, H.; Frohm-Nilsson, M.; Hedblad, M.A.; Hellborg, H.; Kanter-Lewensohn, L.; Krawiec, K.; Lundh Rozell, B.; Månsson-Brahme, E.; Hansson, J. Interobserver variability of histopathological prognostic parameters in cutaneous malignant melanoma: Impact on patient management. Acta Derm. Venereol 2013, 93, 411–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bishop, J.; Tallon, B. Number of levels required to assess Breslow thickness in cutaneous invasive melanoma: An observational study. J. Cutan. Pathol. 2019, 46, 819–822. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, C.; Apalla, Z.; Manoli, S.M.; Lallas, K.; Vakirlis, E.; Lallas, A. Melanoma: Staging and Follow-Up. Dermatol. Pract. Concept. 2021, 11, e2021162S. [Google Scholar] [CrossRef] [PubMed]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. For members of the American Joint Committee on Cancer Melanoma Expert Panel and the International Melanoma Database and Discovery Platform. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadurní, M.B.; Meves, A. Breslow thickness 2.0: Why gene expression profiling is a step toward better patient selection for sentinel lymph node biopsies. Mod. Pathol. 2022, 35, 1509–1514. [Google Scholar] [CrossRef]
- Keung, E.Z.; Gershenwald, J.E. The eighth edition American Joint Committee on Cancer (AJCC) melanoma staging system: Implications for melanoma treatment and care. Expert Rev. Anticancer Ther. 2018, 18, 775–784. [Google Scholar] [CrossRef]
- Parra-Medina, R.; Morales, S.D. Diagnostic utility of epithelial and melanocitic markers with double sequential immunohistochemical staining in differentiating melanoma in situ from invasive melanoma. Ann. Diagn. Pathol. 2017, 26, 70–74. [Google Scholar] [CrossRef]
- Burton, A.L.; Gilbert, J.; Farmer, R.W.; Stromberg, A.J.; Hagendoorn, L.; Ross, M.I.; Martin, R.C., 2nd; McMasters, K.M.; Scoggins, C.R.; Callender, G.G. Regression does not predict nodal metastasis or survival in patients with cutaneous melanoma. Am. Surg. 2011, 77, 1009–1013. [Google Scholar] [CrossRef]
- Aivazian, K.; Ahmed, T.; El Sharouni, M.A.; Stretch, J.R.; Saw, R.P.M.; Spillane, A.J.; Shannon, K.F.; Ch’ng, S.; Nieweg, O.E.; Thompson, J.F.; et al. Histological regression in melanoma: Impact on sentinel lymph node status and survival. Mod. Pathol. 2021, 34, 1999–2008. [Google Scholar] [CrossRef] [PubMed]
- Kamyab-Hesary, K.; Ghanadan, A.; Balighi, K.; Mousavinia, S.F.; Nasimi, M. Immunohistochemical Staining in the Assessment of Melanoma Tumor Thickness. Pathol. Oncol. Res. 2020, 26, 885–891. [Google Scholar] [CrossRef] [PubMed]
- Drabeni, M.; Lopez-Vilaró, L.; Barranco, C.; Trevisan, G.; Gallardo, F.; Pujol, R.M. Differences in tumor thickness between hematoxylin and eosin and Melan-A immunohistochemically stained primary cutaneous melanomas. Am. J. Dermatopathol. 2013, 35, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Fu, Z.; Ji, J.; Huang, J.; Long, X. Predictive Values of Pathological and Clinical Risk Factors for Positivity of Sentinel Lymph Node Biopsy in Thin Melanoma: A Systematic Review and Meta-Analysis. Front. Oncol. 2022, 12, 817510. [Google Scholar] [CrossRef]
- Hu, Y.; Briggs, A.; Gennarelli, R.L.; Bartlett, E.K.; Ariyan, C.E.; Coit, D.G.; Brady, M.S. Sentinel Lymph Node Biopsy for T1b Melanoma: Balancing Prognostic Value and Cost. Ann. Surg. Oncol. 2020, 27, 5248–5256. [Google Scholar] [CrossRef]
- Ferrante di Ruffano, L.; Dinnes, J.; Chuchu, N.; Bayliss, S.E.; Takwoingi, Y.; Davenport, C.; Matin, R.N.; O’Sullivan, C.; Roskell, D.; Deeks, J.J.; et al. Cochrane Skin Cancer Diagnostic Test Accuracy Group. Exfoliative cytology for diagnosing basal cell carcinoma and other skin cancers in adults. Cochrane Database Syst. Rev. 2018, 12, CD013187. [Google Scholar] [CrossRef]
- Monea, M.; Olah, P.; Comaneanu, R.M.; Hancu, V.; Ormenisan, A. The Role of Toluidine Blue as a Visual Diagnostic Method in Oral Premalignant Lesions. Rev. Chim. 2016, 67, 1370–1372. [Google Scholar]
- Maurichi, A.; Miceli, R.; Camerini, T.; Mariani, L.; Patuzzo, R.; Ruggeri, R.; Gallino, G.; Tolomio, E.; Tragni, G.; Valeri, B.; et al. Prediction of survival in patients with thin melanoma: Results from a multi-institution study. J. Clin. Oncol. 2014, 32, 2479–2485. [Google Scholar] [CrossRef] [Green Version]
- Cordeiro, E.; Gervais, M.K.; Shah, P.S.; Look Hong, N.J.; Wright, F.C. Sentinel Lymph Node Biopsy in Thin Cutaneous Melanoma: A Systematic Review and Meta-Analysis. Ann. Surg. Oncol. 2016, 23, 4178–4188. [Google Scholar] [CrossRef]
- Murali, R.; Haydu, L.E.; Long, G.V.; Quinn, M.J.; Saw, R.P.; Shannon, K.; Spillane, A.J.; Stretch, J.R.; Kefford, R.F.; Thompson, J.F.; et al. Clinical and pathologic factors associated with distant metastasis and survival in patients with thin primary cutaneous melanoma. Ann. Surg. Oncol. 2012, 19, 1782–1789. [Google Scholar] [CrossRef]
- Chiaravalloti, A.J.; Jinna, S.; Kerr, P.E.; Whalen, J.; Grant-Kels, J.M. A deep look into thin melanomas: What’s new for the clinician and the impact on the patient. Int. J. Women’s Dermatol. 2018, 4, 119–121. [Google Scholar] [CrossRef] [PubMed]
- Isaksson, K.; Mikiver, R.; Eriksson, H.; Lapins, J.; Nielsen, K.; Ingvar, C.; Lyth, J. Survival in 31 670 patients with thin melanomas: A Swedish population-based study. Br. J. Dermatol. 2021, 184, 60–67. [Google Scholar] [CrossRef] [Green Version]
- Vecchiato, A.; Zonta, E.; Campana, L.; Dal Bello, G.; Rastrelli, M.; Rossi, C.R.; Alaibac, M. Long-term Survival of Patients with Invasive Ultra-thin Cutaneous Melanoma: A Single-center Retrospective Analysis. Medicine 2016, 95, e2452. [Google Scholar] [CrossRef] [PubMed]
- Richetta, A.G.; Valentini, V.; Marraffa, F.; Paolino, G.; Rizzolo, P.; Silvestri, V.; Zelli, V.; Carbone, A.; Di Mattia, C.; Calvieri, S.; et al. Metastases risk in thin cutaneous melanoma: Prognostic value of clinical-pathologic characteristics and mutation profile. Oncotarget 2018, 9, 32173–32181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo, S.N.; Scolyer, R.; Thompson, J.F. Long-Term Survival of Patients with Thin (T1) Cutaneous Melanomas: A Breslow Thickness Cut Point of 0.8 mm Separates Higher-Risk and Lower-Risk Tumors. Ann. Surg. Oncol. 2018, 25, 894–902. [Google Scholar] [CrossRef]
- Chen, T.C.; Hitchcock, M.G. Rate of Immunohistochemistry Utilization in the Diagnosis of Cutaneous Melanocytic Lesions. Am. J. Dermatopathol. 2021, 43, e146–e148. [Google Scholar] [CrossRef]
- Dinehart, M.S.; Dinehart, S.M.; Sukpraprut-Braaten, S.; High, W.A. Immunohistochemistry utilization in the diagnosis of melanoma. J. Cutan. Pathol. 2020, 47, 446–450. [Google Scholar] [CrossRef]
- Kim, R.H.; Meehan, S.A. Immunostain use in the diagnosis of melanomas referred to a tertiary medical center: A 15-year retrospective review (2001–2015). J. Cutan. Pathol. 2017, 44, 221–227. [Google Scholar] [CrossRef]
- Xia, J.; Wang, Y.; Li, F.; Wang, J.; Mu, Y.; Mei, X.; Li, X.; Zhu, W.; Jin, X.; Yu, K. Expression of microphthalmia transcription factor, S100 protein, and HMB-45 in malignant melanoma and pigmented nevi. Biomed. Rep. 2016, 5, 327–331. [Google Scholar] [CrossRef] [Green Version]
- Wilson, M.L.; Hossler, E.W.; Ferringer, T.C.; Elston, D.M. S100-negative junctional melanocytic proliferations. Am. J. DermatoPathol. 2011, 33, 327–329. [Google Scholar] [CrossRef]
- Nonaka, D.; Chiriboga, L.; Rubin, B.P. Differential expression of S100 protein subtypes in malignant melanoma, and benign and malignant peripheral nerve sheath tumors. J. Cutan. Pathol. 2008, 35, 1014–1019. [Google Scholar] [CrossRef] [PubMed]
- Wessely, A.; Steeb, T.; Berking, C.; Heppt, M.V. How Neural Crest Transcription Factors Contribute to Melanoma Heterogeneity, Cellular Plasticity, and Treatment Resistance. Int. J. Mol. Sci. 2021, 22, 5761. [Google Scholar] [CrossRef] [PubMed]
- Potterf, S.B.; Mollaaghababa, R.; Hou, L.; Southard-Smith, E.M.; Hornyak, T.J.; Arnheiter, H.; Pavan, W.J. Analysis of SOX10 function in neural crest-derived melanocyte development: SOX10-dependent transcriptional control of dopachrome tautomerase. Dev. Biol. 2001, 237, 245–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vrotsos, E.; Alexis, J. Can SOX-10 or KBA.62 Replace S100 Protein in Immunohistochemical Evaluation of Sentinel Lymph Nodes for Metastatic Melanoma? Appl. Immunohistochem. Mol. Morphol. 2016, 24, 26–29. [Google Scholar] [CrossRef]
- Dass, S.E.; Huizenga, T.; Farshchian, M.; Mehregan, D.R. Comparison of SOX-10, HMB-45, and Melan-A in Benign Melanocytic Lesions. Clin. Cosmet. Investig. Dermatol. 2021, 14, 1419–1425. [Google Scholar] [CrossRef]
- Hussein, M.R.A. HMB45 protein expression and the immunohistochemical maturation in common blue nevi: A reappraisal. An. Bras. Dermatol. 2022, 97, 387–390. [Google Scholar] [CrossRef]
- Ordóñez, N.G. Value of melanocytic-associated immunohistochemical markers in the diagnosis of malignant melanoma: A review and update. Hum. Pathol. 2014, 45, 191–205. [Google Scholar] [CrossRef]
- Megahed, M.; Schön, M.; Selimovic, D.; Schön, M.P. Reliability of diagnosis of melanoma in situ. Lancet 2002, 359, 1921–1922. [Google Scholar] [CrossRef]
- Panse, G.; McNiff, J.M. Lichenoid dermatoses with pseudomelanocytic nests vs inflamed melanoma in situ: A comparative study. J. Cutan. Pathol. 2021, 48, 745–749. [Google Scholar] [CrossRef]
- Muzumdar, S.; Argraves, M.; Kristjansson, A.; Ferenczi, K.; Dadras, S.S. A quantitative comparison between SOX10 and MART-1 immunostaining to detect melanocytic hyperplasia in chronically sun-damaged skin. J. Cutan. Pathol. 2018, 45, 263–268. [Google Scholar] [CrossRef]
- Lezcano, C.; Jungbluth, A.A.; Busam, K.J. PRAME Immunohistochemistry as an Ancillary Test for the Assessment of Melanocytic Lesions. Surg. Pathol. Clin. 2021, 14, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Kuźbicki, Ł.; Brożyna, A.A. The detectability of intraepidermal melanocytes-A narrative review of immunohistochemical studies. J. Cutan. Pathol. 2022, 49, 1074–1089. [Google Scholar] [CrossRef] [PubMed]
- Helm, T.N.; Helm, K.F. Breslow thickness determined with the use of immunohistochemical techniques could provide misleading information when used with prognostic models based on data obtained by conventional means. Am. J. Dermatopathol. 2014, 36, 757. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Frequency | |
|---|---|---|
| Histological subtype | In situ | 5 (10.9%) |
| Nodular | 26 (56.5%) | |
| Superficial spreading | 10 (21.8%) | |
| Lentigo maligna melanoma | 2 (4.3%) | |
| Acral lentiginous | 3 (6.5%) | |
| Ulceration | Present | 14 (30.4%) |
| Absent | 27 (58.7%) | |
| Not applicable | 5 (10.9%) | |
| Clark level on invasion | I | 5 (10.9%) |
| II | 11 (23.9%) | |
| III | 8 (17.4%) | |
| IV | 17 (36.9%) | |
| V | 5 (10.9%) | |
| Breslow Thickness | Staining | ||||
|---|---|---|---|---|---|
| HE | S-100 | SOX10 | HMB-45 | Melan-A | |
| In situ | 5 | 3 | 3 | 4 | 3 |
| <0.8 mm | 10 | 9 | 11 | 11 | 12 |
| 0.8–1 mm | 5 | 7 | 5 | 5 | 4 |
| >1–2 mm | 7 | 6 | 8 | 7 | 8 |
| >2–4 mm | 8 | 9 | 8 | 8 | 8 |
| >4 mm | 11 | 12 | 11 | 11 | 11 |
| Case | Localization | Histological Subtype | Breslow Thickness (mm) | Clark Level | Mitotic Rate (/mm2) | Ulceration | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| HE | S-100 | SOX10 | HMB-45 | Melan-A | ||||||
| 1 | Trunk | In situ (superficial) | 0 | 0 | 0 | 0 | 0 | I | 0 | N/A |
| 2 | Head and neck | In situ (superficial) | 0 | 0 | 0 | 0 | 0 | I | 0 | N/A |
| 3 | Head and neck | In situ (superficial) | 0 | 0 | 0 | 0 | 0 | I | 0 | N/A |
| 4 | Trunk | In situ (superficial) | 0 | 0.2 | 0.1 | 0 | 0.1 | I | 0 | N/A |
| 5 | Trunk | In situ (superficial) | 0 | 0.2 | 0.1 | 0.1 | 0.1 | I | 1 | N/A |
| 6 | Limbs | Superficial | 0.5 | 0.7 | 0.6 | 0.6 | 0.7 | II | 1 | Absent |
| 7 | Trunk | Superficial | 0.5 | 0.7 | 0.7 | 0.5 | 0.6 | II | 1 | Absent |
| 8 | Head and neck | Superficial | 0.5 | 0.7 | 0.7 | 0.5 | 0.6 | II | 1 | Absent |
| 9 | Trunk | Lentigo maligna | 0.6 | 0.7 | 0.7 | 0.7 | 0.7 | II | 1 | Absent |
| 10 | Limbs | Nodular | 0.6 | 0.7 | 0.8 | 0.6 | 0.7 | III | 2 | Absent |
| 11 | Head and neck | Superficial | 0.6 | 0.7 | 0.7 | 0.7 | 0.7 | II | 1 | Absent |
| 12 | Trunk | Superficial | 0.6 | 0.8 | 0.6 | 0.6 | 0.7 | III | 1 | Absent |
| 13 | Limbs | Nodular | 0.7 | 0.8 | 0.7 | 0.7 | 0.8 | III | 2 | Absent |
| 14 | Trunk | Superficial | 0.6 | 0.9 | 0.8 | 0.7 | 0.7 | II | 1 | Absent |
| 15 | Trunk | Nodular | 0.7 | 1 | 1 | 0.9 | 0.9 | II | 2 | Absent |
| 16 | Head and neck | Lentigo maligna | 0.8 | 1.1 | 0.7 | 0.9 | 0.7 | II | 1 | Absent |
| 17 | Head and neck | Superficial | 0.8 | 0.7 | 0.7 | 0.7 | 0.7 | II | 3 | Absent |
| 18 | Trunk | Nodular | 0.9 | 1.1 | 1.1 | 0.9 | 1.1 | III | 2 | Absent |
| 19 | Head and neck | Nodular | 0.9 | 0.9 | 0.9 | 0.8 | 0.9 | II | 1 | Absent |
| 20 | Limbs | Nodular | 1 | 1 | 1.1 | 0.9 | 1 | II | 2 | Absent |
| 21 | Trunk | Superficial | 1.1 | 1 | 1 | 1.1 | 1.1 | III | 2 | Absent |
| 22 | Trunk | Nodular | 1.4 | 1.5 | 1.6 | 1.6 | 1.5 | III | 2 | Absent |
| 23 | Limbs | Nodular | 1.6 | 1.9 | 1.8 | 1.7 | 1.8 | III | 4 | Absent |
| 24 | Head and neck | Nodular | 1.7 | 2 | 2 | 1.7 | 1.8 | IV | 3 | Absent |
| 25 | Limbs | Nodular | 1.8 | 2.1 | 1.9 | 1.8 | 1.9 | IV | 7 | Present |
| 26 | Extremities | Nodular | 1.8 | 2.1 | 1.9 | 1.9 | 1.9 | III | 6 | Absent |
| 27 | Trunk | Superficial | 1.9 | 2.2 | 2.1 | 1.9 | 2 | IV | 3 | Absent |
| 28 | Trunk | Nodular | 2.1 | 2 | 2 | 2.1 | 2.1 | IV | 5 | Present |
| 29 | Trunk | Nodular | 2.4 | 2.5 | 2.5 | 2.3 | 2.4 | IV | 14 | Present |
| 30 | Limbs | Nodular | 2.7 | 2.9 | 2.8 | 2.8 | 2.8 | IV | 7 | Absent |
| 31 | Limbs | Nodular | 2.9 | 3.1 | 3.1 | 2.9 | 3 | IV | 8 | Absent |
| 32 | Extremities | Nodular | 3.4 | 3.7 | 3.6 | 3.3 | 3.5 | IV | 4 | Present |
| 33 | Extremities | Nodular | 3.5 | 3.7 | 3.8 | 3.6 | 3.7 | IV | 6 | Absent |
| 34 | Limbs | Nodular | 3.7 | 3.8 | 3.9 | 3.6 | 3.8 | IV | 4 | Present |
| 35 | Trunk | Nodular | 3.8 | 4.2 | 4.2 | 3.9 | 4 | IV | 2 | Absent |
| 36 | Trunk | Nodular | 4.1 | 4.2 | 4 | 4.1 | 4.1 | IV | 7 | Present |
| 37 | Trunk | Superficial | 4.7 | 4.8 | 4.8 | 4.7 | 4.8 | V | 7 | Present |
| 38 | Limbs | Nodular | 6.2 | 6.5 | 6.4 | 6.4 | 6.2 | IV | 5 | Present |
| 39 | Trunk | Nodular | 6.7 | 7.3 | 7.1 | 6.7 | 6.9 | IV | 11 | Present |
| 40 | Extremities | Acral | 7.4 | 7.6 | 7.5 | 7.3 | 7.5 | V | 4 | Present |
| 41 | Trunk | Nodular | 7.4 | 7.2 | 7.4 | 7.3 | 7.6 | IV | 6 | Absent |
| 42 | Extremities | Acral | 7.8 | 8.1 | 7.9 | 7.9 | 7.8 | V | 47 | Present |
| 43 | Extremities | Acral | 8.2 | 8.6 | 8.4 | 8.2 | 8.3 | V | 12 | Present |
| 44 | Limbs | Nodular | 8.4 | 8.8 | 8.6 | 8.4 | 8.5 | IV | 7 | Absent |
| 45 | Trunk | Nodular | 9.8 | 10.1 | 9.9 | 9.8 | 9.9 | IV | 9 | Present |
| 46 | Head and neck | Nodular | 12.6 | 12.8 | 12.7 | 12.5 | 12.6 | V | 11 | Present |
| Median of the Breslow thickness | 1.65 | 1.95 | 1.85 | 1.7 | 1.8 | |||||
| p value | <0.0001 * | |||||||||
| Comparison | p Value |
|---|---|
| HE versus S-100 | <0.001 * |
| HE versus SOX10 | <0.001 * |
| HE versus HMB-45 | >0.05 |
| HE versus Melan-A | <0.01 * |
| S-100 versus SOX10 | >0.05 |
| S-100 versus HMB-45 | <0.001 * |
| S-100 versus Melan-A | <0.05 * |
| SOX10 versus HMB-45 | <0.001 * |
| SOX10 versus Melan-A | >0.05 |
| HMB-45 versus Melan-A | <0.05 * |
| S-100 | Kappa Coefficient (95% Confidence Interval) | |||||||
| pTis | pT1a | pT1b | pT2 | pT3 | pT4 | |||
| HE | pTis | 3 | 2 | 0 | 0 | 0 | 0 | 0.601 (0.44–0.762) |
| pT1a | 0 | 6 | 4 | 0 | 0 | 0 | ||
| pT1b | 0 | 1 | 2 | 2 | 0 | 0 | ||
| pT2 | 0 | 0 | 1 | 3 | 3 | 0 | ||
| pT3 | 0 | 0 | 0 | 1 | 6 | 1 | ||
| pT4 | 0 | 0 | 0 | 0 | 0 | 11 | ||
| SOX10 | ||||||||
| pTis | pT1a | pT1b | pT2 | pT3 | pT4 | |||
| HE | pTis | 3 | 2 | 0 | 0 | 0 | 0 | 0.627 (0.467–0.786) |
| pT1a | 0 | 7 | 3 | 0 | 0 | 0 | ||
| pT1b | 0 | 2 | 1 | 2 | 0 | 0 | ||
| pT2 | 0 | 0 | 1 | 5 | 1 | 0 | ||
| pT3 | 0 | 0 | 0 | 1 | 6 | 1 | ||
| pT4 | 0 | 0 | 0 | 0 | 1 | 10 | ||
| HMB-45 | ||||||||
| pTis | pT1a | pT1b | pT2 | pT3 | pT4 | |||
| HE | pTis | 4 | 1 | 0 | 0 | 0 | 0 | 0.896 (0.799–0.993) |
| pT1a | 0 | 9 | 1 | 0 | 0 | 0 | ||
| pT1b | 0 | 1 | 4 | 0 | 0 | 0 | ||
| pT2 | 0 | 0 | 0 | 7 | 0 | 0 | ||
| pT3 | 0 | 0 | 0 | 0 | 8 | 0 | ||
| pT4 | 0 | 0 | 0 | 0 | 0 | 11 | ||
| Melan-A | ||||||||
| pTis | pT1a | pT1b | pT2 | pT3 | pT4 | |||
| HE | pTis | 3 | 2 | 0 | 0 | 0 | 0 | 0.813 (0.687–0.939) |
| pT1a | 0 | 8 | 2 | 0 | 0 | 0 | ||
| pT1b | 0 | 2 | 2 | 1 | 0 | 0 | ||
| pT2 | 0 | 0 | 0 | 7 | 0 | 0 | ||
| pT3 | 0 | 0 | 0 | 0 | 8 | 0 | ||
| pT4 | 0 | 0 | 0 | 0 | 0 | 11 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pop, A.M.; Monea, M.; Olah, P.; Moraru, R.; Cotoi, O.S. The Importance of Immunohistochemistry in the Evaluation of Tumor Depth of Primary Cutaneous Melanoma. Diagnostics 2023, 13, 1020. https://doi.org/10.3390/diagnostics13061020
Pop AM, Monea M, Olah P, Moraru R, Cotoi OS. The Importance of Immunohistochemistry in the Evaluation of Tumor Depth of Primary Cutaneous Melanoma. Diagnostics. 2023; 13(6):1020. https://doi.org/10.3390/diagnostics13061020
Chicago/Turabian StylePop, Anca Maria, Monica Monea, Peter Olah, Raluca Moraru, and Ovidiu Simion Cotoi. 2023. "The Importance of Immunohistochemistry in the Evaluation of Tumor Depth of Primary Cutaneous Melanoma" Diagnostics 13, no. 6: 1020. https://doi.org/10.3390/diagnostics13061020