
[18F]FDG PET/CT in the Evaluation of Melanoma Patients Treated with Immunotherapy
 , ,
, ,
Abstract
:1. Introduction
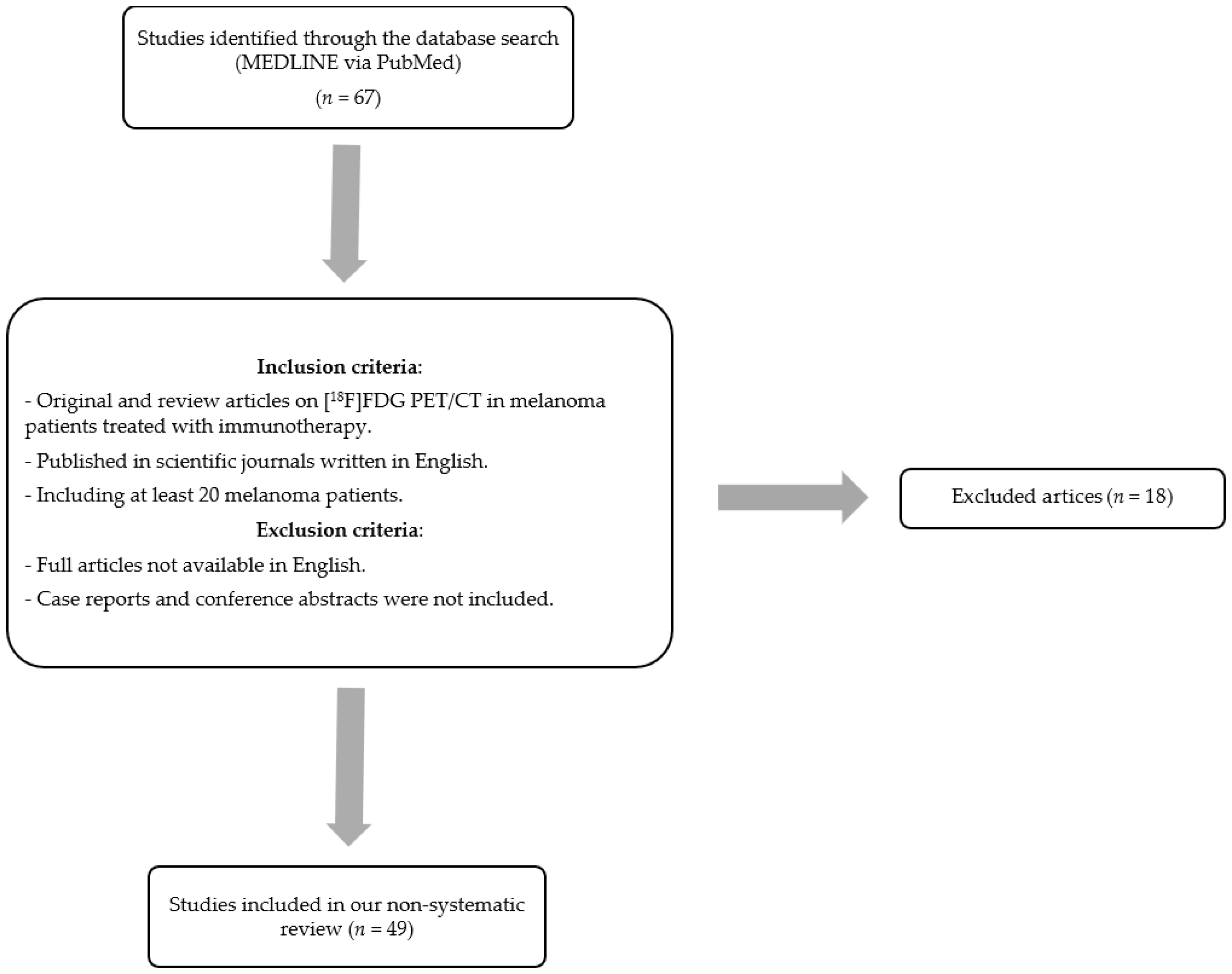
2. Materials and Methods
3. Evaluation Criteria for Response Assessment
4. Distinguishing between “Atypical” Response Patterns
4.1. Pseudoprogressive Disease (PPD)
4.2. Hyperprogressive Disease (HPD)
4.3. Dissociated Response (DR)
4.4. Sustained Response (SR)
5. Application of PET Biomarkers as Predictive and Response Evaluation Parameters
5.1. Analysis Focused on the Baseline [18F]FDG PET/CT
5.2. Analysis Focused on the Interval Changes between Baseline and Follow-Up [18F]FDG PET/CT
6. Diagnosis and Management of Immunorelated Adverse Effects
6.1. Nodal Activation and Sarcoid-like Reaction
6.2. Reactive Bone Marrow
6.3. Splenic Activity
6.4. Thyroiditis
6.5. Pneumonitis
6.6. Colitis
6.7. Hepatitis
6.8. Pancreatitis
6.9. Hypophysitis
6.10. Skin and Soft Tissue
7. Discussion
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wouters, M.W.; Michielin, O.; Bastiaannet, E.; Beishon, M.; Catalano, O.; del Marmol, V.; Delgado-Bolton, R.; Dendale, R.; Trill, M.D.; Ferrari, A.; et al. ECCO essential requirements for quality cancer care: Melanoma. Crit. Rev. Oncol. Hematol. 2018, 122, 164–178. [Google Scholar] [CrossRef] [PubMed]
- Rasilla, J.M.; Arboniés, J.C.; Bolton, R.D.; Pereyra, L.I.; Andía, G.S.; Soriano, A.P.; Fernández, R.A.; Martínez, J.M.; Gutiérrez, L.L.; Maté, A.G.; et al. SPECT-CT in sentinel node detection in patients with melanoma. Rev. Esp. Med. Nucl. 2009, 28, 229–234. [Google Scholar] [CrossRef]
- Jiménez-Requena, F.; Delgado-Bolton, R.C.; Fernández-Pérez, C.; Gambhir, S.S.; Schwimmer, J.; Pérez-Vázquez, J.M.; Carreras-Delgado, J.L. Meta-analysis of the performance of 18F-FDG PET in cutaneous melanoma. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 284–300. [Google Scholar] [CrossRef]
- Ayati, N.; Sadeghi, R.; Kiamanesh, Z.; Lee, S.T.; Zakavi, S.R.; Scott, A.M. The value of 18F-FDG PET/CT for predicting or monitoring immunotherapy response in patients with metastatic melanoma: A systematic review and meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 428–448. [Google Scholar] [CrossRef] [PubMed]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.G.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef]
- Lopci, E.; Hicks, R.J.; Dimitrakopoulou-Strauss, A.; Dercle, L.; Iravani, A.; Seban, R.D.; Sachpekidis, C.; Humbert, O.; Gheysens, O.; Glaudemans, A.W.J.M.; et al. Joint EANM/SNMMI/ANZSNM practice guidelines/procedure standards on recommended use of [18F]FDG PET/CT imaging during immunomodulatory treatments in patients with solid tumors version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 2323–2341. [Google Scholar] [CrossRef]
- Lopci, E.; Aide, N.; Dimitrakopoulou-Strauss, A.; Dercle, L.; Iravani, A.; Seban, R.D.; Sachpekidis, C.; Humbert, O.; Gheysens, O.; Glaudemans, A.W.J.M.; et al. Perspectives on joint EANM/SNMMI/ANZSNM practice guidelines/procedure standards for [18F]FDG PET/CT imaging during immunomodulatory treatments in patients with solid tumors. Cancer Imaging 2022, 22, 73. [Google Scholar] [CrossRef] [PubMed]
- Lopci, E. Immunotherapy Monitoring with Immune Checkpoint Inhibitors Based on [18F]FDG PET/CT in Metastatic Melanomas and Lung Cancer. J. Clin. Med. 2021, 10, 5160. [Google Scholar] [CrossRef]
- Young, H.; Baum, R.; Cremerius, U.; Herholz, K.; Hoekstra, O.; Lammertsma, A.; Pruim, J.; Price, P. Measurement of clinical and subclinical tumour response using [18F]-fluorodeoxyglucose and positron emission tomography: Review and 1999 EORTC recommendations. Eur. J. Cancer 1999, 35, 1773–1782. [Google Scholar] [CrossRef]
- Wahl, R.L.; Jacene, H.; Kasamon, Y.; Lodge, M.A. From RECIST to PERCIST: Evolving Considerations for PET Response Criteria in Solid Tumors. J. Nucl. Med. 2009, 50 (Suppl. S1), 122S–150S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, S.Y.; Lipson, E.J.; Im, H.-J.; Rowe, S.P.; Gonzalez, E.M.; Blackford, A.; Chirindel, A.; Pardoll, D.M.; Topalian, S.L.; Wahl, R.L. Prediction of Response to Immune Checkpoint Inhibitor Therapy Using Early-Time-Point18F-FDG PET/CT Imaging in Patients with Advanced Melanoma. J. Nucl. Med. 2017, 58, 1421–1428. [Google Scholar] [CrossRef] [Green Version]
- Anwar, H.; Sachpekidis, C.; Winkler, J.; Kopp-Schneider, A.; Haberkorn, U.; Hassel, J.C.; Dimitrakopoulou-Strauss, A. Absolute number of new lesions on 18F-FDG PET/CT is more predictive of clinical response than SUV changes in metastatic melanoma patients receiving ipilimumab. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 376–383. [Google Scholar] [CrossRef]
- Goldfarb, L.; Duchemann, B.; Chouahnia, K.; Zelek, L.; Soussan, M. Monitoring anti-PD-1-based immunotherapy in non-small cell lung cancer with FDG PET: Introduction of iPERCIST. EJNMMI Res. 2019, 9, 8. [Google Scholar] [CrossRef]
- Ito, K.; Teng, R.; Schöder, H.; Humm, J.L.; Ni, A.; Michaud, L.; Nakajima, R.; Yamashita, R.; Wolchok, J.D.; Weber, W.A. 18F-FDG PET/CT for Monitoring of Ipilimumab Therapy in Patients with Metastatic Melanoma. J. Nucl. Med. 2019, 60, 335–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seymour, L.; Bogaerts, J.; Perrone, A.; Ford, R.; Schwartz, L.H.; Mandrekar, S.; Lin, N.U.; Litière, S.; Dancey, J.; Chen, A.; et al. iRECIST: Guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol. 2017, 18, e143–e152, Erratum in Lancet Oncol. 2019, 20, e242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leon-Mateos, L.; Garcia-Velloso, M.J.; García-Figueiras, R.; Rodriguez-Moreno, J.F.; Vercher-Conejero, J.L.; Sánchez, M.; Gracia, J.L.P.; Simo-Perdigo, M.; Gorospe, L. A multidisciplinary consensus on the morphological and functional responses to immunotherapy treatment. Clin. Transl. Oncol. 2021, 23, 434–449. [Google Scholar] [CrossRef] [PubMed]
- Jia, W.; Gao, Q.; Han, A.; Zhu, H.; Yu, J. The potential mechanism, recognition and clinical significance of tumor pseudoprogression after immunotherapy. Cancer Biol. Med. 2019, 16, 655–670. [Google Scholar] [CrossRef]
- Di Giacomo, A.M.; Danielli, R.; Guidoboni, M.; Calabro’, L.; Carlucci, D.; Miracco, C.; Volterrani, L.; Mazzei, M.A.; Biagioli, M.; Altomonte, M.; et al. Therapeutic efficacy of ipilimumab, an anti-CTLA-4 monoclonal antibody, in patients with metastatic melanoma unresponsive to prior systemic treatments: Clinical and immunological evidence from three patient cases. Cancer Immunol. Immunother. 2009, 58, 1297–1306. [Google Scholar] [CrossRef] [PubMed]
- Simó-Perdigó, M.; Vercher-Conejero, J.; Viteri, S.; García-Velloso, M. Inmunoterapia, cáncer y PET. Rev. Esp. Med. Nucl. Imagen. Mol. 2021, 40, 123–135. [Google Scholar] [CrossRef]
- Lewis, G.D.; Jonasch, E.; Shah, A.Y.; Fuller, G.N.; Farach, A.M.; Butler, E.B.; Teh, B.S. Renal cell carcinoma brain metastasis with pseudoprogression and radiation necrosis on nivolumab after previous treatment with stereotactic radiosurgery: An illustrative case report and review of the literature. Pr. Radiat. Oncol. 2018, 8, e262–e265. [Google Scholar] [CrossRef]
- Champiat, S.; Dercle, L.; Ammari, S.; Massard, C.; Hollebecque, A.; Postel-Vinay, S.; Chaput, N.; Eggermont, A.M.; Marabelle, A.; Soria, J.-C.; et al. Hyperprogressive Disease Is a New Pattern of Progression in Cancer Patients Treated by Anti-PD-1/PD-L1. Clin. Cancer Res. 2017, 23, 1920–1928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, M.; Vanneste, B.G.L.; Yu, Q.; Chen, Z.; Peng, J.; Cai, X. Hyperprogression under immunotherapy: A new form of immunotherapy response?—A narrative literature review. Transl. Lung Cancer Res. 2021, 10, 3276–3291. [Google Scholar] [CrossRef]
- Humbert, O.; Chardin, D. Dissociated Response in Metastatic Cancer: An Atypical Pattern Brought Into the Spotlight With Immunotherapy. Front. Oncol. 2020, 10, 566297. [Google Scholar] [CrossRef]
- Bernard-Tessier, A.; Baldini, C.; Castanon, E.; Martin, P.; Champiat, S.; Hollebecque, A.; Postel-Vinay, S.; Varga, A.; Bahleda, R.; Gazzah, A.; et al. Patterns of progression in patients treated for immuno-oncology antibodies combination. Cancer Immunol. Immunother. 2021, 70, 221–232. [Google Scholar] [CrossRef] [PubMed]
- Borcoman, E.; Kanjanapan, Y.; Champiat, S.; Kato, S.; Servois, V.; Kurzrock, R.; Goel, S.; Bedard, P.; Le Tourneau, C. Novel patterns of response under immunotherapy. Ann. Oncol. 2019, 30, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Klemen, N.; Wang, M.; Feingold, P.L.; Cooper, K.; Pavri, S.N.; Han, D.; Detterbeck, F.C.; Boffa, D.J.; Khan, S.A.; Olino, K.; et al. Patterns of failure after immunotherapy with checkpoint inhibitors predict durable progression-free survival after local therapy for metastatic melanoma. J. Immunother. Cancer 2019, 7, 196. [Google Scholar] [CrossRef] [Green Version]
- Wolchok, J.D.; Hoos, A.; O’Day, S.; Weber, J.S.; Hamid, O.; Lebbé, C.; Maio, M.; Binder, M.; Bohnsack, O.; Nichol, G.; et al. Guidelines for the Evaluation of Immune Therapy Activity in Solid Tumors: Immune-Related Response Criteria. Clin. Cancer Res. 2009, 15, 7412–7420. [Google Scholar] [CrossRef] [Green Version]
- Pons-Tostivint, E.; Latouche, A.; Vaflard, P.; Ricci, F.; Loirat, D.; Hescot, S.; Sablin, M.-P.; Rouzier, R.; Kamal, M.; Morel, C.; et al. Comparative Analysis of Durable Responses on Immune Checkpoint Inhibitors Versus Other Systemic Therapies: A Pooled Analysis of Phase III Trials. JCO Precis. Oncol. 2019, 3, 1–10. [Google Scholar] [CrossRef]
- Seban, R.-D.; Nemer, J.S.; Marabelle, A.; Yeh, R.; Deutsch, E.; Ammari, S.; Moya-Plana, A.; Mokrane, F.-Z.; Gartrell, R.D.; Finkel, G.; et al. Prognostic and theranostic 18F-FDG PET biomarkers for anti-PD1 immunotherapy in metastatic melanoma: Association with outcome and transcriptomics. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2298–2310. [Google Scholar] [CrossRef]
- Ito, K.; Schöder, H.; Teng, R.; Humm, J.L.; Ni, A.; Wolchok, J.D.; Weber, W.A. Prognostic value of baseline metabolic tumor volume measured on 18F-fluorodeoxyglucose positron emission tomography/computed tomography in melanoma patients treated with ipilimumab therapy. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 930–939. [Google Scholar] [CrossRef]
- Sanli, Y.; Leake, J.; Odu, A.; Xi, Y.; Subramaniam, R.M. Tumor Heterogeneity on FDG PET/CT and Immunotherapy: An Imaging Biomarker for Predicting Treatment Response in Patients With Metastatic Melanoma. Am. J. Roentgenol. 2019, 212, 1318–1326. [Google Scholar] [CrossRef]
- Nobashi, T.; Baratto, L.; Reddy, S.A.; Srinivas, S.; Toriihara, A.; Hatami, N.; Yohannan, T.K.; Mittra, E. Predicting Response to Immunotherapy by Evaluating Tumors, Lymphoid Cell-Rich Organs, and Immune-Related Adverse Events Using FDG-PET/CT. Clin. Nucl. Med. 2019, 44, e272–e279. [Google Scholar] [CrossRef] [PubMed]
- Nakamoto, R.; Zaba, L.C.; Rosenberg, J.; Reddy, S.A.; Nobashi, T.W.; Davidzon, G.; Aparici, C.M.; Nguyen, J.; Moradi, F.; Iagaru, A.; et al. Prognostic value of volumetric PET parameters at early response evaluation in melanoma patients treated with immunotherapy. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2787–2795. [Google Scholar] [CrossRef] [PubMed]
- Seban, R.-D.; Moya-Plana, A.; Antonios, L.; Yeh, R.; Marabelle, A.; Deutsch, E.; Schwartz, L.H.; Gómez, R.G.H.; Saenger, Y.; Robert, C.; et al. Prognostic 18F-FDG PET biomarkers in metastatic mucosal and cutaneous melanoma treated with immune checkpoint inhibitors targeting PD-1 and CTLA-4. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2301–2312. [Google Scholar] [CrossRef]
- Wong, A.; Callahan, J.; Keyaerts, M.; Neyns, B.; Mangana, J.; Aberle, S.; Herschtal, A.; Fullerton, S.; Milne, D.; Iravani, A.; et al. 18F-FDG PET/CT based spleen to liver ratio associates with clinical outcome to ipilimumab in patients with metastatic melanoma. Cancer Imaging 2020, 20, 36. [Google Scholar] [CrossRef]
- Flaus, A.; Habouzit, V.; De Leiris, N.; Vuillez, J.P.; Leccia, M.T.; Perrot, J.L.; Prevot, N.; Cachin, F. FDG PET biomarkers for prediction of survival in metastatic melanoma prior to anti-PD1 immunotherapy. Sci. Rep. 2021, 11, 18795. [Google Scholar] [CrossRef]
- Nakamoto, R.; Zaba, L.C.; Liang, T.; Reddy, S.A.; Davidzon, G.; Aparici, C.M.; Nguyen, J.; Moradi, F.; Iagaru, A.; Franc, B.L. Prognostic Value of Bone Marrow Metabolism on Pretreatment 18F-FDG PET/CT in Patients with Metastatic Melanoma Treated with Anti-PD-1 Therapy. J. Nucl. Med. 2021, 62, 1380–1383. [Google Scholar] [CrossRef] [PubMed]
- Sachpekidis, C.; Kopp-Schneider, A.; Hassel, J.C.; Dimitrakopoulou-Strauss, A. Assessment of early metabolic progression in melanoma patients under immunotherapy: An 18F-FDG PET/CT study. EJNMMI Res. 2021, 11, 89. [Google Scholar] [CrossRef]
- Schweighofer-Zwink, G.; Manafi-Farid, R.; Kölblinger, P.; Hehenwarter, L.; Harsini, S.; Pirich, C.; Beheshti, M. Prognostic value of 2-[18F]FDG PET-CT in metastatic melanoma patients receiving immunotherapy. Eur. J. Radiol. 2022, 146, 110107. [Google Scholar] [CrossRef]
- Kaplan, R.N.; Riba, R.D.; Zacharoulis, S.; Bramley, A.H.; Vincent, L.; Costa, C.; MacDonald, D.D.; Jin, D.K.; Shido, K.; Kerns, S.A.; et al. VEGFR1-positive haematopoietic bone marrow progenitors initiate the pre-metastatic niche. Nature 2005, 438, 820–827. [Google Scholar] [CrossRef] [Green Version]
- Hiratsuka, S.; Nakamura, K.; Iwai, S.; Murakami, M.; Itoh, T.; Kijima, H.; Shipley, J.; Senior, R.M.; Shibuya, M. MMP9 induction by vascular endothelial growth factor receptor-1 is involved in lung-specific metastasis. Cancer Cell 2002, 2, 289–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, A.C.; Emmett, L.; Lo, S.; Liu, V.; Kapoor, R.; Carlino, M.S.; Guminski, A.D.; Long, G.V.; Menzies, A.M. FDG-PET response and outcome from anti-PD-1 therapy in metastatic melanoma. Ann. Oncol. 2018, 29, 2115–2120. [Google Scholar] [CrossRef]
- Dimitriou, F.; Lo, S.; Tan, A.; Emmett, L.; Kapoor, R.; Carlino, M.; Long, G.; Menzies, A. FDG-PET to predict long-term outcome from anti-PD-1 therapy in metastatic melanoma. Ann. Oncol. 2022, 33, 99–106. [Google Scholar] [CrossRef]
- Thomssen, C. Management of immune-related adverse events (irAEs)-what needs to be respected? Gynakologe 2022, 55, 344–350. [Google Scholar] [CrossRef]
- De Britto Evangelista, G.F.; Figueiredo, A.B.; de Barros E Silva, M.J.; Gollob, K.J. Balancing the good and the bad: Controlling immune-related adverse events versus anti-tumor responses in cancer patients treated with immune checkpoint inhibitors. Immunother. Adv. 2022, 2, ltac008. [Google Scholar] [CrossRef]
- Cherk, M.H.; Nadebaum, D.P.; Barber, T.W.; Beech, P.; Haydon, A.; Yap, K.S. 18F-FDG PET/CT features of immune-related adverse events and pitfalls following immunotherapy. J. Med. Imaging Radiat. Oncol. 2022, 66, 483–494. [Google Scholar] [CrossRef]
- Pennock, G.K.; Waterfield, W.; Wolchok, J.D. Patient Responses to Ipilimumab, a Novel Immunopotentiator for Metastatic Melanoma: How different are these from conventional treatment responses? Am. J. Clin. Oncol. 2012, 35, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Sachpekidis, C.; Kopp-Schneider, A.; Hakim-Meibodi, L.; Dimitrakopoulou-Strauss, A.; Hassel, J.C. 18F-FDG PET/CT longitudinal studies in patients with advanced metastatic melanoma for response evaluation of combination treatment with vemurafenib and ipilimumab. Melanoma Res. 2019, 29, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.; Dick, J.; Slynko, A.; Schulz, C.; Dimitrakopoulou-Strauss, A.; Sachpekidis, C.; Enk, A.H.; Hassel, J.C. Clinical significance of signs of autoimmune colitis in 18F-fluorodeoxyglucose positron emission tomography-computed tomography of 100 stage-IV melanoma patients. Immunotherapy 2019, 11, 667–676. [Google Scholar] [CrossRef]
- Garanzini, E.M.; Scaramuzza, D.; Spadarella, G.; Di Guardo, L.; Marchianò, A. Sarcoidosis-like disease mimicking metastases during adjuvant ipilimumab therapy in advanced melanoma patient: CT scan and MRI help in managing difficult clinical decision. BJR/Case Rep. 2020, 6, 20190065. [Google Scholar] [CrossRef] [PubMed]
- Kalisz, K.R.; Ramaiya, N.H.; Laukamp, K.R.; Gupta, A. Immune Checkpoint Inhibitor Therapy–related Pneumonitis: Patterns and Management. Radiographics 2019, 39, 1923–1937. [Google Scholar] [CrossRef] [PubMed]
- Som, A.; Mandaliya, R.; Alsaadi, D.; Farshidpour, M.; Charabaty, A.; Malhotra, N.; Mattar, M.C. Immune checkpoint inhibitor-induced colitis: A comprehensive review. World J. Clin. Cases 2019, 7, 405–418. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Design | Sample Size | Type of Immunotherapy | PET Parameters | Summary Main Findings |
|---|---|---|---|---|---|---|
| Cho et al. [11] | 2017 | Pros. * | 20 | Ipilimumab nivolumab | SUV | No statistically significant differences between SUVmax in basal and late PET |
| Anwar et al. [12] | 2018 | Pros. * | 41 | Ipilimumab | SUV | No statistically significant differences between SUVmax in basal and late PET |
| Ito et al. [30] | 2019 | Retr. # | 142 | Ipilimumab | MTV, TLG | TMTV was a strong independent prognostic factor |
| Sanli et al. [31] | 2019 | Retr. # | 34 | Anti-PD1 | SUV, MTV, TLG, TH index | Analysis showed that SUVmax, SUVpeak, gradient-based TLG and gradient-based TH index had a significant association with OS. There was no correlation between MTV and OS |
| Seban et al. [29] | 2019 | Retr. # | 55 | Anti-PD1 | SUV, MTV, TLG, HISUV, BLR, SLR | Low tumour burden (MTV) correlates with survival and objective response. Hematopoietic tissue metabolism (BLR) correlates inversely with survival |
| Nobashi et al. [32] | 2019 | Retr. # | 40 | Ipilimumab, pembrolizumab, nivolumab | SUV, MTV, TLG | There was no statistical difference for baseline SUVmax, MTV nor TLG between patients with and without clinical benefit |
| Nakamoto et al. [33] | 2020 | Retr. # | 85 | Ipilimumab, pembrolizumab, nivolumab | MTV, TLG, SUV | TMTV was a strong prognostic indicator of OS in melanoma patients |
| Seban et al. [34] | 2020 | Retr. # | 56 | PD-1, CTLA-4 | SUV, MTV, TLG, HISUV, BLR, SLR | For mucosal melanoma patients, the only prognostic imaging biomarker was SUVmax, whereas, for cutaneous melanoma patients, MTV, TLG and BLR were negatively correlated to ICI response duration |
| Wong et al. [35] | 2020 | Retr. # | 90 | Ipilimumab or anti-PD1 | SUV, MTV, SLR | Pre-treatment SLR > 1, 1 was associated with poor outcome after ipilimumab |
| Flavus et al. [36] | 2021 | Retr. # | 56 | Ipilimumab, pembrolizumab | SUV, MTV, LZE | Total MTV and LZE correlated with shorter OS |
| Nakamoto et al. [37] | 2021 | Retr. # | 92 | Ipilimumab, pembrolizumab | SUV, MTV, TLG, BLR | BLR was an independent prognostic biomarker for OS and PFS; high BLR was associated with poor progression-free and overall survival |
| Sachpekidis et al. [38] | 2021 | Retr. # | 31 | Ipilimumab, nivolumab | SLR | Patients catalogued as confirmed progressive metabolic disease had higher SLRmean after 2 cycles of treatment than those catalogued as pseudoprogression |
| Schweighofer-Zwink et al. [39] | 2021 | Retr. # | 51 | Ipilimumab, pembrolizumab, nivolumab | SUL, MTV, TLG, TBR of SUL | On baseline, PET, SULmax and SULpeak as well as most TBRs were predictive for 3- and 5-year OS rates. MTV, TLG and most of the TBRs were predictive on both follow-up studies (3 and 6 months after therapy). Changes in values of MTV, TLG and most of the TBRs from the baseline to the follow-up studies were prognostic |
| Grade | Definition |
|---|---|
| Grade 1 | Mild |
| Grade 2 | Moderate |
| Grade 3 | Severe or requiring hospitalization but not life-threatening |
| Grade 4 | Life-threatening |
| Grade 5 | Death |
| Severity | Symptoms | Management |
|---|---|---|
| Grade 1 | Asymptomatic | Close monitoring immunotherapy. Loperamida/Difenoxilato/atropine |
| Grade 2 | Abdominal pain, mucus, blood in stool | Systemic steroids (if no response in 2–3 days, consider adding infliximab within 2 weeks) |
| Grade 3 | Severe abdominal pain, peritoneal signs | Require hospitalization for supportive care:
|
| Grade 4 | Severe and persistent abdominal pain, fever, ileus, life-threatening complications, such as perforation and peritonitis. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mangas Losada, M.; Romero Robles, L.; Mendoza Melero, A.; García Megías, I.; Villanueva Torres, A.; Garrastachu Zumarán, P.; Boulvard Chollet, X.; Lopci, E.; Ramírez Lasanta, R.; Delgado Bolton, R.C. [18F]FDG PET/CT in the Evaluation of Melanoma Patients Treated with Immunotherapy. Diagnostics 2023, 13, 978. https://doi.org/10.3390/diagnostics13050978
Mangas Losada M, Romero Robles L, Mendoza Melero A, García Megías I, Villanueva Torres A, Garrastachu Zumarán P, Boulvard Chollet X, Lopci E, Ramírez Lasanta R, Delgado Bolton RC. [18F]FDG PET/CT in the Evaluation of Melanoma Patients Treated with Immunotherapy. Diagnostics. 2023; 13(5):978. https://doi.org/10.3390/diagnostics13050978
Chicago/Turabian StyleMangas Losada, María, Leonardo Romero Robles, Alejandro Mendoza Melero, Irene García Megías, Amós Villanueva Torres, Puy Garrastachu Zumarán, Xavier Boulvard Chollet, Egesta Lopci, Rafael Ramírez Lasanta, and Roberto C. Delgado Bolton. 2023. "[18F]FDG PET/CT in the Evaluation of Melanoma Patients Treated with Immunotherapy" Diagnostics 13, no. 5: 978. https://doi.org/10.3390/diagnostics13050978