
Self-Regulating Adaptive Controller for Oxygen Support to Severe Respiratory Distress Patients and Human Respiratory System Modeling

Abstract
:1. Introduction
2. Proposed Components of Respiratory Distress Treatments
2.1. Oxygen Cylinder/Oxygen Concentrator
2.2. Pulse Oximeter
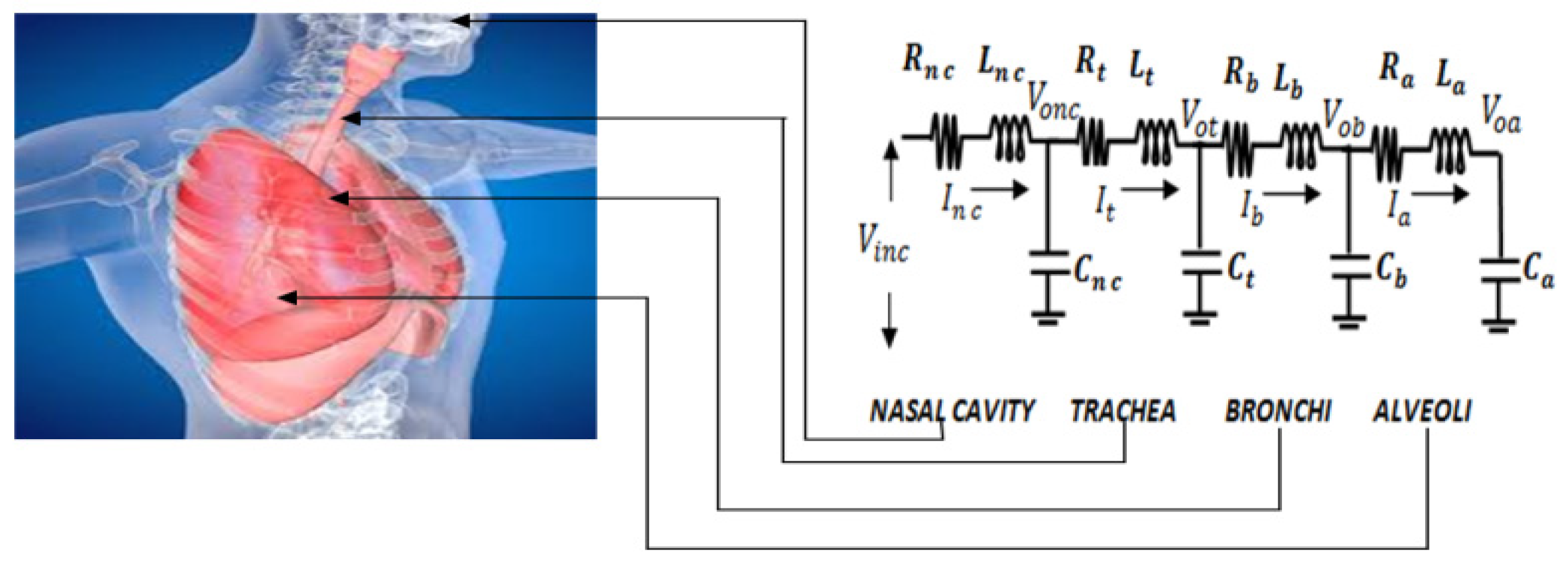
3. Mathematical Model of Respiratory System
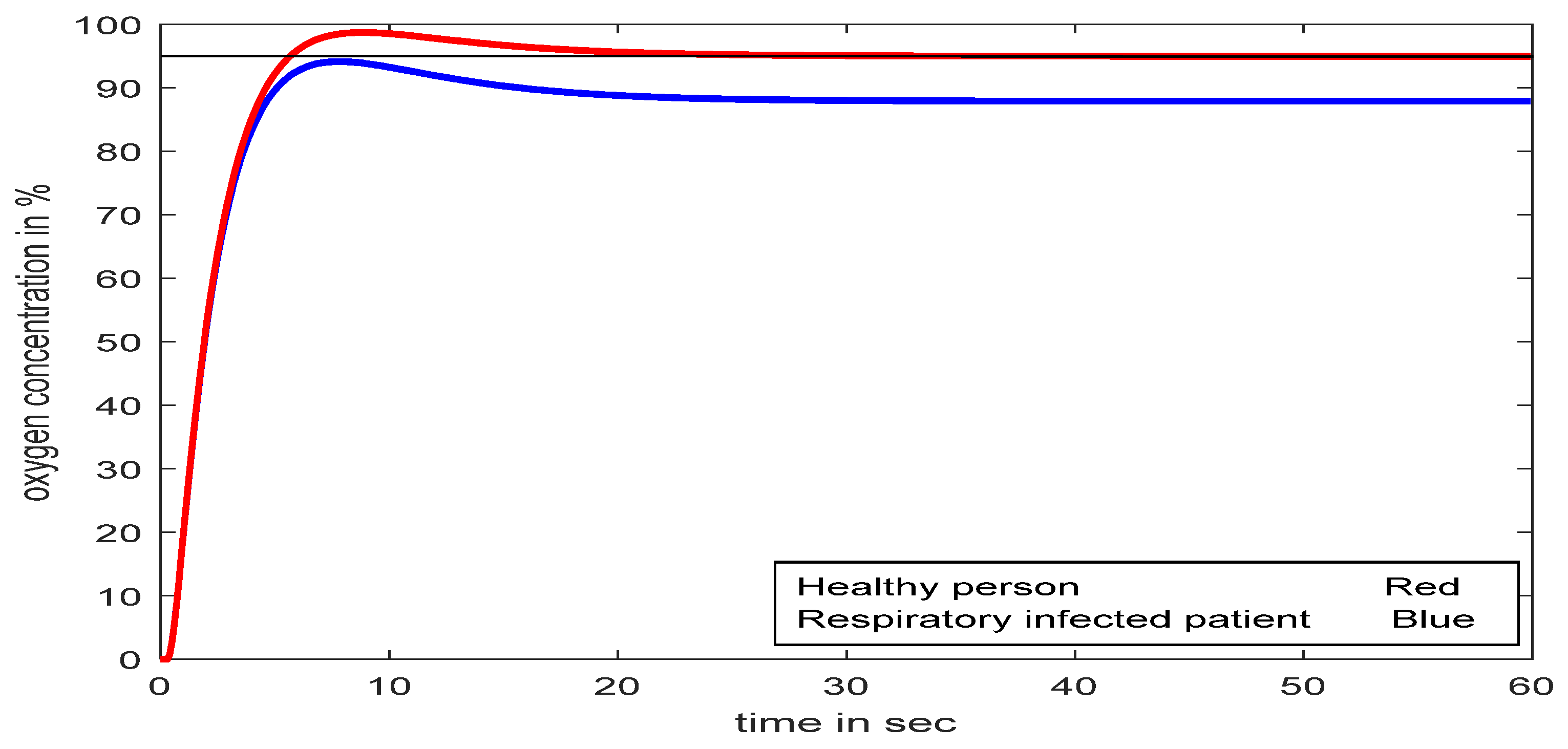
3.1. Respiratory Model Part I
Change in Respiratory Model Due to Defect in Alveoli Area
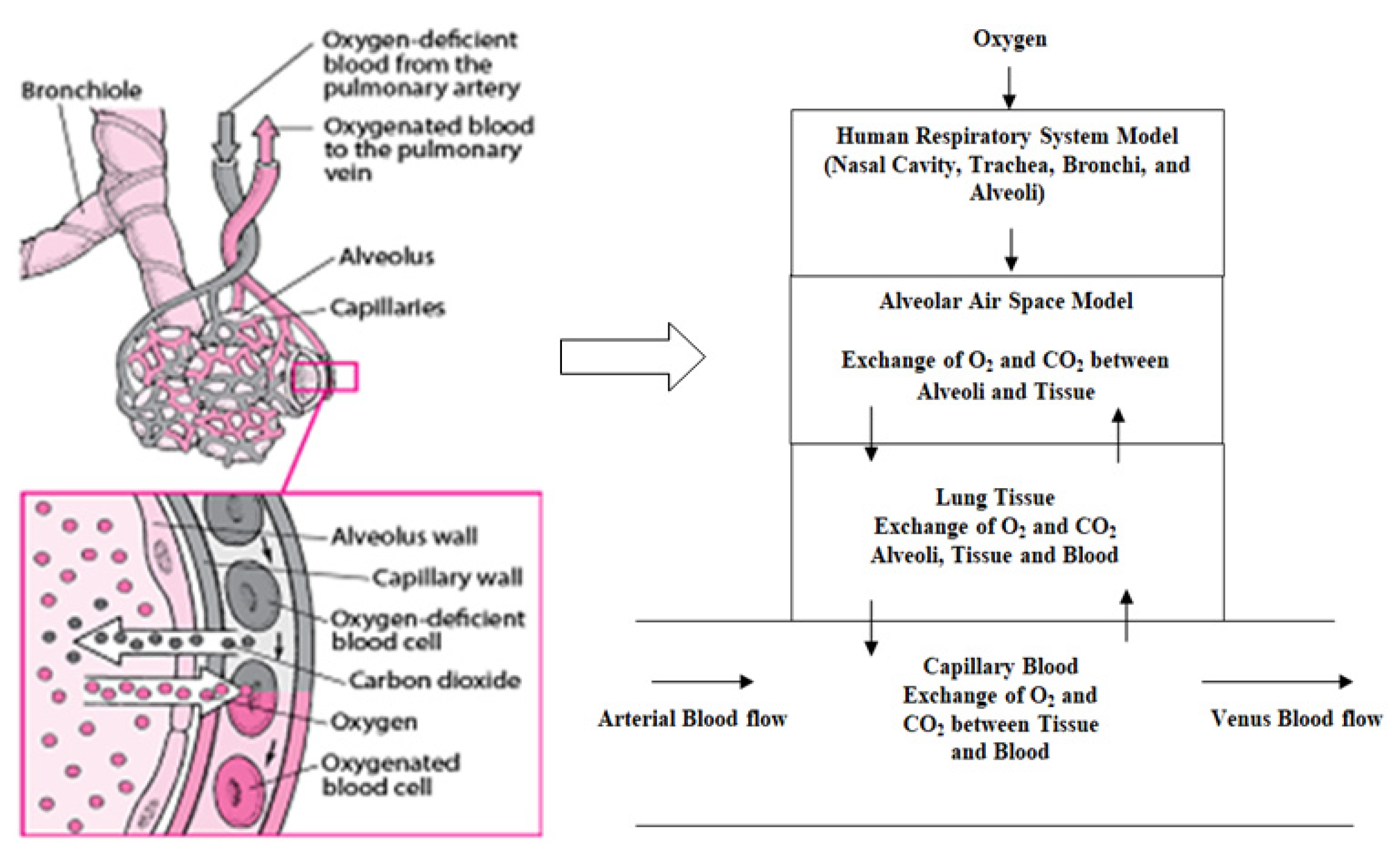
3.2. Respiratory Model Part II (Gas Exchange)
3.3. Partial Pressure Model
- (i)
- Oxygen diffusion from alveolar air space to lung tissue:
- (ii)
- Similarly, oxygen exchange between lung tissue, alveolar air space, and capillary blood is derived by:
- (iii)
- Oxygen transfer between lung tissue and capillary blood:
Electrical Analogy Model
- (i)
- Flow of oxygen from the alveolar air space (AA) to the lung tissue (LT):
- (ii)
- Oxygen exchange between lung tissue (LT), alveolar air space (AA), and capillary blood (CB):
- (iii)
- Oxygen transfer between LT and CB:
3.4. Transport Delay
4. Design of the Proposed Controller
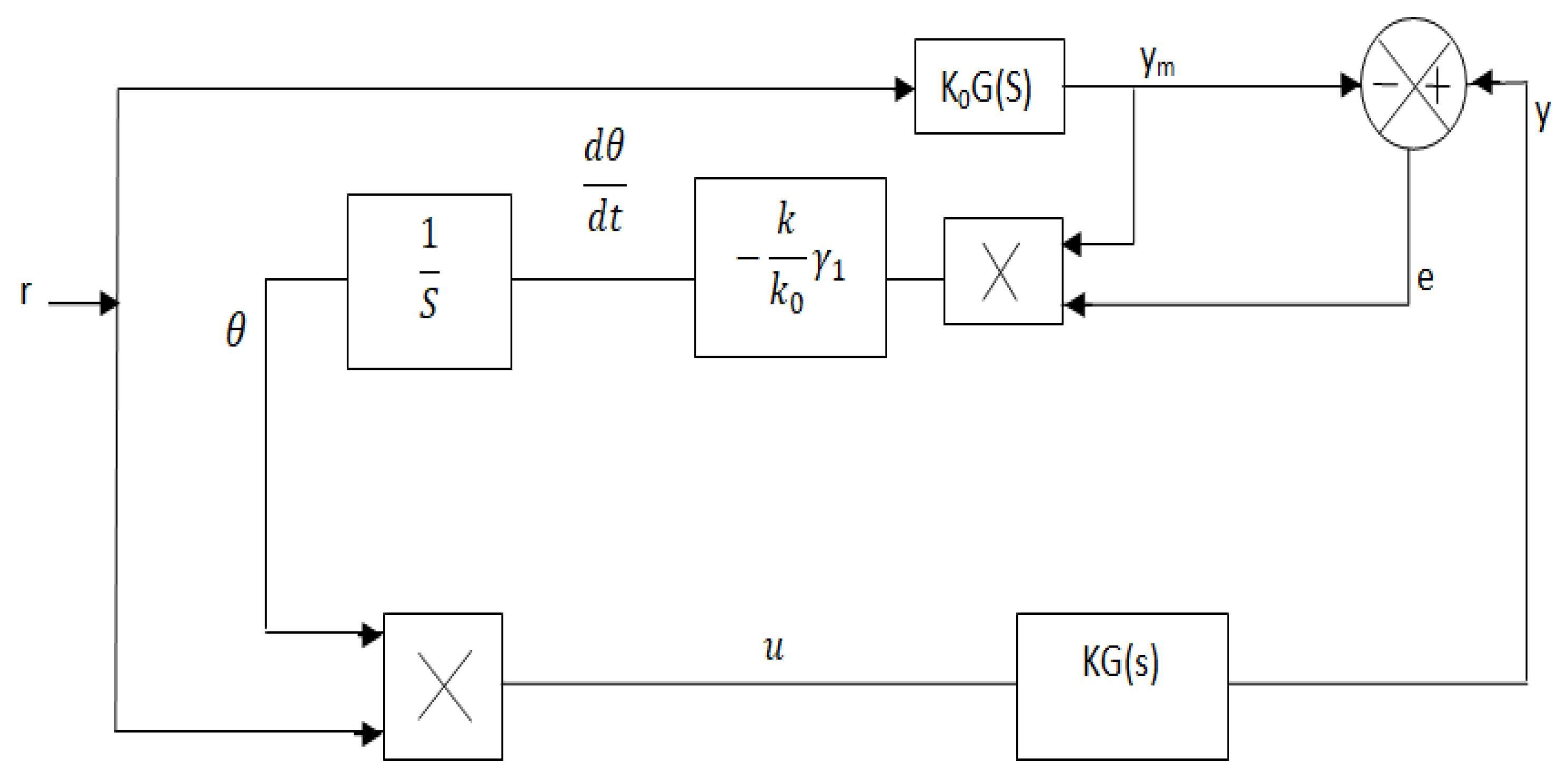
4.1. Design of MRAC
4.2. Design of Set-Point Modulated Fuzzy PI-Based MRAC
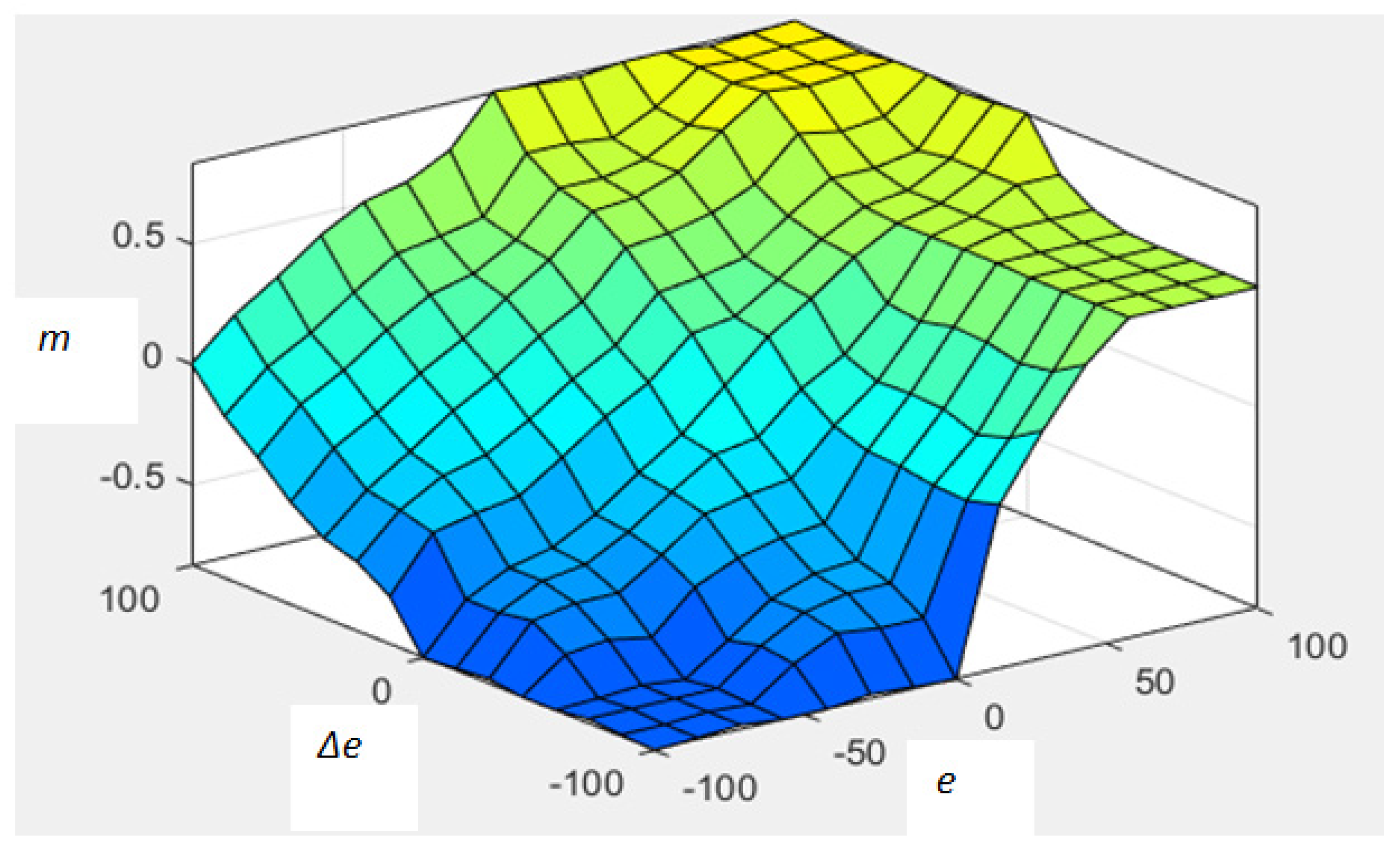
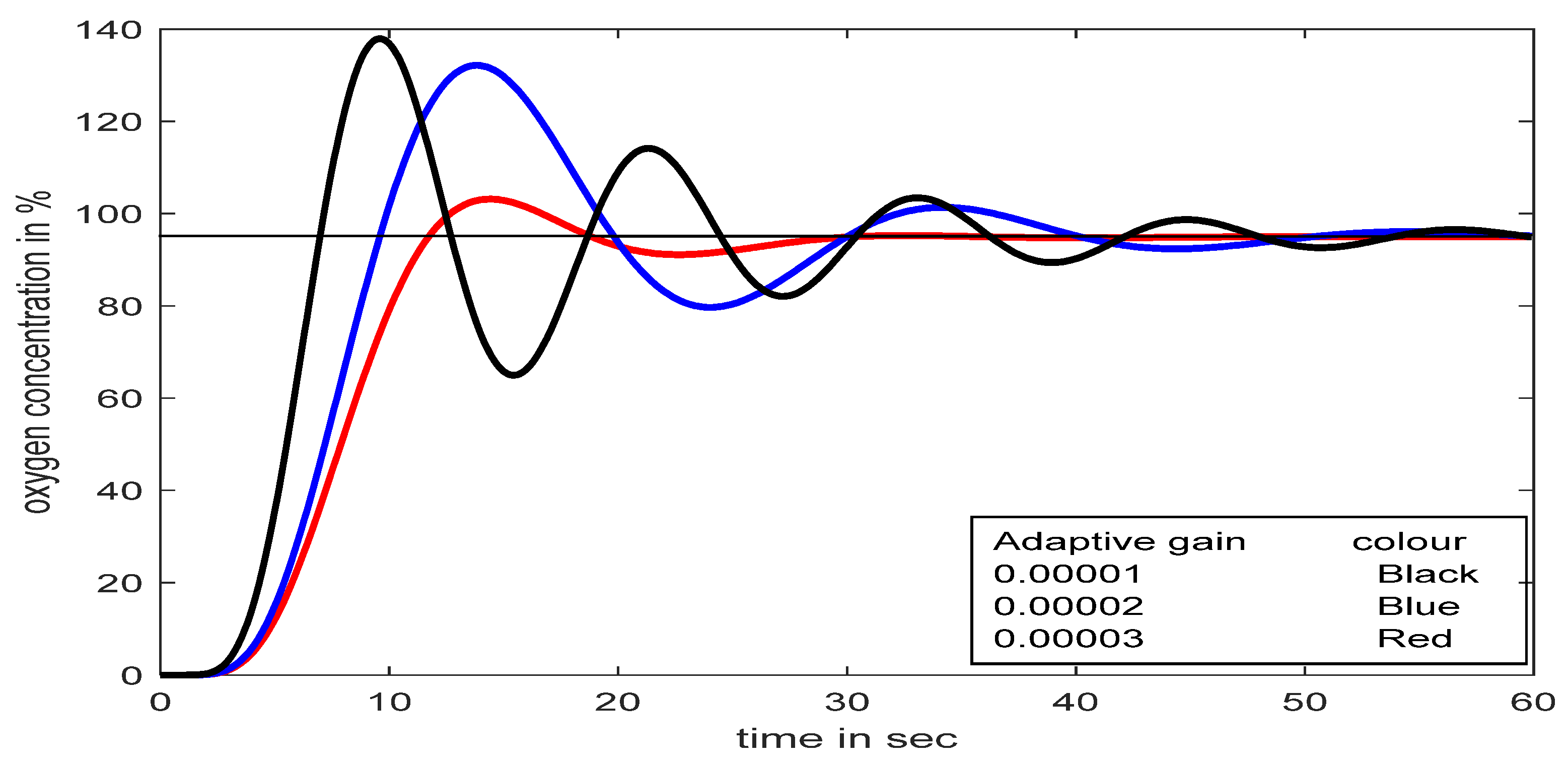
4.2.1. Fuzzy PI for Adaptive Gain (m) Adjustment
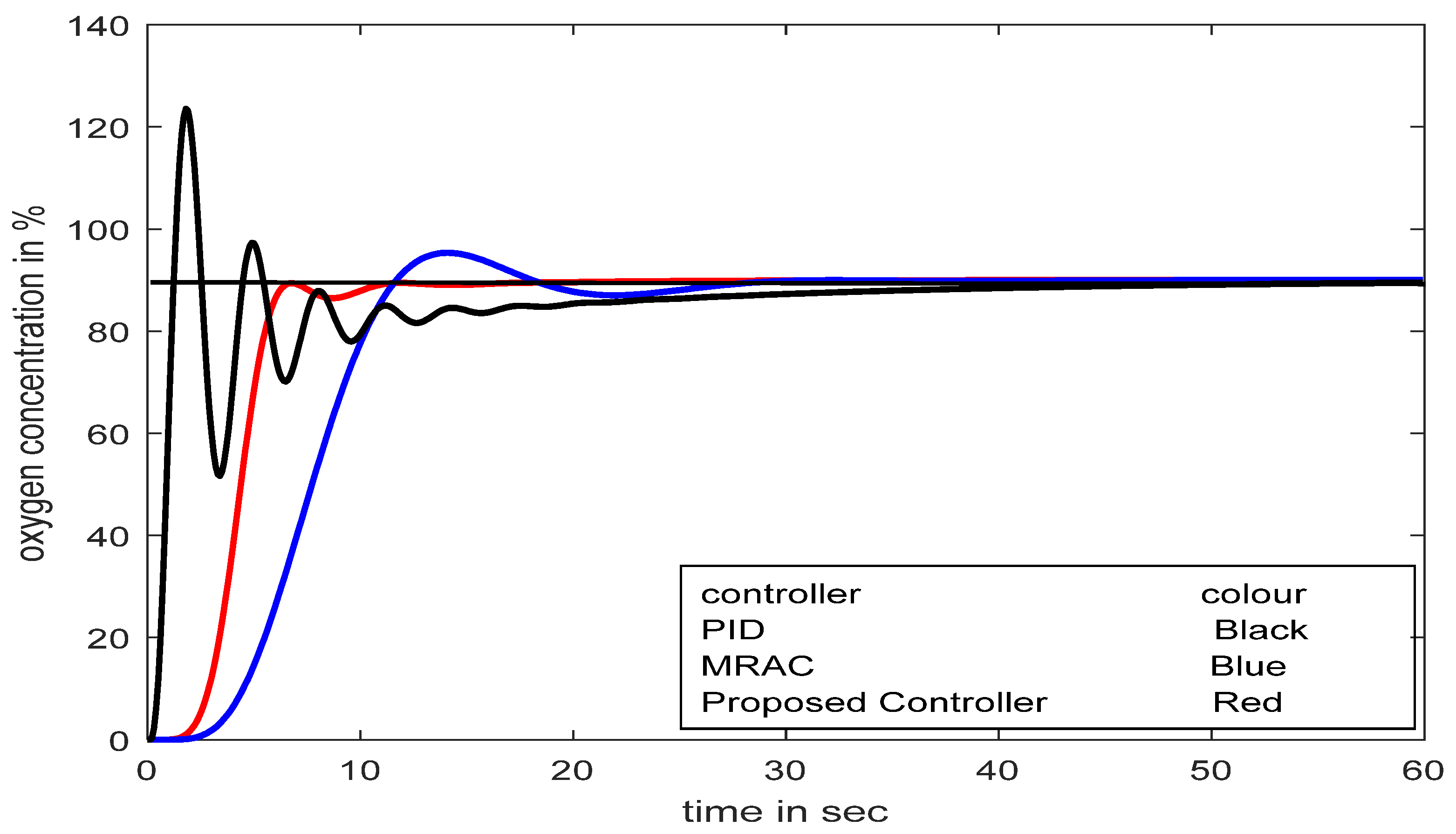
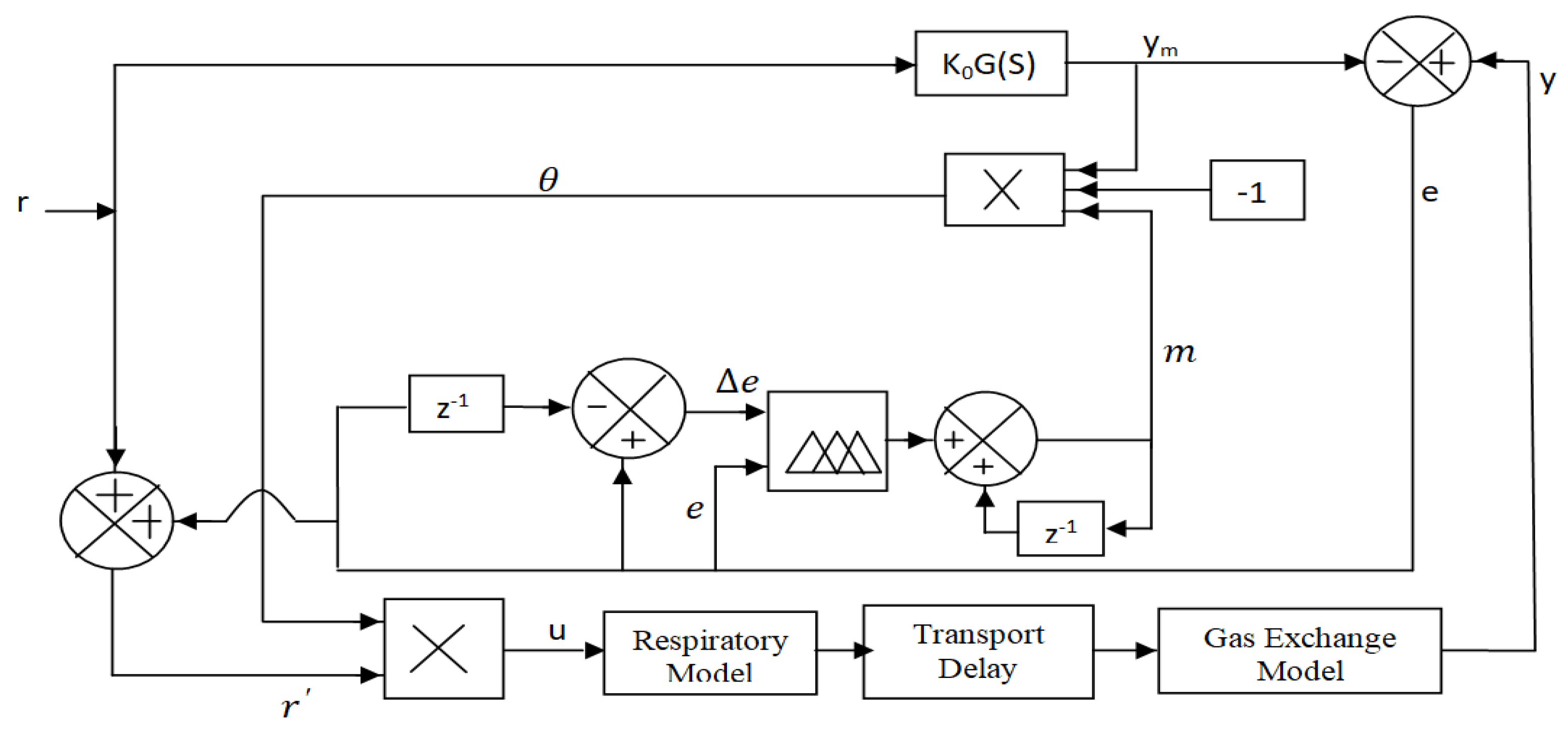
4.2.2. Proposed Scheme (SFPIMRAC)
5. Results and Discussion
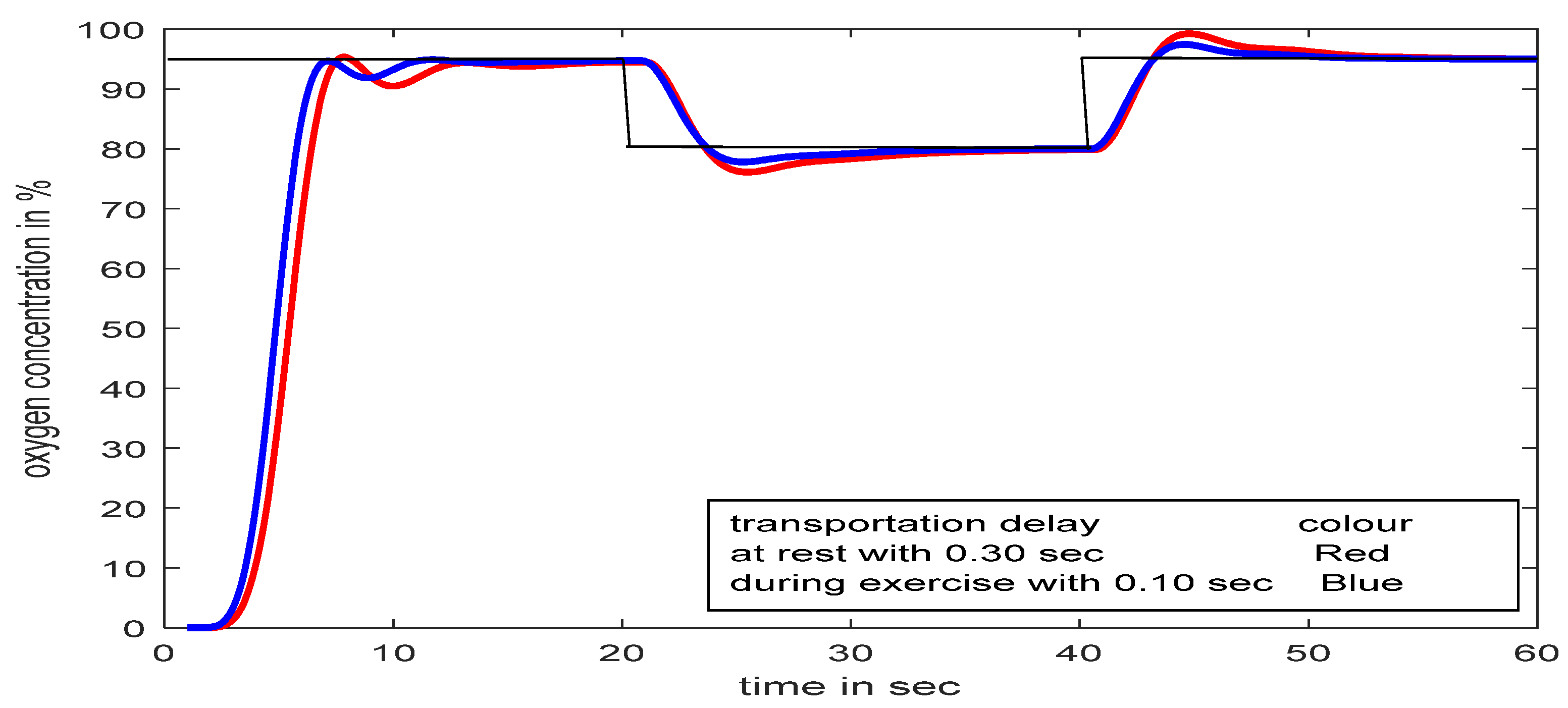
5.1. SFPIMRAC Response with Time Delay at Input and Set-Point/Load Variations
5.2. SFPIMRAC Response with Atime Delay between Two Models and Set-Point/Load Variation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Papadopoulos, N.G.; Skevaki, C.L. Viruses of the Lung. Encycl. Respir. Med. 2006, 483–488. [Google Scholar] [CrossRef]
- Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. ARDS Definition Task Force. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2020, 307, 2526–2533. [Google Scholar]
- WHO Guideline. Technical Specifications for Oxygen Concentrator; WHO: Geneva, Switzerland, 2015; pp. 1–68. [Google Scholar]
- Sul, B.; Oppito, Z.; Jayasekera, S.; Vanger, B.; Zeller, A.; Morris, M.; Ruppert, K.; Altes, T.; Rakesh, V.; Day, S.; et al. Assessing airflow sensitivity to healthy and diseased lung conditions in a computational fluid dynamics model validated in vitro. J. Biomech. Eng. 2018, 140, 1–49. [Google Scholar] [CrossRef] [Green Version]
- Devdatta, K.; Pratibha, V. Mathematical Modeling of Respiratory System: A Review. Indian J. Biomech. 2009, 56–60. [Google Scholar]
- Mehedi, I.M.; Shah, H.S.M.; Saggaf, U.M.; Al Mansouri, R.; Bettayeb, M. Fuzzy PID Control for Respiratory Systems. Hindawi J. Healthc. Eng. 2021, 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Hansen, E.F.; Bech, C.S.; Vestbo, J.; Andersen, O.; Kofod, L.M. Automatic oxygen titration with O2matic® to patients admitted with COVID-19 and hypoxemic respiratory failure. Eur. Clin. Respir. J. 2020, 7, 3695. [Google Scholar] [CrossRef]
- Ghafarian, P.; Jamaati, H.; Hashemian, S.M. A Review on Human Respiratory Modeling. Tanaffos 2016, 15, 61–69. [Google Scholar]
- Sarkar, S.; Bhattacharyya, P.; Mitra, M.; Pal, S. A novel approach towards non-obstructive detection and classification of COPD using ECG derived respiration. Australas. Phys. Eng. Sci. Med. 2019, 42, 1011–1024. [Google Scholar] [CrossRef]
- Reynolds, A.; Ermentrout, G.B.; Clermont, G. A mathematical model of pulmonary gas exchange under inflammatory stress. J. Theor. Biol. 2010, 264, 161–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Axel, R.; Jörn, K.; Knut, M. Predicting eTCO2 response in a model of ventilation-perfusion mismatch. Biomed. Tech. 2013, 58. [Google Scholar] [CrossRef]
- Tehrani, F.T. Mathematical model of the human respiratory system in chronic obstructive pulmonary disease. Healthc. Technol. Lett. 2020, 7, 139–145. [Google Scholar] [CrossRef]
- Trusov, P.V.; Zaitseva, N.V.; Tsinker, M.Y. A Mathematical Model of the Human Respiratory System Considering Environmental Influence. In Proceedings of the 28th Russian Conference on Mathematical Modeling in Natural Sciences, Perm, Russia, 2–5 October 2019. [Google Scholar] [CrossRef]
- Tehrani, F.T. Computerized decision support for differential lung ventilation. Healthc. Technol. Lett. 2019, 6, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Milhorn, H.T.; Benton, R.; Ross, R.; Guyton, A.C. A mathematical model of the human respiratory control system. Biophys. J. 1965, 5, 27–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, S.L.; Guo, N.R.; Chiu, C.C. Modeling and simulation of respiratory control with Lab View. J. Med. Biol. Eng. 2012, 32, 51–60. [Google Scholar] [CrossRef]
- Lutchen, K.R.; Costa, K.D. Physiological interpretations based on lumped element models fit respiratory impedance data: Use of forward-inverse modeling. IEEE Trans. Biomed. Eng. 1990, 37, 1076–1085. [Google Scholar] [CrossRef]
- Wall, W.A.; Wiechert, L.; Comerford, A.; Rausch, S. Towards a comprehensive computational model for the respiratory system. Int. J. Numer. Methods Biomed. Eng. 2010, 26, 807–827. [Google Scholar] [CrossRef]
- Axel, R.; Jörn, K.; Knut, M. Hierarchical structure of human gas exchange models to improve parameter identification. In Proceedings of the 2013 ICME International Conference on Complex Medical Engineering, Beijing, China, 25–28 May 2013; pp. 103–108. [Google Scholar]
- Martin, S.; Maury, B. Modeling of the oxygen transfers in the respiratory process. ESAIM: Mathematical Modeling and Numerical Analysis. EDP Sci. 2013, 47, 935–960. [Google Scholar]
- Xu, L.; Fu, M. Computer Modeling of Interactions of an Electric Motor, Circulatory System, and Rotary Blood Pump. ASAIO J. 2000, 46, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.C.; Donald, I.; Russell, L.; Mussivand, T. Development of a Mathematical Model of the Human Circulatory System. Ann. Biomed. Eng. 2006, 34, 1400–1413. [Google Scholar]
- Shekhar, A.; Sharma, A. Review of Model Reference Adaptive Controller. In Proceedings of the 2018 International Conference on Information, Communication, Engineering and Technology (ICICET), Pune, India, 29–31 August 2018; pp. 1–15. [Google Scholar]
- Tudu, B.; Metla, A.; Das, B.; Bhattacharyya, N.; Jana, A.; Ghosh, D.; Bandyopadhyay, R. Towards versatile electronic nose pattern classifier for black tea quality evaluation: An incremental fuzzy approach. IEEE Trans. Instrum. Meas. 2009, 58, 3069–3078. [Google Scholar] [CrossRef]
- Ghozlane, W.; Knani, J. Model Reference Adaptive Control Design for Nonlinear Plants. Int. J. Adv. Comput. Sci. Appl. 2019, 10, 116–124. [Google Scholar] [CrossRef] [Green Version]
- Mushiri, T.; Mahachil, A.; Mbohwa, C. A Model Reference Adaptive Control (MRAC) System for the Pneumatic Valve of the Bottle Washer in Beverages using Simulink. In Proceedings of the International Conference on Sustainable Materials Processing and Manufacturing, Kruger, South Africa, 23–25 January 2017; pp. 364–373. [Google Scholar]
- Bożena, M.-M.; Dariusz, M.; Stanisław, K. Processing of crisp and fuzzy measures in the fuzzy data warehouse for global natural resources. In International Conference on Industrial, Engineering and Other Applications of Applied Intelligent Systems; Springer: Berlin/Heidelberg, Germany, 2010; pp. 616–625. [Google Scholar]
- Pal, A.K.; Indrajit, N.; Sampa, P. A Fuzzy-Based Modified Gain Adaptive Scheme for Model Reference Adaptive Control. In Information and Decision Sciences, Advances in Intelligent Systems and Computing; Springer: Singapopre, 2018; Volume 701, pp. 315–324. [Google Scholar]
- Pal, A.K.; Indrajit, N.; Sampa, P. Fuzzy-based Gain Adaptive Scheme for Set-Point Modulated Model Reference Adaptive Controller. Int. J. Nat. Comput. Res. 2018, 7, 1–19. [Google Scholar] [CrossRef]
- Pal, A.K.; Indrajit, N.; Sampa, P.; Chakraborty, J. Auto adaptive fuzzy controllers with automatic set-point adjustment. In Intelligent Electrical Systems: A Step towards Smarter Earth; CRC Press: Boca Raton, FL, USA; Taylor & Francis Group: Abingdon, UK, 2020; pp. 181–189. [Google Scholar]
- Andreu-Perez, J.; Cao, F.; Hagras, H.; Yang, G.Z. A self-adaptive online brain–machine interface of a humanoid robot through a general type-2 fuzzy inference system. IEEE Trans. Fuzzy Syst. 2016, 26, 101–116. [Google Scholar] [CrossRef] [Green Version]
- Ravì, D.; Wong, C.; Deligianni, F.; Berthelot, M.; Andreu-Perez, J.; Lo, B. Deep learning for health informatics. IEEE J. Biomed. Health Inform. 2016, 21, 4–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naskar, I.; Pal, A.K. Self Adaptive Fuzzy Controller for Supplementary Oxygen Supply to the Respiratory Distress Patients. J. Sci. Res. 2022, 14, 843–860. [Google Scholar] [CrossRef]

























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Generation Number | Number of Airways Per Generation | Airways Diameter in cm | Length in cm | Total Airways Area in cm2 | Avg. Air Flow Velocity in cm/s | Resistance in cm of H2O/L ltr./s Calculated Using Formula | Inertance in cm of H2O/L/s2 Calculated Using Formula | Compliance in ltr./cm of H2O Calculated Using Formula |
|---|---|---|---|---|---|---|---|---|
| z | n(z) | d = 2r | l | s | u | 8 μL/πr4 | L/s | ls/n(z)u2 |
| 0 | 1 | 1.8 | 12 | 2.54 | 197 | 0.0086 | 0.0059 | 0.06311 |
| 1 | 2 | 1.22 | 4.76 | 2.33 | 215 | 0.008 | 0.0025 | 0.0964 |
| 2 | 4 | 0.83 | 1.9 | 2.13 | 236 | 0.0075 | 0.0011 | 0.0145 |
| 3 | 8 | 0.56 | 0.76 | 2 | 251 | 0.0072 | 0.0004 | 0.0024 |
| 4 | 16 | 0.45 | 1.27 | 2.48 | 202 | 0.0145 | 0.0006 | 0.0038 |
| 5 | 32 | 0.35 | 1.07 | 3.11 | 161 | 0.0167 | 0.0004 | 0.0032 |
| 6 | 64 | 0.28 | 0.9 | 3.96 | 126 | 0.0172 | 0.0002 | 0.0028 |
| 7 | 128 | 0.23 | 0.76 | 5.1 | 98 | 0.0159 | 0.0001 | 0.0025 |
| 8 | 256 | 0.186 | 0.64 | 6.95 | 72 | 0.0157 | 0.0001 | 0.0026 |
| 9 | 512 | 0.154 | 0.54 | 9.56 | 52 | 0.0141 | 7.03 × 10−5 | 0.0029 |
| 10 | 1024 | 0.13 | 0.46 | 13.4 | 37 | 0.0118 | 4.27 × 10−5 | 0.0035 |
| 11 | 2048 | 0.109 | 0.39 | 19.6 | 26 | 0.0101 | 2.48 × 10−5 | 0.0044 |
| 12 | 4096 | 0.095 | 0.33 | 28.8 | 17 | 0.0074 | 1.43 × 10−5 | 0.0064 |
| 13 | 8192 | 0.082 | 0.27 | 44.5 | 11 | 0.0054 | 7.55 × 10−6 | 0.0097 |
| 14 | 16,384 | 0.074 | 0.16 | 69.4 | 7.2 | 0.0024 | 2.87 × 10−6 | 0.0105 |
| 15 | 32,768 | 0.05 | 0.13 | 117 | 4.3 | 0.0048 | 1.41 × 10−6 | 0.0206 |
| 16 | 65,536 | 0.049 | 0.11 | 225 | 2.2 | 0.0022 | 6.19 × 10−7 | 0.0638 |
| 17 | 131,072 | 0.04 | 0.09 | 300 | 1.7 | 0.002 | 3.86 × 10−7 | 0.0591 |
| 18 | 262,144 | 0.038 | 0.08 | 543 | 0.92 | 0.0011 | 1.90 × 10−7 | 0.1632 |
| 19 | 524,288 | 0.036 | 0.07 | 978 | 0.51 | 0.0005 | 8.91 × 10−8 | 0.4034 |
| 20 | 1,048,576 | 0.034 | 0.07 | 1740 | 0.29 | 0.0003 | 5.01 × 10−8 | 1.1099 |
| 21 | 2,097,152 | 0.031 | 0.07 | 2730 | 0.18 | 0.0002 | 3.19 × 10−8 | 2.26 |
| 22 | 4,194,304 | 0.029 | 0.67 | 5070 | 0.99 | 0.0016 | 1.64 × 10−7 | 0.664 |
| 23 | 8,388,608 | 0.025 | 0.07 | 7530 | 0.66 | 0.0001 | 1.24 × 10−8 | 0.1241 |
| Different Section of Human Respiratory System | R H2O/ltr/s | L H2O/ltr/s2 | C ltr/cm of H2O | RC | LC |
|---|---|---|---|---|---|
| NASAL CAVITY | 16.332700 | 0.0200000000 | 0.1320 | 2.156000 | 0.00270000000 |
| TRACHEA | 0.086000 | 0.0059000000 | 0.0631 | 0.005400 | 0.00037000000 |
| BRONCHI | 0.008700 | 0.0002929000 | 0.0461 | 0.000402 | 0.00001440000 |
| ALVEOLI | 0.000550 | 0.0000000647 | 1.0396 | 0.000571 | 0.00000006720 |
| Parameters | Alveolar Air | Tissue | Capillary Blood |
|---|---|---|---|
| Volume (L) | VA = 1.9 × 10−7 | VT = 4.2 × 10−8 | VB = 7.5 × 10−9 |
| Molar concentration (M/mm) | σA = 2.5 × 10−5 | σA = 1.2 × 10−6 | σB = 1.2 × 10−6 |
| Diffusion rate (L/s) | DTA = 2.4 × 10−12 | DTA = (6.7 – 10) × 10−12 |
| e/Δe | NB | NM | ZE | PM | PB |
|---|---|---|---|---|---|
| NB | NB | NB | NB | NM | ZE |
| NM | NB | NB | NM | ZE | PM |
| ZE | NB | NM | ZE | PM | PB |
| PM | PM | PM | PM | PB | PB |
| PB | PM | PM | PB | PB | PB |
| e = (y − ym) | Δe | m | Output (θ = −mym) |
|---|---|---|---|
| +ve (high); y > ym | +ve (high) | +ve (high) | −ve/ need to decrease oxygen flow as y > ym |
| 0; y = ym | 0 | 0 | No change in oxygen flow, maintain the same flow |
| −ve (high); y < ym | −ve (high) | −ve (high) | +ve/ need to increase oxygen flow as y < ym |
| e | r’ = r + e | Remarks |
|---|---|---|
| +ve | r’→+ve | r’ > r |
| −ve | r’→+ve | e < r and r’ < r |
| zero | r’ = r | r’ = r |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naskar, I.; Pal, A.K.; Jana, N.K. Self-Regulating Adaptive Controller for Oxygen Support to Severe Respiratory Distress Patients and Human Respiratory System Modeling. Diagnostics 2023, 13, 967. https://doi.org/10.3390/diagnostics13050967
Naskar I, Pal AK, Jana NK. Self-Regulating Adaptive Controller for Oxygen Support to Severe Respiratory Distress Patients and Human Respiratory System Modeling. Diagnostics. 2023; 13(5):967. https://doi.org/10.3390/diagnostics13050967
Chicago/Turabian StyleNaskar, Indrajit, Arabinda Kumar Pal, and Nandan Kumar Jana. 2023. "Self-Regulating Adaptive Controller for Oxygen Support to Severe Respiratory Distress Patients and Human Respiratory System Modeling" Diagnostics 13, no. 5: 967. https://doi.org/10.3390/diagnostics13050967