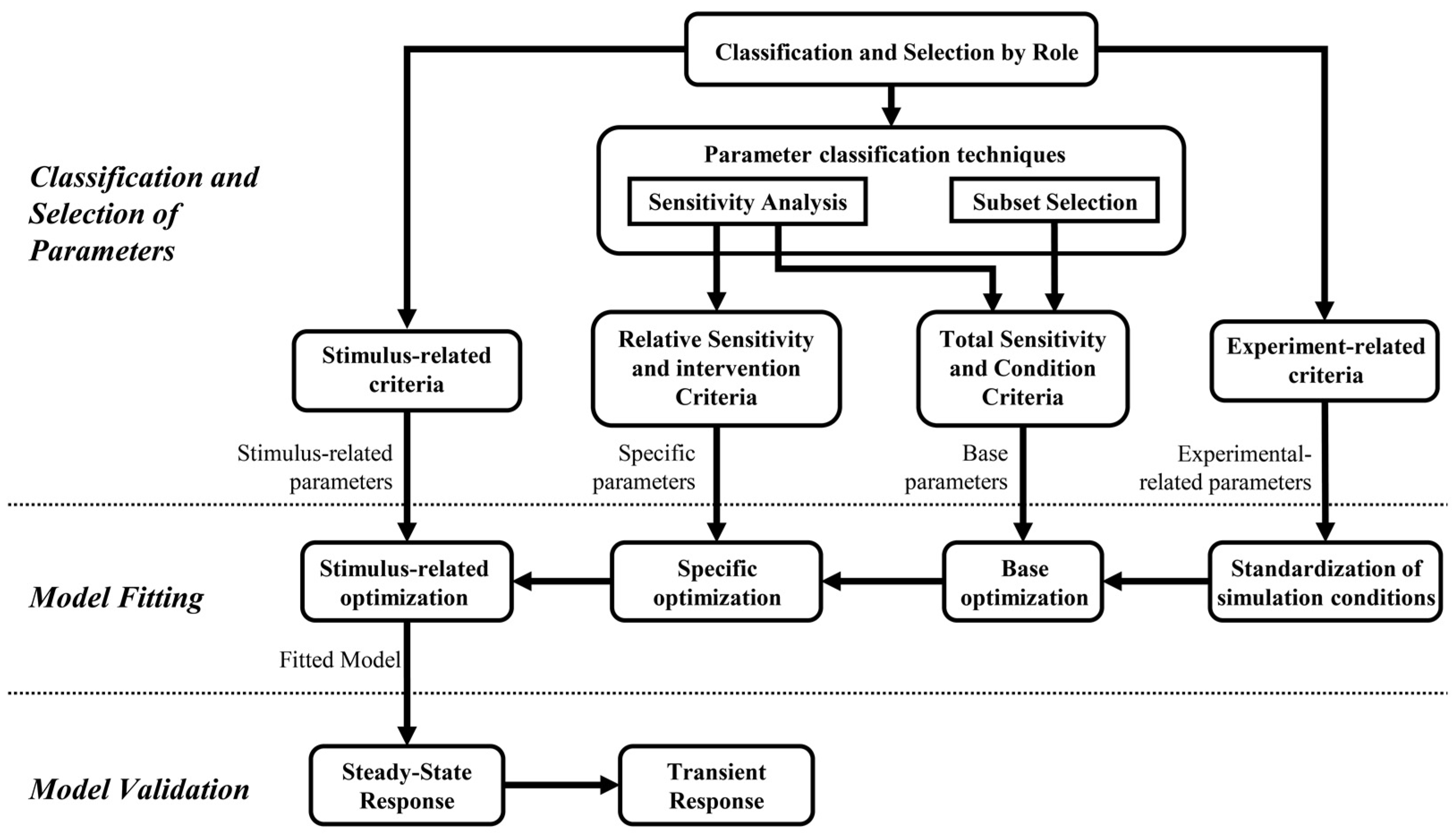
2.1.1. Classification and Selection of Parameters
This procedure aims to highlight and select the parameters that can be considered best-fit candidates. The selection of parameters is justified according to their relationship to available experimental data, role in the model, identifiability, sensitivity to variations, and their relationship to the stimulus evaluated. Initially, it reduces the number of parameters depending on their role in the model and the objective of fitting predictions in steady-state conditions. Subsequently, the resulting parameters are classified and selected according to two reported techniques and established criteria regarding the model fitting approaches.
Classification and Selection of Parameters by Role
It consists of an initial classification of the model parameters according to their roles. It comprises five parameter classes generally found in structured models of physiological systems. They correspond to (i) time constants, i.e., parameters related to transient response; (ii) conversion parameters, which are constant values related to equivalences among measurement units; (iii) covariates, corresponding to values that allow defining simulation conditions regarding external disturbances, environment conditions, and features of the population to be simulated; (iv) initial values, corresponding to initial conditions of the model variables, usually required as initial states of integrators and whose action mainly affect the temporal characteristics of the responses before reaching the model steady state; and (v) gain and thresholds, that either module or saturate variables related to model mechanisms, i.e., the weighting of the chemoreceptors response to set the parasympathetic and sympathetic activity regarding the regulation of peripheral resistances in cardiovascular control models.
The selection of parameters comprises choosing those parameters that mainly define the steady-state behavior of the cardiorespiratory system response and, therefore, can be used to fit the model response in such a condition. The time constant parameters and initial values are discarded, considering that the proposed fitting procedure focuses on the response once the steady state is reached. Conversion parameters do not need fitting because of their nature and meaning. Therefore, only gain and threshold parameters, whose variations have physiological sense, and are correlated with experimental conditions, and covariates will be considered for the subsequent selection procedures and fitting process. Covariates are only used for the standardization of the simulation conditions.
Parameter Classification Techniques
The proposed strategy involves modifying and implementing two of the most widely implemented parameter classification techniques for fitting physiological models [
8,
23]. A detailed description of each is presented below.
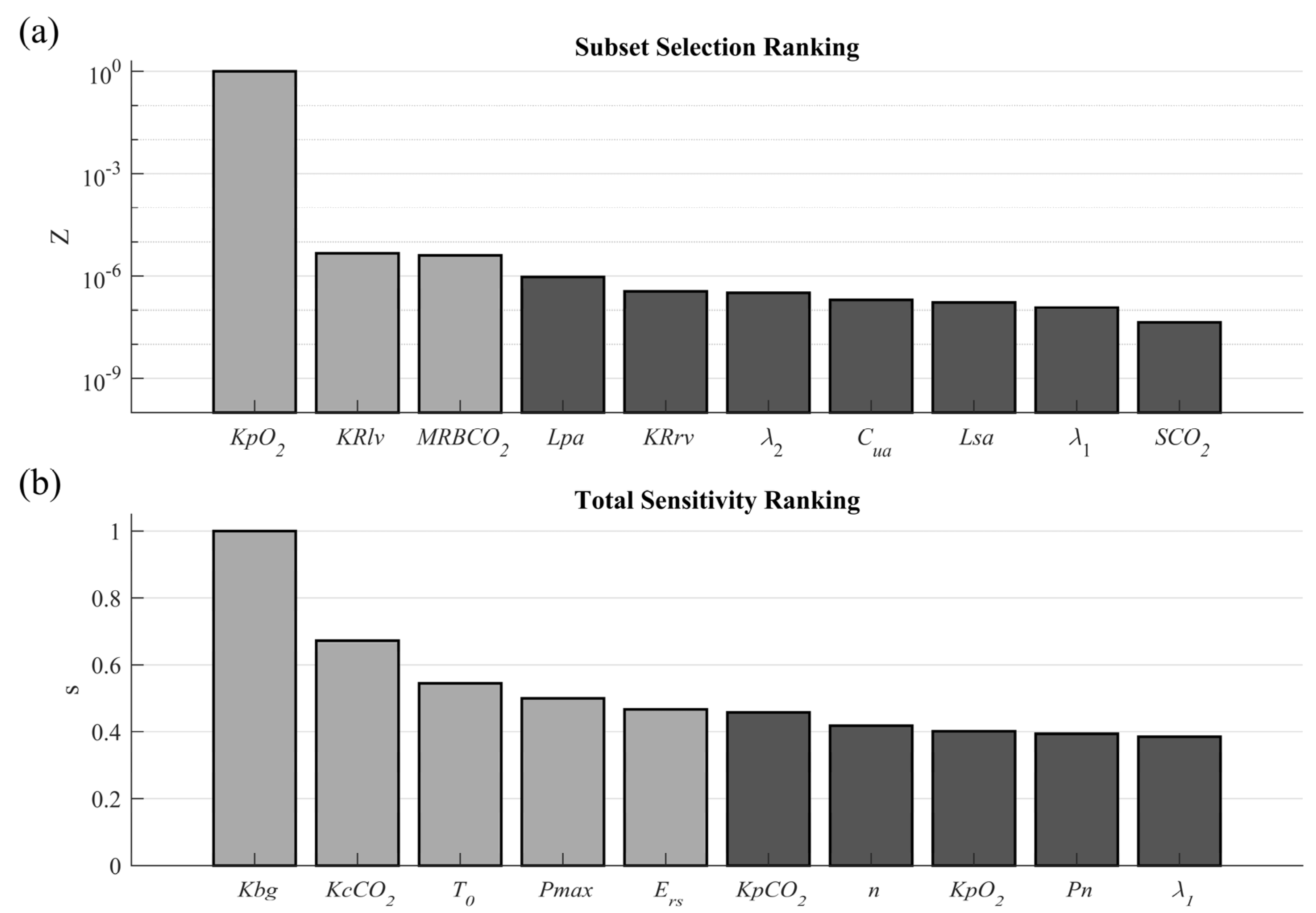
Subset Selection of Parameters
It is a technique based on the classification of model parameters according to how well-conditioned or ill-conditioned they can be identified [
27]. Well-conditioned parameters correspond to those that can be reliably estimated from the constrained experimental data, while ill-conditioned ones are those for which there are multiple fitting solutions.
In this study, the subset selection of parameters is based on QR Factorization with the Column Pivoting method [
28]. It was selected because it has been widely implemented in different physiological models [
2,
8,
23,
29], presented one of the best results regarding cardiorespiratory models among the other methods reported [
28], and considers the difference between model predictions and experimental data as a reference [
2]. This technique is based on the solution of optimization problems using gradient techniques. It establishes a ranking of the well-conditioned parameters for identification by analyzing the interdependencies in the Jacobian.
This technique is complemented by integrating the different stimulus exercise levels (according to the experimental data) and variations in the parameters previously selected in the appropriate physiological range (around their nominal values). These additions would allow the selection of parameters that are more consistent with the desired fit.
According to the above, the Jacobian is calculated according to Equation (1).
where the indexes i, j, and k represent the variable, parameter, and stimulus level to be evaluated, respectively; l is an index that identifies the parameter variation regarding its nominal value.
is the Jacobian for a specific stimulus level and parameter value variation, formed as the matrix of variations of the differences for each variable
regarding the change of each parameter for a specific variation level
;
corresponds to the difference between each experimental data and the model prediction given each parameter’s change for a particular level of variation. The singular value decomposition is calculated for
, according to Equation (2).
where
is the matrix of left singular vectors,
is the diagonal matrix of singular values of
in decreasing order,
is the matrix of the right singular vectors, and
denotes the matrix transpose. Matrix
must be partitioned, as expressed in Equation (3).
where W is the total number of parameters analyzed, and
is a numerical rank that indicates the number of maximally independent columns of
.
is equivalent to the number of parameters that can be identified given the model output and can be determined by the selection of the smallest allowed singular value according to the relation expressed in Equation (4) [
23].
where
is the singular value for
is the largest singular value,
is the normalized singular value for
, and
is a tolerance value that allows differentiating the most significant eigenvalues.
The parameters associated with the
highest singular values are found using QR decomposition with column pivoting, according to Equation (5).
where
is a permutation matrix,
is an orthogonal matrix and the first
columns of
form an upper triangular matrix with diagonal elements in decreasing order.
is then used to reorder the parameters according to Equation (6).
where
is an identification vector of the parameters and
is the vector of the parameters reordered, which is partitioned regarding
, as presented in Equation (7).
where
is a vector containing the
estimable parameters and
are the parameters that would be fixed at nominal values.
The standard 2-norm of the normalized singular value for each parameter in each ranking obtained for each parameter variation must be determined to obtain a general ranking independent of the stimulus level, as presented in Equation (8).
where
corresponds to the standard 2-norm of the normalized singular value of the parameter j for the variation level l,
is the normalized singular value of the parameter j for the stimulus level k and the parameter variation level l, and K is the number of stimulus levels.
Finally, the result of this technique corresponds to the presented in Equation (9).
where
is the standard 2-norm of
of the parameter j, and L is the total number of parameter variations.
This technique is usually implemented with sensitivity analysis techniques because their approaches complement each other regarding the problem solution. QR decomposition identifies the parameters to which the model is sensitive as a group, while sensitivity analysis finds the parameters to which the model is individually sensitive [
2].
Sensitivity Analysis
Sensitivity analysis involves the integration and improvement of the techniques introduced by [
6,
8,
23]. It comprises a deterministic analysis that evaluates the global model and variables’ sensitivity to variations in model parameters and stimulus levels. It also involves an experimental data dependency term that weighs such sensitivity by the error reached by the model at each parameter variation and stimulus level.
The model variable’s sensitivity regarding each parameter variation is based on the standard local differential equation described by [
30] and used by [
8,
19,
23,
31,
32] to calculate time-dependent sensitivities in cardiovascular and respiratory models. Equation (10) shows the computation of this sensitivity.
where
represents the relative sensitivity of the variable
to parameter
, which is dimensionless by the ratio between the parameter
and the variable
values at nominal conditions (no parameter variation). n refers to the parameter’s nominal value.
This work proposes modifying the measurement of relative sensitivity to make it independent of the time and dependent on the stimulus. Therefore, an approach based on steady-state conditions at different stimulus levels is used. Relative sensitivity is evaluated by varying each parameter over a range around its nominal value, while the others are kept at their nominal values. Equation (11) shows the proposed relative sensitivity measure. Time independence avoids significant differences between sensitivity measures due to time lags, considering that the fitting model procedure is focused on minimizing the steady-state differences between the experimental measurements and the model predictions. The evaluation of the stimulus is included by considering the influence of its variations on sensitivity measures.
where, i, j, and k are indexes that refer to the analyzed variable, parameter, and stimulus level.
is a scalar value of the relative sensitivity; Y is the variable value in the steady state;
is the parameter value; n refers to the parameter’s nominal value. Therefore, Equation (11) evaluates changes in the variable
regarding variations in the parameter
at the stimulus level k (first quotient), which is dimensionless by the ratio between the parameter’s nominal values
and the variable
at the stimulus level k (second quotient).
Deriving sensitivity equations can be tedious and error-prone for large systems, mainly when they involve nonlinear features, such as those analyzed in this case study. Alternatively, Equation (11) can be solved using a computational approach consisting of a simple finite difference method. A numerical approximation of the derivatives, which also considers the variation of the parameter relative to its nominal value, is expressed in Equation (12).
where
is a scalar value of the sensitivity for the variable
regarding the variation
in the parameter
at the stimulus level
.
is the vector of change proportions of the parameter regarding its nominal value. This expression can be reduced and organized as expressed in Equation (13).
where the first quotient of the equation, also identified as
, is a dimensionless term representing the rate of change of the variable
when a percentual variation
in the parameter
is applied at the stimulus level k. The second quotient is a dimensionless term representing a weighting factor, giving heavier importance to slight parameter variations. Therefore, the sensitivity
corresponds to a dimensionless scalar value that measures the weighted relative variations of the analyzed variables according to four degrees of freedom.
Standard 2-norm is applied to
to obtain a measure of the relative sensitivity independent of the parameter variations, as expressed in Equation (14). As a result, a positive dimensionless scalar value related to the relative sensitivity’s mean trend is obtained for all parameters.
where L is the total number of parameter variations or elements of the vector
.
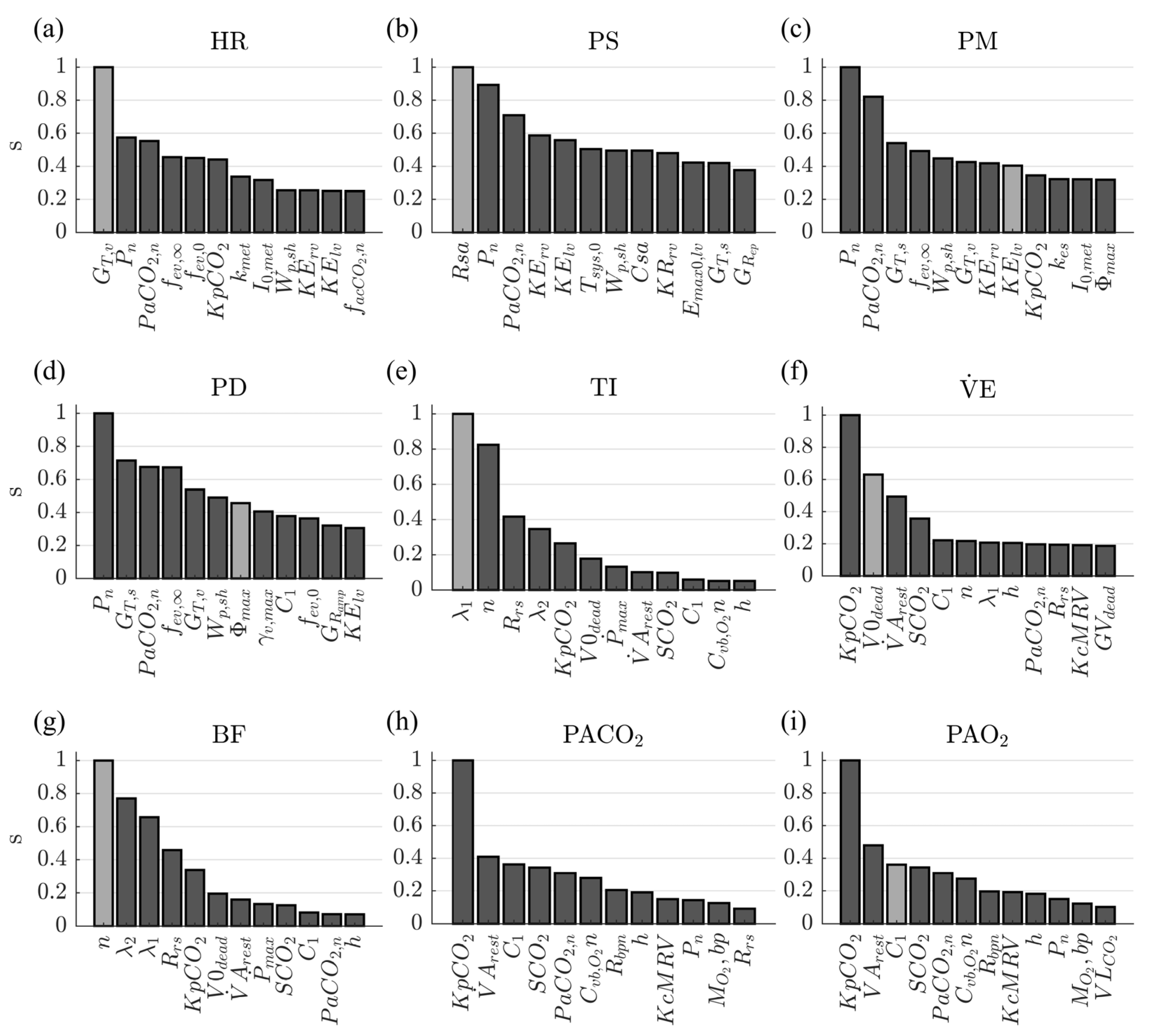
The stimulus level independency relative sensitivity is calculated according to Equation (15).
where K is the total number of stimulus levels;
is the maximum relative sensitivity obtaining for the variable
at the stimulus level k considering all parameters;
is the weighted relative sensitivity; and
is a weighting factor representing the variable error at the stimulus level k.
corresponds to the standard 2-norm of normalized by its maximum value at each stimulus level k and weighted by . Normalization of allows comparing the sensitivity measures between different stimulus levels, whereas the inclusion of the weighting factor prioritizes the sensitivity obtained at the stimulus levels for which the variable’s error is more significant (i.e., errors obtained from predictions resulting from using parameter’s nominal values). As a result, a ranking of the model parameters concerning their variation impact for each variable is obtained.
is calculated according to Equation (16).
where
is the error of the variable
at the stimulus level k, and
is the total error for the variable
(considering all stimulus levels). Equations (17) and (18) are proposed to calculate the mentioned errors.
where
represent the experimental value of the variable
at the stimulus level k.
The model’s total sensitivity to each parameter is calculated according to Equation (19).
where I is the total number of variables evaluated;
is the maximum value of sensitivity among all the parameters for the variable
;
is the weighted sensitivity of each parameter
for the variable
;
is the weighting factor related to the variable and it is calculated according to the Equation (20).
where
is the error of the variable i, and
is the total model error. Equations (21) and (22) are proposed to calculate the mentioned errors.
corresponds to the standard 2-norm of normalized by the maximum sensitivity obtained in each variable and weighted by . Normalization of allows comparing the sensitivity measures of the parameters among different variables, whereas prioritizes the sensitivities of the parameters for which the variable’s error is more significant. As a result, a ranking of the model parameters representing the effect of their variation on the model’s whole output is obtained.
Parameter Selection Criteria
This procedure focuses on applying the selection criteria of the classified parameters concerning four different fitting approaches.
Selection for the Standardization of Simulation Conditions
It consists of selecting the model’s parameters, which can be determined from the available experimental data. It involves those related to the subjects’ characteristics, the stimulus evaluated, or the environmental conditions. They can be established by direct equivalence or by applying previously validated equations.
Selection for the Base Fitting Approach
It comprises selecting the set of parameters for which the model has the highest global sensitivity. This selection aims to reduce the model’s total prediction error by considering the parameter’s overall effect on model behavior. They correspond to the union of the set of parameters obtained in subset selection (i.e., those parameters that have been identified as well-conditioned to be adjusted, Equation (9)) and total sensitivity techniques (i.e., those parameters whose variations generate significant changes in the model output, Equation (19)). In this work, this selection is defined according to the following criteria.
Selection for a Specific Fitting Approach
It corresponds to the set of parameters for each variable’s highest sensitivity at the individual level. Its optimization aims to modify each variable’s predictability to bring it closer to the respective experimental data without significantly affecting the other predictions. It is based on relative sensitivity measures independent of the stimulus level (Equation (15)). Based on the following criteria, only one parameter is selected by each ranking obtained for the evaluated physiological variables.
Remove the parameters selected for the base fitting approach from each variable ranking.
Remove the parameters of systems and controllers that are not directly related to regulating the variable of interest.
Select only those parameters whose sensitivity is high for the variable of interest and low for the remaining ones. Parameters with high sensitivity for other variables could be selected if those variables belong to or are dependent on the same system or controller of the variable of interest.
Selection for the Stimulus-Related Fitting Approach
This corresponds to the parameter selection criteria that relate the stimulus to the regulation mechanisms addressed in the model under study. Their selection is based on the parameters’ role concerning the mechanisms mainly associated with the stimulus, highlighting the weighting factors or gains that link them to regulatory activities.
Eight mechanisms directly related to the exercise stimulus were evaluated in this work. Only one parameter per mechanism was selected.
2.1.2. Model Fitting
Fitting a parametric model involves solving an optimization problem in which the values of the set of parameters minimizing the differences between experimental data and model predictions are identified [
6]. The identification of the parameter values in this strategy results in applying an optimization algorithm in three stages that must be carried out sequentially: first, a base optimization; second, a specific optimization; and third, a stimulus-related optimization. Each stage focuses on the value identification of a specific and reduced number of parameters. It is proposed to apply the following procedures before the mentioned optimization stages to obtain correct, fast, and physiological meaning results: the standardization of simulation conditions, the selection and parameterization of the optimization algorithm, the definition of the parameter evaluation ranges, and the choice of a metric to evaluate the model’s goodness of fit [
33]. Each procedure and optimization stage is detailed below.
Standardization of Simulation Conditions
Its objective is to bring the simulation conditions close to the data used as a fitting reference. To do this, it proposes modifying some model parameters using the values obtained from the experimental data. It replaces the selected parameters’ values with the direct equivalences or results of applying previously validated equations. Its implementation has been previously presented in works on the design and fitting of physiological models, e.g., for the estimation of blood volumes and mechanical characteristics of cardiovascular and respiratory systems [
8,
34,
35]. It reduces the number of fitting candidates and, therefore, the complexity of the optimization problem and the possibility of multiple solutions.
Optimization Algorithm
Different optimization algorithms reported could be applied for the fitting of physiological models. They are divided into those that use deterministic or stochastic methods. Their correct selection depends on the model’s specific characteristics under study and the validation requirements [
33,
36].
In this paper, an evolutionary strategy with a covariance matrix and adaptation (CMA-ES) was selected. It is a stochastic global optimization algorithm based on adaptive and evolutionary strategies [
37]. This algorithm was selected considering the best convergence speed, precision, and accuracy results reported in a comparative study concerning a physiological model similar to the case study [
33].
Parameterization of the Optimization Algorithm
This corresponds to the parameter assignment of the selected optimization algorithm. It is generally related to the number of evaluations, iterations, and error tolerances. These parameters are specific to the algorithm and must be defined based on the fitting’s strictness and computational cost.
The parameter values used for implementing the CMA-ES algorithm are presented in
Table 1. These values are similar to those reported by [
33], considering the similarity regarding the case study model and that the fitting’s strictness is analogous to the desired one.
Evaluation Ranges of the Parameters
The optimization algorithms seek to identify model parameters through strategic variations of their values. The variation ranges should depend on the parameter’s specific function concerning the associated model mechanism since not all possible values provide a consistent result. For physiological models, in addition to obtaining predictions close to experimental data, it is desirable to find optimized values that reflect consistent physiological conditions or characteristics, further constraining the optimization problem [
33].
According to the above, this work proposes the following criteria to determine the evaluation range for each selected parameter:
Determine an initial variation range for each parameter in proportion to its nominal value. The range bounds depend on the expected closeness between the optimized and nominal values. Such closeness can be estimated overall by considering the parameter’s relationship with the condition for which its nominal value was defined and the nature of the experimental dataset for which it is intended to optimize, e.g., variation of respiratory mechanics parameters during rest and exercise [
38]. The variation range is recommended to contain the values evaluated in the parameter selection techniques.
Evaluate the values’ constraints from the equations describing the model mechanisms associated with each parameter and redefine the previously established bounds.
Redefine the variation range’s bounds if the reported information relates the parameter to the experimental conditions. Since not all model parameters are directly related to physiological measures, i.e., those from empirical equations that have been fitted to experimental data, evaluating their variations considering different works in which it has been used is necessary.
Performance Evaluation
It uses a metric that compares the model’s predictions with the experimental data. The optimization algorithm uses this measure as a criterion function to identify the goodness of fit of the model predictions for each parameter’s optimization. Different metric options have been applied in several works related to physiological models. However, the most commonly used is based on the root mean square error (RMSE) [
6,
12,
33], and its application is justified because it is considered more suitable for revealing differences in model performance [
6,
39].
This paper modified the RMSE metric to consider all analyzed variables at different stimulus levels, as expressed in Equation (23).
where
denotes the cost function for the optimization algorithm;
and
represent the variable’s experimental and simulated values;
and K indicate the number of variables and stimuli levels; the subscripts i and k denote each variable and stimulus level.
The error between predictions and experimental data is initially computed by obtaining a dimensionless measurement of each variable’s difference at each stimulus level. Subsequently, the standard 2-norm is calculated regarding stimulus levels to measure each variable’s mean trend. Finally, the global error is calculated as the mean value of every variable’s errors.
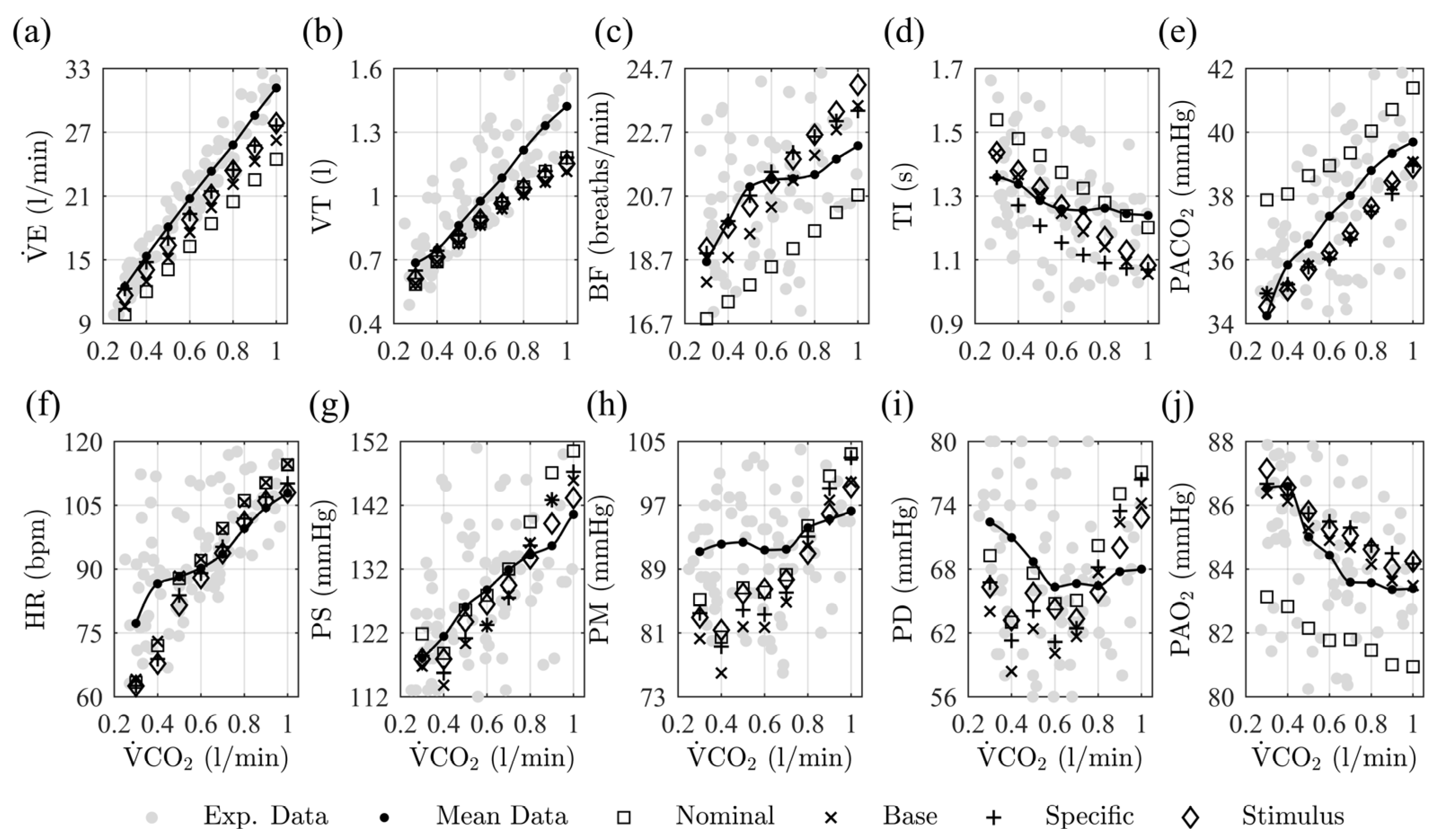
Fitting Stages
This work proposes fitting the model using three approaches. They involve those presented in the parameter selection procedure’s subsections and represent stages sequentially applied to obtain a complete fit of the case study model. In one stage, the previously fitted parameters remained fixed, and only those selected for the current one are optimized.
The first stage corresponds to a base fitting approach. It optimizes the parameters with the highest total sensitivity, whose variations have the most significant overall impact on the controllers and system outputs.
The second stage corresponds to a specific fitting approach. Each variable comprises the parameters’ optimization with the highest relative sensitivity and the least side effect for the remaining variables. This is focused on minimizing the prediction error of each variable individually.
The third stage involves a model mechanisms’ fitting approach. It optimizes the mechanisms’ parameters, mainly associated with the evaluated stimulus, to improve the predictions’ behavior.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}