
Similarities in Pathogenetic Mechanisms Underlying the Bidirectional Relationship between Endometriosis and Pelvic Inflammatory Disease

Abstract
:1. Introduction
2. Materials and Methods
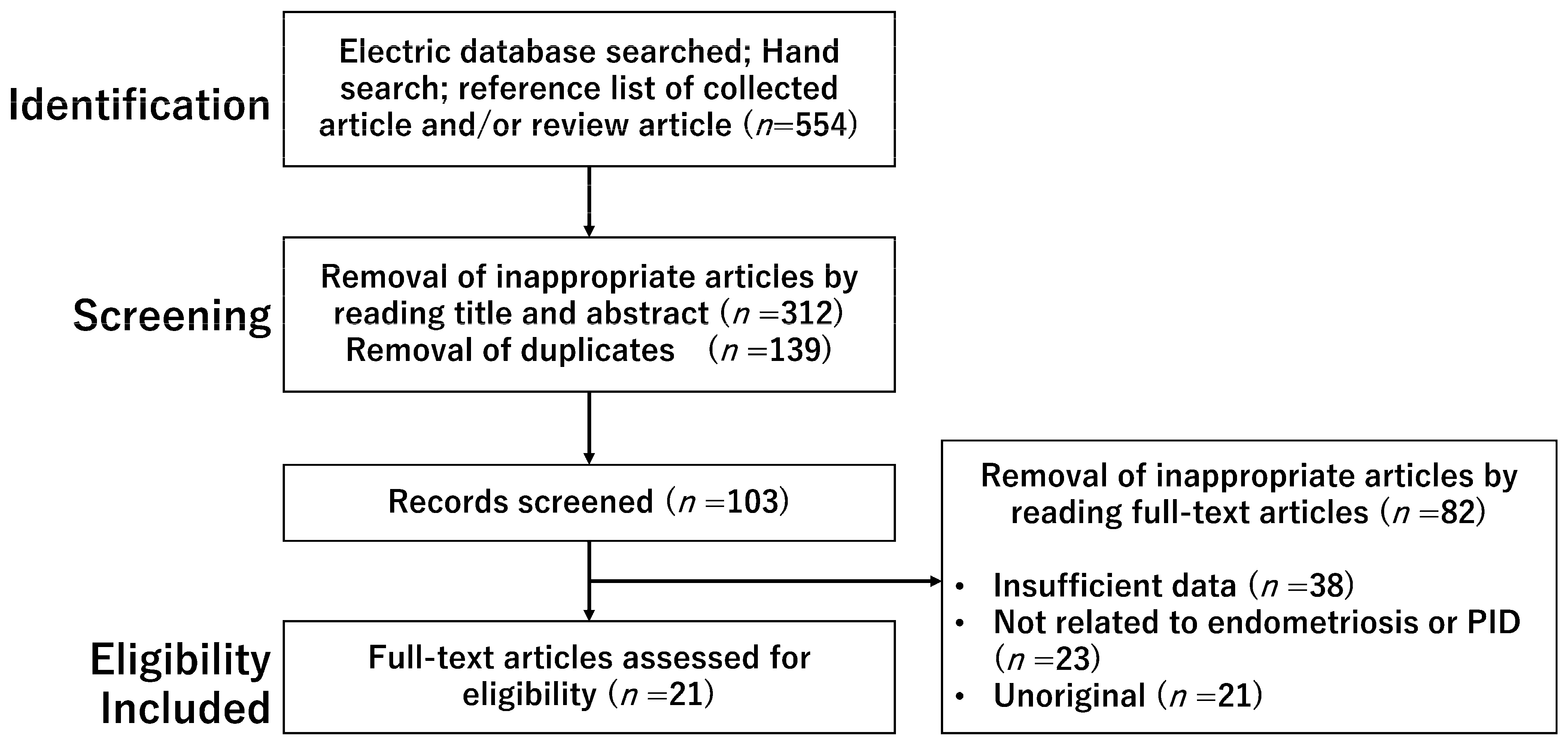
2.1. Search Strategy and Selection Criteria
2.2. Selection of Studies
3. Results
3.1. A Bidirectional Relationship between Endometriosis and PID
3.1.1. PID
3.1.2. Are Women Having PID Prone to Endometriosis?
3.1.3. Are Women Having Endometriosis Prone to PID?
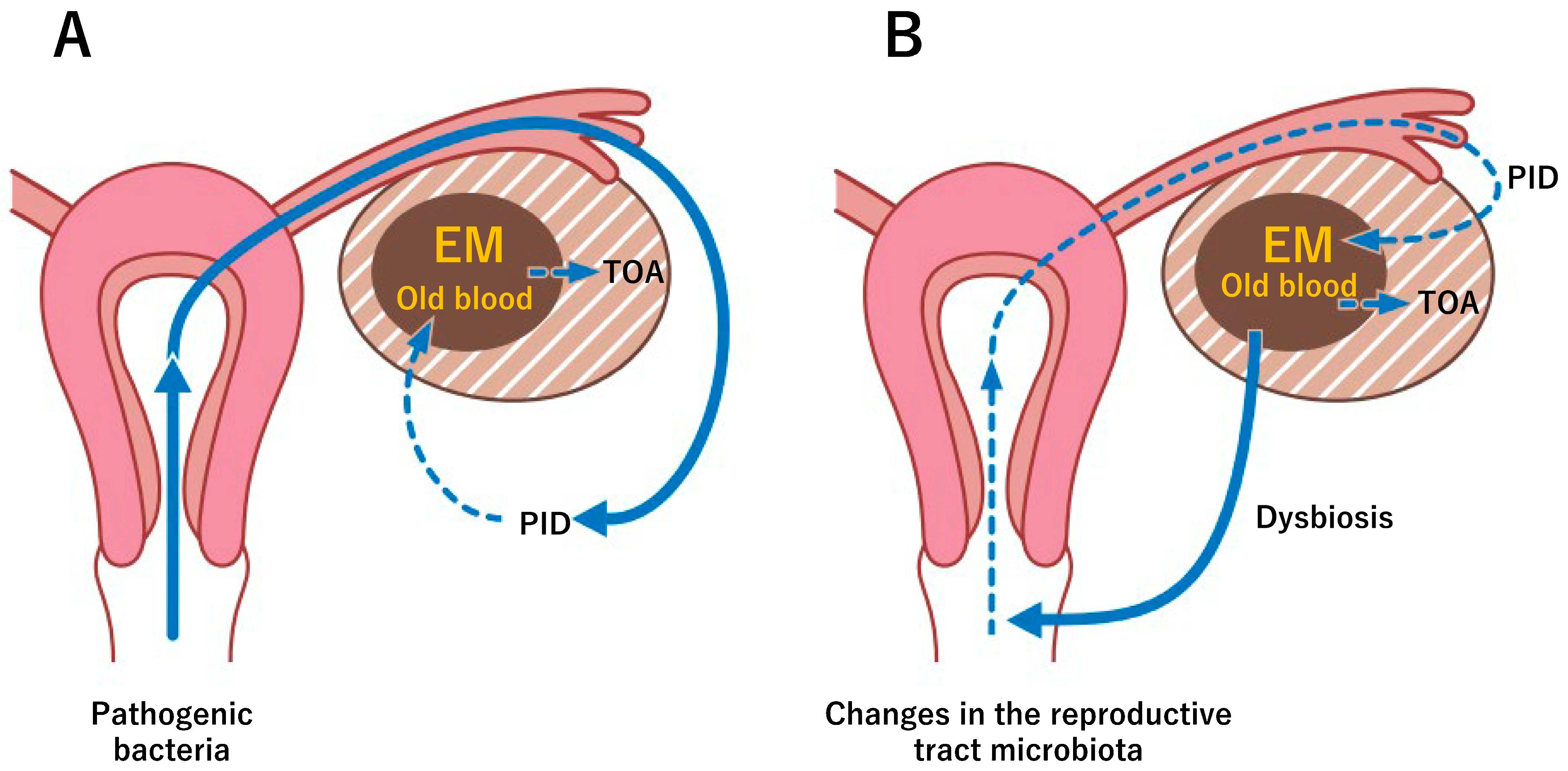
3.2. A Pathophysiological Mechanism Coupling Endometriosis and PID
3.2.1. Distortion of the Pelvic Anatomy Favoring Bacteria Proliferation
3.2.2. Nutrients from Old Blood in Endometriotic Lesions
3.2.3. Alterations of the Gut and Reproductive Tract Microbiome
3.2.4. Impaired Immune Systems
3.2.5. The Immune Landscape Modulated by Epigenetic Factors
4. Discussion
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Smolarz, B.; Szyłło, K.; Romanowicz, H. Endometriosis: Epidemiology, Classification, Pathogenesis, Treatment and Genetics (Review of Literature). Int. J. Mol. Sci. 2021, 22, 10554. [Google Scholar] [CrossRef] [PubMed]
- Kvaskoff, M.; Mu, F.; Terry, K.L.; Harris, H.R.; Poole, E.M.; Farland, L.; Missmer, S.A. Endometriosis: A high-risk population for major chronic diseases? Hum. Reprod. Update 2015, 21, 500–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koninckx, P.R.; Ussia, A.; Tahlak, M.; Adamyan, L.; Wattiez, A.; Martin, D.C.; Gomel, V. Infection as a potential cofactor in the genetic-epigenetic pathophysiology of endometriosis: A systematic review. Facts Views Vis. Obgyn 2019, 11, 209–216. [Google Scholar] [PubMed]
- Curry, A.; Williams, T.; Penny, M.L. Pelvic Inflammatory Disease: Diagnosis, Management, and Prevention. Am. Fam. Physician 2019, 100, 357–364. [Google Scholar]
- Granberg, S.; Gjelland, K.; Ekerhovd, E. The management of pelvic abscess. Best Pract. Res. Clin. Obstet. Gynaecol. 2009, 23, 667–678. [Google Scholar] [CrossRef]
- Bugg, C.W.; Taira, T. Pelvic inflammatory disease: Diagnosis and treatment in the emergency department. Emerg. Med. Pract. 2016, 18, 1–24. [Google Scholar]
- Grammatikakis, I.; Evangelinakis, N.; Salamalekis, G.; Tziortzioti, V.; Samaras, C.; Chrelias, C.; Kassanos, D. Prevalence of severe pelvic inflammatory disease and endometriotic ovarian cysts: A 7-year retrospective study. Clin. Exp. Obstet. Gynecol. 2009, 36, 235–236. [Google Scholar]
- Liu, W.; Zhang, Z.; Li, D. Primary ovarian abscess in virginal young woman with huge endometriosis cyst: A case report. Medicine 2022, 101, e29463. [Google Scholar] [CrossRef]
- Hillier, S.L.; Bernstein, K.T.; Aral, S. A Review of the Challenges and Complexities in the Diagnosis, Etiology, Epidemiology, and Pathogenesis of Pelvic Inflammatory Disease. J. Infect. Dis. 2021, 224 (Suppl. 2), S23–S28. [Google Scholar] [CrossRef]
- Chappell, C.A.; Wiesenfeld, H.C. Pathogenesis, diagnosis, and management of severe pelvic inflammatory disease and tubo-ovarian abscess. Clin. Obstet. Gynecol. 2012, 55, 893–903. [Google Scholar] [CrossRef]
- Shigemi, D.; Matsui, H.; Fushimi, K.; Yasunaga, H. Laparoscopic compared with open surgery for severe pelvic inflammatory disease and tubo-ovarian abscess. Obstet. Gynecol. 2019, 133, 1224–1230. [Google Scholar] [CrossRef]
- Mitchell, C.M.; Anyalechi, G.E.; Cohen, C.R.; Haggerty, C.L.; Manhart, L.E.; Hillier, S.L. Etiology and Diagnosis of Pelvic Inflammatory Disease: Looking Beyond Gonorrhea and Chlamydia. J. Infect. Dis. 2021, 224 (Suppl. 2), S29–S35. [Google Scholar] [CrossRef] [PubMed]
- Saini, S.; Gupta, N.; Batra, G.; Arora, D.R. Role of anaerobes in acute pelvic inflammatory disease. Indian J. Med. Microbiol. 2003, 21, 189–192. [Google Scholar] [CrossRef] [PubMed]
- Landers, D.V.; Sweet, R.L. Tubo-ovarian abscess: Contemporary approach to management. Rev. Infect. Dis. 1983, 5, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Krivak, T.C.; Cooksey, C.; Propst, A.M. Tubo-ovarian abscess: Diagnosis, medical and surgical management. Compr. Ther. 2004, 30, 93–100. [Google Scholar] [CrossRef]
- Cho, H.W.; Koo, Y.J.; Min, K.J.; Hong, J.H.; Lee, J.K. Pelvic inflammatory disease in virgin women with tubo-ovarian abscess: A single-center experience and literature review. J. Pediatr. Adolesc. Gynecol. 2017, 30, 203–208. [Google Scholar] [CrossRef]
- Kavoussi, S.K.; Pearlman, M.D.; Burke, W.M.; Lebovic, D.I. Endometrioma complicated by tubo-ovarian abscess in a woman with bacterial vaginosis. Infect. Dis. Obstet. Gynecol. 2006, 2006, 84140. [Google Scholar] [CrossRef] [Green Version]
- Veale, R.; Hughes, C.; Woolley, I. A novel case of bilateral tubo-ovarian abscesses attributed to Ruminococcus gnavus without gastrointestinal involvement. Anaerobe 2021, 67, 102312. [Google Scholar] [CrossRef]
- Gao, Y.; Qu, P.; Zhou, Y.; Ding, W. Risk factors for the development of tubo-ovarian abscesses in women with ovarian endometriosis: A retrospective matched case–control study. BMC Women’s Health 2021, 21, 43. [Google Scholar] [CrossRef]
- Grimes, D.A. Intrauterine device and upper-genital-tract infection. Lancet 2000, 356, 1013–1019. [Google Scholar] [CrossRef]
- Kapustian, V.; Namazov, A.; Yaakov, O.; Volodarsky, M.; Anteby, E.Y.; Gemer, O. Is intrauterine device a risk factor for failure of conservative management in patients with tubo-ovarian abscess? An observational retrospective study. Arch. Gynecol. Obstet. 2018, 297, 1201–1204. [Google Scholar] [CrossRef] [PubMed]
- Reed, S.D.; Landers, D.V.; Sweet, R.L. Antibiotic treatment of tuboovarian abscess: Comparison of broad-spectrum beta-lactam agents versus clindamycin-containing regimens. Am. J. Obstet. Gynecol. 1991, 164 Pt 1, 1556–1561. [Google Scholar] [CrossRef] [PubMed]
- Topçu, H.O.; Kokanalı, K.; Güzel, A.I.; Tokmak, A.; Erkılınç, S.; Ümit, C.; Doğanay, M. Risk factors for adverse clinical outcomes in patients with tubo-ovarian abscess. J. Obstet. Gynaecol. 2015, 35, 699–702. [Google Scholar] [CrossRef]
- Jiang, X.; Shi, M.; Sui, M.; Wang, T.; Yang, H.; Zhou, H.; Zhao, K. Clinical value of early laparoscopic therapy in the management of tubo-ovarian or pelvic abscess. Exp. Ther. Med. 2019, 18, 1115–1122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, L.; Ma, H.; Liang, J.; Li, L.; Shen, A.; Wang, J.; Li, H.; Tong, X. Effectiveness and Adverse Events of Early Laparoscopic Therapy versus Conservative Treatment for Tubo-Ovarian or Pelvic Abscess: A Single-Center Retrospective Cohort Study. Gynecol. Obstet. Investig. 2019, 84, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Kinay, T.; Unlubilgin, E.; Cirik, D.A.; Kayikcioglu, F.; Akgul, M.A.; Dolen, I. The value of ultrasonographic tubo-ovarian abscess morphology in predicting whether patients will require surgical treatment. Int. J. Gynaecol. Obstet. 2016, 135, 77–81. [Google Scholar] [CrossRef]
- Hakim, J.; Childress, K.J.; Hernandez, A.M.; Bercaw-Pratt, J.L. Tubo-Ovarian Abscesses in Nonsexually Active Adolescent Females: A Large Case Series. J. Adolesc. Health. 2019, 65, 303–305. [Google Scholar] [CrossRef]
- Simpson-Camp, L.; Richardson, E.J.; Alaish, S.M. Streptococcus viridans tubo-ovarian abscess in an adolescent virgin. Pediatr. Int. 2012, 54, 706–709. [Google Scholar] [CrossRef]
- Goodwin, K.; Fleming, N.; Dumont, T. Tubo-ovarian abscess in virginal adolescent females: A case report and review of the literature. J. Pediatr. Adolesc. Gynecol. 2013, 26, e99–e102. [Google Scholar] [CrossRef]
- Matsuda, N.; Jwa, S.C.; Tamura, S.; Suzuki, H.; Takamura, M.; Namba, A.; Kajihara, T.; Okagaki, R.; Kamei, Y.; Ishihara, O. Factors associated with an unfavorable clinical course in hospitalized patients with pelvic inflammatory disease: A retrospective cohort study of 117 patients from a Japanese academic institution. BMC Women’s Health 2022, 22, 348. [Google Scholar] [CrossRef]
- Elizur, S.E.; Lebovitz, O.; Weintraub, A.Y.; Eisenberg, V.H.; Seidman, D.S.; Goldenberg, M.; Soriano, D. Pelvic inflammatory disease in women with endometriosis is more severe than in those without. Aust. N. Z. J. Obstet. Gynaecol. 2014, 54, 162–165. [Google Scholar] [CrossRef]
- Tai, F.W.; Chang, C.Y.; Chiang, J.H.; Lin, W.C.; Wan, L. Association of Pelvic Inflammatory Disease with Risk of Endometriosis: A Nationwide Cohort Study Involving 141,460 Individuals. J. Clin. Med. 2018, 7, 379. [Google Scholar] [CrossRef] [Green Version]
- Zografou Themeli, M.; Nirgianakis, K.; Neumann, S.; Imboden, S.; Mueller, M.D. Endometriosis is a risk factor for recurrent pelvic inflammatory disease after tubo-ovarian abscess surgery. Arch. Gynecol. Obstet. 2022, 307, 139–148. [Google Scholar] [CrossRef]
- Clarizia, R.; Capezzuoli, T.; Ceccarello, M.; Zorzi, C.; Stepniewska, A.; Roviglione, G.; Mautone, D.; Petraglia, F.; Ceccaroni, M. Inflammation calls for more: Severe pelvic inflammatory disease with or without endometriosis. Outcomes on 311 laparoscopically treated women. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 101811. [Google Scholar] [CrossRef]
- Li, H.; Zhao, Y.; Chang, X.H.; Wang, Y.; Zhu, H.L. Clinical characteristics, treatment status and complications in women with tube ovarian abscess and endometriosis: A retrospective study. BMC Women’s Health 2021, 21, 109. [Google Scholar] [CrossRef]
- Chen, M.J.; Yang, J.H.; Yang, Y.S.; Ho, H.N. Increased occurrence of tubo-ovarian abscesses in women with stage III and IV endometriosis. Fertil. Steril. 2004, 82, 498–499. [Google Scholar] [CrossRef] [PubMed]
- Villette, C.; Bourret, A.; Santulli, P.; Gayet, V.; Chapron, C.; de Ziegler, D. Risks of tubo-ovarian abscess in cases of endometrioma and assisted reproductive technologies are both under- and overreported. Fertil. Steril. 2016, 106, 410–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegenthaler, F.; Krause, E.; Mueller, M.D. Management of pelvic inflammatory disease. Ther. Umsch. 2020, 77, 164–170. [Google Scholar] [CrossRef]
- Padilla, S.L. Ovarian abscess following puncture of an endometrioma during ultrasound-guided oocyte retrieval. Hum. Reprod. 1993, 8, 1282–1283. [Google Scholar] [CrossRef] [PubMed]
- Yaron, Y.; Peyser, M.R.; Samuel, D.; Amit, A.; Lessing, J.B. Infected endometriotic cysts secondary to oocyte aspiration for in-vitro fertilization. Hum. Reprod. 1994, 9, 1759–1760. [Google Scholar] [CrossRef]
- Younis, J.S.; Ezra, Y.; Laufer, N.; Ohel, G. Late manifestation of pelvic abscess following oocyte retrieval, for in vitro fertilization, in patients with severe endometriosis and ovarian endometriomata. J. Assist. Reprod. Genet. 1997, 14, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Romero, B.; Aibar, L.; Navarro, L.M.; Fontes, J.; Calderón, M.A.; Mozas, J. Pelvic abscess after oocyte retrieval in women with endometriosis: A case series. Iran. J. Reprod. Med. 2013, 11, 677–680. [Google Scholar] [PubMed]
- Moini, A.; Riazi, K.; Amid, V.; Ashrafi, M.; Tehraninejad, E.; Madani, T.; Owj, M. Endometriosis may contribute to oocyte retrieval-induced pelvic inflammatory disease: Report of eight cases. J. Assist. Reprod. Genet. 2005, 22, 307–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mabrouk, M.; Di Donato, N.; Montanari, G.; Savelli, L.; Ferrini, G.; Seracchioli, R. Do women with deep infiltrating endometriosis have more tubal alterations? Objective evaluation of 473 patients. J. Reprod. Med. 2013, 58, 417–424. [Google Scholar]
- Friedman, M.A.; Aguilar, L.; Heyward, Q.; Wheeler, C.; Caldamone, A. Screening for Mullerian anomalies in patients with unilateral renal agenesis: Leveraging early detection to prevent complications. J. Pediatr. Urol. 2018, 14, 144–149. [Google Scholar] [CrossRef]
- Tachedjian, G.; Aldunate, M.; Bradshaw, C.S.; Cone, R.A. The role of lactic acid production by probiotic Lactobacillus species in vaginal health. Res. Microbiol. 2017, 168, 782–792. [Google Scholar] [CrossRef]
- Awulachew, E.; Diriba, K.; Awoke, N. Bacterial Isolates from CSF Samples and Their Antimicrobial Resistance Patterns Among Children Under Five Suspected to Have Meningitis in Dilla University Referral Hospital. Infect. Drug Resist. 2020, 13, 4193–4202. [Google Scholar] [CrossRef]
- Profet, M. Menstruation as a defense against pathogens transported by sperm. Q. Rev. Biol. 1993, 68, 335–386. [Google Scholar] [CrossRef] [Green Version]
- Mak, P.; Wójcik, K.; Wicherek, L.; Suder, P.; Dubin, A. Antibacterial hemoglobin peptides in human menstrual blood. Peptides 2004, 25, 1839–1847. [Google Scholar] [CrossRef]
- Chen, C.; Song, X.; Wei, W.; Zhong, H.; Dai, J.; Lan, Z.; Li, F.; Yu, X.; Feng, Q.; Wang, Z.; et al. The microbiota continuum along the female reproductive tract and its relation to uterine-related diseases. Nat. Commun. 2017, 8, 875. [Google Scholar] [CrossRef] [Green Version]
- Christen, U. Pathogen infection and autoimmune disease. Clin. Exp. Immunol. 2019, 195, 10–14. [Google Scholar] [CrossRef] [Green Version]
- Bach, J.F. The hygiene hypothesis in autoimmunity: The role of pathogens and commensals. Nat. Rev. Immunol. 2018, 18, 105–120. [Google Scholar] [CrossRef]
- Jain, N. The early life education of the immune system: Moms, microbes and (missed) opportunities. Gut Microbes 2020, 12, 1824564. [Google Scholar] [CrossRef]
- Jiang, I.; Yong, P.J.; Allaire, C.; Bedaiwy, M.A. Intricate Connections between the Microbiota and Endometriosis. Int. J. Mol. Sci. 2021, 22, 5644. [Google Scholar] [CrossRef]
- Lin, W.C.; Chang, C.Y.; Hsu, Y.A.; Chiang, J.H.; Wan, L. Increased Risk of Endometriosis in Patients With Lower Genital Tract Infection: A Nationwide Cohort Study. Medicine 2016, 95, e2773. [Google Scholar] [CrossRef]
- Yuan, M.; Li, D.; Zhang, Z.; Sun, H.; An, M.; Wang, G. Endometriosis Induces Gut Microbiota Alterations in Mice. Hum. Reprod. 2018, 33, 607–616. [Google Scholar] [CrossRef] [Green Version]
- Bailey, M.T.; Coe, C.L. Endometriosis Is Associated with an Altered Profile of Intestinal Microflora in Female Rhesus Monkeys. Hum. Reprod. 2002, 17, 1704–1708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravel, J.; Moreno, I.; Simón, C. Bacterial vaginosis and its association with infertility, endometritis, and pelvic inflammatory disease. Am. J. Obstet. Gynecol. 2021, 224, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Khan, K.N.; Kitajima, M.; Yamaguchi, N.; Fujishita, A.; Nakashima, M.; Ishimaru, T.; Masuzaki, H. Role of prostaglandin E2 in bacterial growth in women with endometriosis. Hum. Reprod. 2012, 27, 3417–3424. [Google Scholar] [CrossRef] [Green Version]
- Khan, K.N.; Kitajima, M.; Hiraki, K.; Yamaguchi, N.; Katamine, S.; Matsuyama, T.; Nakashima, M.; Fujishita, A.; Ishimaru, T.; Masuzaki, H. Escherichia coli contamination of menstrual blood and effect of bacterial endotoxin on endometriosis. Fertil. Steril. 2010, 94, 2860–2863.e3. [Google Scholar] [CrossRef] [Green Version]
- Giordano, N.P.; Cian, M.B.; Dalebroux, Z.D. Outer Membrane Lipid Secretion and the Innate Immune Response to Gram-Negative Bacteria. Infect. Immun. 2020, 88, e00920-19. [Google Scholar] [CrossRef]
- Serezani, C.H.; Chung, J.; Ballinger, M.N.; Moore, B.B.; Aronoff, D.M.; Peters-Golden, M. Prostaglandin E2 suppresses bacterial killing in alveolar macrophages by inhibiting NADPH oxidase. Am. J. Respir. Cell Mol. Biol. 2007, 37, 562–570. [Google Scholar] [CrossRef] [Green Version]
- Noh, E.J.; Kim, D.J.; Lee, J.Y.; Park, J.H.; Kim, J.S.; Han, J.W.; Kim, B.C.; Kim, C.J.; Lee, S.K. Ureaplasma Urealyticum Infection Contributes to the Development of Pelvic Endometriosis Through Toll-Like Receptor 2. Front. Immunol. 2019, 10, 2373. [Google Scholar] [CrossRef]
- Berbic, M.; Fraser, I.S. Immunology of normal and abnormal menstruation. Womens Health 2013, 9, 387–395. [Google Scholar] [CrossRef] [Green Version]
- Symons, L.K.; Miller, J.E.; Kay, V.R.; Marks, R.M.; Liblik, K.; Koti, M.; Tayade, C. The immunopathophysiology of endometriosis. Trends Mol. Med. 2018, 24, 748–762. [Google Scholar] [CrossRef]
- Khan, K.N.; Yamamoto, K.; Fujishita, A.; Muto, H.; Koshiba, A.; Kuroboshi, H.; Saito, S.; Teramukai, S.; Nakashima, M.; Kitawaki, J. Differential levels of regulatory T cells and T-helper-17 cells in women with early and advanced endometriosis. J. Clin. Endocrinol. Metab. 2019, 104, 4715–4729. [Google Scholar] [CrossRef]
- Hill, J.A.; Faris, H.M.; Schiff, I.; Anderson, D.J. Characterization of leukocyte subpopulations in the peritoneal fluid of women with endometriosis. Fertil. Steril. 1988, 50, 216–222. [Google Scholar] [CrossRef]
- Sikora, J.; Mielczarek-Palacz, A.; Kondera-Anasz, Z. Role of natural killer cell activity in the pathogenesis of endometriosis. Curr. Med. Chem. 2011, 18, 200–208. [Google Scholar] [CrossRef]
- Olkowska-Truchanowicz, J.; Bocian, K.; Maksym, R.B.; Bialoszewska, A.; Wlodarczyk, D.; Baranowski, W.; Ząbek, J.; Korczak-Kowalska, G.; Malejczyk, J. CD4+ CD25+ FOXP3+ regulatory T cells in peripheral blood and peritoneal fluid of patients with endometriosis. Hum. Reprod. 2013, 28, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Fainaru, O.; Adini, A.; Benny, O.; Adini, I.; Short, S.; Bazinet, L.; Nakai, K.; Pravda, E.; Hornstein, M.D.; D’Amato, R.J.; et al. Dendritic cells support angiogenesis and promote lesion growth in a murine model of endometriosis. FASEB J. 2008, 22, 522–529. [Google Scholar] [CrossRef]
- Szukiewicz, D. Epigenetic regulation and T-cell responses in endometriosis-something other than autoimmunity. Front. Immunol. 2022, 13, 943839. [Google Scholar] [CrossRef]
- Rier, S.E.; Yeaman, G.R. Immune aspects of endometriosis: Relevance of the uterine mucosal immune system. Semin. Reprod. Endocrinol. 1997, 15, 209–220. [Google Scholar] [CrossRef]
- Laux-Biehlmann, A.; d’Hooghe, T.; Zollner, T.M. Menstruation pulls the trigger for inflammation and pain in endometriosis. Trends Pharmacol. Sci. 2015, 36, 270–276. [Google Scholar] [CrossRef]
- Darville, T. Pelvic Inflammatory Disease Due to Neisseria gonorrhoeae and Chlamydia trachomatis: Immune Evasion Mechanisms and Pathogenic Disease Pathways. J. Infect. Dis. 2021, 224 (Suppl. 2), S39–S46. [Google Scholar] [CrossRef]
- Miller, J.E.; Lingegowda, H.; Symons, L.K.; Bougie, O.; Young, S.L.; Lessey, B.A.; Koti, M.; Tayade, C. IL-33 activates group 2 innate lymphoid cell expansion and modulates endometriosis. JCI Insight 2021, 6, e149699. [Google Scholar] [CrossRef]
- Gogacz, M.; Winkler, I.; Bojarska-Junak, A.; Tabarkiewicz, J.; Semczuk, A.; Rechberger, T.; Adamiak, A. T regulatory lymphocytes in patients with endometriosis. Mol. Med. Rep. 2014, 10, 1072–1076. [Google Scholar] [CrossRef] [Green Version]
- Rowe, J.H.; Ertelt, J.M.; Way, S.S. Foxp3(+) regulatory T cells, immune stimulation and host defence against infection. Immunology 2012, 136, 1–10. [Google Scholar] [CrossRef]
- Patel, B.G.; Rudnicki, M.; Yu, J.; Shu, Y.; Taylor, R.N. Progesterone resistance in endometriosis: Origins, consequences and interventions. Acta Obstet. Gynecol. Scand. 2017, 96, 623–632. [Google Scholar] [CrossRef] [Green Version]
- Trukhacheva, E.; Lin, Z.; Reierstad, S.; Cheng, Y.H.; Milad, M.; Bulun, S.E. Estrogen receptor (ER) beta regulates ERalpha expression in stromal cells derived from ovarian endometriosis. J. Clin. Endocrinol. Metab. 2009, 94, 615–622. [Google Scholar] [CrossRef]
- Ho, H.N.; Wu, M.Y.; Yang, Y.S. Peritoneal cellular immunity and endometriosis. Am. J. Reprod. Immunol. 1997, 38, 400–412. [Google Scholar] [CrossRef]
- Binnie, A.; Tsang, J.L.Y.; Hu, P.; Carrasqueiro, G.; Castelo-Branco, P.; Dos Santos, C.C. Epigenetics of Sepsis. Crit. Care Med. 2020, 48, 745–756. [Google Scholar] [CrossRef] [PubMed]
- Kitaya, K.; Yasuo, T. Commonalities and Disparities between Endometriosis and Chronic Endometritis: Therapeutic Potential of Novel Antibiotic Treatment Strategy against Ectopic Endometrium. Int. J. Mol. Sci. 2023, 24, 2059. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Search Mode | The Keyword and Search Term Combinations |
|---|---|
| Search term 1 | endometriosis OR endometrioma OR ovarian endometrioma |
| Search term 2 | pelvic inflammatory disease |
| Search term 3 | immune response OR immune system OR innate OR adaptive |
| Search term 4 | microbiota OR microbiome OR commensal OR pathogenic |
| Search term 5 | tubo-ovarian abscess OR ovarian abscess |
| Search | Search term 1 AND Search term 2 |
| Search term 1 AND Search term 2 AND Search term 3 | |
| Search term 1 AND Search term 2 AND Search term 4 | |
| Search term 1 AND Search term 2 AND Search term 5 | |
| Search term 1 AND Search term 3 AND Search term 4 | |
| Search term 2 AND Search term 3 AND Search term 5 | |
| Search term 1 AND Search term 5 | |
| Search term 2 AND Search term 5 | |
| Search term 1 AND Search term 2 AND Search term 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kobayashi, H. Similarities in Pathogenetic Mechanisms Underlying the Bidirectional Relationship between Endometriosis and Pelvic Inflammatory Disease. Diagnostics 2023, 13, 868. https://doi.org/10.3390/diagnostics13050868
Kobayashi H. Similarities in Pathogenetic Mechanisms Underlying the Bidirectional Relationship between Endometriosis and Pelvic Inflammatory Disease. Diagnostics. 2023; 13(5):868. https://doi.org/10.3390/diagnostics13050868
Chicago/Turabian StyleKobayashi, Hiroshi. 2023. "Similarities in Pathogenetic Mechanisms Underlying the Bidirectional Relationship between Endometriosis and Pelvic Inflammatory Disease" Diagnostics 13, no. 5: 868. https://doi.org/10.3390/diagnostics13050868