


Meta-Analysis of Cardiovascular Risk Factors in Offspring of Preeclampsia Pregnancies
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Retrieval Strategies
2.2. Inclusion and Exclusion Criteria
2.3. Literature Inclusion and Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Basic Characteristics of the Literature
3.2. Results of Meta-Analysis
3.2.1. Systolic Blood Pressure
3.2.2. Diastolic Blood Pressure
3.2.3. Total Cholesterol
3.2.4. Low-Density Lipoprotein Cholesterol
3.2.5. High-Density Lipoprotein Cholesterol
3.2.6. Non-HDL Cholesterol
3.2.7. Triglycerides
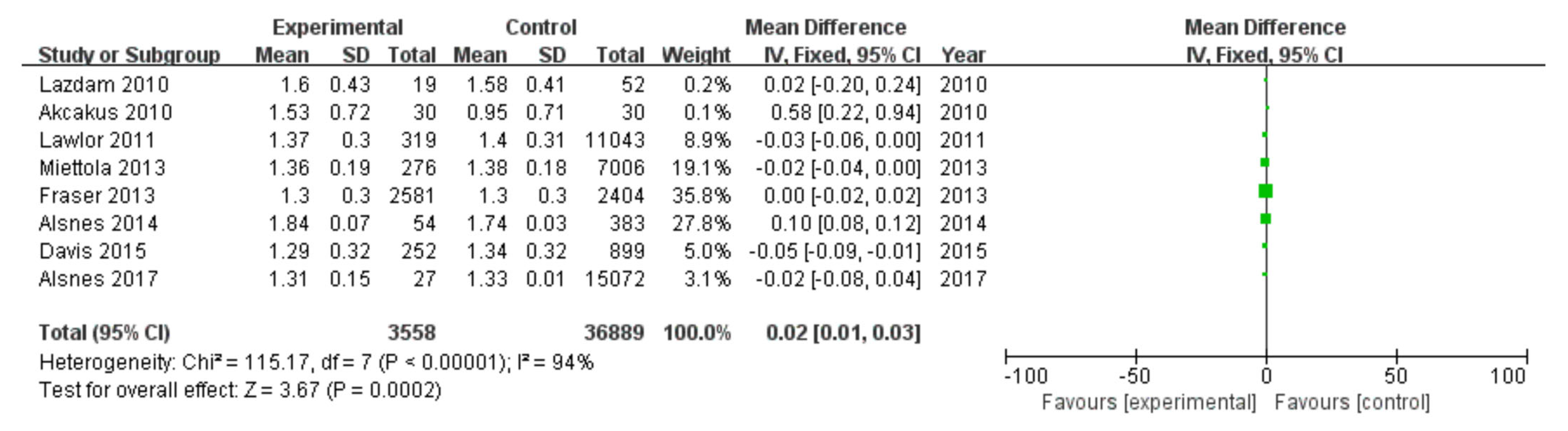
3.2.8. Glucose
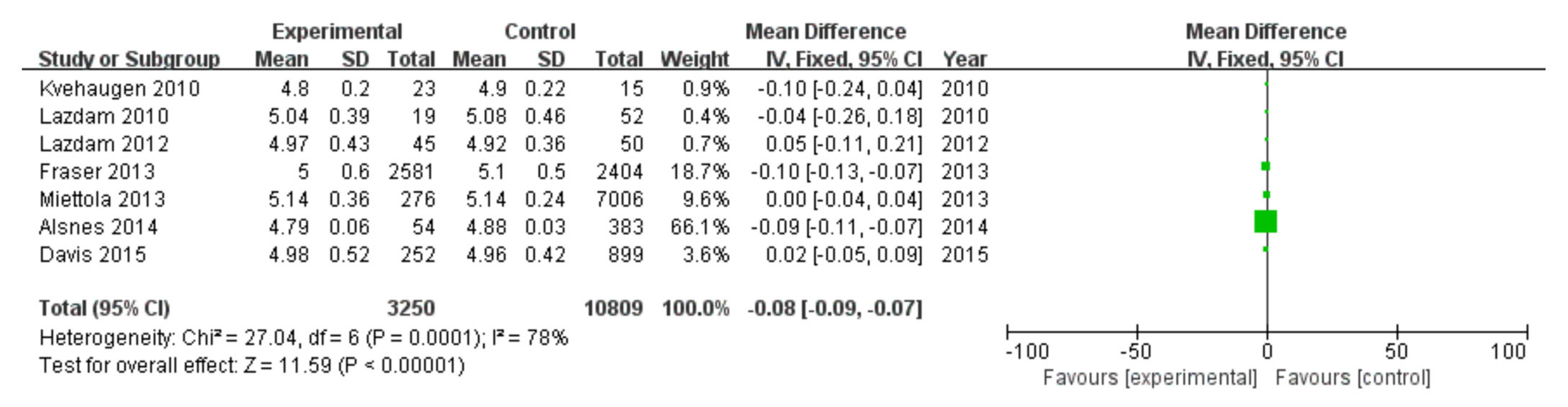
3.2.9. Insulin
3.2.10. BMI
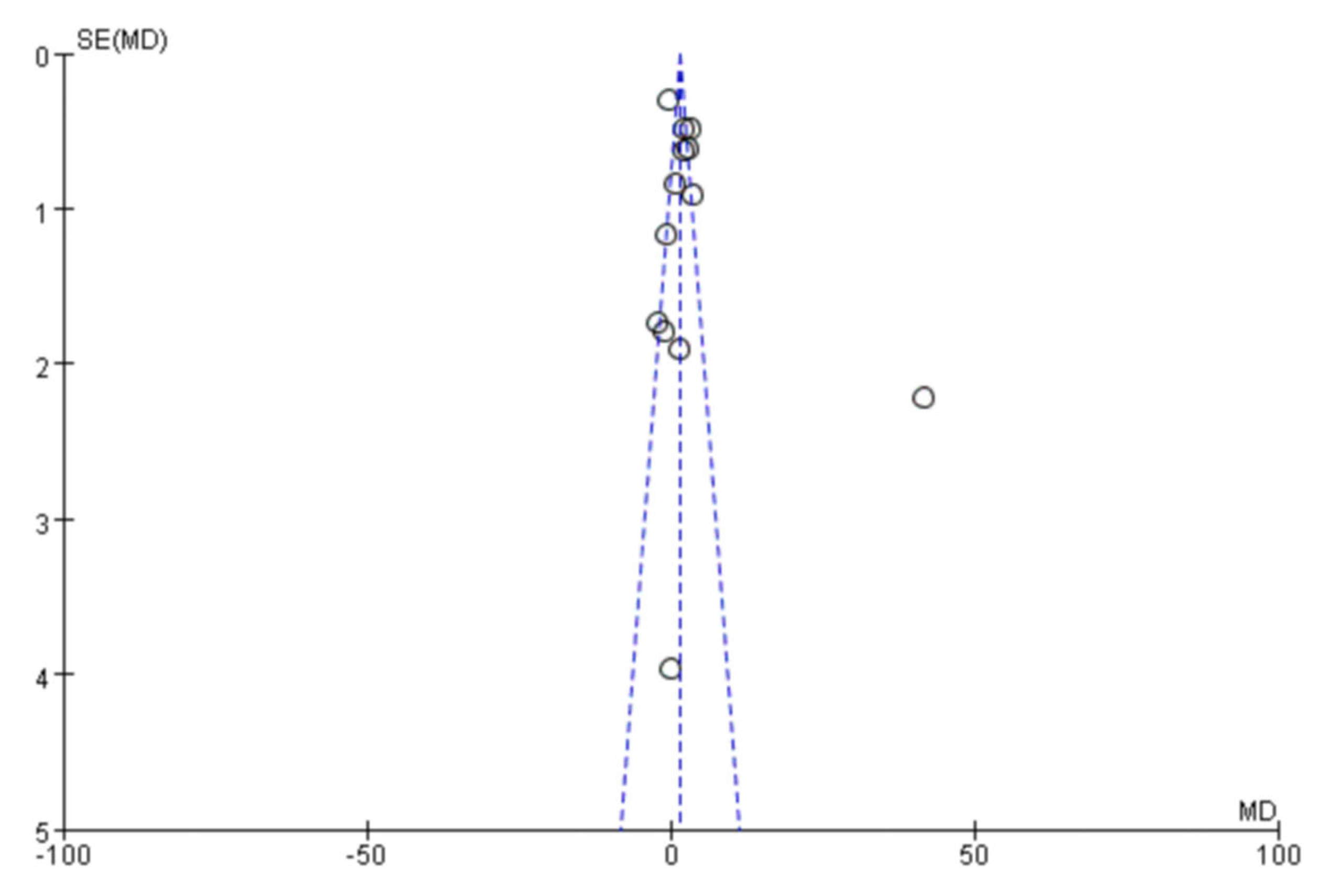
3.3. Analysis of Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kuehn, B.M. Rising Prepregnancy Hypertension, Preeclampsia Disparities Raise Alarm. Circulation 2021, 143, 753–754. [Google Scholar] [CrossRef] [PubMed]
- Sutton, E.F.; Gemmel, M.; Powers, R.W. Nitric oxide signaling in pregnancy and preeclampsia. Nitric Oxide 2020, 95, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Barr, L.; Pudwell, J.; Herr, J.; Johri, A.; Smith, G. Microvascular outcomes of a pregnancy complicated by preeclampsia. Can. J. Cardiol. 2021, 37, e12. [Google Scholar] [CrossRef]
- Le, Q.; Akhter, R.; Coulton, K.; Vo, N.; Duong, L.; Nong, H.; Yaacoub, A.; Condous, G.; Eberhard, J.; Nanan, R. Periodontitis and preeclampsia in pregnancy: A systematic review and meta-analysis. Matern. Child Health J. 2022, 26, 2419–2443. [Google Scholar] [CrossRef] [PubMed]
- Karatza, A.A.; Dimitriou, G. Preeclampsia Emerging as a Novel Risk Factor for Cardiovascular Disease in the Offspring. Curr. Pediatr. Rev. 2020, 16, 194–199. [Google Scholar] [CrossRef]
- Wang, Y.; Wu, N.; Shen, H. A Review of Research Progress of Pregnancy with Twins with Preeclampsia. Risk Manag. Healthc. Policy 2021, 14, 1999–2010. [Google Scholar] [CrossRef]
- Qu, H.; Khalil, R.A. Vascular mechanisms and molecular targets in hypertensive pregnancy and preeclampsia. Am. J. Physiol.-Heart Circ. Physiol. 2020, 319, H661–H681. [Google Scholar] [CrossRef]
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef]
- Ha, M.; Park, J. Shiftwork and metabolic risk factors of cardiovascular disease. J. Occup. Health 2005, 47, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Smith, G.N.; Walker, M.C.; Liu, A.; Wen, S.W.; Swansburg, M.; Ramshaw, H.; White, R.R.; Roddy, M.; Hladunewich, M. A history of preeclampsia identifies women who have underlying cardiovascular risk factors. Am. J. Obstet. Gynecol. 2009, 200, 58.E1–58.E8. [Google Scholar] [CrossRef]
- Heida, K.Y.; Bots, M.L.; de Groot, C.J.; van Dunné, F.M.; Hammoud, N.M.; Hoek, A.; Laven, J.S.; Maas, A.H.; Roeters van Lennep, J.E.; Velthuis, B.K.; et al. Cardiovascular risk management after reproductive and pregnancy-related disorders: A Dutch multidisciplinary evidence-based guideline. Eur. J. Prev. Cardiol. 2016, 23, 1863–1879. [Google Scholar] [CrossRef]
- Kajantie, E.; Eriksson, J.G.; Osmond, C.; Thornburg, K.; Barker, D.J. Pre-eclampsia is associated with increased risk of stroke in the adult offspring: The Helsinki birth cohort study. Stroke 2009, 40, 1176–1180. [Google Scholar] [CrossRef] [Green Version]
- Davis, E.F.; Lazdam, M.; Lewandowski, A.J.; Worton, S.A.; Kelly, B.; Kenworthy, Y.; Adwani, S.; Wilkinson, A.R.; McCormick, K.; Sargent, I.; et al. Cardiovascular risk factors in children and young adults born to preeclamptic pregnancies: A systematic review. Pediatrics 2012, 129, e1552–e1561. [Google Scholar] [CrossRef]
- Akcakus, M.; Altunay, L.; Yikilmaz, A.; Yazici, C.; Koklu, E. The relationship between abdominal aortic intima-media thickness and lipid profile in neonates born to mothers with preeclampsia. J. Pediatr. Endocrinol. Metab. 2010, 23, 1143–1149. [Google Scholar] [CrossRef] [PubMed]
- Lazdam, M.; de la Horra, A.; Pitcher, A.; Mannie, Z.; Diesch, J.; Trevitt, C.; Kylintireas, I.; Contractor, H.; Singhal, A.; Lucas, A.; et al. Elevated blood pressure in offspring born premature to hypertensive pregnancy: Is endothelial dysfunction the underlying vascular mechanism? Hypertension 2010, 56, 159–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kvehaugen, A.S.; Andersen, L.F.; Staff, A.C. Anthropometry and cardiovascular risk factors in women and offspring after pregnancies complicated by preeclampsia or diabetes mellitus. Acta Obstet. Gynecol. Scand. 2010, 89, 1478–1485. [Google Scholar] [CrossRef]
- Geelhoed, J.J.; Fraser, A.; Tilling, K.; Benfield, L.; Davey Smith, G.; Sattar, N.; Nelson, S.M.; Lawlor, D.A. Preeclampsia and gestational hypertension are associated with childhood blood pressure independently of family adiposity measures: The Avon Longitudinal Study of Parents and Children. Circulation 2010, 122, 1192–1199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jayet, P.Y.; Rimoldi, S.F.; Stuber, T.; Salmòn, C.S.; Hutter, D.; Rexhaj, E.; Thalmann, S.; Schwab, M.; Turini, P.; Sartori-Cucchia, C.; et al. Pulmonary and systemic vascular dysfunction in young offspring of mothers with preeclampsia. Circulation 2010, 122, 488–494. [Google Scholar] [CrossRef] [Green Version]
- Fugelseth, D.; Ramstad, H.B.; Kvehaugen, A.S.; Nestaas, E.; Støylen, A.; Staff, A.C. Myocardial function in offspring 5-8years after pregnancy complicated by preeclampsia. Early Hum. Dev. 2011, 87, 531–535. [Google Scholar] [CrossRef]
- Lawlor, D.A.; Macdonald-Wallis, C.; Fraser, A.; Nelson, S.M.; Hingorani, A.; Davey Smith, G.; Sattar, N.; Deanfield, J. Cardiovascular biomarkers and vascular function during childhood in the offspring of mothers with hypertensive disorders of pregnancy: Findings from the Avon Longitudinal Study of Parents and Children. Eur. Heart J. 2012, 33, 335–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kvehaugen, A.S.; Dechend, R.; Ramstad, H.B.; Troisi, R.; Fugelseth, D.; Staff, A.C. Endothelial function and circulating biomarkers are disturbed in women and children after preeclampsia. Hypertension 2011, 58, 63–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazdam, M.; de la Horra, A.; Diesch, J.; Kenworthy, Y.; Davis, E.; Lewandowski, A.J.; Szmigielski, C.; Shore, A.; Mackillop, L.; Kharbanda, R.; et al. Unique blood pressure characteristics in mother and offspring after early onset preeclampsia. Hypertension 2012, 60, 1338–1345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miettola, S.; Hartikainen, A.L.; Vääräsmäki, M.; Bloigu, A.; Ruokonen, A.; Järvelin, M.R.; Pouta, A. Offspring’s blood pressure and metabolic phenotype after exposure to gestational hypertension in utero. Eur. J. Epidemiol. 2013, 28, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Fraser, A.; Nelson, S.M.; Macdonald-Wallis, C.; Sattar, N.; Lawlor, D.A. Hypertensive disorders of pregnancy and cardiometabolic health in adolescent offspring. Hypertension 2013, 62, 614–620. [Google Scholar] [CrossRef] [Green Version]
- Alsnes, I.V.; Janszky, I.; Forman, M.R.; Vatten, L.J.; Økland, I. A population-based study of associations between preeclampsia and later cardiovascular risk factors. Am. J. Obstet. Gynecol. 2014, 211, e651–e657. [Google Scholar] [CrossRef]
- Davis, E.F.; Lewandowski, A.J.; Aye, C.; Williamson, W.; Boardman, H.; Huang, R.C.; Mori, T.A.; Newnham, J.; Beilin, L.J.; Leeson, P. Clinical cardiovascular risk during young adulthood in offspring of hypertensive pregnancies: Insights from a 20-year prospective follow-up birth cohort. BMJ Open 2015, 5, e008136. [Google Scholar] [CrossRef] [Green Version]
- Reveret, M.; Boivin, A.; Guigonnis, V.; Audibert, F.; Nuyt, A.M. Preeclampsia: Effect on newborn blood pressure in the 3 days following preterm birth: A cohort study. J. Hum. Hypertens. 2015, 29, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Alsnes, I.V.; Vatten, L.J.; Fraser, A.; Bjørngaard, J.H.; Rich-Edwards, J.; Romundstad, P.R.; Åsvold, B.O. Hypertension in Pregnancy and Offspring Cardiovascular Risk in Young Adulthood: Prospective and Sibling Studies in the HUNT Study (Nord-Trøndelag Health Study) in Norway. Hypertension 2017, 69, 591–598. [Google Scholar] [CrossRef] [Green Version]
- Gürlek, B.; Yılmaz, A.; Durakoğlugil, M.E.; Karakaş, S.; Kazaz, İ.M.; Önal, Ö.; Şatıroğlu, Ö. Evaluation of serum apelin-13 and apelin-36 concentrations in preeclamptic pregnancies. J. Obstet. Gynaecol. Res. 2020, 46, 58–65. [Google Scholar] [CrossRef]
- Wolf, M.; Hubel, C.A.; Lam, C.; Sampson, M.; Ecker, J.L.; Ness, R.B.; Rajakumar, A.; Daftary, A.; Shakir, A.S.; Seely, E.W.; et al. Preeclampsia and future cardiovascular disease: Potential role of altered angiogenesis and insulin resistance. J. Clin. Endocrinol. Metab. 2004, 89, 6239–6243. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.D.; Malinowski, A.; Zhou, Q.; Yusuf, S.; Devereaux, P.J. Cardiovascular sequelae of preeclampsia/eclampsia: A systematic review and meta-analyses. Am. Heart J. 2008, 156, 918–930. [Google Scholar] [CrossRef] [PubMed]
- Craici, I.; Wagner, S.; Garovic, V.D. Preeclampsia and future cardiovascular risk: Formal risk factor or failed stress test? Ther. Adv. Cardiovasc. Dis. 2008, 2, 249–259. [Google Scholar] [CrossRef] [Green Version]
- Melchiorre, K.; Sharma, R.; Thilaganathan, B. Cardiovascular implications in preeclampsia: An overview. Circulation 2014, 130, 703–714. [Google Scholar] [CrossRef] [PubMed]
- Hibbard, J.U.; Shroff, S.G.; Lang, R.M. Cardiovascular changes in preeclampsia. Semin. Nephrol. 2004, 24, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Kattah, A.G.; Garovic, V.D. The management of hypertension in pregnancy. Adv. Chronic Kidney Dis. 2013, 20, 229–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosca, L.; Benjamin, E.J.; Berra, K.; Bezanson, J.L.; Dolor, R.J.; Lloyd-Jones, D.M.; Newby, L.K.; Piña, I.L.; Roger, V.L.; Shaw, L.J.; et al. Effectiveness-based guidelines for the prevention of cardiovascular disease in women--2011 update: A guideline from the american heart association. Circulation 2011, 123, 1243–1262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouwers, L.; van der Meiden-van Roest, A.J.; Savelkoul, C.; Vogelvang, T.E.; Lely, A.T.; Franx, A.; van Rijn, B.B. Recurrence of pre-eclampsia and the risk of future hypertension and cardiovascular disease: A systematic review and meta-analysis. BJOG 2018, 125, 1642–1654. [Google Scholar] [CrossRef] [Green Version]
- Wellmann, S.; Benzing, J.; Fleischlin, S.; Morgenthaler, N.; Fouzas, S.; Bührer, C.A.; Szinnai, G.; Burkhardt, T.; Lapaire, O. Cardiovascular biomarkers in preeclampsia at triage. Fetal. Diagn. Ther. 2014, 36, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Lei, Q.; Lv, L.J.; Zhang, B.Y.; Wen, J.Y.; Liu, G.C.; Lin, X.H.; Niu, J.M. Ante-partum and post-partum markers of metabolic syndrome in pre-eclampsia. J. Hum. Hypertens. 2011, 25, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carty, D.M.; Delles, C.; Dominiczak, A.F. Preeclampsia and future maternal health. J. Hypertens. 2010, 28, 1349–1355. [Google Scholar] [CrossRef]
- DeFronzo, R.A.; Ferrannini, E. Insulin resistance. A multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidemia, and atherosclerotic cardiovascular disease. Diabetes Care 1991, 14, 173–194. [Google Scholar] [CrossRef]
- Girouard, J.; Giguère, Y.; Moutquin, J.M.; Forest, J.C. Previous hypertensive disease of pregnancy is associated with alterations of markers of insulin resistance. Hypertension 2007, 49, 1056–1062. [Google Scholar] [CrossRef] [Green Version]
- Magnussen, E.B.; Vatten, L.J.; Smith, G.D.; Romundstad, P.R. Hypertensive disorders in pregnancy and subsequently measured cardiovascular risk factors. Obstet. Gynecol. 2009, 114, 961–970. [Google Scholar] [CrossRef] [PubMed]
- Andraweera, P.H.; Lassi, Z.S. Cardiovascular Risk Factors in Offspring of Preeclamptic Pregnancies-Systematic Review and Meta-Analysis. J. Pediatr. 2019, 208, 104–113.e106. [Google Scholar] [CrossRef] [PubMed]
- Georgianos, P.I.; Agarwal, R. Ambulatory Blood Pressure Reduction with SGLT-2 Inhibitors: Dose-Response Meta-analysis and Comparative Evaluation with Low-Dose Hydrochlorothiazide. Diabetes Care 2019, 42, 693–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mosenzon, O.; Wiviott, S.D.; Cahn, A.; Rozenberg, A.; Yanuv, I.; Goodrich, E.L.; Murphy, S.A.; Heerspink, H.J.L.; Zelniker, T.A.; Dwyer, J.P.; et al. Effects of dapagliflozin on development and progression of kidney disease in patients with type 2 diabetes: An analysis from the DECLARE-TIMI 58 randomised trial. Lancet Diabetes Endocrinol. 2019, 7, 606–617. [Google Scholar] [CrossRef]
- Rauch-Kröhnert, U.; Landmesser, U. Gliflozins-in future cardioprotective drugs? Internist 2021, 62, 786–795. [Google Scholar] [CrossRef] [PubMed]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef]
- Zhai, R.; Liu, Y.; Tong, J.; Yu, Y.; Yang, L.; Gu, Y.; Niu, J. Empagliflozin Ameliorates Preeclampsia and Reduces Postpartum Susceptibility to Adriamycin in a Mouse Model Induced by Angiotensin Receptor Agonistic Autoantibodies. Front. Pharmacol. 2022, 13, 826792. [Google Scholar] [CrossRef] [PubMed]
- Oesterle, A.; Laufs, U.; Liao, J.K. Pleiotropic Effects of Statins on the Cardiovascular System. Circ. Res. 2017, 120, 229–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, D.D.; Costantine, M.M. The role of statins in the prevention of preeclampsia. Am. J. Obstet. Gynecol. 2022, 226, S1171–S1181. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Singh, J.; Khan, Y.; Seshan, S.V.; Girardi, G. A new mouse model to explore therapies for preeclampsia. PLoS ONE 2010, 5, e13663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costantine, M.M.; Tamayo, E.; Lu, F.; Bytautiene, E.; Longo, M.; Hankins, G.D.V.; Saade, G.R. Using pravastatin to improve the vascular reactivity in a mouse model of soluble fms-like tyrosine kinase-1-induced preeclampsia. Obstet. Gynecol. 2010, 116, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Soodi, D.; VanWormer, J.J.; Rezkalla, S.H. Aspirin in Primary Prevention of Cardiovascular Events. Clin. Med. Res. 2020, 18, 89–94. [Google Scholar] [CrossRef]
- Roberge, S.; Bujold, E.; Nicolaides, K.H. Aspirin for the prevention of preterm and term preeclampsia: Systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2018, 218, 287–293.e281. [Google Scholar] [CrossRef] [Green Version]
- Rolnik, D.L.; Wright, D.; Poon, L.C.; O’Gorman, N.; Syngelaki, A.; de Paco Matallana, C.; Akolekar, R.; Cicero, S.; Janga, D.; Singh, M.; et al. Aspirin versus Placebo in Pregnancies at High Risk for Preterm Preeclampsia. N. Engl. J. Med. 2017, 377, 613–622. [Google Scholar] [CrossRef]
- Russell, C.; Keshavamurthy, S.; Saha, S. Nutraceuticals in the Management of Cardiovascular Risk Factors: Where is the Evidence? Cardiovasc. Hematol. Disord. Drug Targets 2021, 21, 150–161. [Google Scholar] [CrossRef]
- Jahangir, M.A.; Jain, P.; Verma, R.; Taleuzzaman, M.; Ahsan, M.J.; Chettupalli, A.K.; Muheem, A.; Mirza, M.A. Transdermal Nutraceuticals Delivery System for CNS Disease. CNS Neurol. Disord. Drug Targets 2022, 21, 977–993. [Google Scholar] [CrossRef]
- Breuss, J.M.; Atanasov, A.G.; Uhrin, P. Resveratrol and Its Effects on the Vascular System. Int. J. Mol. Sci. 2019, 20, 1523. [Google Scholar] [CrossRef] [Green Version]
- Rivera, L.; Morón, R.; Zarzuelo, A.; Galisteo, M. Long-term resveratrol administration reduces metabolic disturbances and lowers blood pressure in obese Zucker rats. Biochem. Pharmacol. 2009, 77, 1053–1063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozłowska, A.; Szostak-Węgierek, D. Targeting Cardiovascular Diseases by Flavonols: An Update. Nutrients 2022, 14, 1439. [Google Scholar] [CrossRef] [PubMed]
- Edwards, R.L.; Lyon, T.; Litwin, S.E.; Rabovsky, A.; Symons, J.D.; Jalili, T. Quercetin reduces blood pressure in hypertensive subjects. J. Nutr. 2007, 137, 2405–2411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Gordon, D.; Copeland, T.; D’Agostino, D.; et al. Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease. N. Engl. J. Med. 2019, 380, 33–44. [Google Scholar] [CrossRef]
- Zhao, X.; Fang, R.; Yu, R.; Chen, D.; Zhao, J.; Xiao, J. Maternal Vitamin D Status in the Late Second Trimester and the Risk of Severe Preeclampsia in Southeastern China. Nutrients 2017, 9, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heyden, E.L.; Wimalawansa, S.J. Vitamin D: Effects on human reproduction, pregnancy, and fetal well-being. J. Steroid. Biochem. Mol. Biol. 2018, 180, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Shi, D.D.; Wang, Y.; Guo, J.J.; Zhou, L.; Wang, N. Vitamin D Enhances Efficacy of Oral Nifedipine in Treating Preeclampsia with Severe Features: A Double Blinded, Placebo-Controlled and Randomized Clinical Trial. Front. Pharmacol. 2017, 8, 865. [Google Scholar] [CrossRef] [Green Version]
- Eilers, A.; Witt, S.; Walter, J. Aptamer-Modified Nanoparticles in Medical Applications. Adv. Biochem. Eng. Biotechnol. 2020, 174, 161–193. [Google Scholar] [CrossRef] [PubMed]
- Kumari, P.; Ghosh, B.; Biswas, S. Nanocarriers for cancer-targeted drug delivery. J. Drug Target. 2016, 24, 179–191. [Google Scholar] [CrossRef]
- Pereira, H.; Sousa, D.A.; Cunha, A.; Andrade, R.; Espregueira-Mendes, J.; Oliveira, J.M.; Reis, R.L. Hyaluronic Acid. Adv. Exp. Med. Biol. 2018, 1059, 137–153. [Google Scholar] [CrossRef] [PubMed]
- Vasvani, S.; Kulkarni, P.; Rawtani, D. Hyaluronic acid: A review on its biology, aspects of drug delivery, route of administrations and a special emphasis on its approved marketed products and recent clinical studies. Int. J. Biol. Macromol. 2020, 151, 1012–1029. [Google Scholar] [CrossRef] [PubMed]
- Rosso, F.; Quagliariello, V.; Tortora, C.; Di Lazzaro, A.; Barbarisi, A.; Iaffaioli, R.V. Cross-linked hyaluronic acid sub-micron particles: In vitro and in vivo biodistribution study in cancer xenograft model. J. Mater. Sci. Mater. Med. 2013, 24, 1473–1481. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year of Publication | Selection of Research Subjects (4 Points) | Comparability between Groups (2 Points) | Outcome Measurement/Exposure Factor Measurement (3 Points) | Total Scores |
|---|---|---|---|---|---|
| Mustafa Akcakus [14] | 2010 | 3 | 2 | 3 | 8 |
| Merzaka Lazdam [15] | 2010 | 3 | 2 | 2 | 7 |
| ANNE STINE Kvehaugen [16] | 2010 | 4 | 2 | 3 | 9 |
| JJ Miranda Geelhoed [17] | 2010 | 3 | 1 | 3 | 7 |
| Pierre-Yves Jayet, MD [18] | 2010 | 4 | 1 | 3 | 8 |
| Drude Fugelseth [19] | 2011 | 4 | 2 | 3 | 9 |
| Debbie Anne Lawlor [20] | 2011 | 3 | 1 | 2 | 6 |
| Anne Stine Kvehaugen [21] | 2011 | 4 | 1 | 3 | 8 |
| Merzaka Lazdam [22] | 2012 | 4 | 2 | 3 | 9 |
| Satu Miettola [23] | 2013 | 4 | 1 | 1 | 6 |
| Abigail Fraser [24] | 2013 | 4 | 2 | 2 | 8 |
| Ingvild V. Alsnes [25] | 2014 | 4 | 1 | 3 | 8 |
| Esther F Davis [26] | 2015 | 3 | 2 | 3 | 8 |
| M Reveret [27] | 2015 | 3 | 1 | 3 | 7 |
| Ingvild V. Alsnes [28] | 2017 | 4 | 1 | 2 | 7 |
| Beril Gürlek [29] | 2019 | 4 | 2 | 3 | 9 |
| Author | Year | Type of Study | N | The Studied Risk Factors | |
|---|---|---|---|---|---|
| Experimental Group | Control Group | ||||
| Mustafa Akcakus [14] | 2010 | Case-control | 30 | 30 | c,d,e,g,i |
| Merzaka Lazdam [15] | 2010 | Case-control | 19 | 52 | c,d,e,f,g,h,i,j |
| ANNE STINE Kvehaugen [16] | 2010 | Case-control | 23 | 15 | a,b,h,j |
| JJ Miranda Geelhoed [17] | 2010 | Case-control | 205 | 5345 | a,b,j |
| Pierre-Yves Jayet, MD [18] | 2010 | Case-control | 48 | 90 | a,b,j |
| Drude Fugelseth [19] | 2011 | Case-control | 25 | 15 | a,b,j |
| Debbie Anne Lawlor [20] | 2011 | Case-control | 319 | 11,043 | a,b,e,f,g,j |
| Anne Stine Kvehaugen [21] | 2011 | Case-control | 26 | 17 | a,b,j |
| Merzaka Lazdam [22] | 2012 | Case-control | 45 | 50 | c,d,g,h,i,j |
| Satu Miettola [23] | 2013 | Case-control | 276 | 7006 | a,b,c,d,e,g,h,i,j |
| Abigail Fraser [24] | 2013 | Case-control | 2581 | 2404 | a,b,c,d,e,f,g,i,j |
| Ingvild V. Alsnes [25] | 2014 | Case-control | 54 | 383 | a,b,c,e,f,h |
| Esther F Davis [26] | 2015 | Case-control | 252 | 899 | a,b,c,d,e,g,h,i,j |
| M Reveret [27] | 2015 | Case-control | 72 | 83 | a,b |
| Ingvild V. Alsnes [28] | 2017 | Case-control | 27 | 15,072 | a,b,c,e,f,h |
| Beril Gürlek [29] | 2019 | Case-control | 44 | 44 | a,b,j |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, W.; Lin, R.; Yang, L.; Wang, Y.; Mao, B.; Xu, X.; Yu, J. Meta-Analysis of Cardiovascular Risk Factors in Offspring of Preeclampsia Pregnancies. Diagnostics 2023, 13, 812. https://doi.org/10.3390/diagnostics13040812
Wang W, Lin R, Yang L, Wang Y, Mao B, Xu X, Yu J. Meta-Analysis of Cardiovascular Risk Factors in Offspring of Preeclampsia Pregnancies. Diagnostics. 2023; 13(4):812. https://doi.org/10.3390/diagnostics13040812
Chicago/Turabian StyleWang, Weikai, Ru Lin, Lan Yang, Yanxia Wang, Baohong Mao, Xiaoying Xu, and Jing Yu. 2023. "Meta-Analysis of Cardiovascular Risk Factors in Offspring of Preeclampsia Pregnancies" Diagnostics 13, no. 4: 812. https://doi.org/10.3390/diagnostics13040812