
Serial Changes in Blood-Cell-Count-Derived and CRP-Derived Inflammatory Indices of COVID-19 Patients
 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Statistical Analysis
- Aggregate index of systemic inflammation (AISI) = Neutrophil count × monocyte count × platelet count/lymphocyte count
- C-reactive protein to lymphocytes ratio (CLR) = C-reactive protein (CRP)/lymphocyte count
- Lymphocyte to monocyte ratio (LMR) = Lymphocyte count/monocyte count
- Neutrophil to lymphocyte ratio (NLR) = Neutrophil count/lymphocyte count
- Multi-inflammatory index (MII) = NLR × CRP
- Platelet to lymphocyte ratio (PLR) = Platelet count/lymphocyte count
- Systemic inflammatory index (SII) = Neutrophil count × PLR
- Systemic inflammation response index (SIRI) = Neutrophil count × monocyte count/lymphocyte count
3. Results
3.1. Patient Characteristics
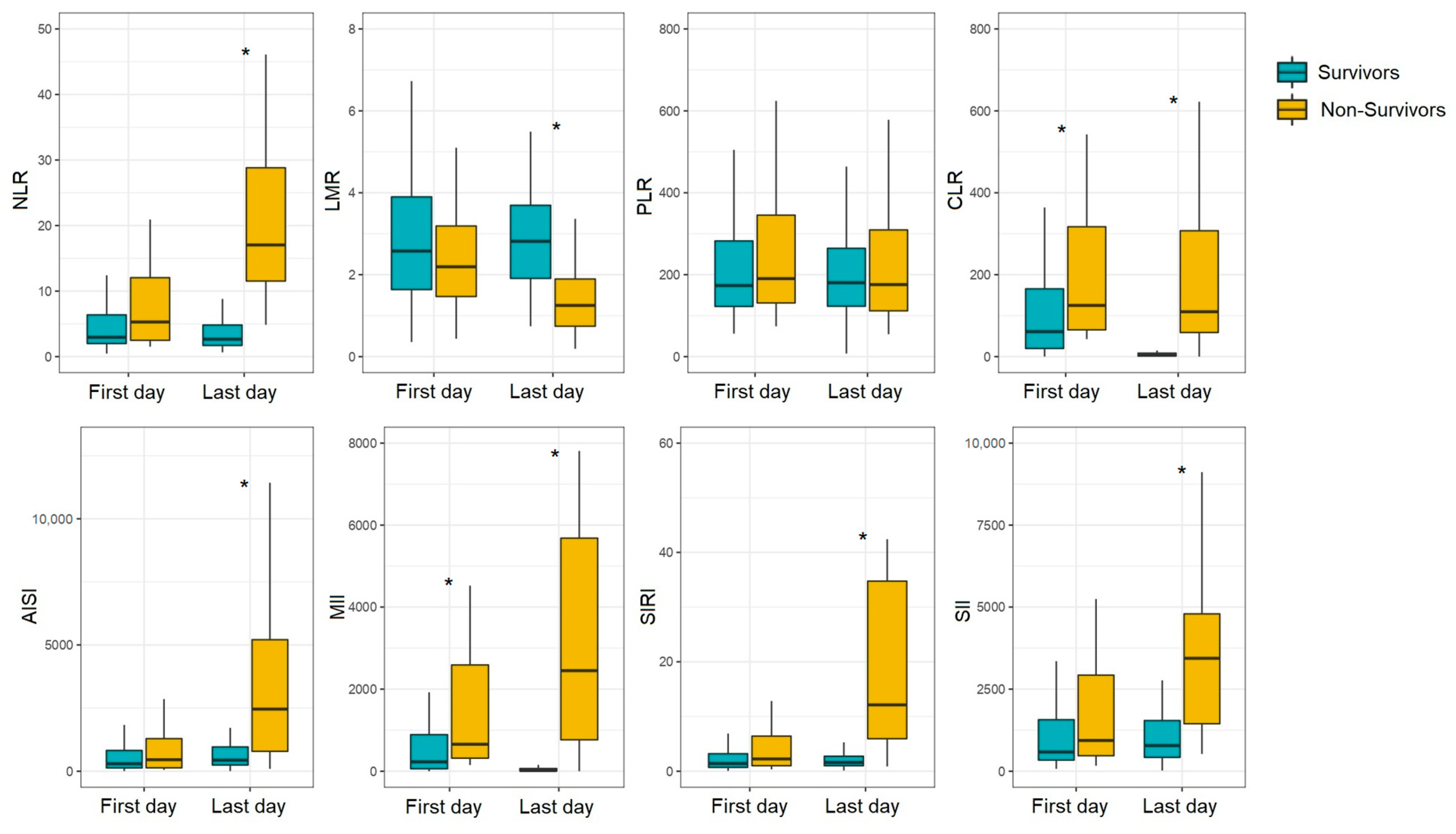
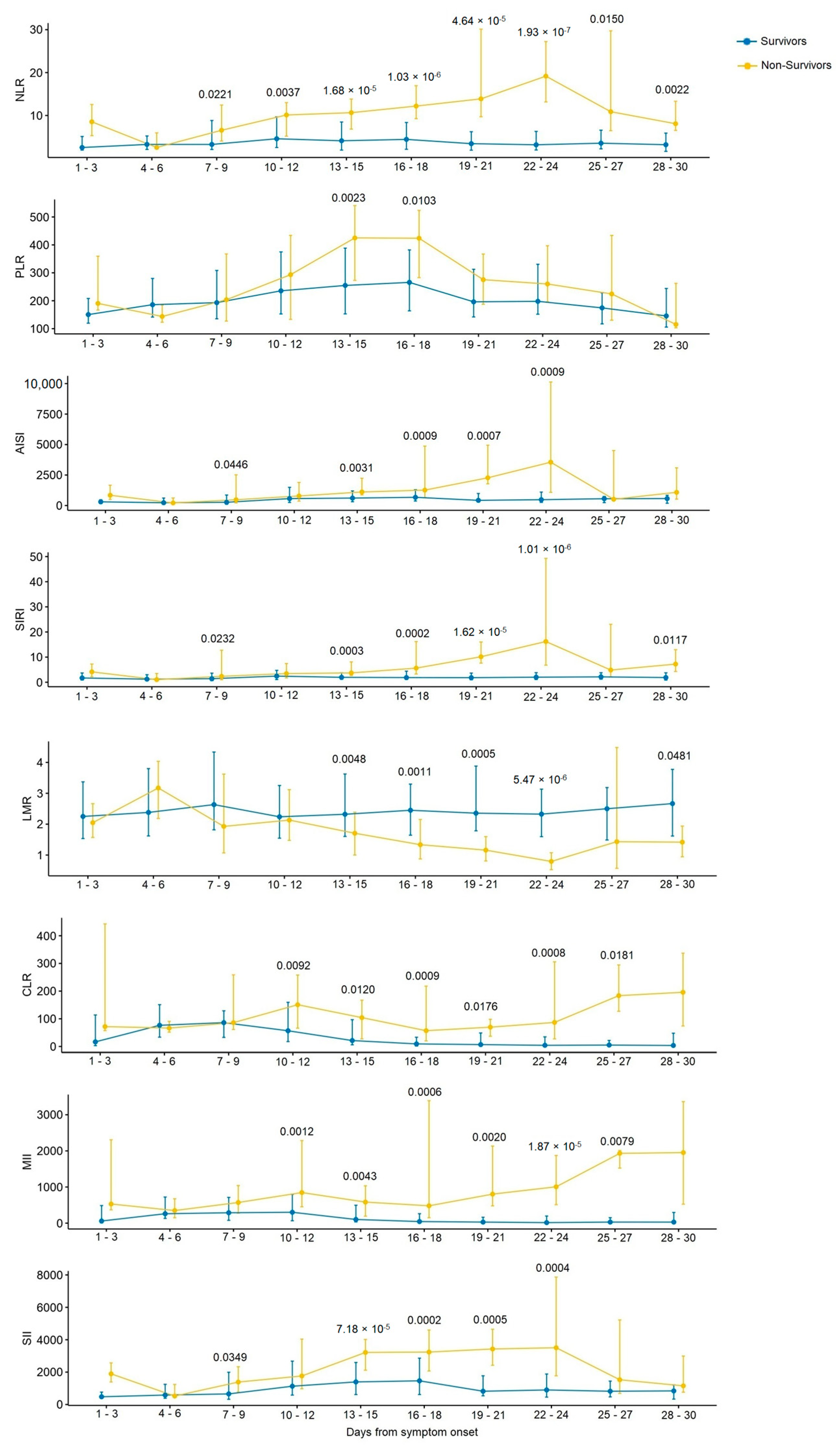
3.2. Serial Changes in Inflammatory Indices in COVID-19 Patients with Different Outcomes
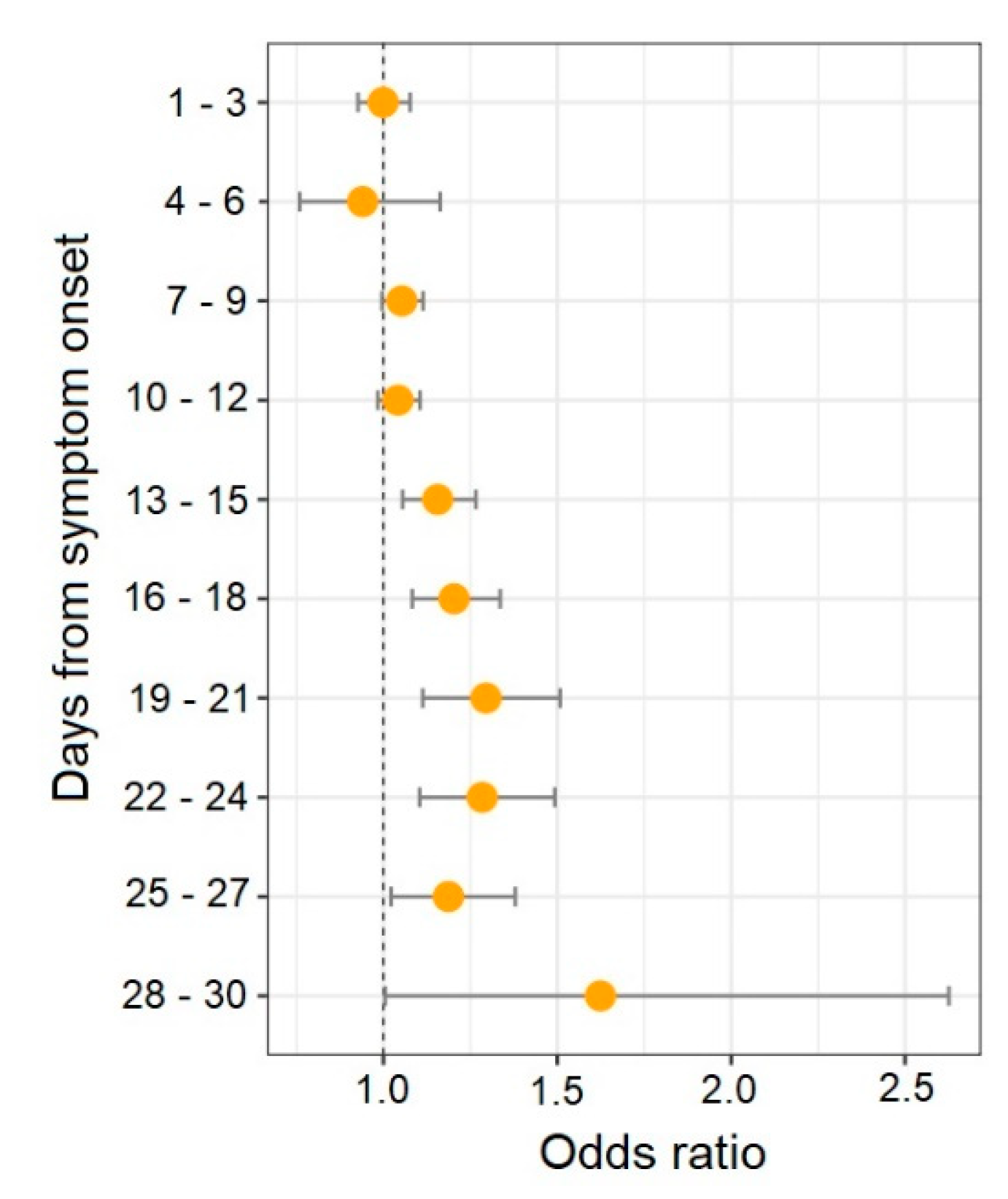
3.3. Inflammatory Indices as Potential Predictors of In-Hospital Mortality in COVID-19 Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Swenson, K.E.; Swenson, E.R. Pathophysiology of Acute Respiratory Distress Syndrome and COVID-19 Lung Injury. Crit. Care Clin. 2021, 37, 749–776. [Google Scholar] [CrossRef] [PubMed]
- Asakura, H.; Ogawa, H. COVID-19-associated coagulopathy and disseminated intravascular coagulation. Int. J. Hematol. 2021, 113, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Zoulikha, M.; Huang, F.; Wu, Z.; He, W. COVID-19 inflammation and implications in drug delivery. J. Control Release 2022, 346, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Salvagno, G.L.; Sanchis-Gomar, F.; Picanza, A.; Lippi, G. Red blood cell distribution width: A simple parameter with multiple clinical applications. Crit. Rev. Clin. Lab. Sci. 2015, 52, 86–105. [Google Scholar] [CrossRef]
- Mare, T.A.; Treacher, D.F.; Shankar-Hari, M.; Beale, R.; Lewis, S.M.; Chambers, D.J.; Brown, K.A. The diagnostic and prognostic significance of monitoring blood levels of immature neutrophils in patients with systemic inflammation. Crit. Care 2015, 19, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Sun, H.; Yin, C.-Q.; Liu, Q.; Wang, F.; Yuan, C.-H. Clinical Significance of Routine Blood Test-Associated Inflammatory Index in Breast Cancer Patients. Med. Sci. Monit. 2017, 23, 5090–5095. [Google Scholar] [CrossRef] [Green Version]
- Mueller, A.A.; Tamura, T.; Crowley, C.P.; DeGrado, J.R.; Haider, H.; Jezmir, J.L.; Keras, G.; Penn, E.H.; Massaro, A.F.; Kim, E.Y. Inflammatory Biomarker Trends Predict Respiratory Decline in COVID-19 Patients. Cell Rep. Med. 2020, 1, 100144. [Google Scholar] [CrossRef]
- Ning, W.; Lei, S.; Yang, J.; Cao, Y.; Jiang, P.; Yang, Q.; Zhang, J.; Wang, X.; Chen, F.; Geng, Z.; et al. Open resource of clinical data from patients with pneumonia for the prediction of COVID-19 outcomes via deep learning. Nat. Biomed. Eng. 2020, 4, 1197–1207. [Google Scholar] [CrossRef]
- Zhang, J.; Cao, Y.; Tan, G.; Dong, X.; Wang, B.; Lin, J.; Yan, Y.; Liu, G.; Akdis, M.; Akdis, C.A.; et al. Clinical, radiological, and laboratory characteristics and risk factors for severity and mortality of 289 hospitalized COVID-19 patients. Allergy 2020, 76, 533–550. [Google Scholar] [CrossRef]
- Henry, B.M.; Benoit, J.; Benoit, S.; Pulvino, C.; Berger, B.A.; De Olivera, M.H.S.; Crutchfield, C.A.; Lippi, G. Red Blood Cell Distribution Width (RDW) Predicts COVID-19 Severity: A Prospective, Observational Study from the Cincinnati SARS-CoV-2 Emergency Department Cohort. Diagnostics 2020, 10, 618. [Google Scholar] [CrossRef]
- Agbuduwe, C.; Basu, S. Haematological manifestations of COVID-19: From cytopenia to coagulopathy. Eur. J. Haematol. 2020, 105, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Ahern, D.J.; Ai, Z.; Ainsworth, M.; Allan, C.; Allcock, A.; Angus, B.; Ansari, M.A.; Arancibia-Cárcamo, C.V.; Aschenbrenner, D.; Attar, M.; et al. A blood atlas of COVID-19 defines hallmarks of disease severity and specificity. Cell 2022, 185, 916–938. [Google Scholar] [CrossRef] [PubMed]
- Kraus, R.F.; Gruber, M.A. Neutrophils—From Bone Marrow to First-Line Defense of the Innate Immune System. Front. Immunol. 2021, 12, 767175. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- Martinod, K.; Deppermann, C. Immunothrombosis and thromboinflammation in host defense and disease. Platelets 2021, 32, 314–324. [Google Scholar] [CrossRef]
- Pepys, M.B.; Hirschfield, G.M. C-reactive protein: A critical update. J. Clin. Invest. 2003, 111, 1805–1812. [Google Scholar] [CrossRef]
- Liu, F.; Li, L.; Xu, M.; Wu, J.; Luo, D.; Zhu, Y.; Li, B.; Song, X.; Zhou, X. Prognostic value of interleukin-6, C-reactive protein, and procalcitonin in patients with COVID-19. J. Clin. Virol. 2020, 127, 104370. [Google Scholar] [CrossRef]
- Stringer, D.; Braude, P.; Myint, P.K.; Evans, L.; Collins, J.T.; Verduri, A.; Quinn, T.J.; Vilches-Moraga, A.; Stechman, M.J.; Pearce, L.; et al. The role of C-reactive protein as a prognostic marker in COVID-19. Int. J. Epidemiol. 2021, 50, 420–429.e58. [Google Scholar] [CrossRef]
- Zinellu, A.; Paliogiannis, P.; Sotgiu, E.; Mellino, S.; Mangoni, A.A.; Zinellu, E.; Negri, S.; Collu, C.; Pintus, G.; Serra, A.; et al. Blood Cell Count Derived Inflammation Indexes in Patients with Idiopathic Pulmonary Fibrosis. Lung 2020, 198, 821–827. [Google Scholar] [CrossRef]
- Nøst, T.H.; Alcala, K.; Urbarova, I.; Byrne, K.S.; Guida, F.; Sandanger, T.M.; Johansson, M. Systemic inflammation markers and cancer incidence in the UK Biobank. Eur. J. Epidemiology 2021, 36, 841–848. [Google Scholar] [CrossRef]
- Fois, A.G.; Paliogiannis, P.; Scano, V.; Cau, S.; Babudieri, S.; Perra, R.; Ruzzittu, G.; Zinellu, E.; Pirina, P.; Carru, C.; et al. The Systemic Inflammation Index on Admission Predicts In-Hospital Mortality in COVID-19 Patients. Molecules 2020, 25, 5725. [Google Scholar] [CrossRef] [PubMed]
- Regolo, M.; Vaccaro, M.; Sorce, A.; Stancanelli, B.; Colaci, M.; Natoli, G.; Russo, M.; Alessandria, I.; Motta, M.; Santangelo, N.; et al. Neutrophil-to-Lymphocyte Ratio (NLR) Is a Promising Predictor of Mortality and Admission to Intensive Care Unit of COVID-19 Patients. J. Clin. Med. 2022, 11, 2235. [Google Scholar] [CrossRef] [PubMed]
- Sokologorskiy, S.V.; Ovechkin, A.M.; Khapov, I.V.; Politov, M.E.; Bulanova, E.L. Risk Factors of Severe Disease and Methods for Clinical Outcome Prediction in Patients with COVID-19 (Review). Gen. Reanimatol. 2022, 18, 31–38. [Google Scholar] [CrossRef]
- Erdolu, B.; As, A.K. C-Reactive Protein and Neutrophil to Lymphocyte Ratio Values in Predicting Inhospital Death in Patients with Stanford Type A Acute Aortic Dissection. Heart Surg. Forum 2020, 23, E488–E492. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.; Long, C.; Huang, X.; Huang, L.; Liao, L.; Tang, W.; Liu, J. Prognostic role and clinical significance of C-reactive protein-lymphocyte ratio in colorectal cancer. Bioengineered 2021, 12, 5138–5148. [Google Scholar] [CrossRef]
- Fan, Z.; Luo, G.; Gong, Y.; Xu, H.; Qian, Y.; Deng, S.; Huang, Q.; Yang, C.; Cheng, H.; Jin, K.; et al. Prognostic Value of the C-Reactive Protein/Lymphocyte Ratio in Pancreatic Cancer. Ann. Surg. Oncol. 2020, 27, 4017–4025. [Google Scholar] [CrossRef]
- Ko, C.; Fang, K.; Hsu, C.; Lee, Y.; Chang, G.; Huang, E.I.; Tsai, M.; Tsai, Y. The preoperative C-reactive protein–lymphocyte ratio and the prognosis of oral cavity squamous cell carcinoma. Head Neck 2021, 43, 2740–2754. [Google Scholar] [CrossRef]
- Koyuncu, S. The Role of C-Reactive Protein to Lymphocyte Ratio in the Differentiation of Acute and Perforated Appendicitis. Turk. J. Trauma Emerg. Surg. 2020, 26, 760–764. [Google Scholar] [CrossRef]
- Çakırca, T.D.; Torun, A.; Çakırca, G.; Portakal, R.D. Role of NLR, PLR, ELR and CLR in differentiating COVID-19 patients with and without pneumonia. Int. J. Clin. Pract. 2021, 75, e14781. [Google Scholar] [CrossRef]
- Ben Jemaa, A.; Salhi, N.; Ben Othmen, M.; Ben Ali, H.; Guissouma, J.; Ghadhoune, H.; Oueslati, R.; Dhaouadi, H. Evaluation of individual and combined NLR, LMR and CLR ratio for prognosis disease severity and outcomes in patients with COVID-19. Int. Immunopharmacol. 2022, 109, 108781. [Google Scholar] [CrossRef]
- Gardini, A.C.; Scarpi, E.; Valgiusti, M.; Monti, M.; Ruscelli, S.; Matteucci, L.; Bartolini, G.; Vertogen, B.; Pagan, F.; Rovesti, G.; et al. Prognostic role of a new index (multi inflammatory index) in patients with metastatic colorectal cancer: Results from the randomized ITACa trial. Ther. Adv. Med. Oncol. 2020, 12, 1758835920958363. [Google Scholar] [CrossRef]
- Gozdas, H.T.; Kayis, S.A.; Damarsoy, T.; Ozsari, E.; Turkoglu, M.; Yildiz, I.; Demirhan, A. Multi-inflammatory Index as a Novel Mortality Predictor in Critically Ill COVID-19 Patients. J. Intensiv. Care Med. 2022, 37, 1480–1485. [Google Scholar] [CrossRef]
- Francone, M.; Iafrate, F.; Masci, G.M.; Coco, S.; Cilia, F.; Manganaro, L.; Panebianco, V.; Andreoli, C.; Colaiacomo, M.C.; Zingaropoli, M.A.; et al. Chest CT score in COVID-19 patients: Correlation with disease severity and short-term prognosis. Eur. Radiol. 2020, 30, 6808–6817. [Google Scholar] [CrossRef] [PubMed]
- Beydoğan, E.; Atasoy, P.Y. The relationship between CRP at admission and thorax CT findings in patients diagnosed with COVID-19. Int. J. Clin. Pract. 2021, 75, e14962. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Meng, G.; Li, W.; Shi, B.; Dong, H.; Su, Z.; Huang, Q.; Gao, P. Relationship of chest CT score with clinical characteristics of 108 patients hospitalized with COVID-19 in Wuhan, China. Respir. Res. 2020, 21, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, B.; Hu, J.; Zuo, X.; Chen, J.; Li, X.; Chen, Y.; Yang, G.; Shi, X.; Deng, A. Predictors of progression from moderate to severe coronavirus disease 2019: A retrospective cohort. Clin. Microbiol. Infect. 2020, 26, 1400–1405. [Google Scholar] [CrossRef]
- Balasubramanian, J.; Suman, F.R.; Stephen, I.R.; Shanmugam, S.G.; Mani, R.; Mathan, B.P.L. Dynamic Profile of Prognostic Hematologic Indicators in Patient Under Intensive Care for COVID-19 Disease: A One-Year Study at a Tertiary Care Centre in South India. Cureus 2021, 13, e19585. [Google Scholar] [CrossRef]
- Ye, W.; Chen, G.; Li, X.; Lan, X.; Ji, C.; Hou, M.; Zhang, D.; Zeng, G.; Wang, Y.; Xu, C.; et al. Dynamic changes of D-dimer and neutrophil-lymphocyte count ratio as prognostic biomarkers in COVID-19. Respir. Res. 2020, 21, 169. [Google Scholar] [CrossRef]
- Citu, C.; Gorun, F.; Motoc, A.; Sas, I.; Gorun, O.M.; Burlea, B.; Tuta-Sas, I.; Tomescu, L.; Neamtu, R.; Malita, D.; et al. The Predictive Role of NLR, d-NLR, MLR, and SIRI in COVID-19 Mortality. Diagnostics 2022, 12, 122. [Google Scholar] [CrossRef]
- Yang, A.-P.; Liu, J.-P.; Tao, W.-Q.; Li, H.-M. The diagnostic and predictive role of NLR, d-NLR and PLR in COVID-19 patients. Int. Immunopharmacol. 2020, 84, 106504. [Google Scholar] [CrossRef]
- Ergenç, H.; Ergenç, Z.; Dog An, M.; Usanmaz, M.; Gozdas, H.T. C-reactive protein and neutrophil–lymphocyte ratio as predictors of mortality in coronavirus disease 2019. Rev. Assoc. Médica Bras. 2021, 67, 1498–1502. [Google Scholar] [CrossRef] [PubMed]
- Simadibrata, D.M.; Calvin, J.; Wijaya, A.D.; Ibrahim, N.A.A. Neutrophil-to-lymphocyte ratio on admission to predict the severity and mortality of COVID-19 patients: A meta-analysis. Am. J. Emerg. Med. 2021, 42, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, S.; Khanna, P.; Singh, A.K. The Impact of Neutrophil-Lymphocyte Count Ratio in COVID-19: A Systematic Review and Meta-Analysis. J. Intensiv. Care Med. 2022, 37, 857–869. [Google Scholar] [CrossRef] [PubMed]
- Ulloque-Badaracco, J.R.; Salas-Tello, W.I.; Al-Kassab-Córdova, A.; Alarcón-Braga, E.A.; Benites-Zapata, V.A.; Maguiña, J.L.; Hernandez, A.V. Prognostic value of neutrophil-to-lymphocyte ratio in COVID-19 patients: A systematic review and meta-analysis. Int. J. Clin. Pract. 2021, 75, e14596. [Google Scholar] [CrossRef]
- Kumar, A.; Sarkar, P.G.; Pant, P.; Kumar, J. Does Neutrophil-to-lymphocyte Ratio at Admission Predict Severity and Mortality in COVID-19 Patients? A Systematic Review and Meta-analysis. Indian J. Crit. Care Med. 2022, 26, 361–375. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Total (n = 169) | Survivors (n = 138) | Non-Survivors (n = 31) | p-Value |
|---|---|---|---|---|
| Age, years | 59.00 (48.00–67.00) | 57.00 (46.00–65.00) | 62.00 (59.00–70.00) | 0.0154 |
| Male | 91/169 (53.85%) | 73/138 (52.52%) | 18/31 (58.06%) | 0.6917 |
| Hypertension | 106/169 (62.72%) | 82/138 (59.42%) | 24/31 (77.42%) | 0.0672 |
| Diabetes mellitus | 40/169 (23.67%) | 30/138 (21.74%) | 10/31 (32.26%) | 0.2439 |
| Coronary heart disease | 42/169 (24.85%) | 31/138 (22.46%) | 11/31 (35.48%) | 0.1666 |
| Obesity | 40/169 (23.67%) | 30/138 (21.74%) | 10/31 (32.26%) | 0.2439 |
| Interval between disease onset and admission, days | 8 (6–11) | 8 (6–11) | 7 (5–9) | 0.3242 |
| Length of stay in hospital/ICU, days | 15 (11–22) | 15 (11–21) | 13 (9–24) | 0.4904 |
| SpO2, % | 94 (89–96) | 94 (91–96) | 90 (87–95) | 0.0278 |
| Missing, n (%) | 7/169 (4.14%) | 6/138 (4.35%) | 1/31 (3.23%) | |
| CT: | 0.0985 | |||
| 0–1 | 54/169 (31.95%) | 45/138 (32.61%) | 9/31 (29.03%) | |
| 2 | 59/169 (34.91%) | 51/138 (36.96%) | 8/31 (25.81%) | |
| 3 | 37/169 (21.89%) | 29/138 (21.01%) | 8/31 (25.81%) | |
| 4 | 19/169 (11.24%) | 13/138 (9.42%) | 6/31 (19.35%) | |
| ARDS | 46/169 (27.22%) | 20/138 (14.49%) | 26/31 (83.87%) | 1.00 × 10−5 |
| WBC (×109/L) | 5.99 (4.12–8.01) | 5.92 (4.00–8.00) | 6.70 (4.60–11.30) | 0.2409 |
| Monocytes (×109/L) | 0.41 (0.28–0.63) | 0.42 (0.29–0.62) | 0.41 (0.22–0.66) | 0.6778 |
| Lymphocytes (×109/L) | 1.11 (0.77–1.46) | 1.15 (0.81–1.49) | 1.03 (0.51–1.36) | 0.1723 |
| Neutrophils (×109/L) | 3.91 (2.45–6.31) | 3.74 (2.36–6.08) | 4.61 (3.17–8.51) | 0.0361 |
| Platelets (×109/L) | 205.00 (168.50–249.00) | 205.00 (172.00–252.00) | 204.00 (156.00–237.00) | 0.3636 |
| CRP (mg/L) | 81.20 (32.92–156.60) | 69.95 (28.71–153.40) | 128.20 (62.10–233.50) | 0.0446 |
| Missing, n (%) | 60/169 (35.50%) | 44/138 (31.88%) | 16/31 (51.61%) |
| Correlation Pairs | Total | Survivors | Non-Survivors | |||
|---|---|---|---|---|---|---|
| ρ | p-Value | ρ | p-Value | ρ | p-Value | |
| CRP and CT score | 0.6287 | 2.49 × 10−13 | 0.6317 | 8.62 × 10−12 | 0.4619 | 0.0831 |
| MII and CT score | 0.6130 | 3.62 × 10−12 | 0.5956 | 5.96 × 10−10 | 0.6622 | 0.0072 |
| CLR and CT score | 0.5927 | 2.71 × 10−11 | 0.5968 | 5.36 × 10−10 | 0.4563 | 0.0873 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khadzhieva, M.B.; Gracheva, A.S.; Belopolskaya, O.B.; Chursinova, Y.V.; Redkin, I.V.; Pisarev, M.V.; Kuzovlev, A.N. Serial Changes in Blood-Cell-Count-Derived and CRP-Derived Inflammatory Indices of COVID-19 Patients. Diagnostics 2023, 13, 746. https://doi.org/10.3390/diagnostics13040746
Khadzhieva MB, Gracheva AS, Belopolskaya OB, Chursinova YV, Redkin IV, Pisarev MV, Kuzovlev AN. Serial Changes in Blood-Cell-Count-Derived and CRP-Derived Inflammatory Indices of COVID-19 Patients. Diagnostics. 2023; 13(4):746. https://doi.org/10.3390/diagnostics13040746
Chicago/Turabian StyleKhadzhieva, Maryam B., Alesya S. Gracheva, Olesya B. Belopolskaya, Yulia V. Chursinova, Ivan V. Redkin, Mikhail V. Pisarev, and Artem N. Kuzovlev. 2023. "Serial Changes in Blood-Cell-Count-Derived and CRP-Derived Inflammatory Indices of COVID-19 Patients" Diagnostics 13, no. 4: 746. https://doi.org/10.3390/diagnostics13040746