
Intracranial Hemorrhage Detection Using Parallel Deep Convolutional Models and Boosting Mechanism

 , ,
, ,  , and
, and 
Abstract
:1. Introduction
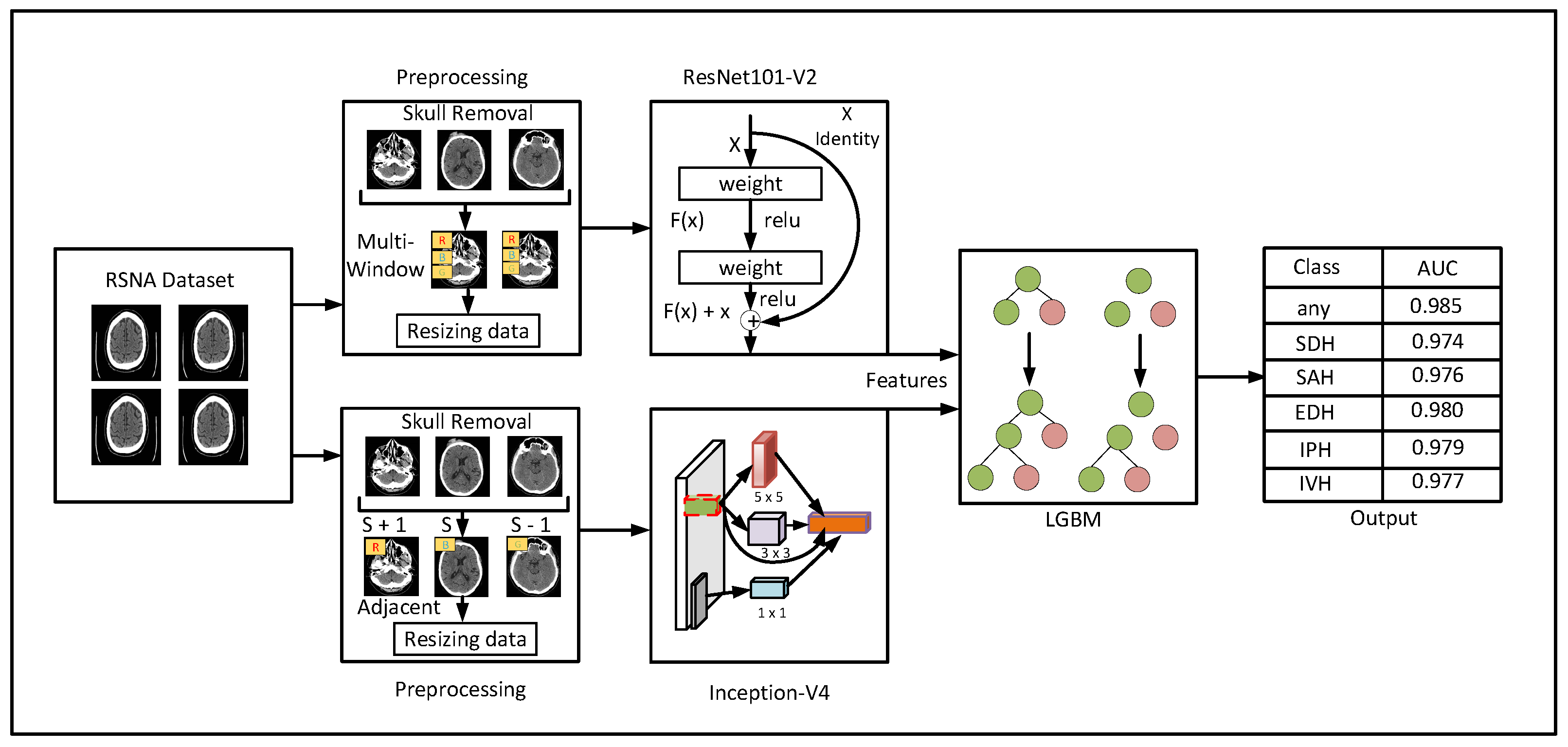
2. Materials and Methods
2.1. Data Preprocessing
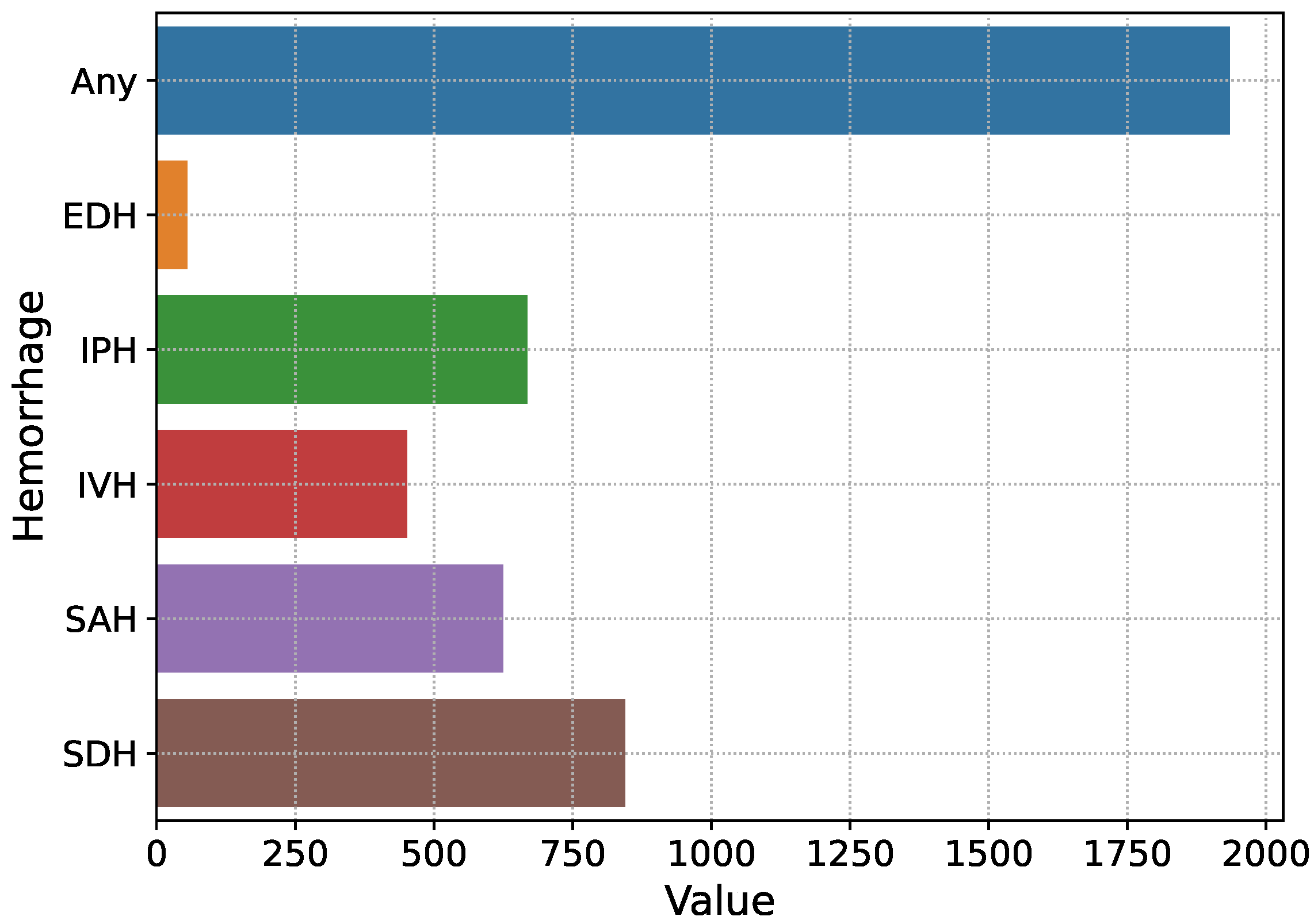
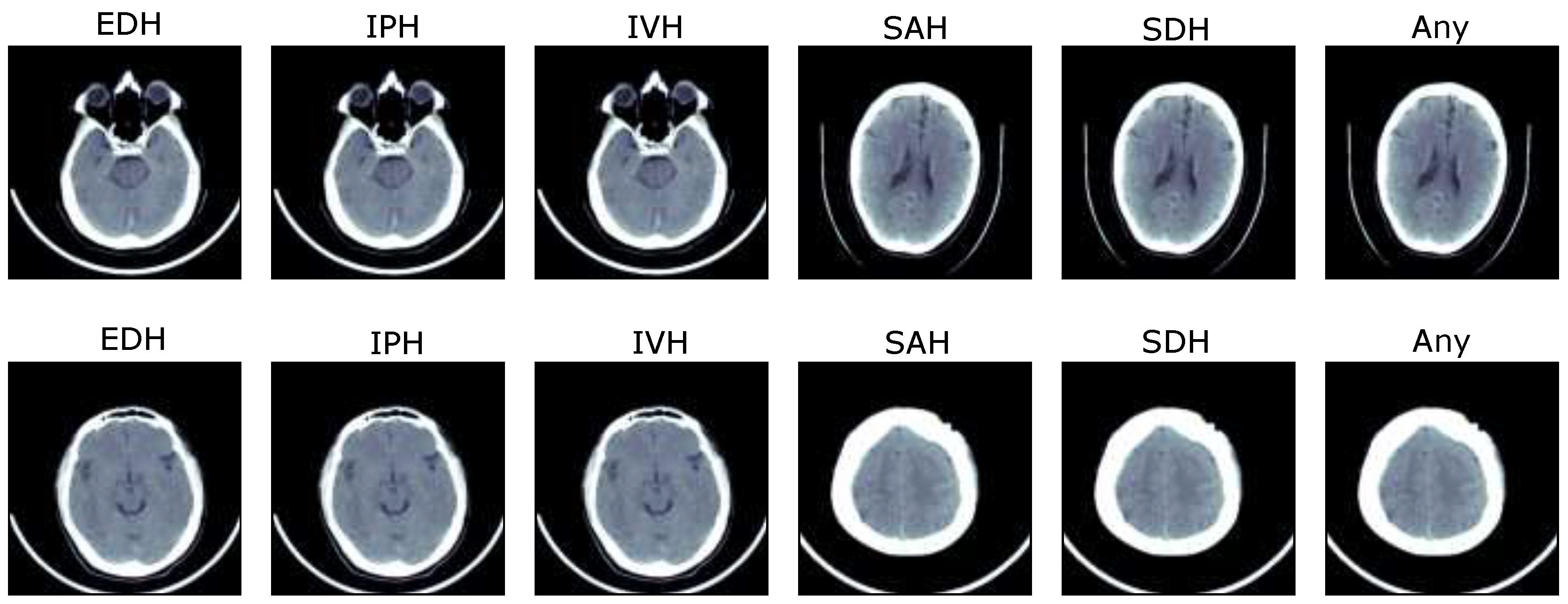
2.1.1. Dataset
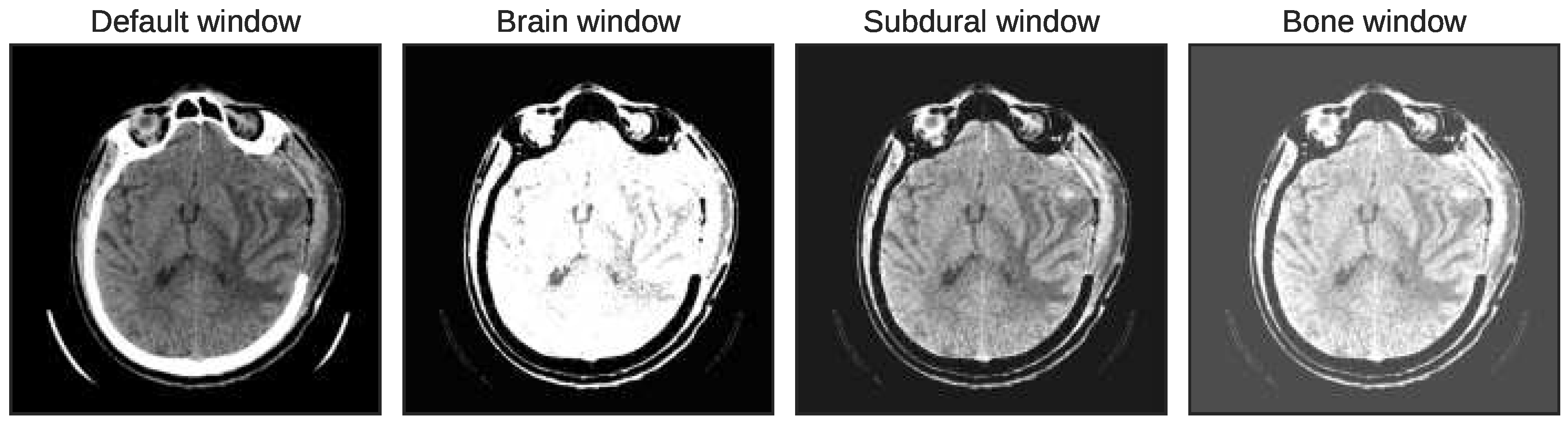
2.1.2. Multiwindowing and Adjacent Slicing
2.2. Feature Extraction Using ResNet101-V2 and Inception-V4
2.3. ICH Detection and Subtype Classification
3. Experimental Results
3.1. Experimental Results of Proposed Solution
3.2. Performance Comparison with Benchmarks
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hssayeni, M.D.; Croock, M.S.; Salman, A.D.; Al-khafaji, H.F.; Yahya, Z.A.; Ghoraani, B. Intracranial hemorrhage segmentation using a deep convolutional model. Data 2020, 5, 14. [Google Scholar] [CrossRef]
- Wang, X.; Shen, T.; Yang, S.; Lan, J.; Xu, Y.; Wang, M.; Zhang, J.; Han, X. A deep learning algorithm for automatic detection and classification of acute intracranial hemorrhages in head CT scans. NeuroImage Clin. 2021, 32, 102785. [Google Scholar] [PubMed]
- Heit, J.J.; Iv, M.; Wintermark, M. Imaging of intracranial hemorrhage. J. Stroke 2017, 19, 11. [Google Scholar] [PubMed]
- Cordonnier, C.; Demchuk, A.; Ziai, W.; Anderson, C.S. Intracerebral haemorrhage: Current approaches to acute management. Lancet 2018, 392, 1257–1268. [Google Scholar] [PubMed]
- Ko, H.; Chung, H.; Lee, H.; Lee, J. Feasible study on intracranial hemorrhage detection and classification using a CNN-LSTM network. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 1290–1293. [Google Scholar]
- Øie, L.R.; Madsbu, M.A.; Solheim, O.; Jakola, A.S.; Giannadakis, C.; Vorhaug, A.; Padayachy, L.; Jensberg, H.; Dodick, D.; Salvesen, Ø.; et al. Functional outcome and survival following spontaneous intracerebral hemorrhage: A retrospective population-based study. Brain Behav. 2018, 8, e01113. [Google Scholar]
- Kuo, W.; Hane, C.; Mukherjee, P.; Malik, J.; Yuh, E.L. Expert-level detection of acute intracranial hemorrhage on head computed tomography using deep learning. Proc. Natl. Acad. Sci. USA 2019, 116, 22737–22745. [Google Scholar] [CrossRef]
- Wu, Y.; Supanich, M.P.; Jie, D. Ensembled deep neural network for intracranial hemorrhage detection and subtype classification on noncontrast CT images. J. Artif. Intell. Med Sci. 2021, 2, 12–20. [Google Scholar]
- Yeo, M.; Tahayori, B.; Kok, H.K.; Maingard, J.; Kutaiba, N.; Russell, J.; Thijs, V.; Jhamb, A.; Chandra, R.V.; Brooks, M.; et al. Review of deep learning algorithms for the automatic detection of intracranial hemorrhages on computed tomography head imaging. J. Neurointerventional Surg. 2021, 13, 369–378. [Google Scholar] [CrossRef]
- Bello, H.R.; Graves, J.A.; Rohatgi, S.; Vakil, M.; McCarty, J.; Van Hemert, R.L.; Geppert, S.; Peterson, R.B. Skull base–related lesions at routine head CT from the emergency department: Pearls, pitfalls, and lessons learned. Radiographics 2019, 39, 1161–1182. [Google Scholar]
- Imran, R.; Hassan, N.; Tariq, R.; Amjad, L.; Wali, A. Intracranial brain Haemorrhage segmentation and classification. iKSP J. Comput. Sci. Eng. 2021, 1, 52–56. [Google Scholar]
- Lee, H.; Yune, S.; Mansouri, M.; Kim, M.; Tajmir, S.H.; Guerrier, C.E.; Ebert, S.A.; Pomerantz, S.R.; Romero, J.M.; Kamalian, S.; et al. An explainable deep-learning algorithm for the detection of acute intracranial haemorrhage from small datasets. Nat. Biomed. Eng. 2019, 3, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Rao, B.; Zohrabian, V.; Cedeno, P.; Saha, A.; Pahade, J.; Davis, M.A. Utility of artificial intelligence tool as a prospective radiology peer reviewer—Detection of unreported intracranial hemorrhage. Acad. Radiol. 2021, 28, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Hostettler, I.C.; Muroi, C.; Richter, J.K.; Schmid, J.; Neidert, M.C.; Seule, M.; Boss, O.; Pangalu, A.; Germans, M.R.; Keller, E. Decision tree analysis in subarachnoid hemorrhage: Prediction of outcome parameters during the course of aneurysmal subarachnoid hemorrhage using decision tree analysis. J. Neurosurg. 2018, 129, 1499–1510. [Google Scholar] [CrossRef] [PubMed]
- Kuang, H.; Qiu, W.; Boers, A.M.; Brown, S.; Muir, K.; Majoie, C.B.; Dippel, D.W.; White, P.; Epstein, J.; Mitchell, P.J.; et al. Computed tomography perfusion–based machine learning model better predicts follow-up infarction in patients with acute ischemic stroke. Stroke 2021, 52, 223–231. [Google Scholar]
- Ramos, L.A.; van der Steen, W.E.; Barros, R.S.; Majoie, C.B.; van den Berg, R.; Verbaan, D.; Vandertop, W.P.; Zijlstra, I.J.A.J.; Zwinderman, A.; Strijkers, G.J.; et al. Machine learning improves prediction of delayed cerebral ischemia in patients with subarachnoid hemorrhage. J. Neurointerventional Surg. 2019, 11, 497–502. [Google Scholar]
- Keshavamurthy, K.N.; Leary, O.P.; Merck, L.H.; Kimia, B.; Collins, S.; Wright, D.W.; Allen, J.W.; Brock, J.F.; Merck, D. Machine learning algorithm for automatic detection of CT-identifiable hyperdense lesions associated with traumatic brain injury. In Proceedings of the Medical Imaging 2017: Computer-Aided Diagnosis SPIE, Orlando, FL, USA, 11–16 February 2017; Volume 10134, pp. 630–638. [Google Scholar]
- Guo, R.; Zhang, R.; Liu, R.; Liu, Y.; Li, H.; Ma, L.; He, M.; You, C.; Tian, R. Machine learning-based approaches for prediction of patients’ functional outcome and mortality after spontaneous intracerebral hemorrhage. J. Pers. Med. 2022, 12, 112. [Google Scholar] [CrossRef]
- Sage, A.; Badura, P. Intracranial hemorrhage detection in head CT using double-branch convolutional neural network, support vector machine, and random forest. Appl. Sci. 2020, 10, 7577. [Google Scholar] [CrossRef]
- Arbabshirani, M.R.; Fornwalt, B.K.; Mongelluzzo, G.J.; Suever, J.D.; Geise, B.D.; Patel, A.A.; Moore, G.J. Advanced machine learning in action: Identification of intracranial hemorrhage on computed tomography scans of the head with clinical workflow integration. NPJ Digit. Med. 2018, 1, 9. [Google Scholar]
- Grewal, M.; Srivastava, M.M.; Kumar, P.; Varadarajan, S. Radnet: Radiologist level accuracy using deep learning for hemorrhage detection in ct scans. In Proceedings of the 2018 IEEE 15th International Symposium on Biomedical Imaging (ISBI 2018), Washington, DC, USA, 4–7 April 2018; pp. 281–284. [Google Scholar]
- Mansour, R.F.; Escorcia-Gutierrez, J.; Gamarra, M.; Díaz, V.G.; Gupta, D.; Kumar, S. Artificial intelligence with big data analytics-based brain intracranial hemorrhage e-diagnosis using CT images. Neural Comput. Appl. 2021, 1–13. [Google Scholar]
- Karki, M.; Cho, J.; Lee, E.; Hahm, M.H.; Yoon, S.Y.; Kim, M.; Ahn, J.Y.; Son, J.; Park, S.H.; Kim, K.H.; et al. CT window trainable neural network for improving intracranial hemorrhage detection by combining multiple settings. Artif. Intell. Med. 2020, 106, 101850. [Google Scholar]
- Anupama, C.; Sivaram, M.; Lydia, E.L.; Gupta, D.; Shankar, K. Synergic deep learning model–based automated detection and classification of brain intracranial hemorrhage images in wearable networks. Pers. Ubiquitous Comput. 2022, 26, 1–10. [Google Scholar] [CrossRef]
- Ye, H.; Gao, F.; Yin, Y.; Guo, D.; Zhao, P.; Lu, Y.; Wang, X.; Bai, J.; Cao, K.; Song, Q.; et al. Precise diagnosis of intracranial hemorrhage and subtypes using a three-dimensional joint convolutional and recurrent neural network. Eur. Radiol. 2019, 29, 6191–6201. [Google Scholar] [CrossRef] [PubMed]
- Burduja, M.; Ionescu, R.T.; Verga, N. Accurate and efficient intracranial hemorrhage detection and subtype classification in 3D CT scans with convolutional and long short-term memory neural networks. Sensors 2020, 20, 5611. [Google Scholar] [PubMed]
- Nguyen, N.T.; Tran, D.Q.; Nguyen, N.T.; Nguyen, H.Q. A CNN-LSTM architecture for detection of intracranial hemorrhage on CT scans. medRxiv 2020, 2020-04. [Google Scholar]
- Chang, P.D.; Kuoy, E.; Grinband, J.; Weinberg, B.D.; Thompson, M.; Homo, R.; Chen, J.; Abcede, H.; Shafie, M.; Sugrue, L.; et al. Hybrid 3D/2D convolutional neural network for hemorrhage evaluation on head CT. Am. J. Neuroradiol. 2018, 39, 1609–1616. [Google Scholar]
- Lee, J.Y.; Kim, J.S.; Kim, T.Y.; Kim, Y.S. Detection and classification of intracranial haemorrhage on CT images using a novel deep-learning algorithm. Sci. Rep. 2020, 10, 20546. [Google Scholar] [PubMed]
- RSNA. Intracranial Hemorrhage Detection Challenge; Technical report; Radiological Society of North America: Oak Brook, IL, USA, 2019. [Google Scholar]
- Flanders, A.E.; Prevedello, L.M.; Shih, G.; Halabi, S.S.; Kalpathy-Cramer, J.; Ball, R.; Mongan, J.T.; Stein, A.; Kitamura, F.C.; Lungren, M.P.; et al. Construction of a machine learning dataset through collaboration: The RSNA 2019 brain CT hemorrhage challenge. Radiol. Artif. Intell. 2020, 2, e190211. [Google Scholar] [CrossRef]
- Chilamkurthy, S.; Ghosh, R.; Tanamala, S.; Biviji, M.; Campeau, N.G.; Venugopal, V.K.; Mahajan, V.; Rao, P.; Warier, P. Deep learning algorithms for detection of critical findings in head CT scans: A retrospective study. Lancet 2018, 392, 2388–2396. [Google Scholar] [CrossRef]
- Das, D.; Kalita, S.K. Skull stripping of brain MRI for analysis of Alzheimer’s disease. Int. J. Biomed. Eng. Technol. 2021, 36, 331–349. [Google Scholar]
- Kumar, K.A.; Boda, R. A multi-objective randomly updated beetle swarm and multi-verse optimization for brain tumor segmentation and classification. Comput. J. 2022, 65, 1029–1052. [Google Scholar]
- Xue, Z.; Antani, S.; Long, L.R.; Demner-Fushman, D.; Thoma, G.R. Window classification of brain CT images in biomedical articles. AMIA Annu. Symp. Proc. 2012, 2012, 1023–1029. [Google Scholar] [PubMed]
- Dinsdale, N.K.; Bluemke, E.; Smith, S.M.; Arya, Z.; Vidaurre, D.; Jenkinson, M.; Namburete, A.I. Learning patterns of the ageing brain in MRI using deep convolutional networks. NeuroImage 2021, 224, 117401. [Google Scholar] [PubMed]
- Rahman, T.; Khandakar, A.; Kadir, M.A.; Islam, K.R.; Islam, K.F.; Mazhar, R.; Hamid, T.; Islam, M.T.; Kashem, S.; Mahbub, Z.B.; et al. Reliable tuberculosis detection using chest X-ray with deep learning, segmentation and visualization. IEEE Access 2020, 8, 191586–191601. [Google Scholar]
- Gunasinghe, H.; McKelvie, J.; Koay, A.; Mayo, M. Comparison of pretrained feature extractors for glaucoma detection. In Proceedings of the 2021 IEEE 18th International Symposium on Biomedical Imaging (ISBI), Nice, France, 13–16 April 2021; pp. 390–394. [Google Scholar]
- Islam, M.; Sanghani, P.; See, A.A.Q.; James, M.L.; King, N.K.K.; Ren, H. ICHNet: Intracerebral hemorrhage (ICH) segmentation using deep learning. In Proceedings of the Brainlesion: Glioma, Multiple Sclerosis, Stroke and Traumatic Brain Injuries: 4th International Workshop, BrainLes 2018, Held in Conjunction with MICCAI 2018, Granada, Spain, 16 September 2018; Revised Selected Papers, Part I. pp. 456–463. [Google Scholar]
- Ni, J.; Zhang, F.; Ma, F.; Yin, Q.; Xiang, D. Random region matting for the high-resolution polsar image semantic segmentation. IEEE J. Sel. Top. Appl. Earth Obs. Remote. Sens. 2021, 14, 3040–3051. [Google Scholar]
- Chollet, F. Keras; GitHub, Inc.: San Francisco, CA, USA, 2015. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Identity mappings in deep residual networks. In Proceedings of the Computer Vision–ECCV 2016: 14th European Conference, Amsterdam, The Netherlands, 11–14 October 2016; pp. 630–645. [Google Scholar]
- Szegedy, C.; Ioffe, S.; Vanhoucke, V.; Alemi, A. Inception-v4, inception-resnet and the impact of residual connections on learning. In Proceedings of the AAAI Conference on Artificial Intelligence, San Francisco, CA, USA, 4–9 February 2017; Volume 31. [Google Scholar]
- Hou, F.; Liu, B.; Zhuo, L.; Zhuo, Z.; Zhang, J. Remote sensing image retrieval with deep features encoding of Inception V4 and largevis dimensionality reduction. Sens. Imaging 2021, 22, 1–14. [Google Scholar] [CrossRef]
- Ke, G.; Meng, Q.; Finley, T.; Wang, T.; Chen, W.; Ma, W.; Ye, Q.; Liu, T.Y. Lightgbm: A highly efficient gradient boosting decision tree. Adv. Neural Inf. Process. Syst. 2017, 30, 52. [Google Scholar]
- Wang, M.; Yue, L.; Yang, X.; Wang, X.; Han, Y.; Yu, B. Fertility-LightGBM: A fertility-related protein prediction model by multi-information fusion and light gradient boosting machine. Biomed. Signal Process. Control. 2021, 68, 102630. [Google Scholar]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hemorrhage | RSNA Instances | CQ500 Scans | |
|---|---|---|---|
| Any | 0 | 11,399 | 205 |
| 1 | 1934 | ||
| IVH | 0 | 12,881 | 28 |
| 1 | 452 | ||
| SAH | 0 | 12,708 | 60 |
| 1 | 625 | ||
| EDH | 0 | 13,279 | 13 |
| 1 | 55 | ||
| SDH | 0 | 12,488 | 53 |
| 1 | 845 | ||
| IPH | 0 | 12,666 | 134 |
| 1 | 668 | ||
| Subtypes | Model | AUC | Sensitivity | Specificity | Precision | F1-Score | AUPR | Accuracy |
|---|---|---|---|---|---|---|---|---|
| any | Res-Inc-LGBM | 0.985 | 0.954 | 0.972 | 0.947 | 0.963 | 0.974 | 0.975 |
| Res-LGBM | 0.938 | 0.764 | 0.926 | 0.825 | 0.843 | 0.892 | 0.926 | |
| Inc-LGBM | 0.952 | 0.803 | 0.926 | 0.863 | 0.875 | 0.952 | 0.936 | |
| SDH | Res-Inc-LGBM | 0.974 | 0.965 | 0.983 | 0.963 | 0.972 | 0.971 | 0.987 |
| Res-LGBM | 0.951 | 0.924 | 0.986 | 0.905 | 0.892 | 0.931 | 0.992 | |
| Inc-LGBM | 0.957 | 0.931 | 0.963 | 0.962 | 0.893 | 0.945 | 0.996 | |
| SAH | Res-Inc-LGBM | 0.976 | 0.962 | 0.973 | 0.964 | 0.963 | 0.972 | 0.985 |
| Res-LGBM | 0.967 | 0.944 | 0.973 | 0.925 | 0.912 | 0.921 | 0.972 | |
| Inc-LGBM | 0.975 | 0.901 | 0.982 | 0.975 | 0.932 | 0.952 | 0.991 | |
| EDH | Res-Inc-LGBM | 0.980 | 0.972 | 0.963 | 0.966 | 0.952 | 0.964 | 0.975 |
| Res-LGBM | 0.927 | 0.804 | 0.896 | 0.883 | 0.832 | 0.844 | 0.936 | |
| Inc-LGBM | 0.935 | 0.822 | 0.885 | 0.895 | 0.875 | 0.902 | 0.945 | |
| IPH | Res-Inc-LGBM | 0.979 | 0.968 | 0.982 | 0.973 | 0.972 | 0.965 | 0.987 |
| Res-LGBM | 0.956 | 0.923 | 0.951 | 0.916 | 0.911 | 0.903 | 0.954 | |
| Inc-LGBM | 0.963 | 0.935 | 0.966 | 0.953 | 0.932 | 0.936 | 0.967 | |
| IVH | Res-Inc-LGBM | 0.977 | 0.962 | 0.973 | 0.972 | 0.963 | 0.968 | 0.985 |
| Res-LGBM | 0.953 | 0.934 | 0.962 | 0.943 | 0.932 | 0.922 | 0.963 | |
| Inc-LGBM | 0.967 | 0.954 | 0.973 | 0.967 | 0.959 | 0.952 | 0.974 |
| ICH | Recall | Specificity | F1-Score | Accuracy |
|---|---|---|---|---|
| any | 0.952 | 0.962 | 0.951 | 0.971 |
| SDH | 0.951 | 0.953 | 0.950 | 0.962 |
| SAH | 0.943 | 0.951 | 0.946 | 0.960 |
| EDH | 0.954 | 0.942 | 0.941 | 0.951 |
| IPH | 0.941 | 0.935 | 0.942 | 0.963 |
| IVH | 0.934 | 0.952 | 0.937 | 0.961 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asif, M.; Shah, M.A.; Khattak, H.A.; Mussadiq, S.; Ahmed, E.; Nasr, E.A.; Rauf, H.T. Intracranial Hemorrhage Detection Using Parallel Deep Convolutional Models and Boosting Mechanism. Diagnostics 2023, 13, 652. https://doi.org/10.3390/diagnostics13040652
Asif M, Shah MA, Khattak HA, Mussadiq S, Ahmed E, Nasr EA, Rauf HT. Intracranial Hemorrhage Detection Using Parallel Deep Convolutional Models and Boosting Mechanism. Diagnostics. 2023; 13(4):652. https://doi.org/10.3390/diagnostics13040652
Chicago/Turabian StyleAsif, Muhammad, Munam Ali Shah, Hasan Ali Khattak, Shafaq Mussadiq, Ejaz Ahmed, Emad Abouel Nasr, and Hafiz Tayyab Rauf. 2023. "Intracranial Hemorrhage Detection Using Parallel Deep Convolutional Models and Boosting Mechanism" Diagnostics 13, no. 4: 652. https://doi.org/10.3390/diagnostics13040652