
Clinical and Technical Validation of Novel Bite Force Measuring Device for Functional Analysis after Mandibular Reconstruction

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
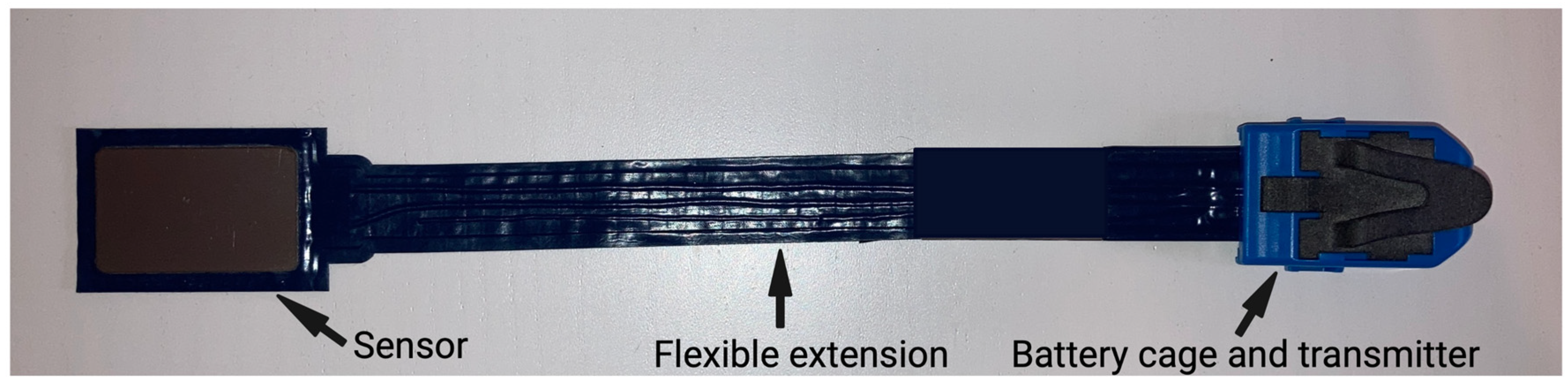
2.1. Bite Force Measuring Sensor
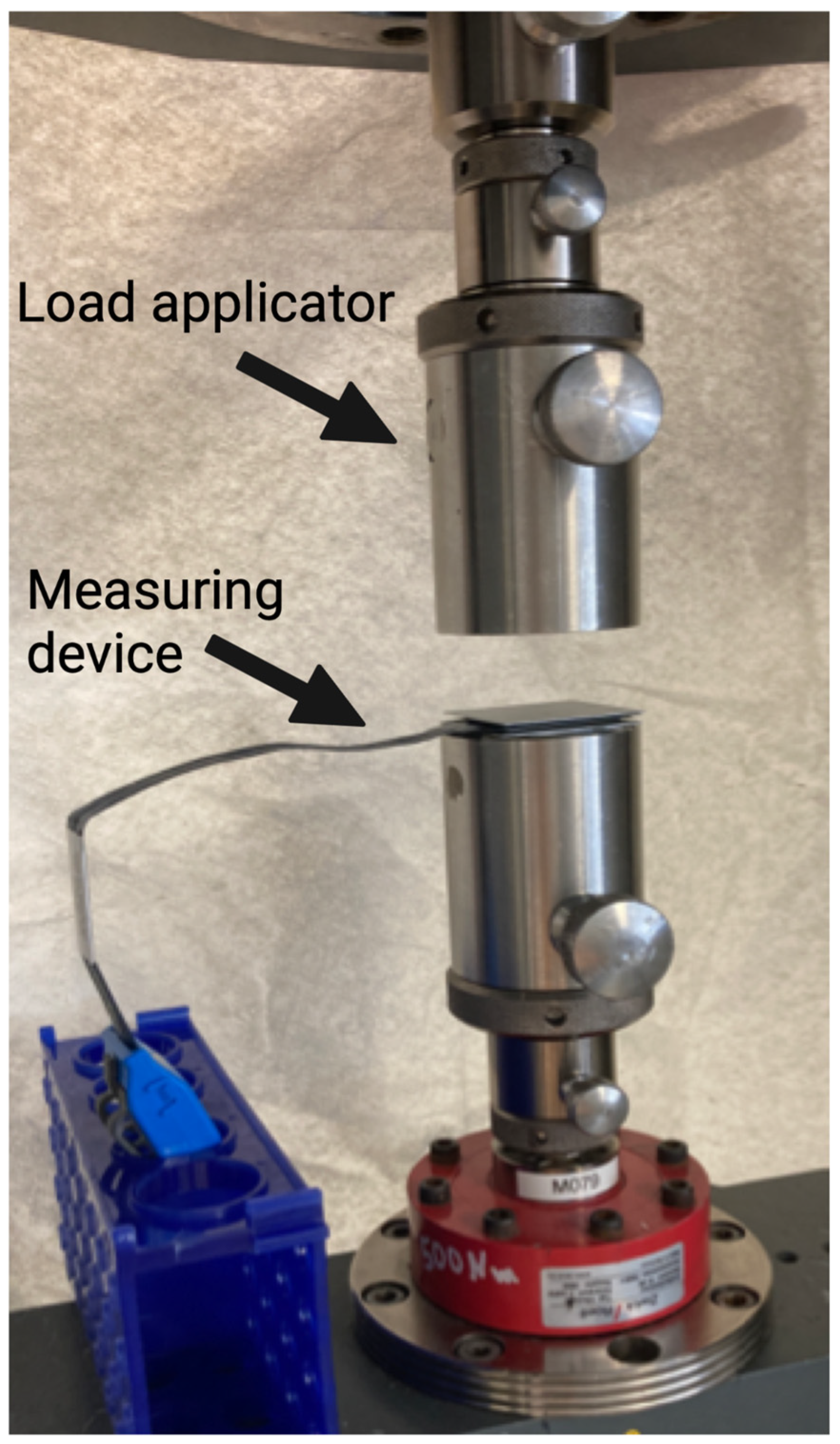
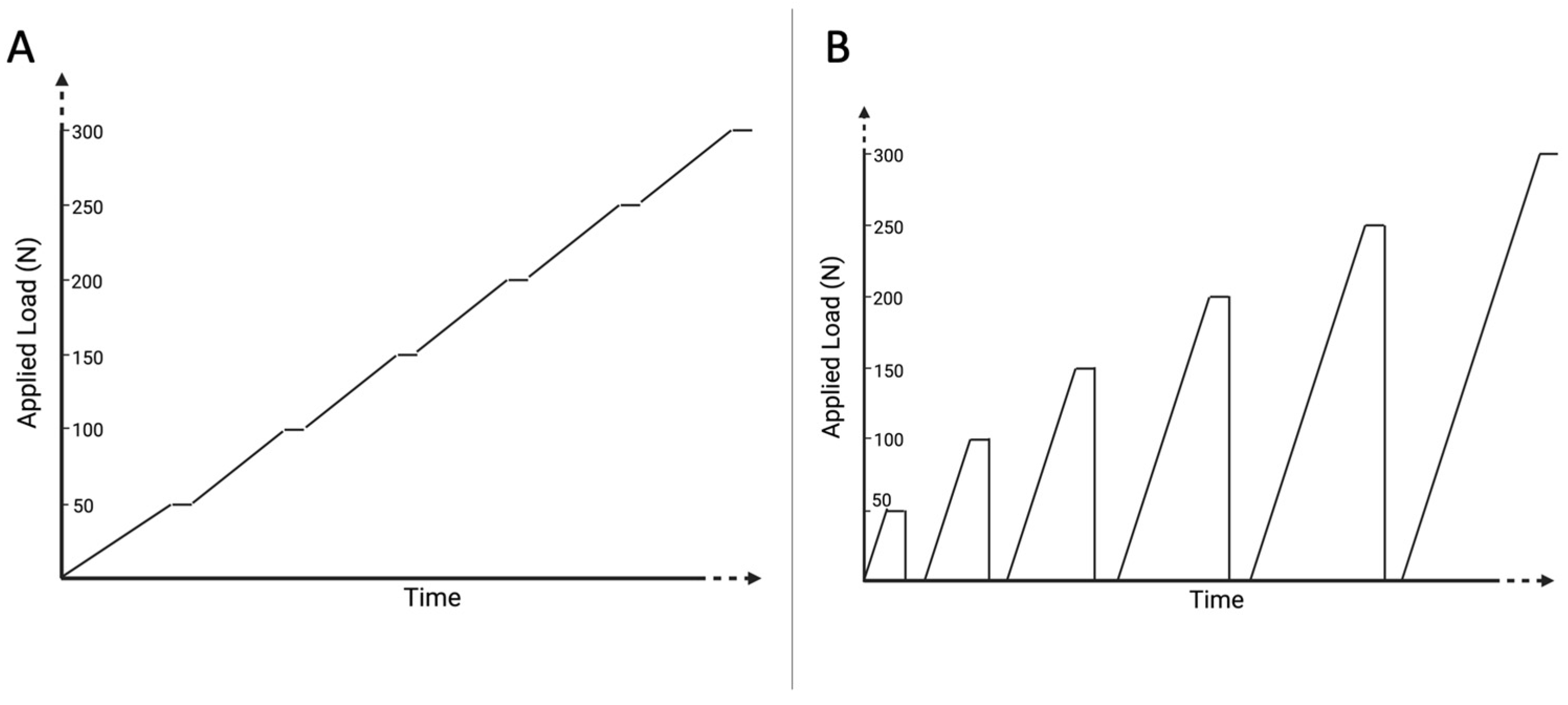
2.2. Validation Measurements
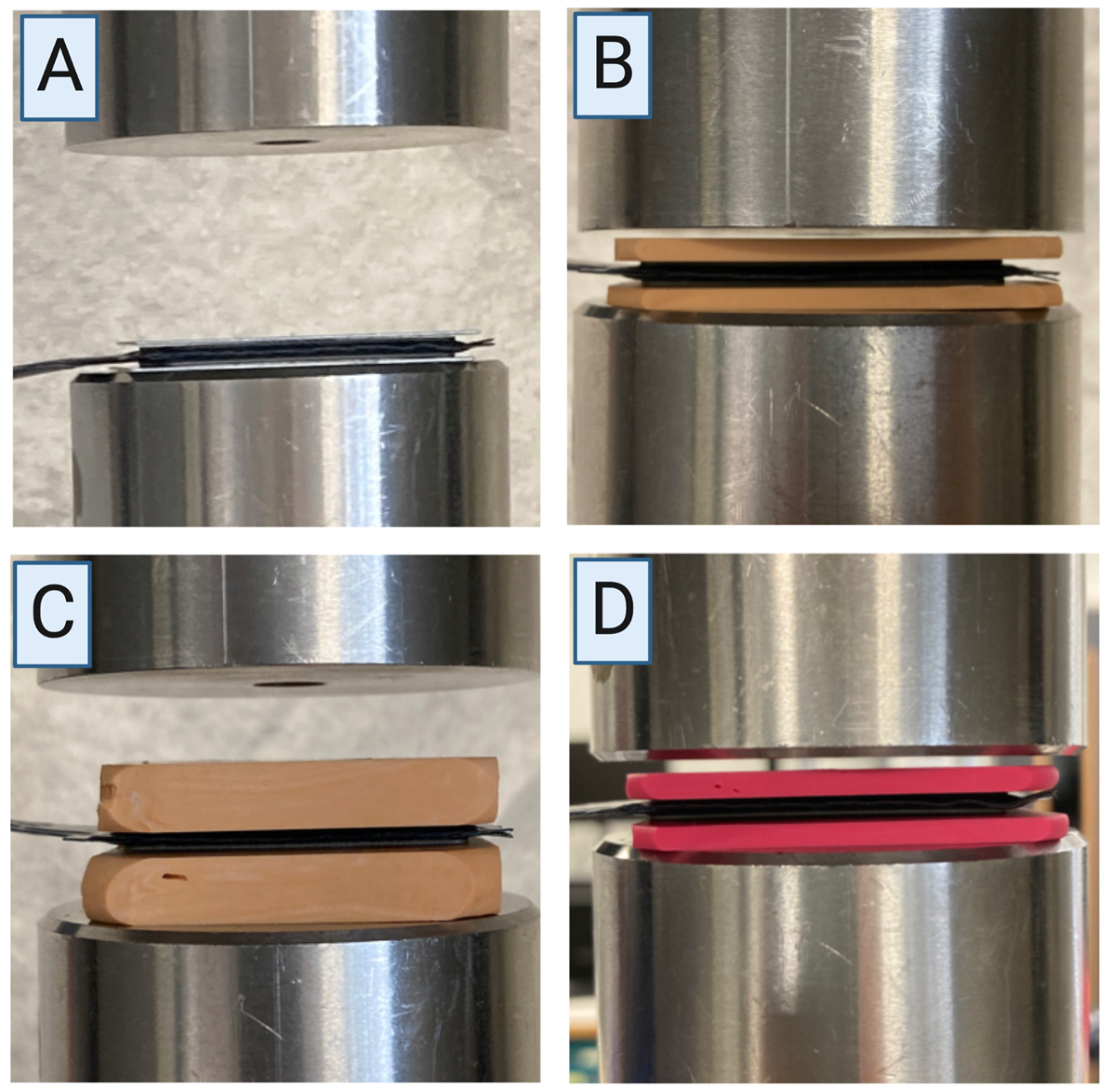
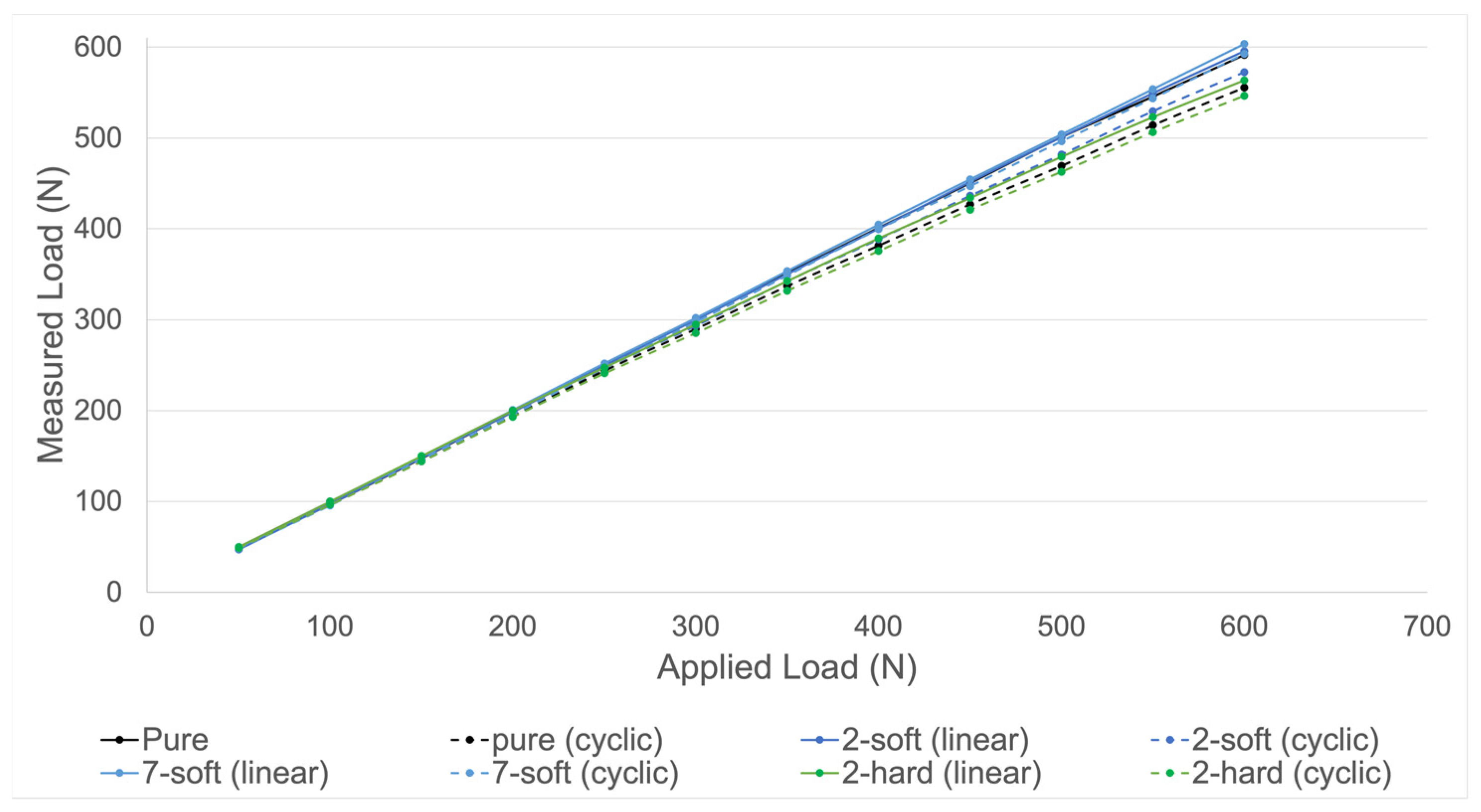
- “Pure”: no silicone layer (Figure 4A);
- “2-soft”: 2.0 mm silicone layer (S1, A-silicone, bisico, Bielefeld, Germany) on both sides of the device with a final hardness of approximately 72 Shore A (Figure 4B);
- “7-soft”: 7.0 mm silicone layer (S1, A-silicone, bisico, Bielefeld, Germany) on both sides of the device with a final hardness of approximately 72 Shore A (Figure 4C);
- “2-hard”: 2.0 mm silicone layer (Regidur® i, A-silicone, bisico, Bielefeld, Germany) on both sides of the device with a final hardness of approximately 90 Shore A (Figure 4D).
2.3. Study Design
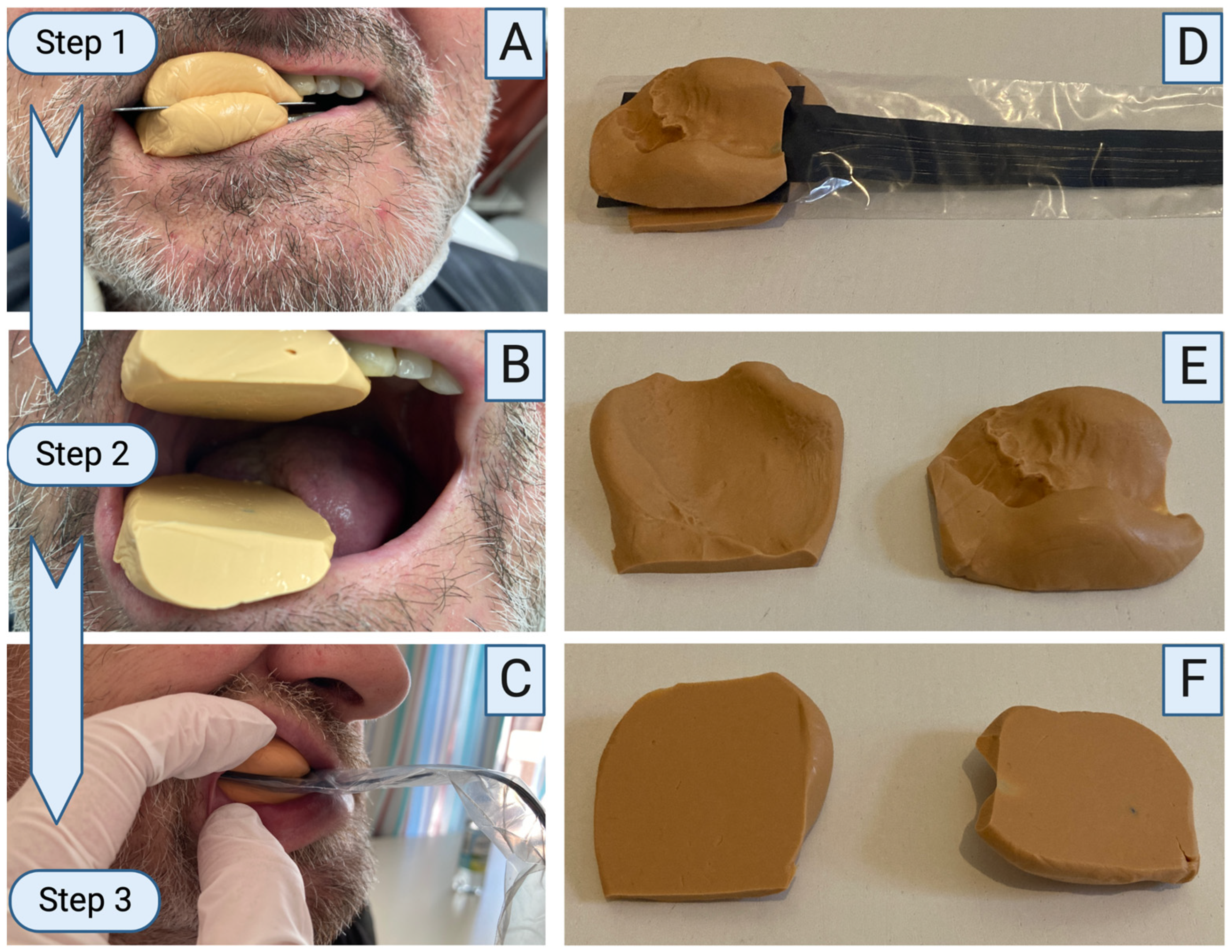
2.4. Clinical Methodology
2.5. Statistical Analysis
3. Results
3.1. Validation Measurements
3.2. Clinical Application
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Okoturo, E.; Ogunbanjo, O.; Akinleye, A.; Bardi, M. Quality of life of patients with segmental mandibular resection and immediate reconstruction with plates. J. Oral. Maxillofac. Surg. 2011, 69, 2253–2259. [Google Scholar] [CrossRef]
- Schierz, O.; Baba, K.; Fueki, K. Functional oral health-related quality of life impact: A systematic review in populations with tooth loss. J. Oral. Rehabil. 2021, 48, 256–270. [Google Scholar] [CrossRef] [PubMed]
- Mehari Abraha, H.; Iriarte-Diaz, J.; Reid, R.R.; Ross, C.F.; Panagiotopoulou, O. Fracture Fixation Technique and Chewing Side Impact Jaw Mechanics in Mandible Fracture Repair. JBMR Plus 2022, 6, e10559. [Google Scholar] [CrossRef]
- Claes, L.E.; Heigele, C.A. Magnitudes of local stress and strain along bony surfaces predict the course and type of fracture healing. J. Biomech. 1999, 32, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Claes, L.E.; Heigele, C.A.; Neidlinger-Wilke, C.; Kaspar, D.; Seidl, W.; Margevicius, K.J.; Augat, P. Effects of mechanical factors on the fracture healing process. Clin. Orthop. Relat. Res. 1998, 355, S132–S147. [Google Scholar] [CrossRef] [PubMed]
- Rendenbach, C.; Steffen, C.; Hanken, H.; Schluermann, K.; Henningsen, A.; Beck-Broichsitter, B.; Kreutzer, K.; Heiland, M.; Precht, C. Complication rates and clinical outcomes of osseous free flaps: A retrospective comparison of CAD/CAM versus conventional fixation in 128 patients. Int. J. Oral. Maxillofac. Surg. 2019, 48, 1156–1162. [Google Scholar] [CrossRef]
- Knitschke, M.; Sonnabend, S.; Roller, F.C.; Pons-Kühnemann, J.; Schmermund, D.; Attia, S.; Streckbein, P.; Howaldt, H.P.; Böttger, S. Osseous Union after Mandible Reconstruction with Fibula Free Flap Using Manually Bent Plates vs. Patient-Specific Implants: A Retrospective Analysis of 89 Patients. Curr. Oncol. 2022, 29, 3375–3392. [Google Scholar] [CrossRef]
- Arakawa, I.; Abou-Ayash, S.; Genton, L.; Tsuga, K.; Leles, C.R.; Schimmel, M. Reliability and comparability of methods for assessing oral function: Chewing, tongue pressure and lip force. J. Oral. Rehabil. 2020, 47, 862–871. [Google Scholar] [CrossRef]
- Sakuraba, M.; Miyamoto, S.; Fujiki, M.; Higashino, T.; Oshima, A.; Hayashi, R. Analysis of functional outcomes in patients with mandible reconstruction using vascularized fibular grafts. Microsurgery 2017, 37, 101–104. [Google Scholar] [CrossRef]
- Mochizuki, Y.; Omura, K.; Harada, H.; Marukawa, E.; Shimamoto, H.; Tomioka, H. Functional outcomes and patient satisfaction after vascularized osteocutaneous scapula flap reconstruction of the mandible in patients with benign or cancerous tumours. Int. J. Oral. Maxillofac. Surg. 2014, 43, 1330–1338. [Google Scholar] [CrossRef]
- Kosaka, T.; Ono, T.; Kida, M.; Kikui, M.; Yamamoto, M.; Yasui, S.; Nokubi, T.; Maeda, Y.; Kokubo, Y.; Watanabe, M.; et al. A multifactorial model of masticatory performance: The Suita study. J. Oral. Rehabil. 2016, 43, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Bai, Y.; Xie, X. Bite Force Transducers and Measurement Devices. Front. Bioeng. Biotechnol. 2021, 9, 665081. [Google Scholar] [CrossRef] [PubMed]
- Soni, R.; Yadav, H.; Pathak, A.; Bhatnagar, A.; Kumar, V. Comparative evaluation of biting force and chewing efficiency of all-on-four treatment concept with other treatment modalities in completely edentulous individuals. J. Indian Prosthodont. Soc. 2020, 20, 312–320. [Google Scholar] [CrossRef]
- Shiga, H.; Komino, M.; Uesugi, H.; Sano, M.; Yokoyama, M.; Nakajima, K.; Ishikawa, A. Comparison of two dental prescale systems used for the measurement of occlusal force. Odontology 2020, 108, 676–680. [Google Scholar] [CrossRef] [PubMed]
- Fastier-Wooller, J.; Phan, H.P.; Dinh, T.; Nguyen, T.K.; Cameron, A.; Öchsner, A.; Dao, D.V. Novel Low-Cost Sensor for Human Bite Force Measurement. Sensors 2016, 16, 1244. [Google Scholar] [CrossRef]
- Lantada, A.D.; Bris, C.G.; Morgado, P.L.; Maudes, J.S. Novel system for bite-force sensing and monitoring based on magnetic near field communication. Sensors 2012, 12, 11544–11558. [Google Scholar] [CrossRef]
- Takahashi, M.; Yamaguchi, S.; Fujii, T.; Watanabe, M.; Hattori, Y. Contribution of each masticatory muscle to the bite force determined by MRI using a novel metal-free bite force gauge and an index of total muscle activity. J. Magn. Reson. Imaging 2016, 44, 804–813. [Google Scholar] [CrossRef]
- Umesh, S.; Padma, S.; Asokan, S.; Srinivas, T. Fiber Bragg Grating based bite force measurement. J. Biomech. 2016, 49, 2877–2881. [Google Scholar] [CrossRef]
- Linsen, S.; Schmidt-Beer, U.; Fimmers, R.; Grüner, M.; Koeck, B. Craniomandibular pain, bite force, and oral health-related quality of life in patients with jaw resection. J. Pain Symptom. Manag. 2009, 37, 94–106. [Google Scholar] [CrossRef] [PubMed]
- Maurer, P.; Pistner, H.; Schubert, J. Computer assisted chewing power in patients with segmental resection of the mandible. Mund Kiefer Gesichtschir 2006, 10, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Marunick, M.T.; Mathes, B.E.; Klein, B.B. Masticatory function in hemimandibulectomy patients. J. Oral. Rehabil. 1992, 19, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Curtis, D.A.; Plesh, O.; Miller, A.J.; Curtis, T.A.; Sharma, A.; Schweitzer, R.; Hilsinger, R.L.; Schour, L.; Singer, M. A comparison of masticatory function in patients with or without reconstruction of the mandible. Head Neck 1997, 19, 287–296. [Google Scholar] [CrossRef]
- Iwasaki, M.; Maeda, I.; Kokubo, Y.; Tanaka, Y.; Ueno, T.; Takahashi, W.; Watanabe, Y.; Hirano, H. Capacitive-Type Pressure-Mapping Sensor for Measuring Bite Force. Int. J. Environ. Res. Public Health 2022, 19, 31273. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, M.; Maeda, I.; Kokubo, Y.; Tanaka, Y.; Ueno, T.; Ohara, Y.; Motokawa, K.; Hayakawa, M.; Shirobe, M.; Edahiro, A.; et al. Standard Values and Concurrent Validity of a Newly Developed Occlusal Force-Measuring Device among Community-Dwelling Older Adults: The Otassha Study. Int. J. Environ. Res. Public Health 2022, 19, 95588. [Google Scholar] [CrossRef] [PubMed]
- Linsen, S.S.; Oikonomou, A.; Martini, M.; Teschke, M. Mandibular kinematics and maximum voluntary bite force following segmental resection of the mandible without or with reconstruction. Clin. Oral. Investig. 2018, 22, 1707–1716. [Google Scholar] [CrossRef]
- Santilli, M.; D’Addazio, G.; Rexhepi, I.; Sinjari, B.; Filippini, A. Multiple Free Flap Reconstruction of a Complex Intraoral Defect after Squamous Cell Carcinoma Excision: A Case Report. Medicina 2021, 58, 54. [Google Scholar] [CrossRef]
- Steffen, C.; Fischer, H.; Sauerbrey, M.; Heintzelmann, T.; Voss, J.O.; Koerdt, S.; Checa, S.; Kreutzer, K.; Heiland, M.; Rendenbach, C. Increased rate of pseudarthrosis in the anterior intersegmental gap after mandibular reconstruction with fibula free flaps: A volumetric analysis. Dentomaxillofac. Radiol. 2022, 51, 20220131. [Google Scholar] [CrossRef]
- Heberer, S.; Nelson, K. Clinical evaluation of a modified method of vestibuloplasty using an implant-retained splint. J. Oral. Maxillofac. Surg. 2009, 67, 624–629. [Google Scholar] [CrossRef]
- Kreutzer, K.; Steffen, C.; Nahles, S.; Koerdt, S.; Heiland, M.; Rendenbach, C.; Beck-Broichsitter, B. Removal of patient-specific reconstruction plates after mandible reconstruction with a fibula free flap: Is the plate the problem? Int. J. Oral. Maxillofac. Surg. 2022, 51, 182–190. [Google Scholar] [CrossRef]
- Klein, P.; Schell, H.; Streitparth, F.; Heller, M.; Kassi, J.P.; Kandziora, F.; Bragulla, H.; Haas, N.P.; Duda, G.N. The initial phase of fracture healing is specifically sensitive to mechanical conditions. J. Orthop. Res. 2003, 21, 662–669. [Google Scholar] [CrossRef]
- Steffen, C.; Sellenschloh, K.; Vollmer, M.; Morlock, M.M.; Heiland, M.; Huber, G.; Rendenbach, C. Biomechanical comparison of titanium miniplates versus a variety of CAD/CAM plates in mandibular reconstruction. J. Mech. Behav. Biomed. Mater. 2020, 111, 104007. [Google Scholar] [CrossRef] [PubMed]
- Bakke, M. Bite Force and Occlusion. Semin. Orthod. 2006, 12, 120–126. [Google Scholar] [CrossRef]
- Koizumi, K.; Shintani, T.; Yoshimi, Y.; Higaki, M.; Kunimatsu, R.; Yoshioka, Y.; Tsuga, K.; Tanimoto, K.; Shiba, H.; Toratani, S. Impact of Maximum Tongue Pressure in Patients with Jaw Deformities Who Underwent Orthognathic Surgery. Diagnostics 2022, 12, 404. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Set Load (N) | Pure (Linear) | Pure (Cyclic) | 2-Soft (Linear) | 2-Soft (Cyclic) | 7-Soft (Linear) | 7-Soft (Cyclic) | 2-Hard (Linear) | 2-Hard (Cyclic) | 2-Soft (Old) (Cyclic) |
|---|---|---|---|---|---|---|---|---|---|
| Measured load by force device (absolute values (N)) | |||||||||
| 50 | 47.5 | 49.0 | 47.0 | 49.0 | 49.0 | 48.0 | 50.0 | 49.0 | 47.0 |
| 100 | 97.0 | 97.0 | 97.0 | 97.5 | 100 | 95.5 | 100 | 96.5 | 94.0 |
| 150 | 147.5 | 145.0 | 148.0 | 146.0 | 149.5 | 146.5 | 150 | 144.0 | 144.0 |
| 200 | 198.5 | 194.5 | 198.5 | 196.5 | 200.5 | 195.5 | 200 | 193.0 | 194.5 |
| 250 | 249.5 | 244.0 | 249.0 | 247.0 | 252.0 | 247.5 | 247.5 | 241.0 | 243.5 |
| 300 | 300.5 | 290.0 | 300.0 | 293.5 | 302.0 | 297.5 | 295.0 | 285.5 | 294.5 |
| 350 | 351.0 | 337.0 | 350.0 | 342.5 | 353.5 | 348.5 | 342.5 | 332.0 | 343.0 |
| 400 | 401.0 | 381.5 | 400.0 | 388.5 | 404.5 | 399.5 | 389.5 | 375.5 | 393.0 |
| 450 | 450.5 | 427.0 | 451.5 | 436.5 | 454.5 | 447.0 | 434.0 | 421.0 | 441.5 |
| 500 | 501.0 | 469.5 | 501.0 | 482.0 | 504.0 | 496.5 | 479.5 | 463.0 | 486.5 |
| 550 | 545.5 | 514.0 | 549.0 | 529.5 | 553.5 | 543.5 | 523.0 | 506.5 | 533.0 |
| 600 | 591.5 | 555.5 | 595.5 | 572.5 | 603.5 | 592.5 | 563.5 | 546.5 | 575.5 |
| Relative deviations from set load (%) | |||||||||
| 50 | 5.00 | 2.00 | 6.00 | 2.00 | 2.00 | 4.00 | 0.00 | 2.00 | 6.00 |
| 100 | 3.00 | 3.00 | 3.00 | 2.50 | 0.00 | 4.50 | 0.00 | 3.50 | 6.00 |
| 150 | 1.67 | 3.33 | 1.33 | 2.67 | 0.33 | 2.33 | 0.00 | 4.00 | 4.00 |
| 200 | 0.75 | 2.75 | 0.75 | 1.75 | 0.25 | 2.25 | 0.00 | 3.50 | 2.75 |
| 250 | 0.20 | 2.40 | 0.40 | 1.20 | 0.80 | 1.00 | 1.00 | 3.60 | 2.60 |
| 300 | 0.17 | 3.33 | 0.00 | 2.17 | 0.67 | 0.83 | 1.67 | 4.83 | 1.83 |
| 350 | 0.29 | 3.71 | 0.00 | 2.14 | 1.00 | 0.43 | 2.14 | 5.14 | 2.00 |
| 400 | 0.25 | 4.63 | 0.00 | 2.88 | 1.13 | 0.12 | 2.63 | 6.13 | 1.75 |
| 450 | 0.11 | 5.11 | 0.33 | 3.00 | 1.00 | 0.67 | 3.56 | 6.44 | 1.89 |
| 500 | 0.20 | 6.10 | 0.20 | 3.60 | 0.80 | 0.70 | 4.10 | 7.40 | 2.70 |
| 550 | 0.82 | 6.55 | 0.18 | 3.73 | 0.64 | 1.18 | 4.91 | 7.91 | 3.09 |
| 600 | 1.42 | 7.42 | 0.75 | 4.58 | 0.58 | 1.25 | 6.08 | 8.92 | 4.08 |
| Mean 600 | 1.16 | 4.19 | 1.08 | 2.68 | 0.77 | 1.61 | 2.17 | 5.28 | 3.22 |
| Patient | Edentulous? | Bite Force (N) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Preoperative | Postoperative | Difference Postop.max − Preop.max | ||||||||
| 1 | 2 | 3 | Maximum | 1 | 2 | 3 | Maximum | |||
| 1 | No | 39.5 | 45.0 | 43.5 | 45.0 | 44.5 | 37.0 | 40.0 | 44.5 | −0.5 |
| 2 | No | 380.0 | 387.5 | 411.0 | 411.0 | 271.5 | 281.0 | 282.5 | 282.5 | −128.5 |
| 3 | No | 292.0 | 335.5 | 315.0 | 335.5 | 162.5 | 164.5 | 180.0 | 180.0 | −155.5 |
| 4 | Yes | 113.0 | 109.5 | 120.0 | 120.0 | 57.0 | 59.5 | 59.5 | 59.5 | −60.5 |
| 5 | Yes | 40.0 | 46.5 | 48.5 | 48.5 | 38.5 | 38.0 | 41.0 | 38.5 | −7.5 |
| 6 | No | 62.0 | 101.0 | 127.5 | 127.5 | 90.5 | 111.0 | 131.5 | 131.5 | 4.0 |
| 7 | No | 336.0 | 323.5 | 352.5 | 352.5 | 258.5 | 226.5 | 237.5 | 258.5 | −94.0 |
| 8 | No | 173.0 | 249.0 | 248.5 | 249.0 | 60.0 | 60.5 | 71.5 | 71.5 | −177.5 |
| 9 | No | 506.0 | 554.5 | 673.5 | 673.5 | 53.0 | 47.5 | 115.0 | 115.0 | −558.5 |
| 10 | No | 285.0 | 339.0 | 366.5 | 366.5 | 43.5 | 104.0 | 130.5 | 130.5 | −236.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steffen, C.; Duda, K.; Wulsten, D.; Voss, J.O.; Koerdt, S.; Nahles, S.; Heiland, M.; Checa, S.; Rendenbach, C. Clinical and Technical Validation of Novel Bite Force Measuring Device for Functional Analysis after Mandibular Reconstruction. Diagnostics 2023, 13, 586. https://doi.org/10.3390/diagnostics13040586
Steffen C, Duda K, Wulsten D, Voss JO, Koerdt S, Nahles S, Heiland M, Checa S, Rendenbach C. Clinical and Technical Validation of Novel Bite Force Measuring Device for Functional Analysis after Mandibular Reconstruction. Diagnostics. 2023; 13(4):586. https://doi.org/10.3390/diagnostics13040586
Chicago/Turabian StyleSteffen, Claudius, Katharina Duda, Dag Wulsten, Jan O. Voss, Steffen Koerdt, Susanne Nahles, Max Heiland, Sara Checa, and Carsten Rendenbach. 2023. "Clinical and Technical Validation of Novel Bite Force Measuring Device for Functional Analysis after Mandibular Reconstruction" Diagnostics 13, no. 4: 586. https://doi.org/10.3390/diagnostics13040586