
The Proper Diagnosis of Thrombophilic Status in Preventing Fetal Growth Restriction

Abstract
:1. Introduction
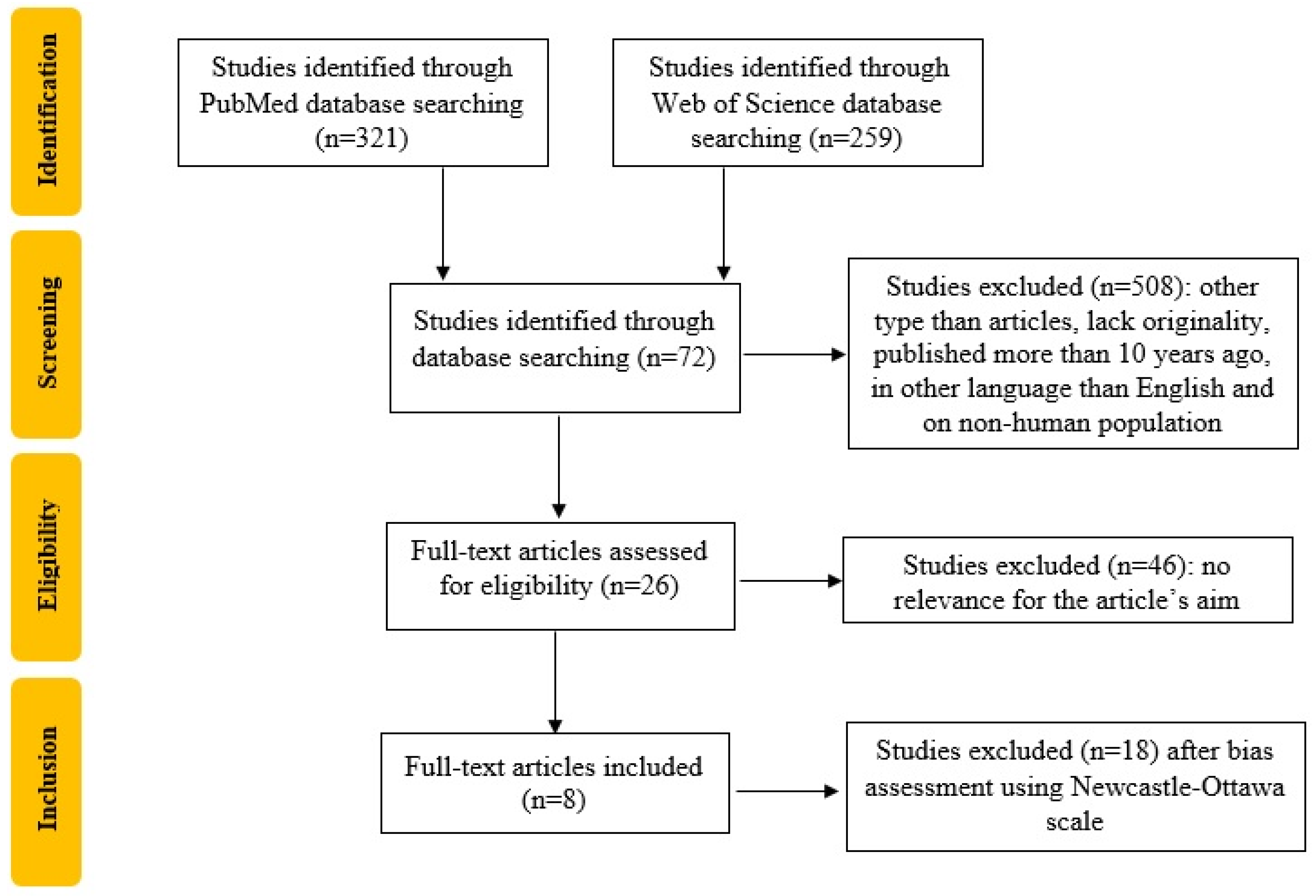
2. Materials and Methods
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nardozza, L.M.M.; Caetano, A.C.R.; Zamarian, A.C.P.; Mazzola, J.B.; Silva, C.P.; Marçal, V.M.G.; Lobo, T.F.; Peixoto, A.B.; Júnior, E.A. Fetal growth restriction: Current knowledge. Arch. Gynecol. Obstet. 2017, 295, 1061–1077. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins—Obstetrics and the Society forMaternal-FetalMedicin. ACOG Practice Bulletin No. 204: Fetal Growth Restriction. Obstet. Gynecol. 2019, 133, e97–e109. [Google Scholar] [CrossRef]
- Maulik, D. Fetal Growth Restriction: The Etiology. Clin. Obstet. Gynecol. 2006, 49, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Bohîlțea, R.E.; Dima, V.; Ducu, I.; Iordache, A.M.; Mihai, B.M.; Munteanu, O.; Grigoriu, C.; Veduță, A.; Pelinescu-Onciul, D.; Vlădăreanu, R. Clinically Relevant Prenatal Ultrasound Diagnosis of Umbilical Cord Pathology. Diagnostics 2022, 12, 236. [Google Scholar] [CrossRef] [PubMed]
- Bohiltea, R.E.; Varlas, V.-N.; Dima, V.; Iordache, A.-M.; Salmen, T.; Mihai, B.-M.; Bohiltea, A.T.; Vladareanu, E.M.; Ducu, I.; Grigoriu, C. The Strategy against Iatrogenic Prematurity Due to True Umbilical Knot: From Prenatal Diagnosis Challenges to the Favorable Fetal Outcome. J. Clin. Med. 2022, 11, 818. [Google Scholar] [CrossRef]
- Infante-Rivard, C.; Rivard, G.-E.; Yotov, W.V.; Génin, E.; Guiguet, M.; Weinberg, C.; Gauthier, R.; Feoli-Fonseca, J.C. Absence of Association of Thrombophilia Polymorphisms with Intrauterine Growth Restriction. N. Engl. J. Med. 2002, 347, 19–25. [Google Scholar] [CrossRef]
- McCowan, L.M.; Craigie, S.; Taylor, R.S.; Ward, C.; McLintock, C.; North, R.A. Inherited thrombophilias are not increased in “idiopathic” small-for-gestational-age pregnancies. Am. J. Obstet. Gynecol. 2003, 188, 981–985. [Google Scholar] [CrossRef]
- Martins, J.G.; Biggio, J.R.; Abuhamad, A. Society for Maternal-Fetal Medicine Consult Series #52: Diagnosis and management of fetal growth restriction. Am. J. Obstet. Gynecol. 2020, 223, B2–B17. [Google Scholar] [CrossRef]
- Shand, A.W.; Hornbuckle, J.; Nathan, E.; Dickinson, J.E.; French, N.P. Small for gestational age preterm infants and relationship of abnormal umbilical artery Doppler blood flow to perinatal mortality and neurodevelopmental outcomes. Aust. N. Z. J. Obstet. Gynaecol. 2009, 49, 52–58. [Google Scholar] [CrossRef]
- Leitner, Y.; Fattal-Valevski, A.; Geva, R.; Eshel, R.; Toledano-Alhadef, H.; Rotstein, M.; Bassan, H.; Radianu, B.; Bitchonsky, O.; Jaffa, A.J.; et al. Neurodevelopmental Outcome of Children with Intrauterine Growth Retardation: A Longitudinal, 10-Year Prospective Study. J. Child Neurol. 2007, 22, 580–587. [Google Scholar] [CrossRef]
- Gordijn, S.J.; Beune, I.M.; Thilaganathan, B.; Papageorghiou, A.; Baschat, A.A.; Baker, P.N.; Silver, R.M.; Wynia, K.; Ganzevoort, W. Consensus definition of fetal growth restriction: A Delphi procedure. Ultrasound Obstet. Gynecol. 2016, 48, 333–339. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists’ Committee on Practice Bulletins–Obstetrics. ACOG Practice Bulletin No. 197: Inherited Thrombophilias in Pregnancy. Obstet. Gynecol. 2018, 132, e18–e34. [Google Scholar] [CrossRef] [PubMed]
- McLintock, C.; Brighton, T.; Chunilal, S.; Dekker, G.; McDonnell, N.; McRae, S.; Müller, P.; Tran, H.; Walters, B.N.; Young, L.; et al. Recommendations for the prevention of pregnancy-associated venous thromboembolism. Aust. N. Z. J. Obstet. Gynaecol. 2011, 52, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.S.; Rey, E.; Kent, N.E.; VTE in Pregnancy Guideline Working Group; Chan, W.S.; Kent, N.E.; Rey, E.; Corbett, T.; David, M.; Douglas, M.J.; et al. Venous Thromboembolism and Antithrombotic Therapy in Pregnancy. J. Obstet. Gynaecol. Can. 2014, 36, 527–553. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Pereson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (N.O.S.) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses; The Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011; Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 4 December 2022).
- Mirzaei, F.; Farzad-Mahajeri, Z. Association of hereditary thrombophilia with intrauterine growth restriction. Iran. J. Reprod. Med. 2013, 11, 275–278. [Google Scholar]
- Berks, D.; Duvekot, J.J.; Basalan, H.; De Maat, M.P.; Steegers, E.A.; Visser, W. Associations between phenotypes of preeclampsia and thrombophilia. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 194, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Reshetnikov, E.; Zarudskaya, O.; Polonikov, A.; Bushueva, O.; Orlova, V.; Krikun, E.; Dvornyk, V.; Churnosov, M. Genetic markers for inherited thrombophilia are associated with fetal growth retardation in the population of Central Russia. J. Obstet. Gynaecol. Res. 2017, 43, 1139–1144. [Google Scholar] [CrossRef]
- Mutlu, I.; Mutlu, M.F.; Biri, A.; Bulut, B.; Erdem, M.; Erdem, A. Effects of anticoagulant therapy on pregnancy outcomes in patients with thrombophilia and previous poor obstetric history. Blood Coagul. Fibrinolysis 2015, 26, 267–273. [Google Scholar] [CrossRef]
- Vicoveanu, P.; Craiova, C.C.E.H.O. The association between factor V Leiden, MTHFR C667T/A1298C polymorphisms and pregnancy outcomes. Rev. Medico-Chir. 2021, 125, 563–569. [Google Scholar] [CrossRef]
- Kovac, M.; Mitic, G.; Mikovic, Z.; Mandic, V.; Miljic, P.; Mitrovic, M.; Tomic, B.; Bereczky, Z. The influence of specific mutations in the AT gene (SERPINC1) on the type of pregnancy related complications. Thromb. Res. 2018, 173, 12–19. [Google Scholar] [CrossRef]
- Zemet, R.; Dulitzki, M.; Baum, M.; Friedman, H.O.; Morag, I.; Simchen, M.J. Early-onset preeclampsia—The impact of antiphospholipid antibodies on disease severity. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 263, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Saccone, G.; Berghella, V.; Maruotti, G.M.; Ghi, T.; Rizzo, G.; Simonazzi, G.; Rizzo, N.; Facchinetti, F.; Dall’Asta, A.; Visentin, S.; et al. Antiphospholipid antibody profile based obstetric outcomes of primary antiphospholipid syndrome: The PREGNANTS study. Am. J. Obstet. Gynecol. 2017, 216, 525.e1–525.e12. [Google Scholar] [CrossRef] [PubMed]
- Dautaj, A.; Krasi, G.; Bushati, V.; Precone, V.; Gheza, M.; Fioretti, F.; Sartori, M.; Costantini, A.; Benedetti, S.; Bertelli, M. Hereditary thrombophilia. Acta Biomed. 2019, 90 (Suppl. S10), 44–46. [Google Scholar] [CrossRef]
- Paidas, M.J.; Ku, D.-H.W.; Arkel, Y.S. Screening and management of inherited thrombophilias in the setting of adverse pregnancy outcome. Clin. Perinatol. 2004, 31, 783–805. [Google Scholar] [CrossRef] [PubMed]
- Unterscheider, J.; O’Donoghue, K.; Daly, S.; Geary, M.P.; Kennelly, M.M.; McAuliffe, F.M.; Hunter, A.; Morrison, J.J.; Burke, G.; Dicker, P.; et al. Fetal growth restriction and the risk of perinatal mortality–case studies from the multicentre PORTO study. BMC Pregnancy Childbirth 2014, 14, 63. [Google Scholar] [CrossRef] [Green Version]
- Gerhardt, A.; Scharf, R.E.; Greer, I.A.; Zotz, R.B. Hereditary risk factors for thrombophilia and probability of venous thromboembolism during pregnancy and the puerperium. Blood 2016, 128, 2343–2349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paidas, M.J.; Hossain, N.; Shamsi, T.S.; Rodger, M.A.; Langhoff-Roos, J.; Lockwood, C.J. Hemostasis and Thrombosis in Obstetrics & Gynecology; John Wiley & Sons Ltd.: Chichester, UK, 2011. [Google Scholar]
- Kujovich, J.L. Factor V Leiden thrombophilia. Genet Med. 2011, 13, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attia, J.; Dudding, T.E. The association between adverse pregnancy outcomes and maternal factor V Leiden genotype: A meta-analysis. Thromb. Haemost. 2004, 91, 700–711. [Google Scholar] [CrossRef]
- Hemsworth, E.M.; O’Reilly, A.M.; Allen, V.M.; Kuhle, S.; Brock, J.-A.K.; Shah, P.; Ohlsson, A.; Shah, V.; Murphy, K.E.; McDonald, S.D.; et al. Association Between Factor V Leiden Mutation, Small for Gestational Age, and Preterm Birth: A Systematic Review and Meta-Analysis. J. Obstet. Gynaecol. Can. 2016, 38, 897–908. [Google Scholar] [CrossRef]
- Howley, H.; Walker, M.; Rodger, M.A. A systematic review of the association between factor V Leiden or prothrombin gene variant and intrauterine growth restriction. Am. J. Obstet. Gynecol. 2005, 192, 694–708. [Google Scholar] [CrossRef]
- Voicu, D.I.; Munteanu, O.; Gherghiceanu, F.; Arsene, L.V.; Bohiltea, R.E.; Gradinaru, D.M.; Cirstoiu, M.M. Maternal inherited thrombophilia and pregnancy outcomes. Exp. Ther. Med. 2020, 20, 2411–2414. [Google Scholar] [CrossRef]
- Bahrami, R.; Schwartz, D.A.; Asadian, F.; Karimi-Zarchi, M.; Dastgheib, S.A.; Tabatabaie, R.S.; Meibodi, B.; Neamatzadeh, H. Association of MTHFR 677C>T polymorphism with IUGR and placental abruption risk: A systematic review and meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 256, 130–139. [Google Scholar] [CrossRef]
- Dugalić, S.; Petronijevic, M.; Stefanovic, A.; Jeremic, K.; Petronijevic, S.V.; Soldatovic, I.; Pantic, I.; Djunic, I.; Jokic, Z.; Djokovic, F.; et al. The association between IUGR and maternal inherited thrombophilias. Medicine 2018, 97, e12799. [Google Scholar] [CrossRef]
- Del Gobbo, G.F.; Price, E.M.; Hanna, C.W.; Robinson, W.P. No evidence for association of MTHFR 677C>T and 1298A>C variants with placental DNA methylation. Clin. Epigenet. 2018, 10, 34. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; He, X.; Xiong, X.; Chuan, J.; Zhong, L.; Chen, G.; Yu, D. The association between maternal methylenetetrahydrofolate reductase C677T and A1298C polymorphism and birth defects and adverse pregnancy outcomes. Prenat. Diagn. 2018, 39, 3–9. [Google Scholar] [CrossRef]
- Alfirevic, Z.; Roberts, D.; Martlew, V. How strong is the association between maternal thrombophilia and adverse pregnancy outcome?: A systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2002, 101, 6–14. [Google Scholar] [CrossRef]
- Fernández-Alba, J.J.; González-Macías, C.; Sánchez, A.V.; Cepero, P.T.; Teruel, R.G.; García-Cabanillas, M.J.; Moreno-Corral, L.J.; Cardoso, R.T. Birthweight in pregnant women with protein S deficiency treated with low-molecular-weight heparin: A retrospective cohort study. J. Matern. Neonatal Med. 2016, 30, 2193–2197. [Google Scholar] [CrossRef]
- Xu, J.; Chen, D.; Tian, Y.; Wang, X.; Peng, B. Antiphospholipid Antibodies Increase the Risk of Fetal Growth Restriction: A Systematic Meta-Analysis. Int. J. Clin. Pr. 2022, 2022, 4308470. [Google Scholar] [CrossRef]
- Committee on Practice Bulletins—Obstetrics, American College of Obstetricians and Gynecologists Practice Bulletin No. 132: Antiphospholipid syndrome. Obstet. Gynecol. 2012, 120, 1514–1521. [CrossRef]
- Tranquilli, A.L.; Giannubilo, S.R.; Dell’Uomo, B.; Grandone, E. Adverse pregnancy outcomes are associated with multiple maternal thrombophilic factors. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 117, 144–147. [Google Scholar] [CrossRef]
- DE Vries, J.I.P.; VAN Pampus, M.G.; Hague, W.M.; Bezemer, P.D.; Joosten, J.H. Low-molecular-weight heparin added to aspirin in the prevention of recurrent early-onset pre-eclampsia in women with inheritable thrombophilia: The FRUIT-RCT. J. Thromb. Haemost. 2012, 10, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Abheiden, C.; Van Hoorn, M.; Hague, W.; Kostense, P.; van Pampus, M.; de Vries, J. Does low-molecular-weight heparin influence fetal growth or uterine and umbilical arterial Doppler in women with a history of early-onset uteroplacental insufficiency and an inheritable thrombophilia? Secondary randomised controlled trial results. BJOG Int. J. Obstet. Gynaecol. 2015, 123, 797–805. [Google Scholar] [CrossRef] [PubMed]
- De Carolis, S.; Ferrazzani, S.; De Stefano, V.; Garofalo, S.; Fatigante, G.; Rossi, E.; Leone, G.; Caruso, A. Inherited Thrombophilia: Treatment during Pregnancy. Fetal Diagn. Ther. 2006, 21, 281–286. [Google Scholar] [CrossRef]
- Blue, N.R.; Page, J.M.; Silver, R.M. Recurrence Risk of Fetal Growth Restriction: Management of Subsequent Pregnancies. Obstet. Gynecol. Clin. N. Am. 2021, 48, 419–436. [Google Scholar] [CrossRef]
- Tan, M.Y.; Poon, L.C.; Rolnik, D.L.; Syngelaki, A.; Matallana, C.D.P.; Akolekar, R.; Cicero, S.; Janga, D.; Singh, M.; Molina, F.S.; et al. Prediction and prevention of small-for-gestational-age neonates: Evidence from SPREE and ASPRE. Ultrasound Obstet. Gynecol. 2018, 52, 52–59. [Google Scholar] [CrossRef] [Green Version]
- Orudzhova, E.A.; Bitsadze, V.O.; Tretyakova, M.V.; Doronicheva, D.A.; Yakubova, F. Prevention of recurrent fetal growth retardation in patients with circulating antiphospholipid antibodies and genetic thrombophilia. Obstet. Gynecol. Reprod. 2022, 16, 134–142. [Google Scholar] [CrossRef]


{kind=link}
| Author | Diagnosis | Thrombophilia Type | Fetal Outcome |
|---|---|---|---|
| Mirzaei et al. [16] | Genetic | MTHFR C667T mutation | IUGR 48% vs. normal 20%, OR 69% with 95% CI, p = 0.037 |
| Biological | Protein S deficiency | IUGR 32% vs. normal 8%, OR 5.41% with 95% CI, p = 0.034 | |
| Genetic and biological | Multiple thrombophilia | IUGR 24% vs. normal 0, OR 2.1% with 95% CI 0–0.2, p = 0.009 | |
| Berks [17] | Genetic and biological | ≥1 thrombophilia factor (antiphospholipid antibodies, APC-resistance, protein C deficiency and protein S deficiency, hyperhomocysteinemia, factor V Leiden and prothrombin gene mutation) | IUGR 36.8% vs. normal 25.1%, p < 0.01 |
| Biological | Antiphospholipid antibodies | IUGR 9.5% vs. normal 5.1%, p < 0.01 | |
| Reshetnikov [18] | Genetic | Polymorphism G>A FVII rs6046 | G alleles: IUGR OR 2.34 with 95% CI 1.60–3.44, p < 0.001 GG alleles: IUGR OR 2.64 with 95% CI 1.71–4.09, p < 0.001 GA alleles: IUGR OR 0.42 with 95% CI 0.27–0.64, p < 0.001 |
| Mutlu [19] | Genetic | MTHFR mutations (C677T and A1298C) | IUGR in 90.9% cases |
| Vicoveanu [20] | Genetic | Homozygous mutation of factor V Leiden | IUGR in 33.3% cases, p = 0.04 |
| Factor V Leiden and MTHFR mutations | IUGR in 83.4% cases, p = 0.02 | ||
| Kovac [21] | Genetic | Homozygous type II HBS (Antithrombin Budapest 3) | IUGR in 22% cases |
| Zemet [22] | Biological | Antiphospholipid antibodies (anticardiolipin antibodies, β2 Glycoprotein1 antibodies or lupus anticoagulant) | IUGR in 25% cases vs. normal 17.1%, p = 0.7 |
| Saccone [23] | Biological | Antiphospholipid antibodies (anticardiolipin antibodies, β2 glycoprotein1 antibodies or lupus anticoagulant) | IUGR in 40.8% cases with single positive antiphospholipid antibody and 53.6% in more than 1 positive antibody—OR 2.55 with 95% CI 1.07–2.59, p < 0.01 Severe preterm IUGR in 13.4% cases with single positive antiphospholipid antibody and 28.2% in more than 1 positive antibody—OR 2.09 with 95% CI 1.44–3.04, p < 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mihai, B.-M.; Salmen, T.; Cioca, A.-M.; Bohîlțea, R.-E. The Proper Diagnosis of Thrombophilic Status in Preventing Fetal Growth Restriction. Diagnostics 2023, 13, 512. https://doi.org/10.3390/diagnostics13030512
Mihai B-M, Salmen T, Cioca A-M, Bohîlțea R-E. The Proper Diagnosis of Thrombophilic Status in Preventing Fetal Growth Restriction. Diagnostics. 2023; 13(3):512. https://doi.org/10.3390/diagnostics13030512
Chicago/Turabian StyleMihai, Bianca-Margareta, Teodor Salmen, Ana-Maria Cioca, and Roxana-Elena Bohîlțea. 2023. "The Proper Diagnosis of Thrombophilic Status in Preventing Fetal Growth Restriction" Diagnostics 13, no. 3: 512. https://doi.org/10.3390/diagnostics13030512