
Investigation of the Relationship between Sagittal Skeletal Nasal Profile Morphology and Malocclusions: A Lateral Cephalometric Film Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethic and Sample Selection
- Individuals over 16 years of age;
- No prior orthodontic treatment;
- No tooth loss;
- Not having undergone any nasal surgery or aesthetic operation;
- Not having a facial pathology or/and syndrome;
- No nasal trauma.
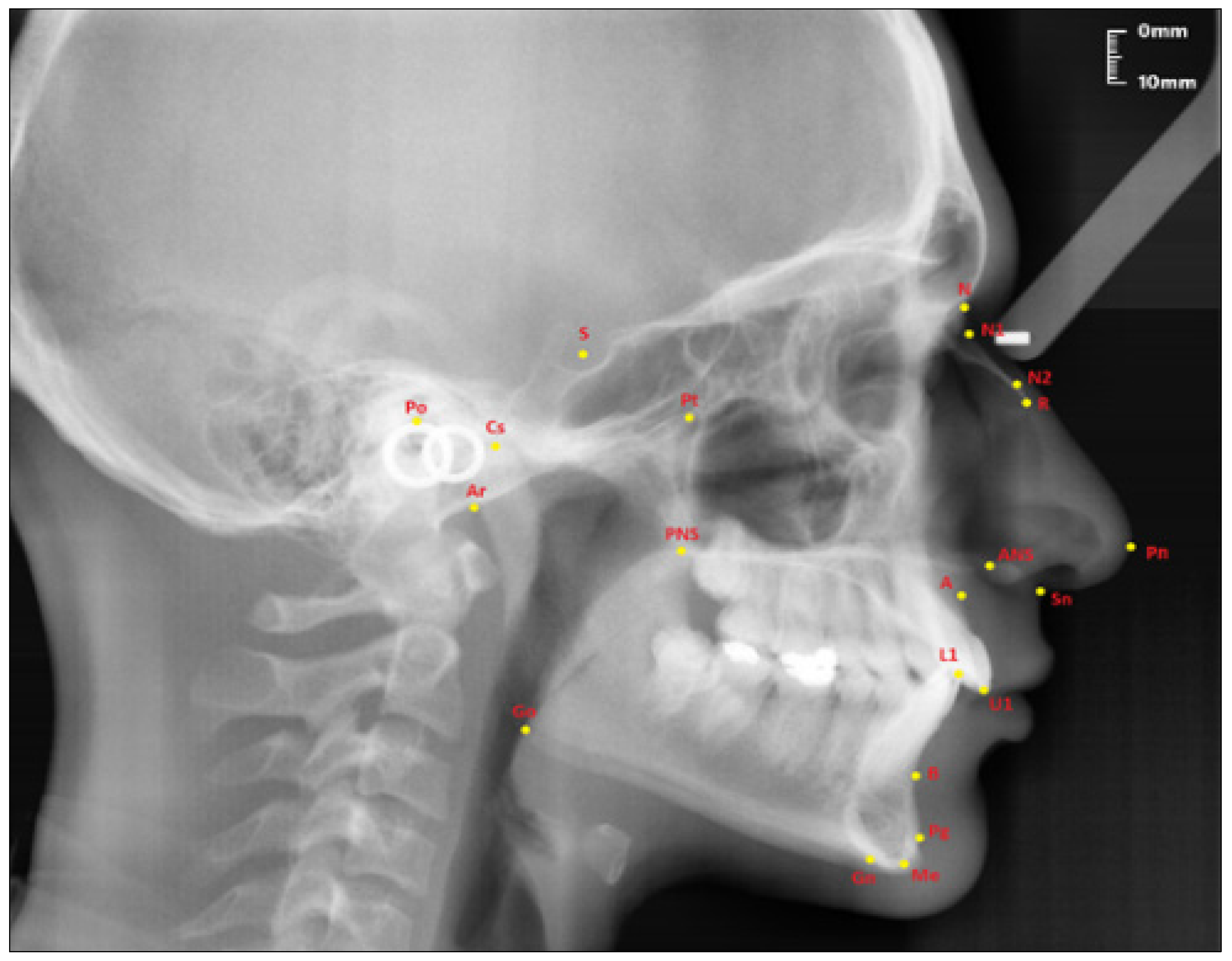
2.2. Cephalometric Analysis
2.3. Sample Groups
- Sella (S); the center of Sella turcica.
- Nasion (N); the most anterior point of the sutura frontonasalis and the deepest place of the recess in that region.
- Rhinion (R); the most anterior and inferior point on the tip of the nasal bone.
- Subspinal–point A; below the ANS point, the maxilla is the deepest point of the alveolar bone recess.
- Supramental–point B; deepest midline point on the mandible between infradentale and pogonion.
- Anterior nasal spine (ANS) point; the tip of the median, sharp bony process of the maxilla at the lower margin of the anterior nasal opening.
- N1 point; the most concave point of the nasal bone.
- N2 point; the most convex point of the nasal bone.
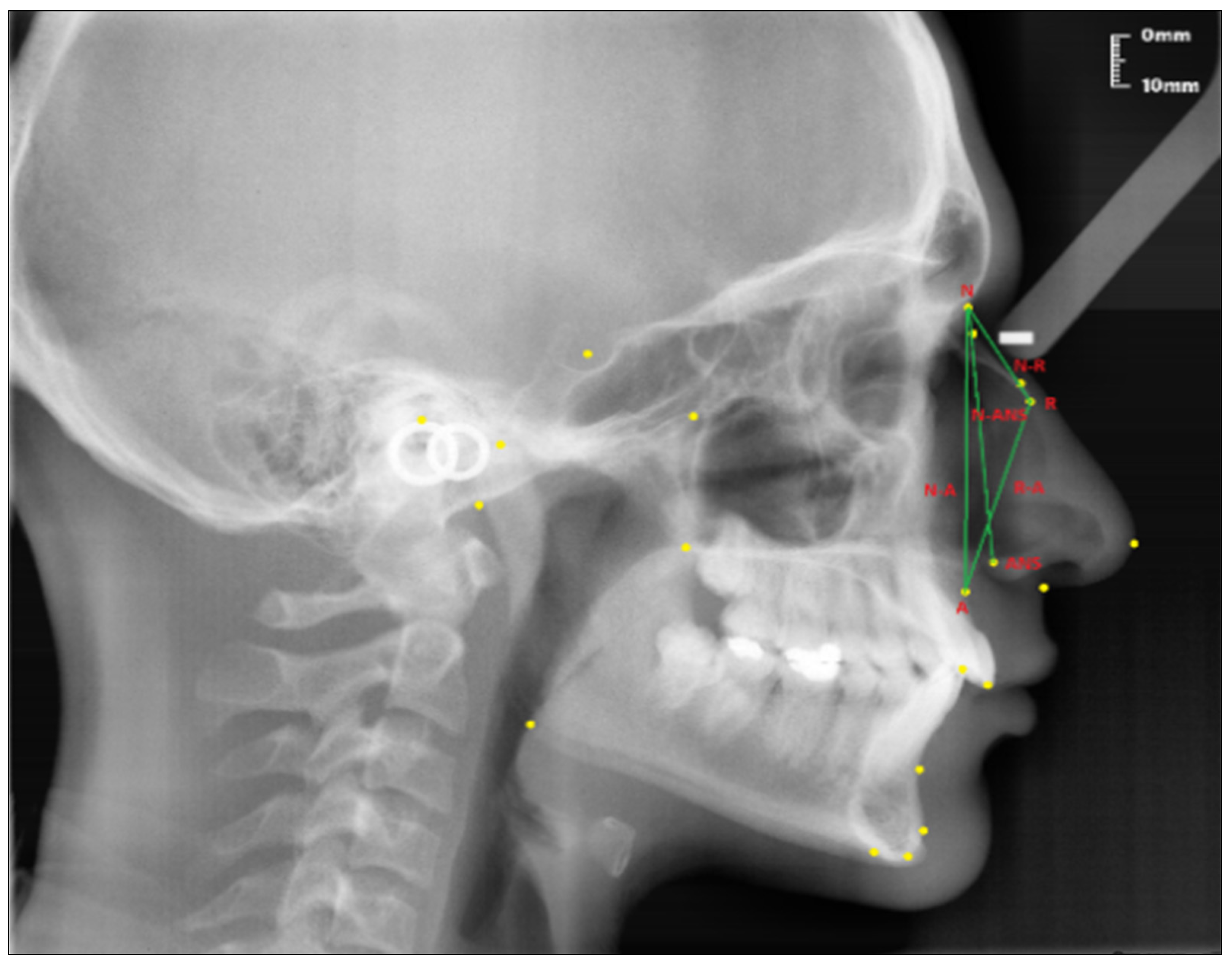
- Nasion-Rhinion (N-R); the distance between the nasion and the rhinion points.
- Nasion-Anterior nasal spina (N-ANS); the distance between the nasion and the anterior nasal spina points.
- Rhinion-Subspinale (R-A); the distance between the rhinion and the subspinale points.
- Nasion-Subspinale (N-A); the distance between the nasion and the subspinale points.
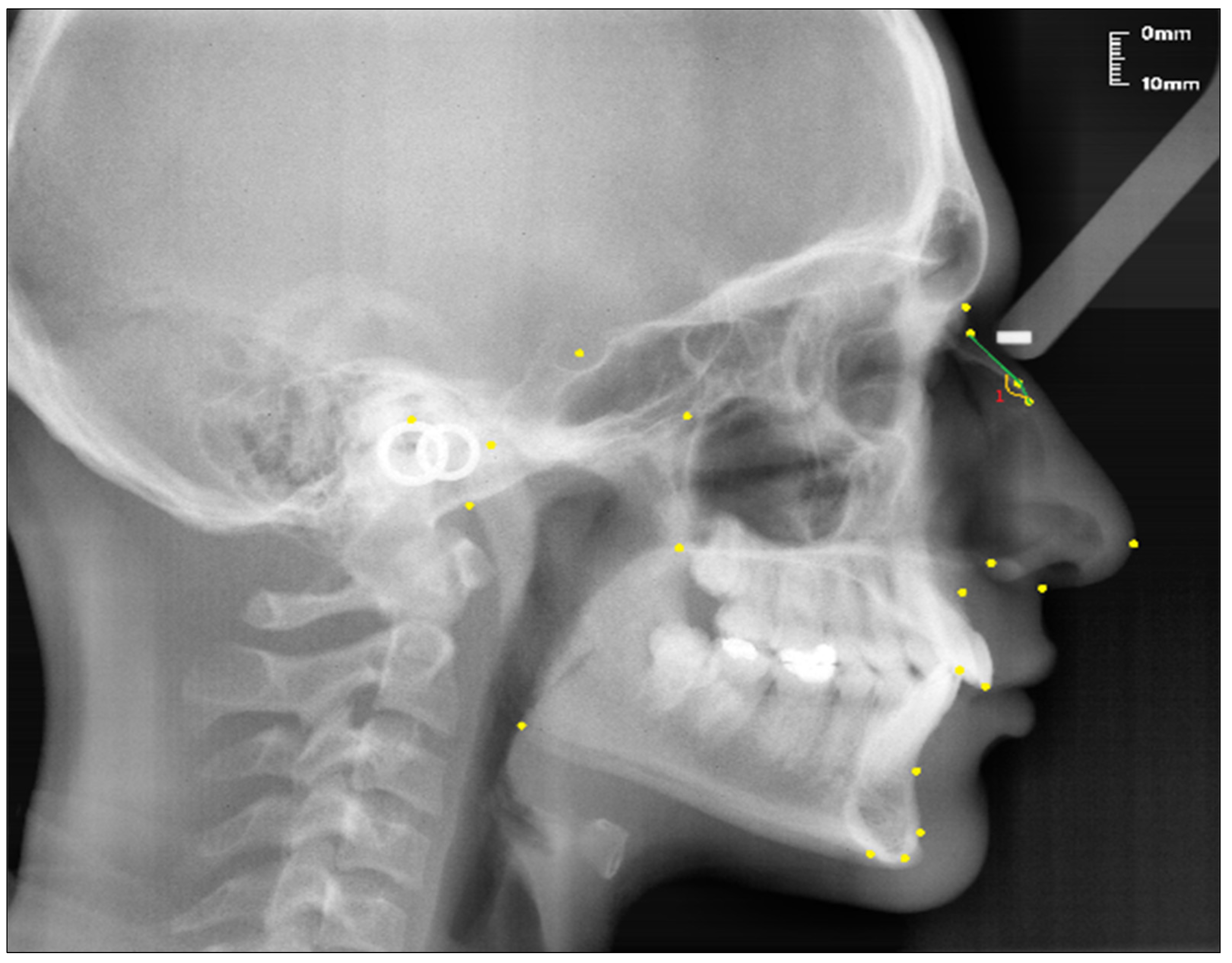
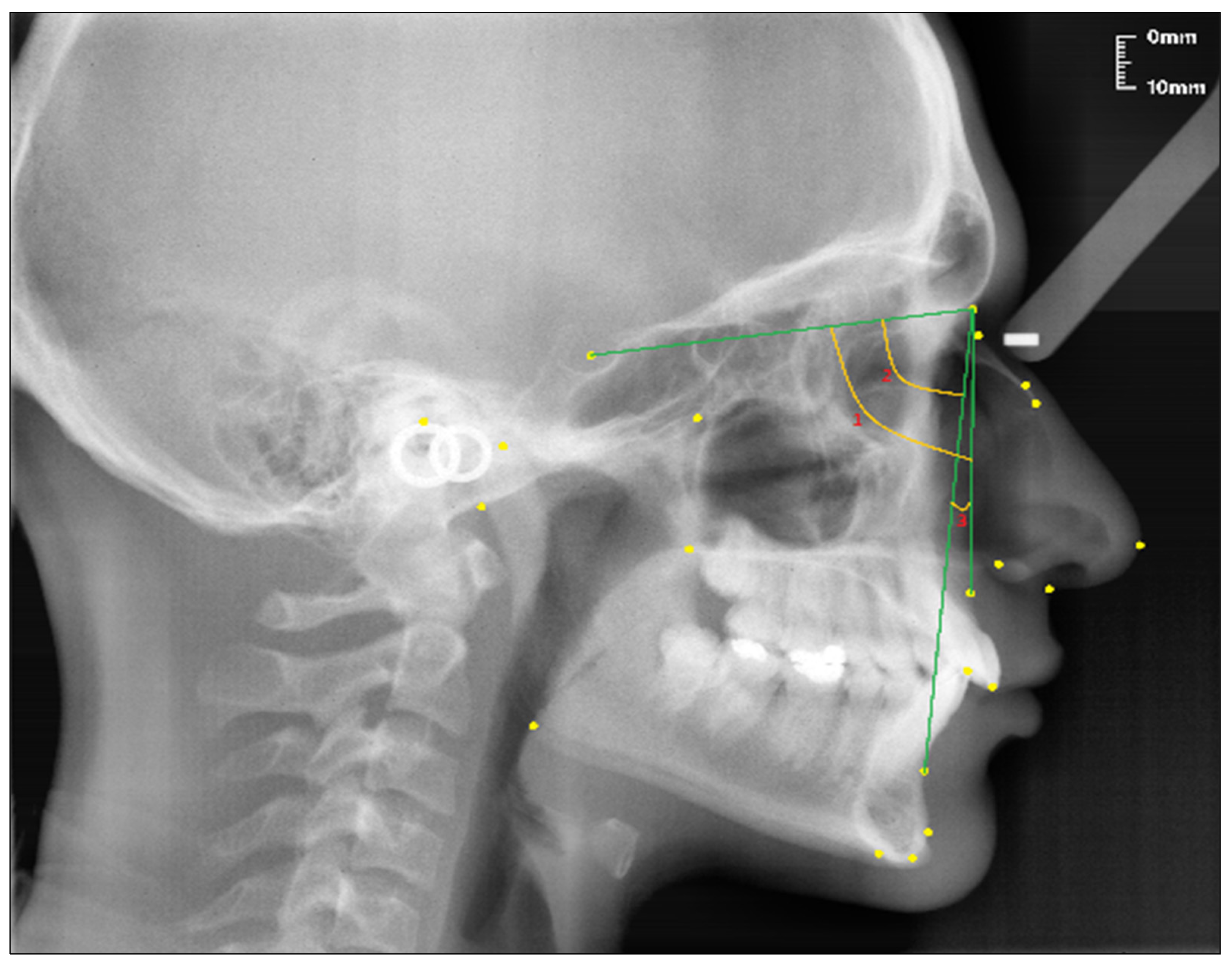
- Nasal Bone Concavity Angle (Nbone Angle); the posterior angle formed between the N1-N2 line and the N2-R line.
- SNA (°); the angle between the SN line and the NA line.
- SNB (°); the angle between the SN line and the NB line.
- ANB (°); the angle between the lines NA and NB.
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- All nasal dimensions were longer in males than females;
- It was observed that skeletal Class 3 individuals had longer nasal linear parameters than skeletal Class 1 and skeletal Class 2 individuals;
- Although the nasal bone concavity angle was greater in skeletal Class 2 individuals, it was not associated with other malocclusions;
- For the sake of detailed and distinctive findings, there is a need for new studies to be conducted on identical twins, fraternal twins, and ordinary siblings. In addition, some investigations should be taken to determine the effects of heredity and environment on nasal growth and development, by forming groups in a larger sample in vertical and transversal directions.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gulsen, A.; Okay, C.; Aslan, B.I.; Uner, O.; Yavuzer, R. The relationship between craniofacial structures and the nose in Anatolian Turkish adults: A cephalometric evaluation. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 131.e15–132.e25. [Google Scholar] [CrossRef]
- Arman, A.; Toygar, T.U.; Abuhijleh, E. Profile changes associated with different orthopedic treatment approaches in Class III malocclusions. Angle Orthod. 2004, 74, 733–740. [Google Scholar] [PubMed]
- Ruf, S.; Pancherz, H. Dentoskeletal effects and facial profile changes in young adults treated with the Herbst appliance. Angle Orthod. 1999, 69, 239–246. [Google Scholar] [PubMed]
- Naran, S.; Steinbacher, D.M.; Taylor, J.A. Current Concepts in Orthognathic Surgery. Plast. Reconstr. Surg. 2018, 141, 925e–936e. [Google Scholar] [CrossRef] [PubMed]
- Park, H.S.; Rhee, S.C.; Kang, S.R.; Lee, J.H. Harmonized profiloplasty using balanced angular profile analysis. Aesthetic Plast. Surg. 2004, 28, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Layoun, W.; Guyot, L.; Richard, O.; Gola, R. Augmentation of cheek bone contour using malar osteotomy. Aesthetic Plast. Surg. 2003, 27, 269–274. [Google Scholar] [CrossRef]
- Santanchè, P.; Bonarrigo, C. Lifting of the upper lip: Personal technique. Plast. Reconstr. Surg. 2004, 113, 1828–1835. [Google Scholar] [CrossRef] [PubMed]
- Nehra, K.; Sharma, V. Nasal morphology as an indicator of vertical maxillary skeletal pattern. J. Orthod. 2009, 36, 160–166. [Google Scholar] [CrossRef]
- Prasad, M.; Chaitanya, N.; Reddy, K.P.K.; Talapaneni, A.K.; Myla, V.B.; Shetty, S.K. Evaluation of nasal morphology in predicting vertical and sagittal maxillary skeletal discrepancies. Eur. J. Dent. 2014, 8, 197–204. [Google Scholar] [CrossRef] [Green Version]
- Cankaya, O.S.; Celebi, F.; Bicakci, A.A. Effects of different nose types on class II treatments for female patients. Prog. Orthod. 2019, 20, 1–8. [Google Scholar] [CrossRef]
- Palma, P.; Bignami, M.; Delù, G.; De Bernardi, F.; Castelnuovo, P. Rhinoplasty for the Mediterranean nose. Facial Plast. Surg. 2003, 19, 279–294. [Google Scholar] [PubMed]
- Posen, J.M. A longitudinal study of the growth of the nose. Am. J. Orthod. Dentofac. Orthop. 1967, 53, 746–756. [Google Scholar] [CrossRef] [PubMed]
- Chaconas, S.J. A statistical evaluation of nasal growth. Am. J. Orthod. Dentofac. Orthop. 1969, 56, 403–414. [Google Scholar] [CrossRef] [PubMed]
- Papesch, E.; Papesch, M. The nasal pyriform aperture and its importance. OTOHNS 2016, 1, 89–91. [Google Scholar] [CrossRef]
- Kabakci, A.D.A.; Saygin, D.A.; Alpa, Ş.; Buyukmumcu, M.; Yılmaz, M.T. An evaluation on the morphology of the nasal bone, piriform aperture, and choana on dry skulls. J. Anat. Soc. India 2020, 69, 213. [Google Scholar] [CrossRef]
- Yüzbasioglu, N.; Yilmaz, M.T.; Çicekcibasi, A.E.; Seker, M.; Sakarya, M.E. The evaluation of morphometry of nasal bone and pyriform aperture using multidetector computed tomography. J. Craniofac. Surg. 2014, 25, 2214–2219. [Google Scholar] [CrossRef]
- Proffit, W.R. The Etiology of Orthodontic Problems. In Contemporary Orthodontics, 6th ed.; Proffit, W.R., Fields, H.W., Larson, B., Sarver, D.M., Eds.; Elsevier Health Sciences: Philadelphia, PA, USA, 2018; pp. 107–140. [Google Scholar]
- Ochoa, B.K.; Nanda, R.S. Comparison of maxillary and mandibular growth. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 148–159. [Google Scholar] [CrossRef]
- Viteporn, S. The technique of cephalometric radiography. In Orthodontic Cephalometry; Mosby-Wolfe: London, UK, 1995; pp. 9–20. [Google Scholar]
- Broadbent, B.H. A new x-ray technique and its application to orthodontia. Angle Orthod. 1931, 1, 45–66. [Google Scholar]
- Tweed, C.H. The Frankfort-mandibular plane angle in orthodontic diagnosis, classification, treatment planning, and prognosis. Am. J. Orthod. Oral Surg. 1946, 32, 175–230. [Google Scholar] [CrossRef]
- Downs, W.B. Variations in facial relationships: Their significance in treatment and prognosis. Am. J. Orthod. Dentofac. Orthop. 1948, 34, 812–840. [Google Scholar] [CrossRef]
- Sassouni, V. Diagnosis and treatment planning via roentgenographic cephalometry. Am. J. Orthod. Dentofac. Orthop. 1958, 44, 433–463. [Google Scholar] [CrossRef]
- Ricketts, R.M. A foundation for cephalometric communication. Am. J. Orthod. Dentofac. Orthop. 1960, 46, 330–357. [Google Scholar] [CrossRef]
- Steiner, C.C. Cephalometrics for you and me. Am. J. Orthod. 1953, 39, 729–755. [Google Scholar] [CrossRef]
- Robison, J.M.; Rinchuse, D.J.; Zullo, T.G. Relationship of skeletal pattern and nasal form. Am. J. Orthod. Dentofac. Orthop. 1986, 89, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Lai, E.H.-H.; Liu, J.-P.; Chang, J.Z.-C.; Tsai, S.-J.; Yao, C.-C.J.; Chen, M.-H.; Chen, Y.-J.; Lin, C.-P. Radiographic assessment of skeletal maturation stages for orthodontic patients: Hand-wrist bones or cervical vertebrae? J. Formos. Med. Assoc. 2008, 107, 316–325. [Google Scholar] [CrossRef] [Green Version]
- Baccetti, T.; Franchi, L.; McNamara Jr, J.A. The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. In Seminars in Orthodontics; Elsevier: Amsterdam, The Netherlands, 2005. [Google Scholar]
- Steiner, C.C. Cephalometrics in clinical practice. Angle Orthod. 1959, 29, 8–29. [Google Scholar]
- Ülgen, M. (Ed.) Sefalometri. In Ortodonti: Anomaliler, Sefalometri, Etiloji, Büyüme ve Gelişim, Tanı; 5.Baskı; Dicle Üniversitesi: Diyarbakır, Türkiye, 2000; pp. 41–107. [Google Scholar]
- Rynn, C.; Wilkinson, C.M.; Peters, H.L. Prediction of nasal morphology from the skull. Forensic Sci. Med. Pathol. 2010, 6, 20–34. [Google Scholar] [CrossRef]
- Mommaerts, M.Y.; Lippens, F.; Abeloos, J.V.; Neyt, L.F. Nasal profile changes after maxillary impaction and advancement surgery. J. Oral Maxillofac. Surg. 2000, 58, 470–475. [Google Scholar] [CrossRef]
- Chung, C.; Lee, Y.; Park, K.-H.; Park, S.-H.; Park, Y.-C.; Kim, K.-H. Nasal changes after surgical correction of skeletal Class III malocclusion in Koreans. Angle Orthod. 2008, 78, 427–432. [Google Scholar] [CrossRef]
- Altug-Atac, A.T.; Bolatoglu, H.; Memikoglu, U.T. Facial soft tissue profile following bimaxillary orthognathic surgery. Angle Orthod. 2008, 78, 50–57. [Google Scholar] [CrossRef]
- Alhammadi, M.S.; Al-Mashraqi, A.A.; Alnami, R.H.; Ashqar, N.M.; Alamir, O.H.; Halboub, E.; Reda, R.; Testarelli, L.; Patil, S. Accuracy and reproducibility of facial measurements of digital photographs and wrapped cone beam computed tomography (CBCT) photographs. Diagnostics 2021, 11, 757. [Google Scholar] [CrossRef]
- Lee, S.R.; Lee, J.; Chung, D.; Lee, S. Short-term impact of microimplant-assisted rapid palatal expansion on the nasal soft tissues in adults: A three-dimensional stereophotogrammetry study. Korean J. Orthod. 2020, 50, 75. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, R.B.N.; Çakan, D.G.; Altay, M.; İbrahim Canter, H. Reliability of measurements on plaster and digital models of patients with a cleft lip and palate. Turk. J. Orthod. 2019, 32, 65. [Google Scholar] [CrossRef] [PubMed]
- Kusnoto, B. Two-dimensional cephalometry and computerized orthognathic surgical treatment planning. Clin. Plast. Surg. 2007, 34, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Jankowska, A.; Janiszewska-Olszowska, J.; Jedliński, M.; Grocholewicz, K. Methods of analysis of the nasal profile: A systematic review with meta-analysis. Biomed. Res. Int. 2021, 2021, 6680175. [Google Scholar] [CrossRef] [PubMed]
- Hambleton, R.S. The soft-tissue covering of the skeletal face as related to orthodontic problems. Am. J. Orthod. Dentofac. Orthop. 1964, 50, 405–420. [Google Scholar] [CrossRef]
- Bergman, R.T.; Waschak, J.; Borzabadi-Farahani, A.; Murphy, N.C. Longitudinal study of cephalometric soft tissue profile traits between the ages of 6 and 18 years. Angle Orthod. 2014, 84, 48–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Loon, B.; Van Heerbeek, N.; Bierenbroodspot, F.; Verhamme, L.; Xi, T.; de Koning, M.; Ingels, K.; Bergé, S.; Maal, T. Three-dimensional changes in nose and upper lip volume after orthognathic surgery. Int. J. Oral Maxillofac. Surg. 2015, 44, 83–89. [Google Scholar] [CrossRef]
- Karadag, D.; Ozdol, N.; Beriat, K.; Akinci, T. CT evaluation of the bony nasal pyramid dimensions in Anatolian people. DMFR 2011, 40, 160–164. [Google Scholar] [CrossRef]
- Hwang, T.-S.; Song, J.; Yoon, H.; Cho, B.-P.; Kang, H.-S. Morphometry of the nasal bones and piriform apertures in Koreans. Anat. Anz. 2005, 187, 411–414. [Google Scholar] [CrossRef] [PubMed]
- Lang, J.; Baumeister, R. Über das postnatale Wachstum der Nasenhöhle. Gegenbaurs Morphol Jb 1982, 128, 354–493. [Google Scholar]
- Ofodile, F.A. Nasal bones and pyriform apertures in blacks. Ann. Plast. Surg. 1994, 32, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Ellis III, E.; McNamara Jr, J.A. Components of adult Class III malocclusion. J. Oral Maxillofac. Surg. 1984, 42, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Basciftci, F.A.; Uysal, T.; Buyukerkmen, A. Craniofacial structure of Anatolian Turkish adults with normal occlusions and well-balanced faces. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Ligthelm-Bakker, A.; Wattel, E.; Uljee, I.; Prahl-Andersen, B. Vertical growth of the anterior face: A new approach. Am. J. Orthod. Dentofac. Orthop. 1992, 101, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Genecov, J.S.; Sinclair, P.M.; Dechow, P.C. Development of the nose and soft tissue profile. Angle Orthod. 1990, 60, 191–198. [Google Scholar] [CrossRef]
- Ardani, I.G.A.W.; Willyanti, I.; Narmada, I.B. Correlation between vertical components and skeletal Class II malocclusion in ethnic Javanese. Clin. Cosmet. Investig. Dent. 2018, 10, 297. [Google Scholar] [CrossRef] [Green Version]
- Buschang, P.H.; De La Cruz, R.; Viazis, A.D.; Demirjian, A. Longitudinal shape changes of the nasal dorsum. Am. J. Orthod. Dentofac. Orthop. 1993, 104, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Arshad, T.; Shaikh, A.; Fida, M. Comparison of nasal profiles in various skeletal patterns. JAMC 2013, 25, 31–35. [Google Scholar]
- Richmond, S.; Howe, L.J.; Lewis, S.; Stergiakouli, E.; Zhurov, A. Facial genetics: A brief overview. Front. Genet. 2018, 9, 462. [Google Scholar] [CrossRef] [Green Version]
- Bishara, S.E. Class II malocclusions: Diagnostic and clinical considerations with and without treatment. In Seminars in Orthodontics; Elsevier: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Küchler, E.C.; Barreiros, D.; da Silva, R.O.; de Abreu, J.G.B.; Teixeira, E.C.; da Silva, R.A.B.; da Silva, L.A.B.; Nelson, P.; Romano, F.L.; Granjeiro, J.M. Genetic polymorphism in MMP9 may be associated with anterior open bite in children. Braz. Dent. J. 2017, 28, 277–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markovic, M.D. At the crossroads of oral facial genetics. Eur. J. Orthod. 1992, 14, 469–481. [Google Scholar] [CrossRef] [PubMed]
- Neela, P.K.; Atteeri, A.; Mamillapalli, P.K.; Sesham, V.M.; Keesara, S.; Chandra, J.; Monica, U.; Mohan, V. Genetics of dentofacial and orthodontic abnormalities. Glob. Med. Genet. 2020, 7, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Hartsfield, J.K., Jr.; Morford, L.A.; Otero, L.M. Genetic factors affecting facial growth. In Orthodontics-Basic Aspects and Clinical Considerations; Bourzgui, F., Ed.; InTech: Rijeka, Croatia, 2012; pp. 125–152. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | ||
|---|---|---|
| Skeletal Angular Parameters | Nasal Parameters | |
| Linear Parameters | Angular Parameter | |
| SNA SNB ANB | N-R R-A N-A N-ANS | N1N2-N2R (Nasal bone concavity angle) |
| Skeletal Class 1 (n/%) | Skeletal Class 2 (n/%) | Skeletal Class 3 (n/%) | |
|---|---|---|---|
| Males | 20/14.8 | 17/12.5 | 12/9 |
| Females | 33/24.4 | 39/28.8 | 14/10.5 |
| Total | 53/39.2 | 56/41.3 | 26/19.5 |
| Distance N-R (mm) | Distance R-A (mm) | Distance N-A (mm) | Distance N-ANS (mm) | |||||
|---|---|---|---|---|---|---|---|---|
| ± ss | p | ± ss | p | ± ss | p | ± ss | p | |
| Gender + | ||||||||
| Males | 24.96 ± 3.73 | 0.283 | 42.59 ± 3.05 | 0.000 * | 59.35 ± 3.98 | 0.000 * | 54.32 ± 3.45 | 0.000 * |
| Females | 24.32 ± 3.12 | 38.60 ± 2.87 | 55.95 ± 3.52 | 51.81 ± 3.05 | ||||
| Skeletal Classification ++ | ||||||||
| Class 1 | 24.13 ± 3.11 | 0.028 * | 39.60 ± 2.92 | 0.493 | 56.36 ± 3.39 | 0.084 | 51.96 ± 3.07 | 0.073 |
| Class 2 | 24.22 ± 3.42 | 40.28 ± 3.73 | 57.37 ± 4.10 | 52.97 ± 3.50 | ||||
| Class 3 | 26.12 ± 3.36 | 40.54 ± 4.08 | 58.46 ± 4.79 | 53.72 ± 3.41 | ||||
| Skeletal Classification | Skeletal Classification | Average Difference | p |
|---|---|---|---|
| Class 1 | Class 2 | −0.09068 ± 0.63 | 0.989 |
| Class 3 | −1.99373 ± 0.78 | 0.034 * | |
| Class 2 | Class 1 | 0.09068 ± 0.63 | 0.989 |
| Class 3 | −1.90305 ± 0.78 | 0.043 * | |
| Class 3 | Class 1 | 1.99373 ± 0.78 | 0.034 * |
| Class 2 | 1.90305 ± 0.78 | 0.043 * |
| N1-N2/N2-R Angle (Nasal Bone Concavity Angle) | ||
|---|---|---|
| ± ss | p | |
| Gender + | ||
| Males | 162.11° ± 6.89° | 0.206 |
| Females | 163.60° ± 6.30° | |
| Skeletal Classification ++ | ||
| Class 1 | 162.45°± 7.16° | 0.180 |
| Class 2 | 164.25° ± 6.28° | |
| Class 3 | 161.71° ± 5.42° | |
| Linear Nasal Parameters | Skeletal Classification | Males | Females | |
|---|---|---|---|---|
| ± ss | ± ss | p | ||
| N-R | Class 1 | 24.63 ± 3.96 | 23.83 ± 2.48 | 0.367 |
| Class 2 | 24.67 ± 3.,43 | 24.02 ± 3.44 | 0.517 | |
| Class 3 | 25.93 ± 3.92 | 26.29 ± 2.99 | 0.794 | |
| R-A | Class 1 | 41.86 ± 2.20 | 38.23 ± 2.42 | 0.000 * |
| Class 2 | 42.76 ± 3.88 | 39.20 ± 3.14 | 0.001 * | |
| Class 3 | 43.54 ± 2.91 | 37.80 ± 2.91 | 0.000 * | |
| N-A | Class 1 | 58.20 ± 3.88 | 55.24 ± 2.50 | 0.001 * |
| Class 2 | 59.63 ± 3.97 | 56.39 ± 3.80 | 0.006 * | |
| Class 3 | 60.87 ± 3.91 | 56.39 ± 4.61 | 0.014 * | |
| N-ANS | Class 1 | 53.29 ± 3.41 | 51.16 ± 2.47 | 0.111 |
| Class 2 | 55.13 ± 3.01 | 52.03 ± 3.31 | 0.102 | |
| Class 3 | 54.88 ± 3.93 | 52.76 ± 3.39 | 0.153 | |
| N1-N2/N2-R | Class 1 | 162.13 ± 7.90 | 162.64 ± 6.80 | 0.803 |
| Class 2 | 164.26 ± 6.50 | 164.25 ± 6.28 | 0.997 | |
| Class 3 | 159.03 ± 4.55 | 164.01 ± 5.16 | 0.116 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ocak, Y.; Cicek, O.; Ozkalayci, N.; Erener, H. Investigation of the Relationship between Sagittal Skeletal Nasal Profile Morphology and Malocclusions: A Lateral Cephalometric Film Study. Diagnostics 2023, 13, 463. https://doi.org/10.3390/diagnostics13030463
Ocak Y, Cicek O, Ozkalayci N, Erener H. Investigation of the Relationship between Sagittal Skeletal Nasal Profile Morphology and Malocclusions: A Lateral Cephalometric Film Study. Diagnostics. 2023; 13(3):463. https://doi.org/10.3390/diagnostics13030463
Chicago/Turabian StyleOcak, Yunus, Orhan Cicek, Nurhat Ozkalayci, and Hande Erener. 2023. "Investigation of the Relationship between Sagittal Skeletal Nasal Profile Morphology and Malocclusions: A Lateral Cephalometric Film Study" Diagnostics 13, no. 3: 463. https://doi.org/10.3390/diagnostics13030463