
Invasive Pulmonary Aspergillosis: Not Only a Disease Affecting Immunosuppressed Patients
 , , and
, , and
Abstract
:1. Introduction
2. Relevant Sections
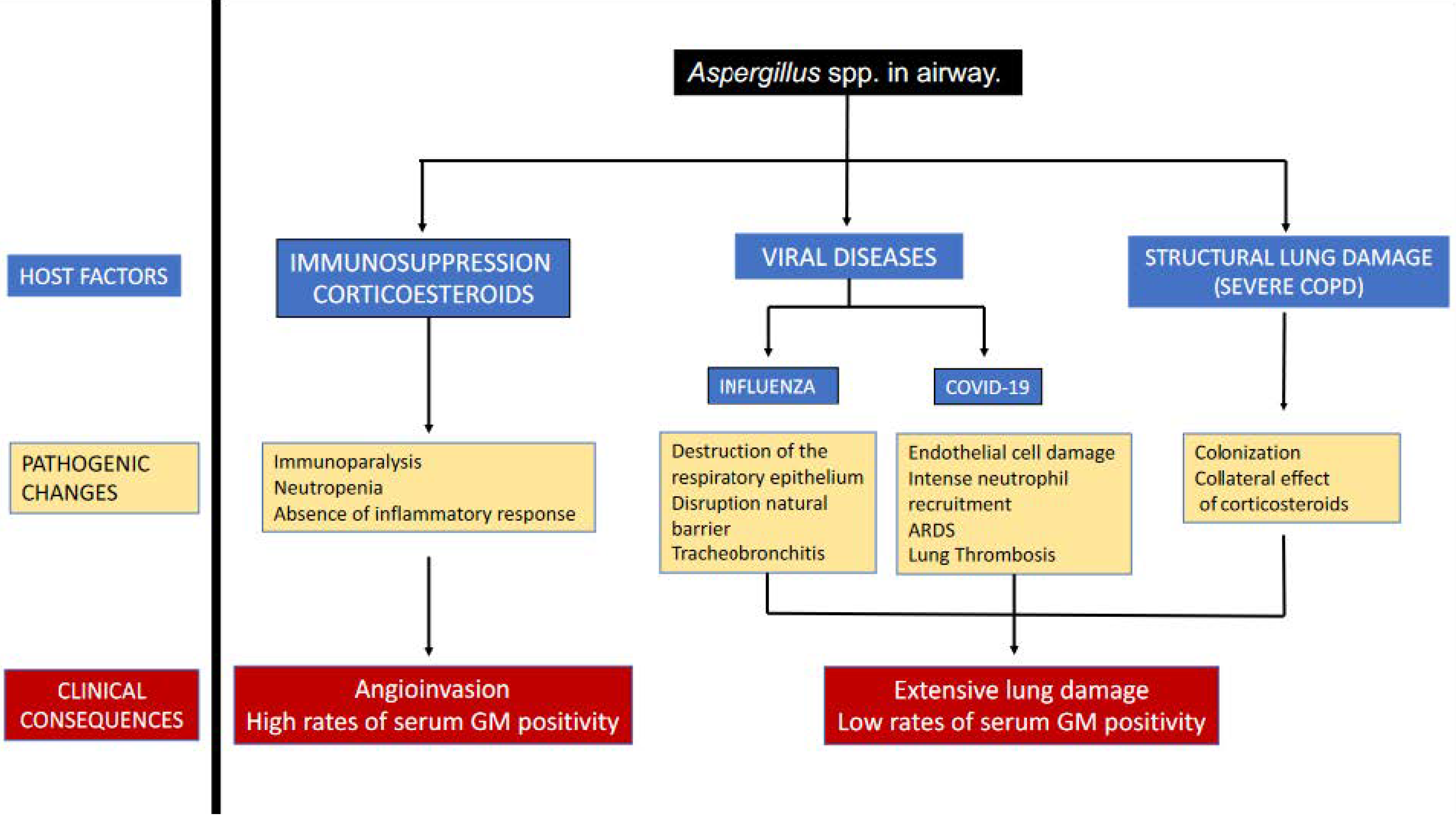
2.1. Physiopathology
2.2. Other Populations. Does It Really Exist as a Risk Factor in Non-Immunosuppressed?
2.3. IAPA and CAPA Parallelisms and Differences
3. Discussion
4. Conclusions
5. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vincent, J.-L.; Sakr, Y.; Singer, M.; Martin-Loeches, I.; Machado, F.R.; Marshall, J.C.; Finfer, S.; Pelosi, P.; Brazzi, L.; Aditianingsih, D.; et al. Prevalence and Outcomes of Infection Among Patients in Intensive Care Units in 2017. JAMA 2020, 323, 1478. Available online: https://jamanetwork.com/journals/jama/fullarticle/2763669 (accessed on 17 January 2023). [CrossRef] [PubMed]
- Vincent, J.-L.; Rello, J.; Marshall, J.K.; Silva, E.; Anzueto, A.; Martin, C.D.; Moreno, R.; Lipman, J.; Gomersall, C.; Sakr, Y.; et al. INternational study of the prevalence and outcomes of infection in intensive care units. JAMA 2009, 302, 2323–2329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zilberberg, M.D.; Shorr, A.F. Fungal infections in the ICU. Infect. Dis. Clin. North. Am. 2009, 23, 625–642. Available online: http://www.ncbi.nlm.nih.gov/pubmed/19665087 (accessed on 22 January 2013). [CrossRef] [PubMed]
- Matthaiou, D.K.; Christodoulopoulou, T.; Dimopoulos, G. How to treat fungal infections in ICU patients. BMC Infect. Dis. 2015, 15, 205. Available online: http://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-015-0934-8 (accessed on 17 January 2023). [CrossRef] [Green Version]
- Vallabhaneni, S.; Mody, R.K.; Walker, T.; Chiller, T. The Global Burden of Fungal Diseases. Infect. Dis. Clin. 2017, 30, 1–11. [Google Scholar] [CrossRef]
- De Pascale, G.; Tumbarello, M. Fungal infections in the ICU: Advances in treatment and diagnosis. Curr. Opin. Crit. Care 2015, 21, 421–429. [Google Scholar] [CrossRef]
- Limper, A.H.; Knox, K.S.; Sarosi, G.A.; Ampel, N.M.; Bennett, J.E.; Catanzaro, A.; Davies, S.F.; Dismukes, W.E.; Hage, C.A.; Marr, K.A.; et al. An official American Thoracic Society statement: Treatment of fungal infections in adult pulmonary and critical care patients. Am. J. Respir. Crit. Care Med. 2011, 183, 96–128. Available online: http://www.ncbi.nlm.nih.gov/pubmed/21193785 (accessed on 17 January 2023). [CrossRef] [Green Version]
- Townsend, L.; Martin-Loeches, I. Invasive Aspergillosis in the Intensive Care Unit. Diagnostics 2022, 12, 2712. [Google Scholar] [CrossRef]
- Thevissen, K.; Jacobs, C.; Holtappels, M.; Toda, M.; Verweij, P.; Wauters, J. International survey on influenza-associated pulmonary aspergillosis (IAPA) in intensive care units: Responses suggest low awareness and potential underdiagnosis outside Europe. Crit. Care 2020, 24, 84. [Google Scholar] [CrossRef] [Green Version]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.A.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Flörl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect. Dis. 2021, 21, e149–e162. [Google Scholar] [CrossRef]
- Gago, S.; Denning, D.W.; Bowyer, P. Pathophysiological aspects of Aspergillus colonization in disease. Med. Mycol. 2019, 57, S219–S227. [Google Scholar] [CrossRef]
- Denning, D.W. Invasive Aspergillosis. Clin. Infect. Dis. 1998, 26, 781–803. [Google Scholar] [CrossRef]
- Smith, N.L.; Denning, D.W. Underlying conditions in chronic pulmonary aspergillosis including simple aspergilloma. Eur. Respir. J. 2011, 37, 865–872. [Google Scholar] [CrossRef] [Green Version]
- Marr, K.A.; Platt, A.; Tornheim, J.A.; Zhang, S.X.; Datta, K.; Cardozo, C.; Garcia-Vidal, C. Aspergillosis Complicating Severe Coronavirus Disease. Emerg. Infect. Dis. 2021, 27, 18–25. [Google Scholar] [CrossRef]
- Shibuya, K.; Hasegawa, C.; Hamatani, S.; Hatori, T.; Nagayama, T.; Nonaka, H.; Ando, T.; Wakayama, M. Pathophysiology of pulmonary aspergillosis. J. Infect. Chemother. 2004, 10, 138–145. [Google Scholar] [CrossRef]
- Van de Veerdonk, F.L.; Wauters, J.; Verweij, P.E. Invasive Aspergillus Tracheobronchitis Emerging as a Highly Lethal Complication of Severe Influenza. Am. J. Respir. Crit. Care Med. 2020, 202, 646–648. [Google Scholar] [CrossRef]
- Lamoth, F.; Lewis, R.E.; Walsh, T.J.; Kontoyiannis, D.P. Navigating the Uncertainties of COVID-19–Associated Aspergillosis: A Comparison with Influenza-Associated Aspergillosis. J. Infect. Dis. 2021, 224, 1631–1640. [Google Scholar] [CrossRef]
- Paulussen, C.; Hallsworth, J.E.; Álvarez-Pérez, S.; Nierman, W.C.; Hamill, P.G.; Blain, D.; Rediers, H.; Lievens, B. Ecology of aspergillosis: Insights into the pathogenic potency of Aspergillus fumigatus and some other Aspergillus species. Microb. Biotechnol. 2017, 10, 296–322. [Google Scholar] [CrossRef] [Green Version]
- Sakr, Y.; Jaschinski, U.; Wittebole, X.; Szakmany, T.; Lipman, J.; Ñamendys-Silva, S.A.; Martin-Loeches, I.; Leone, M.; Lupu, M.-N.; Vincent, J.-L.; et al. Sepsis in Intensive Care Unit Patients: Worldwide Data From the Intensive Care over Nations Audit. Open Forum. Infect. Dis. 2018, 5, ofy313. Available online: http://www.ncbi.nlm.nih.gov/pubmed/30555852 (accessed on 17 January 2023). [CrossRef]
- Mokart, D.; Darmon, M.; Schellongowski, P.; Pickkers, P.; Soares, M.; Rello, J.; Bauer, P.R.; van de Louw, A.; Lemiale, V.; Taccone, F.S.; et al. Acute respiratory failure in immunocompromised patients: Outcome and clinical features according to neutropenia status. Ann. Intensive Care 2020, 10, 146. [Google Scholar] [CrossRef]
- Torres, A.; Martin-Loeches, I. Invasive Pulmonary Aspergillosis in Ventilator-associated Pneumonia: The Hidden Enemy? Am. J. Respir. Crit. Care Med. 2020, 202, 1071–1073. [Google Scholar] [CrossRef] [PubMed]
- Verweij, P.E.; Brüggemann, R.J.M.; Azoulay, E.; Bassetti, M.; Blot, S.; Buil, J.B.; Calandra, T.; Chiller, T.; Clancy, C.J.; Cornely, O.A.; et al. Taskforce report on the diagnosis and clinical management of COVID-19 associated pulmonary aspergillosis. Intensive Care Med. 2021, 47, 819–834. [Google Scholar] [CrossRef] [PubMed]
- Martin-Loeches, I.; Quinn, A.; Daniels, R.; Artigas, A.; Marsh, B.; Sakr, Y.; Povoa, P.; Salluh, J.; Martin, C.; Schultz, M. SEPsis REcognition and MAnagement (SEPREMA survey). Intensive Care Med. 2016, 42, 477–478. [Google Scholar] [CrossRef] [PubMed]
- Martin-Loeches, I.; Levy, M.M.M.M.; Artigas, A. Management of severe sepsis: Advances, challenges, and current status. Drug Des. Dev. Ther. 2015, 9, 2079–2088. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25926718 (accessed on 17 January 2023). [CrossRef] [Green Version]
- Kosmidis, C.; Denning, D.W. The clinical spectrum of pulmonary aspergillosis. Thorax 2015, 70, 270–277. [Google Scholar] [CrossRef] [Green Version]
- Patterson, T.F.; Thompson, G.R.; Denning, D.W.; Fishman, J.A.; Hadley, S.; Herbrecht, R.; Kontoyiannis, D.P.; Marr, K.A.; Morrison, V.A.; Nguyen, M.H.; et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 63, e1–e60. [Google Scholar] [CrossRef] [Green Version]
- Iversen, M.; Burton, C.M.; Vand, S.; Skovfoged, L.; Carlsen, J.; Milman, N.; Andersen, C.B.; Rasmussen, M.; Tvede, M. Aspergillus infection in lung transplant patients: Incidence and prognosis. Eur. J. Clin. Microbiol. Infect. Dis. 2007, 26, 879–886. [Google Scholar] [CrossRef]
- Nelson, J.; Alvey, N.; Bowman, L.; Schulte, J.; Segovia, M.C.; McDermott, J.; Te, H.S.; Kapila, N.; Levine, D.J.; Gottlieb, R.L.; et al. Consensus recommendations for use of maintenance immunosuppression in solid organ transplantation: Endorsed by the American College of Clinical Pharmacy, American Society of Transplantation, and the International Society for Heart and Lung Transplantation. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2022, 42, 599–633. [Google Scholar] [CrossRef]
- Verweij, P.E.; Rijnders, B.J.A.; Brüggemann, R.J.M.; Azoulay, E.; Bassetti, M.; Blot, S.; Calandra, T.; Clancy, C.J.; Cornely, O.A.; Chiller, T.; et al. Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: An expert opinion. Intensive Care Med. 2020, 46, 1524–1535. [Google Scholar] [CrossRef]
- Hoenigl, M.; Sprute, R.; Egger, M.; Arastehfar, A.; Cornely, O.A.; Krause, R.; Lass-Flörl, C.; Prattes, J.; Spec, A.; Thompson, G.R.; et al. The Antifungal Pipeline: Fosmanogepix, Ibrexafungerp, Olorofim, Opelconazole, and Rezafungin. Drugs 2021, 81, 1703–1729. [Google Scholar] [CrossRef]
- Klein, E.Y.; Monteforte, B.; Gupta, A.; Jiang, W.; May, L.; Hsieh, Y.-H.; Dugas, A. The frequency of influenza and bacterial coinfection: A systematic review and meta-analysis. Influenza Other Respir Viruses 2016, 10, 394–403. [Google Scholar] [CrossRef] [Green Version]
- Chertow, D.S. Contribution of bacterial coinfection to severe influenza infection. Crit. Care Med. 2012, 40, 1664–1665. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22511151 (accessed on 17 December 2012). [CrossRef]
- Martín-Loeches, I.; Sanchez-Corral, A.; Diaz, E.; Granada, R.M.; Zaragoza, R.; Villavicencio, C.; Albaya, A.; Cerdá, E.; Catalán, R.M.; Luque, P.; et al. Community-acquired respiratory coinfection in critically III patients with pandemic 2009 influenza A(H1N1) virus. Chest 2011, 139, 555–562. [Google Scholar] [CrossRef]
- Rice, T.W.; Rubinson, L.; Uyeki, T.M.; Vaughn, F.L.; John, B.B.; Miller, R.R.; Higgs, E.; Randolph, A.G.; Smoot, B.E.; Thompson, B.T. Critical illness from 2009 pandemic influenza A virus and bacterial coinfection in the United States. Crit. Care Med. 2012, 40, 1487–1498. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22511131 (accessed on 17 December 2012). [CrossRef] [Green Version]
- Rodríguez, A.H.A.H.; Avilés-Jurado, F.X.F.X.; Díaz, E.; Schuetz, P.; Trefler, S.I.S.I.; Solé-Violán, J.; Cordero, L.; Vidaur, L.; Estella, Á.; Pozo Laderas, J.C.J.C.; et al. Procalcitonin (PCT) levels for ruling-out bacterial coinfection in ICU patients with influenza: A CHAID decision-tree analysis. J. Infect. 2015, 72, 143–151. Available online: http://www.ncbi.nlm.nih.gov/pubmed/26702737 (accessed on 17 January 2023). [CrossRef]
- O’Donnell, J.S.; Peyvandi, F.; Martin-Loeches, I. Pulmonary immuno-thrombosis in COVID-19 ARDS pathogenesis. Intensive Care Med. 2021, 47, 899–902. [Google Scholar] [CrossRef]
- Martin-Loeches, I.; JSchultz, M.; Vincent, J.-L.; Alvarez-Lerma, F.; Bos, L.D.; Solé-Violán, J.; Torres, A.; Rodriguez, A. Increased incidence of co-infection in critically ill patients with influenza. Intensive Care Med. 2017, 43. [Google Scholar] [CrossRef]
- Hotchkiss, R.S.; Monneret, G.; Payen, D. Sepsis-induced immunosuppression: From cellular dysfunctions to immunotherapy. Nat. Rev. Immunol. 2013, 13, 862–874. Available online: http://www.ncbi.nlm.nih.gov/pubmed/24232462 (accessed on 20 October 2014). [CrossRef] [Green Version]
- Rubio, I.; Osuchowski, M.F.; Shankar-Hari, M.; Skirecki, T.; Winkler, M.S.; Lachmann, G.; la Rosée, P.; Monneret, G.; Venet, F.; Bauer, M.; et al. Current gaps in sepsis immunology: New opportunities for translational research. Lancet Infect. Dis. 2019, 19, e422–e436. [Google Scholar] [CrossRef]
- Rynda-Apple, A.; Robinson, K.M.; Alcorn, J.F. Influenza and Bacterial Superinfection: Illuminating the Immunologic Mechanisms of Disease. Infect. Immun 2015, 83, 3764–3770. [Google Scholar] [CrossRef]
- Siopi, M.; Antonopoulou, S.; Mantzana, P.; Georgiou, P.-C.; Vourli, S.; Protonotariou, E.; Vagiakou, E.; Skoura, L.; Pournaras, S.; Meletiadis, J. Can bronchial secretion cultures identify the etiologic agent of COVID-19-associated pulmonary aspergillosis in ICU patients? Comparison with a species-specific Aspergillus PCR in serum. Med. Mycol. 2022, 61, myac094. [Google Scholar] [CrossRef] [PubMed]
- Armstrong-James, D.; Youngs, J.; Bicanic, T.; Abdolrasouli, A.; Denning, D.W.; Johnson, E.; Mehra, V.; Pagliuca, T.; Patel, B.; Rhodes, J.; et al. Confronting and mitigating the risk of COVID-19 associated pulmonary aspergillosis. Eur. Respir. J. 2020, 56, 2002554. [Google Scholar] [CrossRef] [PubMed]
- White, P.L.; Springer, J.; Wise, M.P.; Einsele, H.; Löffler, C.; Seif, M.; Prommersberger, S.; Backx, M.; Löffler, J. A Clinical Case of COVID-19-Associated Pulmonary Aspergillosis (CAPA), Illustrating the Challenges in Diagnosis (Despite Overwhelming Mycological Evidence). J. Fungi 2022, 8, 81. [Google Scholar] [CrossRef] [PubMed]
- Blot, S.I.; Taccone, F.S.; van den Abeele, A.-M.; Bulpa, P.; Meersseman, W.; Brusselaers, N.; Dimopoulos, G.; Paiva, J.A.; Misset, B.; Rello, J.; et al. A Clinical Algorithm to Diagnose Invasive Pulmonary Aspergillosis in Critically Ill Patients. Am. J. Respir. Crit. Care Med. 2012, 186, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Gangneux, J.-P.; Dannaoui, E.; Fekkar, A.; Luyt, C.-E.; Botterel, F.; de Prost, N.; Tadié, J.-M.; Reizine, F.; Houzé, S.; Timsit, J.-F.; et al. Fungal infections in mechanically ventilated patients with COVID-19 during the first wave: The French multicentre MYCOVID study. Lancet Respir. Med. 2022, 10, 180–190. [Google Scholar] [CrossRef]
- Rouzé, A.; Lemaitre, E.; Martin-Loeches, I.; Povoa, P.; Diaz, E.; Nyga, R.; Torres, A.; Metzelard, M.; du Cheyron, D.; Lambiotte, F.; et al. Invasive pulmonary aspergillosis among intubated patients with SARS-CoV-2 or influenza pneumonia: A European multicenter comparative cohort study. Crit. Care 2022, 26, 11. [Google Scholar] [CrossRef]
- Nyga, R.; Maizel, J.; Nseir, S.; Chouaki, T.; Milic, I.; Roger, P.-A.; van Grunderbeeck, N.; Lemyze, M.; Totet, A.; Castelain, S.; et al. Invasive Tracheobronchial Aspergillosis in Critically Ill Patients with Severe Influenza. A Clinical Trial. Am. J. Respir. Crit. Care Med. 2020, 202, 708–716. [Google Scholar] [CrossRef]
- Bellmann, R.; Smuszkiewicz, P. Pharmacokinetics of antifungal drugs: Practical implications for optimized treatment of patients. Infection 2017, 45, 737–779. [Google Scholar] [CrossRef]
- Keane, S.; Geoghegan, P.; Povoa, P.; Nseir, S.; Rodriguez, A.; Martin-Loeches, I. Systematic review on the first line treatment of amphotericin B in critically ill adults with candidemia or invasive candidiasis. Expert Rev. Anti-Infect. Ther. 2018, 16, 839–847. Available online: http://www.ncbi.nlm.nih.gov/pubmed/30257597 (accessed on 17 January 2023). [CrossRef]
- Lewis, J.S.; Wiederhold, N.P.; Hakki, M.; Thompson, G.R. New Perspectives on Antimicrobial Agents: Isavuconazole. Antimicrob. Agents Chemother. 2022, 66, e00177-22. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Various Definitions Used: EORTC/MSGERC; AspICU; ECMM/ISHAM |
|---|
| During the ‘first wave’ in early 2020 bronchoscopy was considered contraindicated in many centres, which probably led to under-reporting. |
| Criteria for defining CAPA relies on mycology, which may result in over-reporting. |
| Treatment modalities are evolving, which may impact on risk and incidence. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaragoza, R.; Sole-Violan, J.; Cusack, R.; Rodriguez, A.; Reyes, L.F.; Martin-Loeches, I. Invasive Pulmonary Aspergillosis: Not Only a Disease Affecting Immunosuppressed Patients. Diagnostics 2023, 13, 440. https://doi.org/10.3390/diagnostics13030440
Zaragoza R, Sole-Violan J, Cusack R, Rodriguez A, Reyes LF, Martin-Loeches I. Invasive Pulmonary Aspergillosis: Not Only a Disease Affecting Immunosuppressed Patients. Diagnostics. 2023; 13(3):440. https://doi.org/10.3390/diagnostics13030440
Chicago/Turabian StyleZaragoza, Rafael, Jordi Sole-Violan, Rachel Cusack, Alejandro Rodriguez, Luis Felipe Reyes, and Ignacio Martin-Loeches. 2023. "Invasive Pulmonary Aspergillosis: Not Only a Disease Affecting Immunosuppressed Patients" Diagnostics 13, no. 3: 440. https://doi.org/10.3390/diagnostics13030440