
A Laboratory-Based Study on Multiple Biomarker Testing in the Diagnosis of COVID-19-Associated Pulmonary Aspergillosis (CAPA): Real-Life Data
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Flörl, C.; Lewis, R.E.; Munoz, P.; Verweij, P.E.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 2018, 24, E1–E38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, C.C.; Yu, W.L. COVID-19 associated with pulmonary aspergillosis: A literature review. J. Microbiol. Immunol. Infect. 2021, 54, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Prattes, J.; Wauters, J.; Giacobbe, D.R.; Salmanton-Garcia, J.; Maertens, J.; Bourgeois, M.; Reynders, M.; Rutsaert, L.; Van Regenmortel, N.; Lormans, P.; et al. Risk factors and outcome of pulmonary aspergillosis in critically ill coronavirus disease 2019 patients-a multinational observational study by the European Confederation of Medical Mycology. Clin. Microbiol. Infect. 2021, 28, 580–587. [Google Scholar] [CrossRef]
- Lackner, N.; Thome, C.; Ofner, D.; Joannidis, M.; Mayerhofer, T.; Arora, R.; Samardzic, E.; Posch, W.; Breitkopf, R.; Lass-Florl, C. COVID-19 associated pulmonary aspergillosis: Diagnostic performance, fungal epidemiology and antifungal susceptibility. J. Fungi 2022, 8, 93. [Google Scholar] [CrossRef]
- Verweij, P.E.; Bruggemann, R.J.M.; Azoulay, E.; Bassetti, M.; Blot, S.; Buil, J.B.; Calandra, T.; Chiller, T.; Clancy, C.J.; Cornely, O.A.; et al. Taskforce report on the diagnosis and clinical management of COVID-19 associated pulmonary aspergillosis. Intensive Care Med. 2021, 47, 819–834. [Google Scholar] [CrossRef]
- Kariyawasam, R.M.; Dingle, T.C.; Kula, B.E.; Vandermeer, B.; Sligl, W.I.; Schwartz, I.S. Defining COVID-19-associated pulmonary aspergillosis: Systematic review and meta-analysis. Clin. Microbiol. Infect. 2022, 28, 920–927. [Google Scholar] [CrossRef]
- Muthu, V.; Agarwal, R.; Patel, A.; Kathirvel, S.; Abraham, O.C.; Aggarwal, A.N.; Bal, A.; Bhalla, A.S.; Chhajed, P.N.; Chaudhry, D.; et al. Definition, diagnosis, and management of COVID-19-associated pulmonary mucormycosis: Delphi consensus statement from the Fungal Infection Study Forum and Academy of Pulmonary Sciences, India. Lancet Infect. Dis. 2022, 22, e240–e253. [Google Scholar] [CrossRef] [PubMed]
- Koehler, P.; Bassetti, M.; Chakrabarti, A.; Chen, S.C.A.; Colombo, A.L.; Hoenigl, M.; Klimko, N.; Lass-Florl, C.; Oladele, R.O.; Vinh, D.C.; et al. Defining and managing COVID-19-associated pulmonary aspergillosis: The 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect. Dis. 2021, 21, e149–e162. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Bassetti, M.; Giacobbe, D.R.; Grecchi, C.; Rebuffi, C.; Zuccaro, V.; Scudeller, L.; Investigators, F. Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, adult patients: A systematic review with qualitative evidence synthesis. J. Infect. 2020, 81, 131–146. [Google Scholar] [CrossRef]
- Vandewoude, K.H.; Blot, S.I.; Depuydt, P.; Benoit, D.; Temmerman, W.; Colardyn, F.; Vogelaers, D. Clinical relevance of Aspergillus isolation from respiratory tract samples in critically ill patients. Crit. Care 2006, 10, R31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lass-Florl, C.; Mutschlechner, W.; Aigner, M.; Grif, K.; Marth, C.; Girschikofsky, M.; Grander, W.; Greil, R.; Russ, G.; Cerkl, P.; et al. Utility of PCR in diagnosis of invasive fungal infections: Real-life data from a multicenter study. J. Clin. Microbiol. 2013, 51, 863–868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arastehfar, A.; Carvalho, A.; Houbraken, J.; Lombardi, L.; Garcia-Rubio, R.; Jenks, J.D.; Rivero-Menendez, O.; Aljohani, R.; Jacobsen, I.D.; Berman, J.; et al. Aspergillus fumigatus and aspergillosis: From basics to clinics. Stud. Mycol. 2021, 100, 100115. [Google Scholar] [CrossRef]
- Borman, A.M.; Palmer, M.D.; Fraser, M.; Patterson, Z.; Mann, C.; Oliver, D.; Linton, C.J.; Gough, M.; Brown, P.; Dzietczyk, A.; et al. COVID-19-associated invasive aspergillosis: Data from the UK National Mycology Reference Laboratory. J. Clin. Microbiol. 2021, 59, e02136-20. [Google Scholar] [CrossRef] [PubMed]
- Paulussen, C.; Hallsworth, J.E.; Alvarez-Perez, S.; Nierman, W.C.; Hamill, P.G.; Blain, D.; Rediers, H.; Lievens, B. Ecology of aspergillosis: Insights into the pathogenic potency of Aspergillus fumigatus and some other Aspergillus species. Microb. Biotechnol. 2017, 10, 296–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lass-Flörl, C. How to make a fast diagnosis in invasive aspergillosis. Med. Mycol. 2019, 57, S155–S160. [Google Scholar] [CrossRef]
- Delliere, S.; Dudoignon, E.; Voicu, S.; Collet, M.; Fodil, S.; Plaud, B.; Chousterman, B.; Bretagne, S.; Azoulay, E.; Mebazaa, A.; et al. Combination of mycological criteria: A better surrogate to identify COVID-19-associated pulmonary aspergillosis patients and evaluate prognosis? J. Clin. Microbiol. 2022, 60, e02169-21. [Google Scholar] [CrossRef] [PubMed]
- Blot, S.I.; Taccone, F.S.; Van den Abeele, A.M.; Bulpa, P.; Meersseman, W.; Brusselaers, N.; Dimopoulos, G.; Paiva, J.A.; Misset, B.; Rello, J.; et al. A clinical algorithm to diagnose invasive pulmonary aspergillosis in critically ill patients. Am. J. Resp. Crit. Care 2012, 186, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Rouze, A.; Lemaitre, E.; Martin-Loeches, I.; Povoa, P.; Diaz, E.; Nyga, R.; Torres, A.; Metzelard, M.; Du Cheyron, D.; Lambiotte, F.; et al. Invasive pulmonary aspergillosis among intubated patients with SARS-CoV-2 or influenza pneumonia: A European multicenter comparative cohort study. Crit. Care 2022, 26, 11. [Google Scholar] [CrossRef]
- Aigner, M.; Wanner, M.; Kreidl, P.; Lass-Florl, C.; Lackner, M. Candida in the respiratory tract potentially triggers galactomannan positivity in nonhematological patients. Antimicrob. Agents Chemother. 2019, 63, e00138-19. [Google Scholar] [CrossRef]
- Tavakoli, M.; Shokohi, T.; Lass Florl, C.; Hedayati, M.T.; Hoenigl, M. Immunological response to COVID-19 and its role as a predisposing factor in invasive aspergillosis. Curr. Med. Mycol. 2020, 6, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Lass-Flörl, C.; Samardzic, E.; Knoll, M. Serology anno 2021-fungal infections: From invasive to chronic. Clin. Microbiol. Infect. 2021, 27, 1230–1241. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Tests | Results | No. of Specimens and Microscopy | Sen | CI | Spec | CI | PPV | CI | NPV | CI | LR+ | CI | LR− | CI | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| + | − | ||||||||||||||
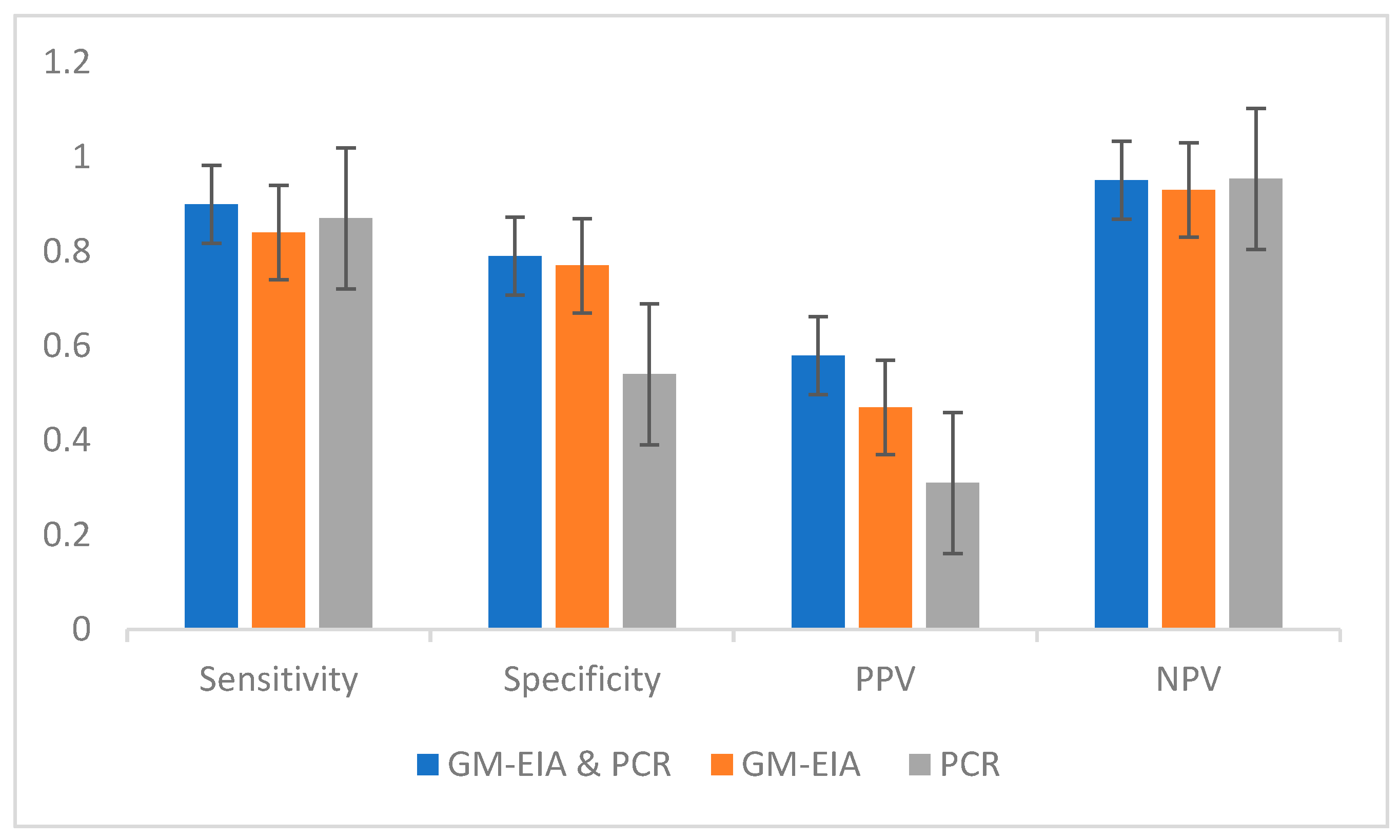
| GM-EIA/PCR | +/+ | 27 | 19 | 0.9 | 0.84–0.95 | 0.77 | 0.72–0.81 | 0.58 | 0.51–0.66 | 0.95 | 0.92–0.98 | 3.9 | 3.16–4.88 | 0.12 | 0.07–0.22 |
| −/− | 3 | 64 | |||||||||||||
| GM-EIA/PCR | +/− | 1 | 12 | These results fall out of the analysis illustrated above, as are either positive or negative in GM-EIA or Aspergillus PCR. | |||||||||||
| GM-EIA/PCR | −/+ | 2 | 44 | ||||||||||||
| Single GM-EIA | + | 28 | 31 | 0.84 | 0.78–0.91 | 0.77 | 0.74–0.81 | 0.47 | 0.40–0.54 | 0.95 | 0.93–0.97 | 3.8 | 3.17–4.55 | 0.19 | 0.12–0.29 |
| Single GM-EIA | − | 5 | 108 | ||||||||||||
| Single PCR | + | 29 | 63 | 0.87 | 0.81–0.93 | 0.54 | 0.50–0.59 | 0.31 | 0.26–0.36 | 0.95 | 0.92–0.97 | 1.93 | 1.72–2.18 | 0.22 | 0.13–0.36 |
| Single PCR | − | 4 | 76 | ||||||||||||
| GM-EIA & PCR | No. (%) of Specimens and Microscopic Examination | Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value | |
|---|---|---|---|---|---|---|
| + | − | |||||
| +/+ | 0 | 7 (10.1) | NA | 0.80 | NA | 100 |
| −/− | 0 | 42 (60.8) | ||||
| +/− | 2 (2.8) | 12 (17.3) | All specimens investigated showed a high frequency of yeasts detected by culture. C. albicans and C. glabrata were the dominant species involved. | |||
| −/+ | 2 (2.8) | 4 (4.4) | ||||
| Culture-Positive Species | No. | PCR-Positive Specimens | No. |
|---|---|---|---|
| A. fumigatus species complex (s.p) | 85 | A. fumigatus s.c | 66 |
| A. terreus s.c | 53 | A. terreus s.c | 30 |
| A. flavus s.c | 12 | A. flavus s.c | 6 |
| A. nidulans s.c | 6 | A. niger s.c | 3 |
| A. fumigatus s.c and A. terreus s.c | 5 | ||
| A. niger s.c | 5 | ||
| A. niger s.c and A. flavus s.c | 4 | ||
| A. glaucus s.c | 1 | ||
| A. versicolor s.c | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lass-Flörl, C.; Knoll, M.; Posch, W.; Joannidis, M.; Mayerhöfer, T.; Breitkopf, R.; Bellmann, R. A Laboratory-Based Study on Multiple Biomarker Testing in the Diagnosis of COVID-19-Associated Pulmonary Aspergillosis (CAPA): Real-Life Data. Diagnostics 2023, 13, 114. https://doi.org/10.3390/diagnostics13010114
Lass-Flörl C, Knoll M, Posch W, Joannidis M, Mayerhöfer T, Breitkopf R, Bellmann R. A Laboratory-Based Study on Multiple Biomarker Testing in the Diagnosis of COVID-19-Associated Pulmonary Aspergillosis (CAPA): Real-Life Data. Diagnostics. 2023; 13(1):114. https://doi.org/10.3390/diagnostics13010114
Chicago/Turabian StyleLass-Flörl, Cornelia, Miriam Knoll, Wilfried Posch, Michael Joannidis, Timo Mayerhöfer, Robert Breitkopf, and Romuald Bellmann. 2023. "A Laboratory-Based Study on Multiple Biomarker Testing in the Diagnosis of COVID-19-Associated Pulmonary Aspergillosis (CAPA): Real-Life Data" Diagnostics 13, no. 1: 114. https://doi.org/10.3390/diagnostics13010114