
Diagnostic Performance of Ovarian Morphology on Ultrasonography across Anovulatory Conditions—Impact of Body Mass Index
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Ethical Considerations
2.3. Clinical Assessments
2.4. Ultrasonography
2.5. Biochemical Assays
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Participants across Reproductive Phenotypes
3.2. Diagnostic Potential of Ovarian Morphology across Reproductive Phenotypes
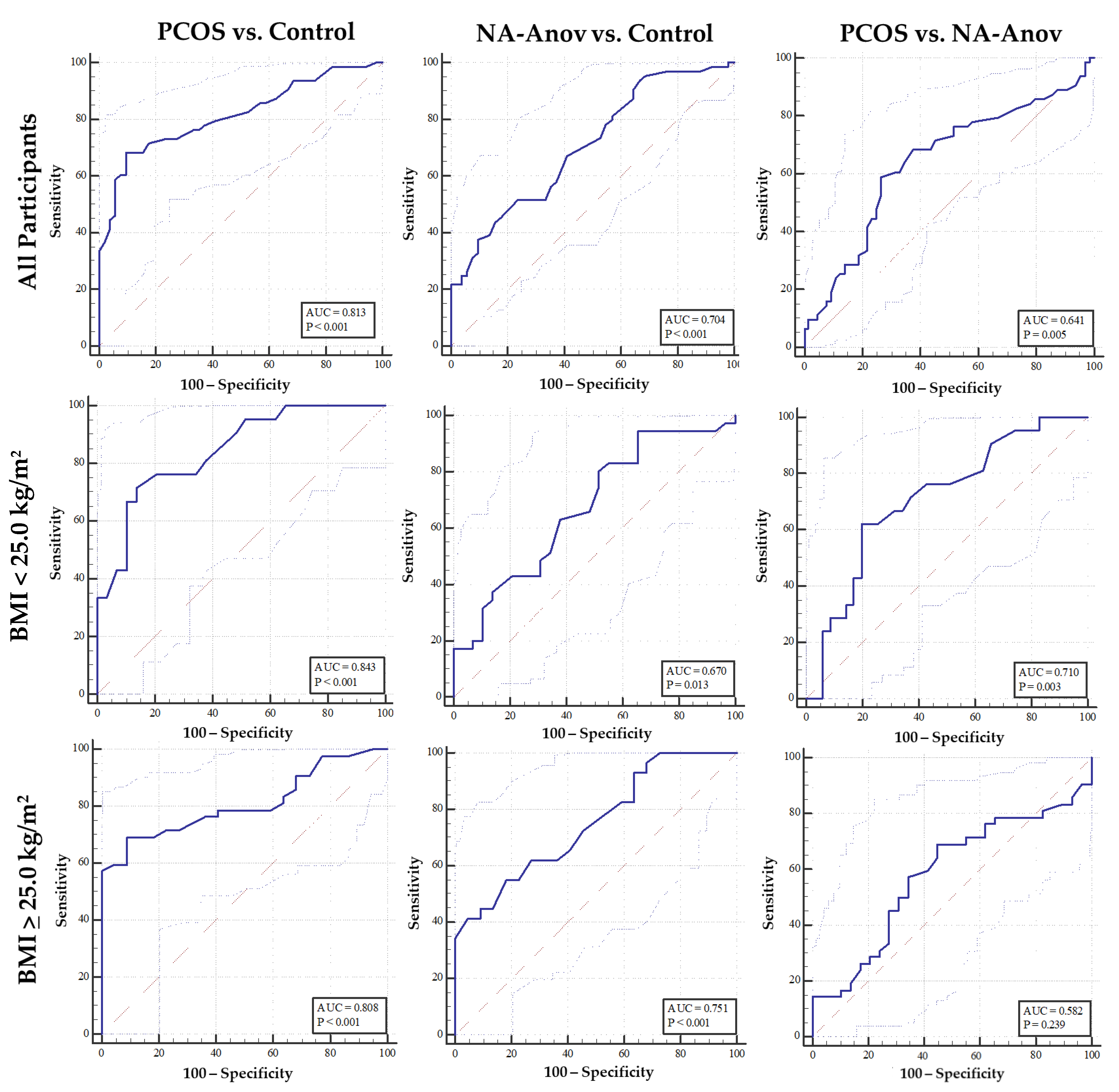
3.3. Impact of Body Mass Index on Diagnostic Potential of Ovarian Morphology across Reproductive Phenotypes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum. Reprod. 2018, 33, 1602–1618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewailly, D.; Lujan, M.E.; Carmina, E.; Cedars, M.I.; Laven, J.; Norman, R.J.; Escobar-Morreale, H. Definition and significance of polycystic ovarian morphology: A task force report from the Androgen Excess and Polycystic Ovary Syndrome Society. Hum. Reprod. Updat. 2013, 20, 334–352. [Google Scholar] [CrossRef] [PubMed]
- Welt, C.K.; Gudmundsson, J.A.; Arason, G.; Adams, J.; Palsdottir, H.; Gudlaugsdottir, G.; Ingadottir, G.; Crowley, W.F. Characterizing Discrete Subsets of Polycystic Ovary Syndrome as Defined by the Rotterdam Criteria: The Impact of Weight on Phenotype and Metabolic Features. J. Clin. Endocrinol. Metab. 2006, 91, 4842–4848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barber, T.M.; Wass, J.A.H.; McCarthy, M.; Franks, S. Metabolic characteristics of women with polycystic ovaries and oligo-amenorrhoea but normal androgen levels: Implications for the management of polycystic ovary syndrome. Clin. Endocrinol. 2007, 66, 513–517. [Google Scholar] [CrossRef] [PubMed]
- Carmina, E.; Chu, M.C.; Longo, R.A.; Rini, G.B.; Lobo, R.A. Phenotypic Variation in Hyperandrogenic Women Influences the Findings of Abnormal Metabolic and Cardiovascular Risk Parameters. J. Clin. Endocrinol. Metab. 2005, 90, 2545–2549. [Google Scholar] [CrossRef]
- Guastella, E.; Longo, R.A.; Carmina, E. Clinical and endocrine characteristics of the main polycystic ovary syndrome phenotypes. Fertil. Steril. 2010, 94, 2197–2201. [Google Scholar] [CrossRef]
- Shroff, R.; Syrop, C.H.; Davis, W.; Van Voorhis, B.J.; Dokras, A. Risk of metabolic complications in the new PCOS phenotypes based on the Rotterdam criteria. Fertil. Steril. 2007, 88, 1389–1395. [Google Scholar] [CrossRef]
- Daan, N.M.; Louwers, Y.V.; Koster, M.P.; Eijkemans, M.J.; de Rijke, Y.B.; Lentjes, E.W.; Fauser, B.C.; Laven, J.S. Cardiovascular and metabolic profiles amongst different polycystic ovary syndrome phenotypes: Who is really at risk? Fertil. Steril. 2014, 102, 1444–1451.e3. [Google Scholar] [CrossRef]
- Huddleston, H.G.; Quinn, M.M.; Kao, C.-N.; Lenhart, N.; Rosen, M.P.; Cedars, M.I. Women with polycystic ovary syndrome demonstrate worsening markers of cardiovascular risk over the short-term despite declining hyperandrogenaemia: Results of a longitudinal study with community controls. Clin. Endocrinol. 2017, 87, 775–782. [Google Scholar] [CrossRef]
- Broekmans, F.J.; Knauff, E.A.H.; Valkenburg, O.; Laven, J.S.; Eijkemans, M.J.; Fauser, B.C.J.M. PCOS according to the Rotterdam consensus criteria: Change in prevalence among WHO-II anovulation and association with metabolic factors. BJOG Int. J. Obstet. Gynaecol. 2006, 113, 1210–1217. [Google Scholar] [CrossRef]
- Chen, M.-J.; Yang, W.-S.; Chen, C.-L.; Wu, M.-Y.; Yang, Y.-S.; Ho, H.-N. The relationship between anti-Mullerian hormone, androgen and insulin resistance on the number of antral follicles in women with polycystic ovary syndrome. Hum. Reprod. 2008, 23, 952–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jonard, S.; Robert, Y.; Cortet-Rudelli, C.; Pigny, P.; Decanter, C.; Dewailly, D. Ultrasound examination of polycystic ovaries: Is it worth counting the follicles? Hum. Reprod. 2003, 18, 598–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balen, A.H.; Conway, G.S.; Kaltsas, G.; Techatraisak, K.; Manning, P.J.; West, C.; Jacobs, H.S. Andrology: Polycystic ovary syndrome: The spectrum of the disorder in 1741 patients. Hum. Reprod. 1995, 10, 2107–2111. [Google Scholar] [CrossRef]
- Hahn, S.; van Halteren, W.B.; Roesler, S.; Schmidt, M.; Kimmig, R.; Tan, S.; Mann, K.; Janssen, O. The Combination of Increased Ovarian Volume and Follicle Number is Associated with More Severe Hyperandrogenism in German Women with Polycystic Ovary Syndrome. Exp. Clin. Endocrinol. Diabetes 2006, 114, 175–181. [Google Scholar] [CrossRef]
- Christ, J.P.; Brink, H.V.; Brooks, E.D.; Pierson, R.A.; Chizen, D.R.; Lujan, M.E. Ultrasound features of polycystic ovaries relate to degree of reproductive and metabolic disturbance in polycystic ovary syndrome. Fertil. Steril. 2015, 103, 787–794. [Google Scholar] [CrossRef]
- Rosner, W.; Auchus, R.J.; Azziz, R.; Sluss, P.M.; Raff, H. Utility, Limitations, and Pitfalls in Measuring Testosterone: An Endocrine Society Position Statement. J. Clin. Endocrinol. Metab. 2006, 92, 405–413. [Google Scholar] [CrossRef]
- Rosner, W.; Vesper, H. Toward Excellence in Testosterone Testing: A Consensus Statement. J. Clin. Endocrinol. Metab. 2010, 95, 4542–4548. [Google Scholar] [CrossRef]
- Vanden Brink, H.; Pea, J.; Lujan, M.E. Ultrasonographic features of ovarian morphology capture nutritional and metabolic influences on the reproductive axis: Implications for biomarker development in ovulatory disorders. Curr. Opin. Biotechnol. 2021, 70, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Reid, S.P.; Kao, C.-N.; Pasch, L.; Shinkai, K.; Cedars, M.I.; Huddleston, H.G. Ovarian morphology is associated with insulin resistance in women with polycystic ovary syndrome: A cross sectional study. Fertil. Res. Pract. 2017, 3, 8. [Google Scholar] [CrossRef] [Green Version]
- Alviggi, C.; Conforti, A.; De Rosa, P.; Strina, I.; Palomba, S.; Vallone, R.; Gizzo, S.; Borrelli, R.; Andersen, C.Y.; De Placido, G.; et al. The Distribution of Stroma and Antral Follicles Differs between Insulin-Resistance and Hyperandrogenism-Related Polycystic Ovarian Syndrome. Front. Endocrinol. 2017, 8, 117. [Google Scholar] [CrossRef]
- Fulghesu, A.M.; Villa, P.; Pavone, V.; Guido, M.; Apa, R.; Caruso, A.; Lanzone, A.; Rossodivita, A.; Mancuso, S. The Impact of Insulin Secretion on the Ovarian Response to Exogenous Gonadotropins in Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 1997, 82, 644–648. [Google Scholar] [CrossRef] [PubMed]
- Bishop, C.V.; Mishler, E.C.; Takahashi, D.L.; Reiter, T.E.; Bond, K.R.; True, C.A.; Slayden, O.D.; Stouffer, R.L. Chronic hyperandrogenemia in the presence and absence of a western-style diet impairs ovarian and uterine structure/function in young adult rhesus monkeys. Hum. Reprod. 2017, 33, 128–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, N.; Luo, L.-L.; Xu, J.-J.; Xu, M.-Y.; Zhang, X.-M.; Zhou, X.-L.; Liu, W.-J.; Fu, Y.-C. Obesity accelerates ovarian follicle development and follicle loss in rats. Metabolism 2013, 63, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; McGee, W.K.; Bishop, C.; Park, B.S.; Cameron, J.L.; Zelinski, M.; Stouffer, R.L. Exposure of Female Macaques to Western-Style Diet With or Without Chronic T In Vivo Alters Secondary Follicle Function During Encapsulated 3-Dimensional Culture. Endocrinology 2015, 156, 1133–1142. [Google Scholar] [CrossRef] [Green Version]
- Hanley, J.A.; McNeil, B.J. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982, 143, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Hatch, R.; Rosenfield, R.L.; Kim, M.H.; Tredway, D. Hirsutism: Implications, etiology, and management. Am. J. Obstet. Gynecol. 1981, 140, 815–830. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Yeckel, C.W.; Weiss, R.; Dziura, J.; Taksali, S.E.; Dufour, S.; Burgert, T.S.; Tamborlane, W.V.; Caprio, S. Validation of Insulin Sensitivity Indices from Oral Glucose Tolerance Test Parameters in Obese Children and Adolescents. J. Clin. Endocrinol. Metab. 2004, 89, 1096–1101. [Google Scholar] [CrossRef] [Green Version]
- Lujan, M.E.; Brooks, E.D.; Kepley, A.L.; Chizen, D.R.; Pierson, R.; Peppin, A.K. Grid Analysis Improves Reliability in Follicle Counts Made by Ultrasonography in Women With Polycystic Ovary Syndrome. Ultrasound Med. Biol. 2010, 36, 712–718. [Google Scholar] [CrossRef] [Green Version]
- Vermeulen, A.; Verdonck, L.; Kaufman, J.M. A Critical Evaluation of Simple Methods for the Estimation of Free Testosterone in Serum. J. Clin. Endocrinol. Metab. 1999, 84, 3666–3672. [Google Scholar] [CrossRef]
- Lujan, M.E.; Jarrett, B.Y.; Brooks, E.D.; Reines, J.K.; Peppin, A.K.; Muhn, N.; Haider, E.; Pierson, R.; Chizen, D.R. Updated ultrasound criteria for polycystic ovary syndrome: Reliable thresholds for elevated follicle population and ovarian volume. Hum. Reprod. 2013, 28, 1361–1368. [Google Scholar] [CrossRef]
- Allemand, C.M.; Tummon, I.S.; Phy, J.L.; Foong, S.C.; Dumesic, D.A.; Session, D.R. Diagnosis of polycystic ovaries by three-dimensional transvaginal ultrasound. Fertil Steril. 2006, 85, 214–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenfield, R.L. The Polycystic Ovary Morphology-Polycystic Ovary Syndrome Spectrum. J. Pediatr. Adolesc. Gynecol. 2014, 28, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanden Brink, H.; Willis, A.D.; Jarrett, B.Y.; Lin, A.W.; Soler, S.; Best, S.; Bender, E.L.; Peppin, A.K.; Hoeger, K.M.; Lujan, M.E. Sonographic markers of ovarian morphology, but not hirsutism indices, predict serum total testosterone in women with regular menstrual cycles. Fertil. Steril. 2016, 105, 1322–1329.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karrer-Voegeli, S.; Rey, F.; Reymond, M.J.; Meuwly, J.-Y.; Gaillard, R.C.; Gomez, F. Androgen Dependence of Hirsutism, Acne, and Alopecia in Women: Retrospective analysis of 228 patients investigated for hyperandrogenism. Medicine 2009, 88, 32–45. [Google Scholar] [CrossRef] [PubMed]
- Christ, J.P.; Willis, A.D.; Brooks, E.D.; Vanden Brink, H.; Jarrett, B.Y.; Pierson, R.A.; Chizen, D.R.; Lujan, M.E. Follicle number, not assessments of the ovarian stroma, represents the best ultrasonographic marker of polycystic ovary syndrome. Fertil. Steril. 2013, 101, 280–287.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobo, R.A.; Goebelsmann, U.; Horton, R. Evidence for the Importance of Peripheral Tissue Events in the Development of Hirsutism in Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 1983, 57, 393–397. [Google Scholar] [CrossRef]
- Dewailly, D.; Gronier, H.; Poncelet, E.; Robin, G.; Leroy, M.; Pigny, P.; Duhamel, A.; Catteau-Jonard, S. Diagnosis of polycystic ovary syndrome (PCOS): Revisiting the threshold values of follicle count on ultrasound and of the serum AMH level for the definition of polycystic ovaries. Hum. Reprod. 2011, 26, 3123–3129. [Google Scholar] [CrossRef] [Green Version]
- Carmina, E.; Campagna, A.M.; Fruzzetti, F.; Lobo, R.A. Amh Measurement Versus Ovarian Ultrasound In The Diagnosis of Polycystic Ovary Syndrome in Different Phenotypes. Endocr. Pract. 2016, 22, 287–293. [Google Scholar] [CrossRef]
- Chen, Y.; Li, L.; Chen, X.; Zhang, Q.; Wang, W.; Li, Y.; Yang, D. Ovarian volume and follicle number in the diagnosis of polycystic ovary syndrome in Chinese women. Ultrasound Obstet. Gynecol. 2008, 32, 700–703. [Google Scholar] [CrossRef]
- Carmina, E.; Fruzzetti, F.; Lobo, R.A. Increased anti-Mullerian hormone levels and ovarian size in a subgroup of women with functional hypothalamic amenorrhea: Further identification of the link between polycystic ovary syndrome and functional hypothalamic amenorrhea. Am. J. Obstet. Gynecol. 2016, 214, 714.e1–714.e6. [Google Scholar] [CrossRef]
- Pache, T.D.; Wladimiroff, J.W.; Hop, W.C.; Fauser, B.C. How to discriminate between normal and polycystic ovaries: Transvaginal US study. Radiology 1992, 183, 421–423. [Google Scholar] [CrossRef]
- Atiomo, W.; Pearson, S.; Shaw, S.; Prentice, A.; Dubbins, P. Ultrasound criteria in the diagnosis of polycystic ovary syn-drome (PCOS). Ultrasound Med. Biol. 2000, 26, 977–980. [Google Scholar] [CrossRef]
- Jonard, S.; Robert, Y.; Dewailly, D. Revisiting the ovarian volume as a diagnostic criterion for polycystic ovaries. Hum. Reprod. 2005, 20, 2893–2898. [Google Scholar] [CrossRef] [Green Version]
- Fong, S.L.; Laven, J.S.E.; Duhamel, A.; Dewailly, D. Polycystic ovarian morphology and the diagnosis of polycystic ovary syndrome: Redefining threshold levels for follicle count and serum anti-Müllerian hormone using cluster analysis. Hum. Reprod. 2017, 32, 1723–1731. [Google Scholar] [CrossRef]
- McGee, W.K.; Bishop, C.V.; Pohl, C.R.; Chang, R.J.; Marshall, J.C.; Pau, F.K.; Stouffer, R.L.; Cameron, J.L. Effects of hyperandrogenemia and increased adiposity on reproductive and metabolic parameters in young adult female monkeys. Am. J. Physiol. Metab. 2014, 306, E1292–E1304. [Google Scholar] [CrossRef] [Green Version]
- Nteeba, J.; Ganesan, S.; Keating, A.F. Progressive Obesity Alters Ovarian Folliculogenesis with Impacts on Pro-Inflammatory and Steroidogenic Signaling in Female Mice1. Biol. Reprod. 2014, 91, 86. [Google Scholar] [CrossRef]
- Gaspar, R.S.; Benevides, R.O.A.; Fontelles, J.L.D.L.; Vale, C.C.; França, L.M.; Barros, P.D.T.S.; Paes, A.M.D.A. Reproductive alterations in hyperinsulinemic but normoandrogenic MSG obese female rats. J. Endocrinol. 2016, 229, 61–72. [Google Scholar] [CrossRef] [Green Version]
- Bazzano, M.; Torelli, C.; Pustovrh, M.; Paz, D.; Elia, E. Obesity induced by cafeteria diet disrupts fertility in the rat by affecting multiple ovarian targets. Reprod. Biomed. Online 2015, 31, 655–667. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Woods, K.S.; Bartolucci, A.A.; Azziz, R. Prevalence of adrenal androgen excess in patients with the polycystic ovary syndrome (PCOS). Clin. Endocrinol. 2005, 62, 644–649. [Google Scholar] [CrossRef]


{kind=link}
| Controls | NA-Anov | PCOS | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Demographics | ||||||
| N | 51 | 64 | 66 | |||
| Age (y) | 28 | 5.4 a | 26 | 5.4 b | 26 | 5.3 b |
| Age at menarche (y) | 12 | 1.3 | 13 | 1.4 | 13 | 1.8 |
| Ethnicity (N, (%)) | ||||||
| Hispanic or Latino | 6 | (12) | 6 | (9) | 6 | (9) |
| Not Hispanic or Latino | 36 | (70) | 51 | (80) | 55 | (83) |
| Other or Not Reported | 9 | (18) | 7 | (11) | 5 | (8) |
| Race (N, (%)) | ||||||
| White | 33 | (65) | 41 | (64) | 44 | (66) |
| Black or African American | 5 | (10) | 6 | (9) | 8 | (12) |
| Asian | 3 | (5) | 13 | (20) | 7 | (11) |
| Native Hawaiian or Other Pacific Islander | 0 | (0) | 0 | (0) | 0 | (0) |
| More than one race | 5 | (10) | 1 | (2) | 2 | (3) |
| Other or Not Reported | 5 | (10) | 3 | (5) | 5 | (8) |
| Diagnostic Features | ||||||
| Menstrual Cycle Length (d) | 29 | 2.2 a | 72 | 63.8 b | 98 | 105.5 b |
| Hirsutism Score | 3 | 2.1 a | 3 | 1.8 a | 10 | 5.2 b |
| Total T (ng/dL) | 29.0 | 14.47 a | 33.7 | 15.58 a | 52.3 | 27.43 b |
| Metabolic Status | ||||||
| BMI (kg/m2) | 27.1 | 6.7 a | 28.2 | 9.0 a,b | 31.2 | 9.3 b |
| WHR | 0.83 | 0.06 | 0.81 | 0.08 | 0.85 | 0.09 |
| Fasting Glucose (mg/dL) | 94.9 | 9.41 | 92.7 | 9.99 | 96.0 | 12.90 |
| Fasting Insulin (uIU/mL) | 7.8 | 6.11 | 9.5 | 8.27 | 13.9 | 12.63 |
| 2-HR Glucose | 93.5 | 26.43 | 93.4 | 20.22 | 105.0 | 34.61 |
| 2-HR Insulin | 33.4 | 30.75 a | 54.4 | 37.93 b | 83.1 | 87.72 b |
| HOMA-IR | 1.8 | 1.50 | 2.2 | 1.97 | 3.5 | 3.56 |
| WBISI | 10.4 | 6.68 a | 7.9 | 6.34 a,b | 6.2 | 5.39 b |
| Reproductive Endocrinology | ||||||
| LH (mIU/mL) | 4.7 | 2.33 a | 7.6 | 5.15 a,b | 7.9 | 3.48 b |
| FSH (mIU/mL) | 6.5 | 2.20 | 6.0 | 2.06 | 6.1 | 1.73 |
| Estradiol (pg/mL) | 55.7 | 38.55 | 54.9 | 32.96 | 58.3 | 42.25 |
| SHBG (nmol/L) | 56.8 | 25.88 | 57.2 | 42.39 | 42.2 | 25.09 |
| Free T (ng/dL) | 0.4 | 0.19 a | 0.5 | 0.33 a | 0.9 | 0.56 b |
| Bioavailable T (ng/dL) | 8.9 | 4.47 a | 12.1 | 7.68 a | 21.3 | 13.12 b |
| FAI (%) | 2.1 | 1.61 a | 3.1 | 2.59 a | 6.1 | 5.18 b |
| Ovarian Morphology | ||||||
| FNPS | 7 | 3.3 a | 9 | 4.2 b | 10 | 4.4 b |
| FNPO 2–9 mm | 24 | 10.2 a | 35 | 16.5 b | 45 | 24.0 c |
| OV (cm3) | 6 | 2.2 a | 8 | 3.3 b | 10 | 3.5 c |
| Threshold | AUCROC | p Value | Sensitivity (%) | Specificity (%) | |
|---|---|---|---|---|---|
| PCOS vs. Control | |||||
| FNPS | >8 | 0.753 | <0.0001 | 71 (58–82) | 71 (56–83) |
| >9 [31] | 58 (46–71) | 77 (63–87) | |||
| >10 [32] | 48 (35–61) | 86 (74–94) | |||
| FNPO | >35 | 0.813 | <0.0001 | 68 (55–79) | 90 (77–97) |
| >20 [2] | 87 (77–94) | 37 (24–52) | |||
| >25 [1] | 83 (71–91) | 47 (33–62) | |||
| OV (cm3) | >8.2 | 0.830 | <0.0001 | 73 (60–83) | 84 (71–94) |
| >10 [1,31] | 42 (30–55) | 94 (84–99) | |||
| NA-Anov vs. Control | |||||
| FNPS | >8 | 0.685 | <0.0001 | 56 (43–69) | 70 (56–83) |
| >9 | 50 (37–63) | 74 (63–87) | |||
| >10 | 37 (26–51) | 86 (74–94) | |||
| FNPO | >33 | 0.704 | <0.0001 | 44 (31–57) | 84 (71–93) |
| >20 | 86 (75–93) | 37 (24–52) | |||
| >25 | 73 (61–83) | 47 (33–62) | |||
| OV (cm3) | >5.7 | 0.656 | 0.0023 | 75 (63–85) | 55 (40–69) |
| >10 | 17 (9–29) | 94 (84–99) | |||
| PCOS vs. NA-Anov | |||||
| FNPS | >7 | 0.570 | 0.1667 | 78 (67–88) | 38 (26–51) |
| >9 | 58 (46–71) | 50 (37–63) | |||
| >10 | 48 (35–61) | 63 (50–74) | |||
| FNPO | >39 | 0.641 | 0.0051 | 59 (46–71) | 73 (61–84) |
| >20 | 87 (77–94) | 14 (7–25) | |||
| >25 | 83 (71–91) | 27 (16–39) | |||
| OV (cm3) | >8.1 | 0.698 | <0.0001 | 74 (62–84) | 69 (56–80) |
| >10 | 42 (30–55) | 80 (68–89) | |||
| Threshold | AUCROC | p Value | Sensitivity (%) | Specificity(%) | |
|---|---|---|---|---|---|
| HA-PCOS vs. Control | |||||
| FNPS | |||||
| Lean | >7 | 0.806 | <0.001 | 100 (85–100) | 58 (39–77) |
| OW | >10 | 0.762 | <0.001 | 47 (31–62) | 100 (85–100) |
| FNPO | |||||
| Lean | >32 | 0.843 | <0.001 | 71 (48–89) | 87 (69–96) |
| OW | >35 | 0.808 | <0.001 | 69 (53–83) | 91 (71–99) |
| OV | |||||
| Lean | >7.9 | 0.763 | <0.001 | 65 (43–84) | 79 (60–92) |
| OW | >7.1 | 0.885 | <0.001 | 84 (69–93) | 86 (65–97) |
| NA-Anov vs. Control | |||||
| FNPS | |||||
| Lean | >8 | 0.687 | 0.005 | 63 (45–77) | 69 (49–84) |
| OW | >10 | 0.679 | 0.017 | 34 (18–955 | 100 (85–75) |
| FNPO | |||||
| Lean | >16 | 0.670 | 0.013 | 94 (81–99) | 35 (18–55) |
| OW | >33 | 0.751 | <0.001 | 55 (36–74) | 81 (60–95) |
| OV | |||||
| Lean | >5.6 | 0.580 | 0.275 | 69 (51–83) | 55 (36–74) |
| OW | >7.1 | 0.754 | <0.001 | 62 (42–79) | 86 (65–97) |
| HA-PCOS vs. NA-Anov | |||||
| FNPS | |||||
| Lean | >7 | 0.607 | 0.151 | 100 (85–100) | 29 (15–46) |
| OW | >7 | 0.574 | 0.293 | 67 (51–80) | 48 (29–68) |
| FNPO | |||||
| Lean | >39 | 0.710 | 0.003 | 62 (38–82) | 80 (63–92) |
| OW | >34 | 0.582 | 0.239 | 69 (53–82) | 55 (36–74) |
| OV | |||||
| Lean | >8.1 | 0.684 | 0.014 | 65 (43–84) | 77 (60–90) |
| OW | >7.5 | 0.673 | 0.010 | 81 (67–92) | 58 (39–77) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vanden Brink, H.; Jarrett, B.Y.; Pereira, N.; Spandorfer, S.D.; Hoeger, K.M.; Lujan, M.E. Diagnostic Performance of Ovarian Morphology on Ultrasonography across Anovulatory Conditions—Impact of Body Mass Index. Diagnostics 2023, 13, 374. https://doi.org/10.3390/diagnostics13030374
Vanden Brink H, Jarrett BY, Pereira N, Spandorfer SD, Hoeger KM, Lujan ME. Diagnostic Performance of Ovarian Morphology on Ultrasonography across Anovulatory Conditions—Impact of Body Mass Index. Diagnostics. 2023; 13(3):374. https://doi.org/10.3390/diagnostics13030374
Chicago/Turabian StyleVanden Brink, Heidi, Brittany Y. Jarrett, Nigel Pereira, Steven D. Spandorfer, Kathy M. Hoeger, and Marla E. Lujan. 2023. "Diagnostic Performance of Ovarian Morphology on Ultrasonography across Anovulatory Conditions—Impact of Body Mass Index" Diagnostics 13, no. 3: 374. https://doi.org/10.3390/diagnostics13030374