
Polycystic Ovary Syndrome, Subclinical Hypothyroidism, the Cut-Off Value of Thyroid Stimulating Hormone; Is There a Link? Findings of a Population-Based Study

 ,
,
Abstract
:1. Introduction
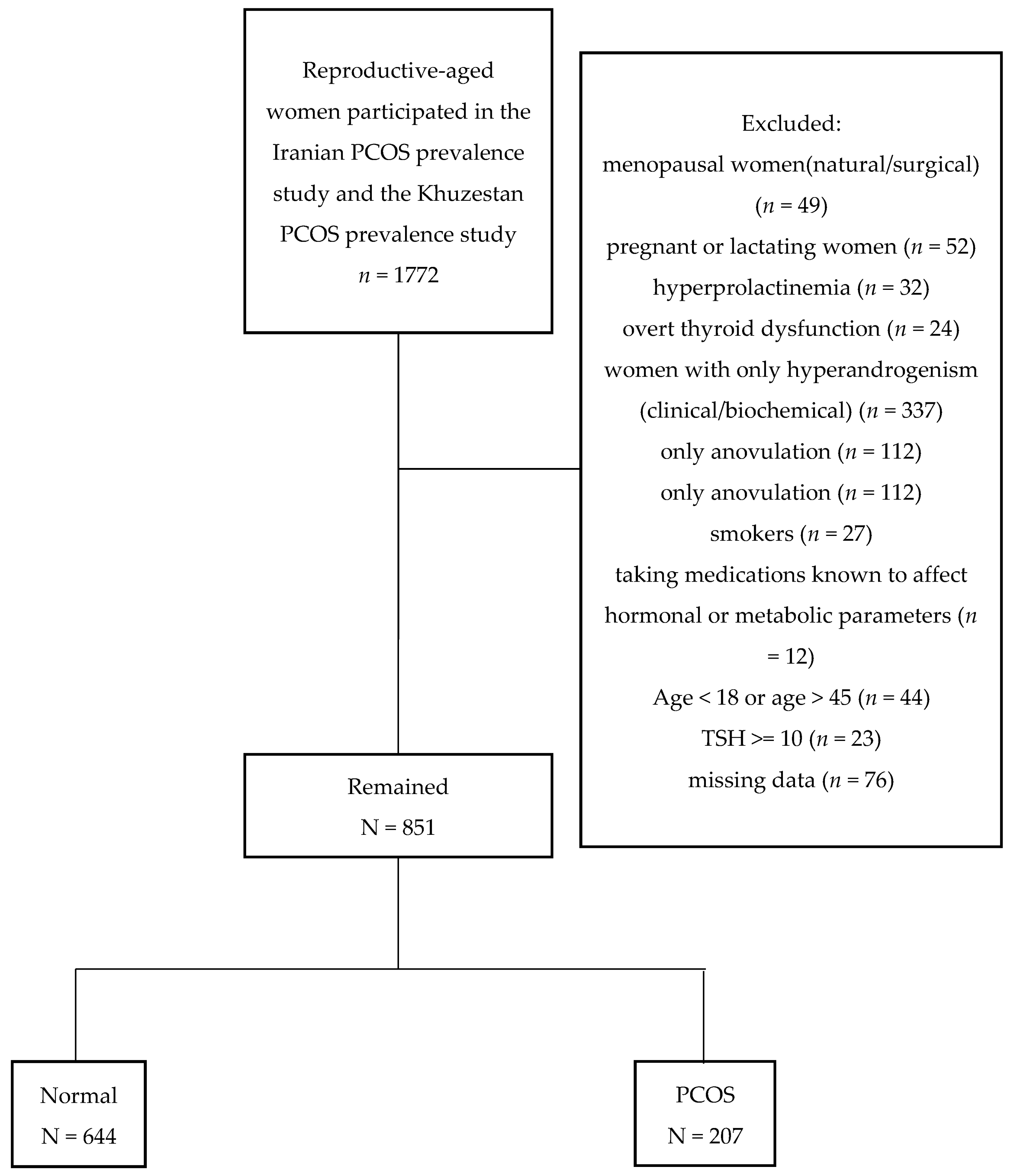
2. Materials and Methods
- PCOS group: Women diagnosed with PCOS based on the Rotterdam criteria (n = 207).
- Control: Those without any feature of PCOS; eumenorrheic not hirsute women without polycystic ovary morphology (PCOM) (n = 644).
2.1. Definitions
2.2. Measurements
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stein, I.F.; Leventhal, M.L. Amenorrhea associated with bilateral polycystic ovaries. Am. J. Obstet. Gynecol. 1935, 29, 181–191. [Google Scholar] [CrossRef]
- Franks, S. Controversy in clinical endocrinology: Diagnosis of polycystic ovarian syndrome: In defense of the Rotterdam criteria. J. Clin. Endocrinol. Metab. 2006, 91, 786–789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil. Steril. 2004, 81, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Szydlarska, D.; Machaj, M.; Jakimiuk, A. History of discovery of polycystic ovary syndrome. Adv. Clin. Exp. Med. 2017, 26, 555–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, P.N.; Albrecht, D.; Scholz, A.; Gutierrez-Buey, G.; Lazarus, J.H.; Dayan, C.M.; Okosieme, O.E. Global epidemiology of hyperthyroidism and hypothyroidism. Nat. Rev. Endocrinol. 2018, 14, 301–316. [Google Scholar] [CrossRef]
- James, S.R.; Franklyn, J.A.; Kilby, M.D. Placental transport of thyroid hormone. Best Pract. Res. Clin. Endocrinol. Metab. 2007, 21, 253–264. [Google Scholar] [CrossRef]
- Maruo, T.; Katayama, K.; Barnea, E.R.; Mochizuki, M. A role for thyroid hormone in the induction of ovulation and corpus luteum function. Horm. Res. Paediatr. 1992, 37 (Suppl. 1), 12–18. [Google Scholar] [CrossRef]
- Silva, J.F.; Ocarino, N.M.; Serakides, R. Thyroid hormones and female reproduction. Biol Reprod. 2018, 99, 907–921. [Google Scholar] [CrossRef]
- Witchel, S.F.; Oberfield, S.E.; Pena, A.S. Polycystic Ovary Syndrome: Pathophysiology, Presentation, and Treatment With Emphasis on Adolescent Girls. J. Endocr. Soc. 2019, 3, 1545–1573. [Google Scholar] [CrossRef] [Green Version]
- Rochon, C.; Tauveron, I.; Dejax, C.; Benoit, P.; Capitan, P.; Fabricio, A.; Berry, C.; Champredon, C.; Thieblot, P.; Grizard, J. Response of glucose disposal to hyperinsulinaemia in human hypothyroidism and hyperthyroidism. Clin. Sci. 2003, 104, 7–15. [Google Scholar] [CrossRef]
- Raber, W.; Nowotny, P.; Vytiska-Binstorfer, E.; Vierhapper, H. Thyroxine treatment modified in infertile women according to thyroxine-releasing hormone testing: 5 year follow-up of 283 women referred after exclusion of absolute causes of infertility. Hum. Reprod. 2003, 18, 707–714. [Google Scholar] [CrossRef] [Green Version]
- Singla, R.; Gupta, Y.; Khemani, M.; Aggarwal, S. Thyroid disorders and polycystic ovary syndrome: An emerging relationship. Indian J. Endocrinol. Metab. 2015, 19, 25–29. [Google Scholar] [CrossRef]
- Cooper, D.S. Clinical practice. Subclinical hypothyroidism. N. Engl. J. Med. 2001, 345, 260–265. [Google Scholar] [CrossRef]
- Ding, X.; Yang, L.; Wang, J.; Tang, R.; Chen, Q.; Pan, J.; Yang, H.; Chen, X.; Chen, Z.; Mu, L. Subclinical Hypothyroidism in Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2018, 9, 700. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Wang, J.; Shen, S.; Liu, J.; Sun, J.; Gu, T.; Zhu, D.; Bi, Y. Subclinical hypothyroidism is not a risk factor for polycystic ovary syndrome in obese women of reproductive age. Gynecol. Endocrinol. 2018, 34, 875–879. [Google Scholar] [CrossRef]
- Tehrani, F.R.; Simbar, M.; Tohidi, M.; Hosseinpanah, F.; Azizi, F. The prevalence of polycystic ovary syndrome in a community sample of Iranian population: Iranian PCOS prevalence study. Reprod. Biol. Endocrinol. 2011, 9, 39. [Google Scholar] [CrossRef] [Green Version]
- Rashidi, H.; Ramezani Tehrani, F.; Bahri Khomami, M.; Tohidi, M.; Azizi, F. To what extent does the use of the Rotterdam criteria affect the prevalence of polycystic ovary syndrome? A community-based study from the Southwest of Iran. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 174, 100–105. [Google Scholar] [CrossRef]
- Amouzegar, A.; Delshad, H.; Mehran, L.; Tohidi, M.; Khafaji, F.; Azizi, F. Reference limit of thyrotropin (TSH) and free thyroxine (FT4) in thyroperoxidase positive and negative subjects: A population based study. J. Endocrinol. Invest. 2013, 36, 950–954. [Google Scholar]
- Harding, M.; Lamarche, C. A quantile regression approach for estimating panel data models using instrumental variables. Econ. Lett. 2009, 104, 133–135. [Google Scholar] [CrossRef]
- Sridhar, G.R.; Nagamani, G. Hypothyroidism presenting with polycystic ovary syndrome. J. Assoc. Physicians India 1993, 41, 88–90. [Google Scholar]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Clin. Endocrinol. 2018, 89, 251–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krassas, G.E.; Pontikides, N.; Kaltsas, T.H.; Papadopoulou, P.H.; Paunkovic, J.; Paunkovic, N.; Duntas, H.L. Disturbances of menstruation in hypothyroidism. Clin. Endocrinol. 1999, 50, 655–659. [Google Scholar] [CrossRef] [PubMed]
- Calvar, C.E.; Bengolea, S.V.; Deutsch, S.I.; Hermes, R.; Ramos, G.; Loyato, M. High frequency of thyroid abnormalities in polycystic ovary syndrome. Medicina 2015, 75, 213–217. [Google Scholar] [PubMed]
- Morgante, G.; Musacchio, M.C.; Orvieto, R.; Massaro, M.G.; De Leo, V. Alterations in thyroid function among the different polycystic ovary syndrome phenotypes. Gynecol. Endocrinol. 2013, 29, 967–969. [Google Scholar] [CrossRef] [PubMed]
- Novais Jde, S.; Benetti-Pinto, C.L.; Garmes, H.M.; Jales, R.M.; Juliato, C.R. Polycystic ovary syndrome and chronic autoimmune thyroiditis. Gynecol. Endocrinol. 2015, 31, 48–51. [Google Scholar] [CrossRef]
- Sinha, U.; Sinharay, K.; Saha, S.; Longkumer, T.A.; Baul, S.N.; Pal, S.K. Thyroid disorders in polycystic ovarian syndrome subjects: A tertiary hospital based cross-sectional study from Eastern India. Indian J. Endocrinol. Metab. 2013, 17, 304–309. [Google Scholar] [CrossRef]
- Tagliaferri, V.; Romualdi, D.; Guido, M.; Mancini, A.; De Cicco, S.; Di Florio, C.; Immediata, V.; Di Segni, C.; Lanzone, A. The link between metabolic features and TSH levels in polycystic ovary syndrome is modulated by the body weight: An euglycaemic-hyperinsulinaemic clamp study. Eur. J Endocrinol. 2016, 175, 433–441. [Google Scholar] [CrossRef] [Green Version]
- Yu, Q.; Wang, J.B. Subclinical Hypothyroidism in PCOS: Impact on Presentation, Insulin Resistance, and Cardiovascular Risk. Biomed. Res. Int. 2016, 2016, 2067087. [Google Scholar] [CrossRef] [Green Version]
- Biondi, B.; Cappola, A.R.; Cooper, D.S. Subclinical Hypothyroidism: A Review. JAMA 2019, 322, 153–160. [Google Scholar] [CrossRef]
- Beagley, K.W.; Gockel, C.M. Regulation of innate and adaptive immunity by the female sex hormones oestradiol and progesterone. FEMS Immunol. Med. Microbiol. 2003, 38, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Janssen, O.E.; Mehlmauer, N.; Hahn, S.; Offner, A.H.; Gartner, R. High prevalence of autoimmune thyroiditis in patients with polycystic ovary syndrome. Eur. J. Endocrinol. 2004, 150, 363–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrikova, J.; Lazurova, I.; Yehuda, S. Polycystic ovary syndrome and autoimmunity. Eur. J. Intern. Med. 2010, 21, 369–371. [Google Scholar] [CrossRef] [PubMed]
- Romitti, M.; Fabris, V.C.; Ziegelmann, P.K.; Maia, A.L.; Spritzer, P.M. Association between PCOS and autoimmune thyroid disease: A systematic review and meta-analysis. Endocr. Connect. 2018, 7, 1158–1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nazeri, P.; Mirmiran, P.; Mehrabi, Y.; Hedayati, M.; Delshad, H.; Azizi, F. Evaluation of iodine nutritional status in Tehran, Iran: Iodine deficiency within iodine sufficiency. Thyroid 2010, 20, 1399–1406. [Google Scholar] [CrossRef] [PubMed]
- Delshad, H.; Azizi, F. Review of Iodine Nutrition in Iranian Population in the Past Quarter of Century. Int. J. Endocrinol. Metab. 2017, 15, e57758. [Google Scholar] [CrossRef] [Green Version]
- Vanderpump, M.P. The epidemiology of thyroid disease. Br. Med. Bull. 2011, 99, 39–51. [Google Scholar] [CrossRef] [Green Version]
- Chiovato, L.; Magri, F.; Carle, A. Hypothyroidism in Context: Where We’ve Been and Where We’re Going. Adv. Ther. 2019, 36 (Suppl. 2), 47–58. [Google Scholar] [CrossRef] [Green Version]
- Waldmann, E. Quantile regression: A short story on how and why. Stat. Model. 2018, 18, 203–218. [Google Scholar] [CrossRef]
- Arduc, A.; Aycicek Dogan, B.; Bilmez, S.; Imga Nasiroglu, N.; Tuna, M.M.; Isik, S.; Berker, D.; Guler, S. High prevalence of Hashimoto’s thyroiditis in patients with polycystic ovary syndrome: Does the imbalance between estradiol and progesterone play a role? Endocr. Res. 2015, 40, 204–210. [Google Scholar] [CrossRef]
- Duran, C.; Basaran, M.; Kutlu, O.; Kucukaydin, Z.; Bakdik, S.; Burnik, F.S.; Aslan, U.; Erdem, S.S.; Ecirli, S. Frequency of nodular goiter and autoimmune thyroid disease in patients with polycystic ovary syndrome. Endocrine 2015, 49, 464–469. [Google Scholar] [CrossRef]
- Karaköse, M.; Hepsen, S.; Çakal, E.; Arslan, M.S.; Tutal, E.; Akın, Ş.; Ünsal, İ.; Özbek, M. Frequency of nodular goiter and autoimmune thyroid disease and association of these disorders with insulin resistance in polycystic ovary syndrome. J. Turk. Ger. Gynecol. Assoc. 2017, 18, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Sinha, K.; Kolte, S.; Mandal, A. Endocrinal and autoimmune linkage: Evidences from a controlled study of subjects with polycystic ovarian syndrome. J. Hum. Reprod. Sci. 2016, 9, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Menon, M.; Ramachandran, V. Antithyroid Peroxidase Antibodies in Women with Polycystic Ovary Syndrome. J. Obstet. Gynecol. India 2017, 67, 61–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitkov, M.; Nyagolova, P.; Orbetzova, M. Thyroid Stimulating Hormone Levels in Euthyroid Women with Polycystic Ovary Syndrome. Akusherstvo Ginekol. 2015, 54, 10–15. [Google Scholar]
- Mele, C.; Mai, S.; Cena, T.; Pagano, L.; Scacchi, M.; Biondi, B.; Aimaretti, G.; Marzullo, P. The pattern of TSH and fT4 levels across different BMI ranges in a large cohort of euthyroid patients with obesity. Front. Endocrinol. 2022, 13, 1029376. [Google Scholar] [CrossRef]
- Sanyal, D.; Raychaudhuri, M. Hypothyroidism and obesity: An intriguing link. Indian J. Endocrinol. Metab. 2016, 20, 554–557. [Google Scholar] [CrossRef]
- Friedrich, N.; Schwarz, S.; Thonack, J.; John, U.; Wallaschofski, H.; Volzke, H. Association between parity and autoimmune thyroiditis in a general female population. Autoimmunity 2008, 41, 174–180. [Google Scholar] [CrossRef]
- Zimmermann, M.B.; Boelaert, K. Iodine deficiency and thyroid disorders. Lancet Diabetes Endocrinol. 2015, 3, 286–295. [Google Scholar] [CrossRef]
- Shin, D.Y.; Kim, K.J.; Kim, D.; Hwang, S.; Lee, E.J. Low serum vitamin D is associated with anti-thyroid peroxidase antibody in autoimmune thyroiditis. Yonsei Med. J. 2014, 55, 476–481. [Google Scholar] [CrossRef] [Green Version]
- Tabrizi, R.; Moosazadeh, M.; Akbari, M.; Dabbaghmanesh, M.H.; Mohamadkhani, M.; Asemi, Z.; Heydari, S.T.; Akbari, M.; Lankarani, K.B. High Prevalence of Vitamin D Deficiency among Iranian Population: A Systematic Review and Meta-Analysis. Iran. J. Med. Sci. 2018, 43, 125–139. [Google Scholar]
- Menichini, D.; Facchinetti, F. Effects of vitamin D supplementation in women with polycystic ovary syndrome: A review. Gynecol. Endocrinol. 2020, 36, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Le Cook, B.; Manning, W.G. Thinking beyond the mean: A practical guide for using quantile regression methods for health services research. Shanghai Arch. Psychiatry 2013, 25, 55–59. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Hormone | Measurement Method | Kit & Instrument | Intra-Assay | Inter-Assay |
|---|---|---|---|---|
| Total testosterone (TT) | enzyme immunoassay (EIA) | Diagnostic biochem Canada Co., London, ON, Canada | 1.7% | 2.3% |
| Dehydroepiandrosterone sulfate (DHEAS) | enzyme immunoassay (EIA) | DRG Instruments, GmbH, Marburg, Germany | 1.9% | 2.5% |
| Sex hormone-binding globulin (SHBG) | immunoenzymometric assay (IEMA) | Diagnostic biochem Canada Co., London, ON, Canada | 0.8% | 2.4% |
| Luteinizing hormone (LH) | immunoradiometric assay (IRMA) | commercial kits (Izotop, Budapest, Hungary) and a Dream Gamma- 10 gamma counter (Shin Jin Medics Inc., Koyang, Korea) | 1.6% | 4.2% |
| follicle-stimulating hormone (FSH) | 1.4% | 2% | ||
| thyroid-stimulating hormone (TSH) * | 2.1% | 3.1% | ||
| FT4 * | electrochemiluminescence immunoassay (ECLIA) | commercial kits on the Cobas e411 analyzer (Roche Diagnostics GmbH, Mannheim, Germany) | 1.3% | 3.3% |
| Variable | Total (n = 851) | Control (n = 644) | PCOS (n = 207) | p-Value |
|---|---|---|---|---|
| Age a (years) | 33.3 (7.5) | 34.1 (7.3) | 30.7 (7.5) | <0.001 |
| BMI a (kg/m2) | 26.7 (5.2) | 26.7 (5.1) | 26.6 (5.5) | 0.8 |
| Number of pregnancy a | 2.8 (1.6) | 2.9 (1.6) | 2.5 (1.5) | 0.01 |
| Number of delivery a | 2.5 (1.4) | 2.5 (1.4) | 2.1 (1.3) | 0.001 |
| Number of abortion a | 0.4 (0.7) | 0.4 (0.7) | 0.4 (0.6) | 0.9 |
| WC a (cm) | 83.2 (11.8) | 83.1 (11.7) | 83.2 (12.3) | 0.9 |
| Height a (cm) | 158.9 (6.2) | 158.9 (6.2) | 159.3 (6.1) | 0.4 |
| Weight a (kg) | 67.3 (13.0) | 67.3 (12.8) | 67.4 (13.7) | 0.9 |
| Hip a (cm) | 102.9 (12.2) | 102.9 (11.9) | 102.9 (13.3) | 0.9 |
| WHR a | 0.81 (0.09) | 0.81 (0.09) | 0.81 (0.07) | 0.9 |
| WHtR a | 0.52 (0.08) | 0.52 (0.08) | 0.52 (0.08) | 0.8 |
| FAI b | 1.9 (0.8,3.6) | 1.7 (0.7,3.2) | 3.3 (1.5,5.4) | <0.001 d |
| FSH b (microU/mL) | 7.6 (5.7,9.8) | 8.0 (5.9,10.1) | 8.9 (6.9,10.4) | <0.001 d |
| LH b (microU/mL) | 4.7 (3.4–6.5) | 4.6 (3.4–6.4) | 4.9 (3.3–7.0) | 0.2 |
| LH/FSH b | 0.6 (0.42–0.85) | 0.58 (0.40–0.81) | 0.69 (0.48–0.98) | <0.001 d |
| SHBG b (nmol/L) | 56.4 (42.7–81.9) | 59.4 (43.8–85.6) | 50.5 (40.8–67.5) | 0.001 d |
| DHEAS b (microg/dL) | 138.9 (73.6–195.6) | 118.9 (65.6–186.7) | 179.4 (119.3–221.0) | <0.001 d |
| Testosterone b (nmol/L) | 0.35 (0.14–0.61) | 0.31 (0.12–0.56) | 0.49 (0.24–0.79) | <0.001 d |
| TSH b (microU/mL) | 2.1 (1.5–3.4) | 2.1 (1.5–3.4) | 2.0 (1.4–3.4) | 0.2 |
| SCH c | 89 (10.5) | 65 (10.1) | 24 (11.6) | 0.5 |
| Variable | SCH PCOS (n = 24) | SCH Control (n = 65) | p-Value |
|---|---|---|---|
| Age a (years) | 32.3 (8.1) | 35.1 (7.5) | 0.1 |
| BMI a (kg/m2) | 28.0 (5.6) | 27.8 (4.5) | 0.8 |
| Number of pregnancy a | 2.7 (1.7) | 2.8 (1.4) | 0.8 |
| Number of delivery a | 2.1 (1.4) | 2.5 (1.3) | 0.3 |
| Number of abortion a | 0.5 (0.6) | 0.2 (0.4) | 0.07 |
| WC a (cm) | 87.9 (11.8) | 86.3 (9.6) | 0.5 |
| Height a (cm) | 158.9 (4.7) | 158.6 (5.7) | 0.9 |
| Weight a (kg) | 70.6 (13.7) | 69.9 (10.7) | 0.8 |
| Hip a (cm) | 107.7 (10.6) | 105.2 (9.7) | 0.3 |
| WHR a | 0.81 (0.07) | 0.82 (0.06) | 0.4 |
| WHtR a | 0.55 (0.08) | 0.54 (0.06) | 0.6 |
| FAI b | 4.9 (2.4–7.0) | 2.7 (1.2–3.8) | 0.004 d |
| FSH b (microU/mL) | 6.7 (5.5–9.0) | 6.5 (5.2–9.6) | 0.9 |
| LH b (microU/mL) | 4.3 (3.5–7.9) | 4.5 (3.5–6.4) | 0.5 |
| LH/FSH b | 0.6 (0.5–1.3) | 0.6 (0.5–0.8) | 0.5 |
| SHBG b (nmol/L) | 44.1 (33.2–54.8) | 60.1 (49.9–89.3) | 0.001 d |
| DHEAS b (microg/dL) | 191.9 (148.0–221.5) | 136.1 (55.8–214.8) | 0.01 f |
| Testosterone b (nmol/L) | 0.6 (0.3–0.8) | 0.5 (0.2–0.7) | 0.08 |
| Model | Variable | OR | 95% CI | p-Value |
|---|---|---|---|---|
| Unadjusted model | PCOS | 1.17 | 0.71, 1.92 | 0.5 |
| Adjusted model * | PCOS | 1.40 | 0.79, 2.50 | 0.2 |
| Age (year) | 1.02 | 0.97, 1.07 | 0.4 | |
| BMI (kg/m2) | 1.04 | 0.99, 1.09 | 0.1 | |
| parity | 0.90 | 0.74, 1.09 | 0.3 |
| Model | 5th Centile | 25th Centile | Median | 75th Centile | 95th Centile | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Coef. 95% CI | p-Value | Coef. 95% CI | p-Value | Coef. 95% CI | p-Value | Coef. 95% CI | p-Value | Coef. 95% CI | p-Value | |
| Unadjusted | −0.19 −0.47, 0.09 | 0.2 | −0.10 −0.29,0.09 | 0.3 | −0.16 −0.39, 0.07 | 0.2 | −0.04 −0.84, 0.76 | 0.9 | −0.44 −1.25, 0.37 | 0.3 |
| Adjusted * | −0.18 −0.44, 0.06 | 0.1 | −0.07 −0.26, 0.11 | 0.4 | −0.16 −0.32, −0.01 | 0.04 | 0.05 −0.65, 0.77 | 0.9 | −0.24 −1.55, 1.07 | 0.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rojhani, E.; Rahmati, M.; Firouzi, F.; Saei Ghare Naz, M.; Azizi, F.; Ramezani Tehrani, F. Polycystic Ovary Syndrome, Subclinical Hypothyroidism, the Cut-Off Value of Thyroid Stimulating Hormone; Is There a Link? Findings of a Population-Based Study. Diagnostics 2023, 13, 316. https://doi.org/10.3390/diagnostics13020316
Rojhani E, Rahmati M, Firouzi F, Saei Ghare Naz M, Azizi F, Ramezani Tehrani F. Polycystic Ovary Syndrome, Subclinical Hypothyroidism, the Cut-Off Value of Thyroid Stimulating Hormone; Is There a Link? Findings of a Population-Based Study. Diagnostics. 2023; 13(2):316. https://doi.org/10.3390/diagnostics13020316
Chicago/Turabian StyleRojhani, Ehsan, Maryam Rahmati, Faegheh Firouzi, Marzieh Saei Ghare Naz, Fereidoun Azizi, and Fahimeh Ramezani Tehrani. 2023. "Polycystic Ovary Syndrome, Subclinical Hypothyroidism, the Cut-Off Value of Thyroid Stimulating Hormone; Is There a Link? Findings of a Population-Based Study" Diagnostics 13, no. 2: 316. https://doi.org/10.3390/diagnostics13020316