
Expression of the Immunohistochemical Markers CK5, CD117, and EGFR in Molecular Subtypes of Breast Cancer Correlated with Prognosis

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
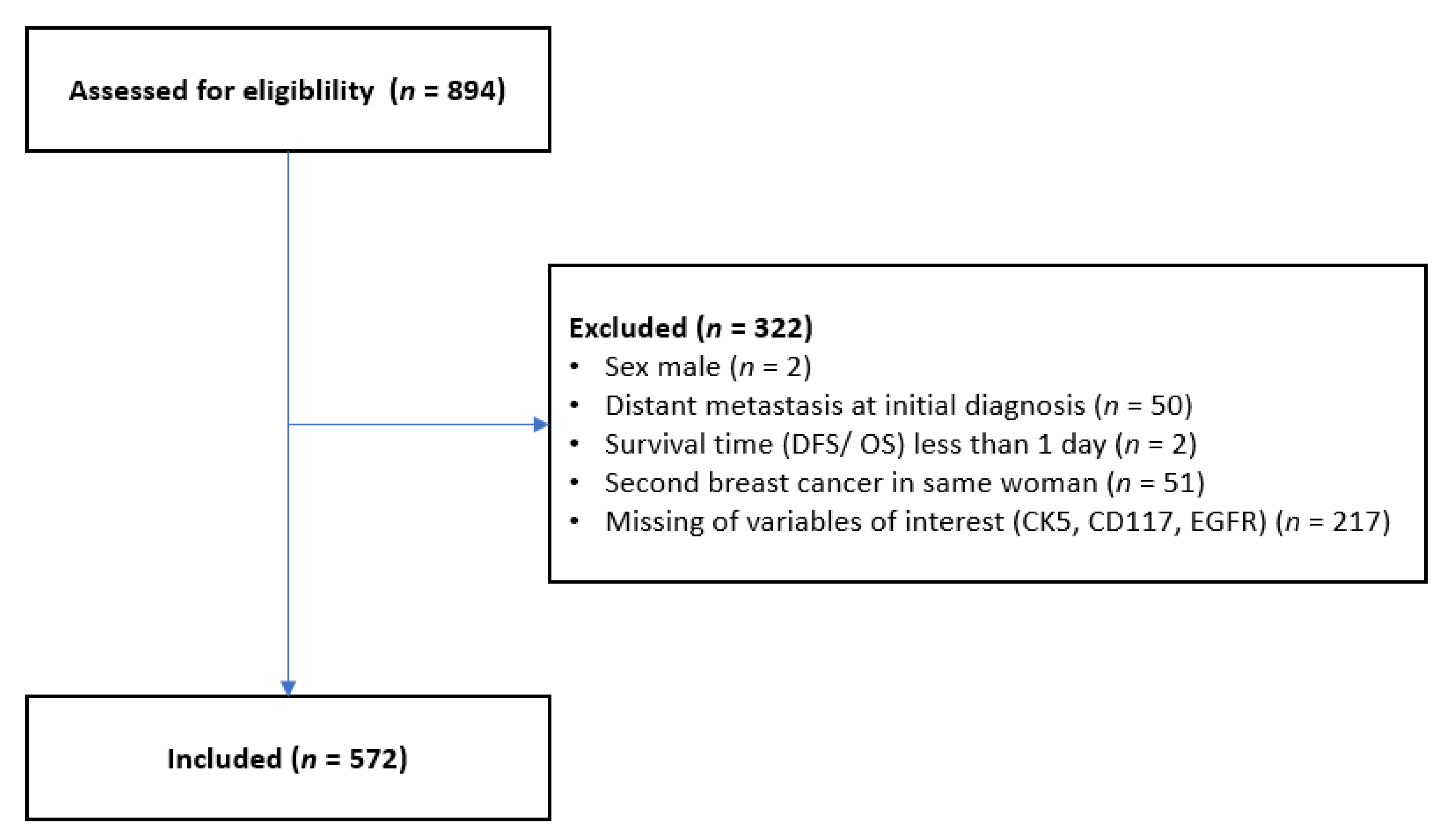
2.1. Patient Selection
2.2. Clinical Data
2.3. Histopathological Assessment
2.4. Evaluation of CK5, CD117, and EGFR
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Distribution of CK5, CD117, and EGFR
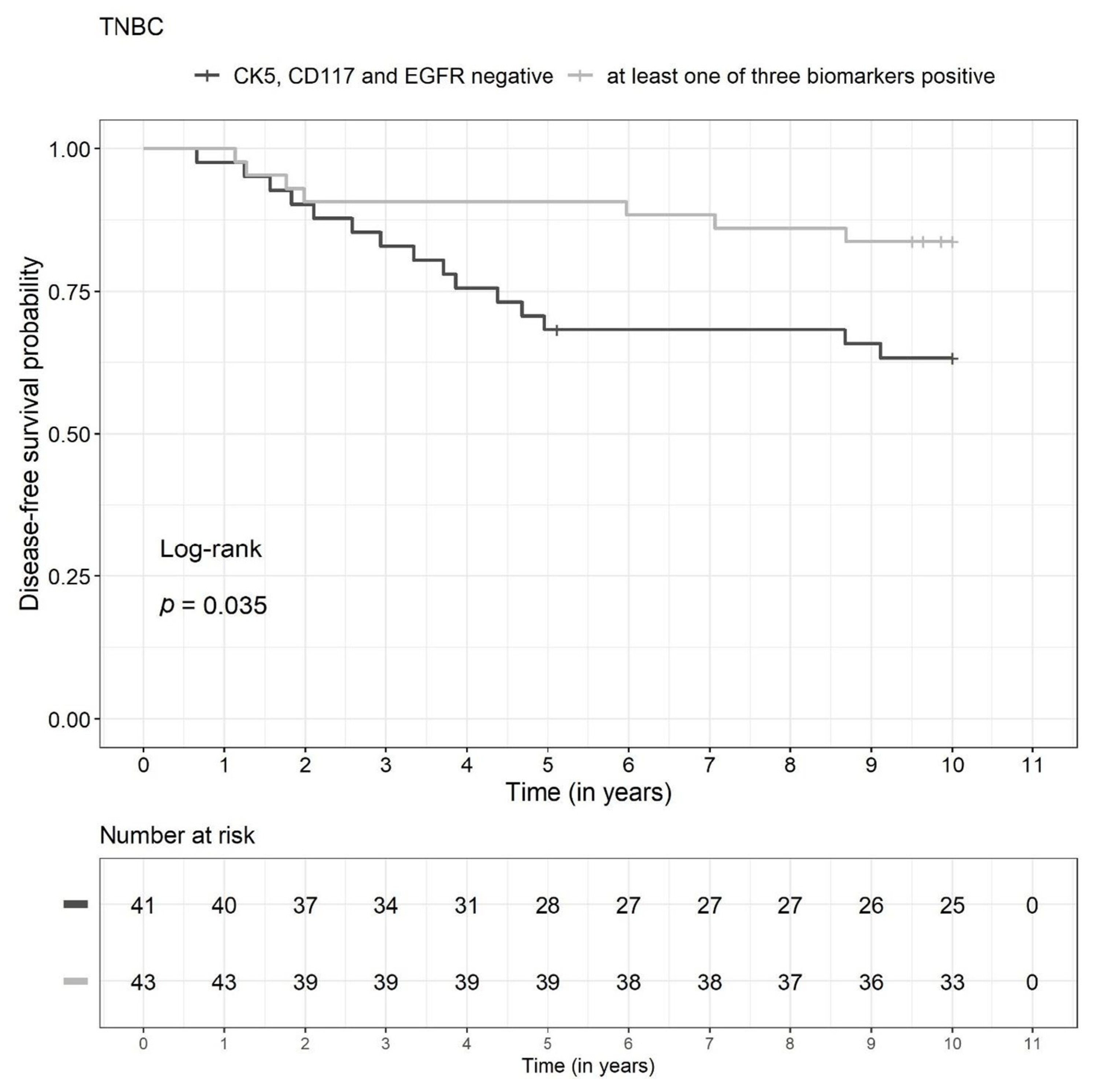
3.3. Prognosis in the TNBC Subgroup
3.4. Prognosis in Other Molecular Subclasses
4. Discussion
4.1. Prognostic Impact of CK5 in Breast Cancer
4.2. Prognostic Impact of CD117 in Breast Cancer
4.3. Prognostic Impact of EGFR in Breast Cancer
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schneeweiss, A.; Denkert, C.; Fasching, P.A.; Fremd, C.; Gluz, O.; Kolberg-Liedtke, C.; Loibl, S.; Lueck, H.J. Diagnosis and Therapy of Triple-Negative Breast Cancer (TNBC)—Recommendations for Daily Routine Practice. Geburtshilfe Frauenheilkd 2019, 79, 605–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fasching, P.A.; Lux, M.P.; Beckmann, K.; Strick, R.; Beckmann, M.W. Entscheidungshilfen bei der Therapiewahl für Patientinnen mit Mammakarzinom. Der Gynäkologe 2005, 38, 388–397. [Google Scholar] [CrossRef]
- Burstein, H.J.; Curigliano, G.; Loibl, S.; Dubsky, P.; Gnant, M.; Poortmans, P.; Colleoni, M.; Denkert, C.; Piccart-Gebhart, M.; Regan, M.; et al. Estimating the benefits of therapy for early-stage breast cancer: The St. Gallen International Consensus Guidelines for the primary therapy of early breast cancer 2019. Ann. Oncol. 2019, 30, 1541–1557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E.; ESMO Guidelines Committee. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 1674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pusztai, L.; Foldi, J.; Dhawan, A.; DiGiovanna, M.P.; Mamounas, E.P. Changing frameworks in treatment sequencing of triple-negative and HER2-positive, early-stage breast cancers. Lancet Oncol. 2019, 20, e390–e396. [Google Scholar] [CrossRef]
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Costantino, J.P.; Wolmark, N.; Bonnefoi, H.; Cameron, D.; Gianni, L.; Valagussa, P.; et al. Pathological complete response and long-term clinical benefit in breast cancer: The CTNeoBC pooled analysis. Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef] [Green Version]
- Spring, L.M.; Fell, G.; Arfe, A.; Sharma, C.; Greenup, R.; Reynolds, K.L.; Smith, B.L.; Alexander, B.; Moy, B.; Isakoff, S.J.; et al. Pathologic Complete Response after Neoadjuvant Chemotherapy and Impact on Breast Cancer Recurrence and Survival: A Comprehensive Meta-analysis. Clin. Cancer Res. 2020, 26, 2838–2848. [Google Scholar] [CrossRef]
- Massafra, R.; Comes, M.C.; Bove, S.; Didonna, V.; Gatta, G.; Giotta, F.; Fanizzi, A.; La Forgia, D.; Latorre, A.; Pastena, M.I.; et al. Robustness Evaluation of a Deep Learning Model on Sagittal and Axial Breast DCE-MRIs to Predict Pathological Complete Response to Neoadjuvant Chemotherapy. J. Pers. Med. 2022, 12, 953. [Google Scholar] [CrossRef]
- Amoroso, N.; Pomarico, D.; Fanizzi, A.; Didonna, V.; Giotta, F.; La Forgia, D.; Latorre, A.; Monaco, A.; Pantaleo, E.; Petruzzellis, N.; et al. A Roadmap towards Breast Cancer Therapies Supported by Explainable Artificial Intelligence. Appl. Sci. 2021, 11, 4881. [Google Scholar] [CrossRef]
- Vasileiou, G.; Costa, M.J.; Long, C.; Wetzler, I.R.; Hoyer, J.; Kraus, C.; Popp, B.; Emons, J.; Wunderle, M.; Wenkel, E.; et al. Breast MRI texture analysis for prediction of BRCA-associated genetic risk. BMC Med. Imaging 2020, 20, 86. [Google Scholar] [CrossRef]
- Dent, R.; Trudeau, M.; Pritchard, K.I.; Hanna, W.M.; Kahn, H.K.; Sawka, C.A.; Lickley, L.A.; Rawlinson, E.; Sun, P.; Narod, S.A. Triple-negative breast cancer: Clinical features and patterns of recurrence. Clin. Cancer Res. 2007, 13, 4429–4434. [Google Scholar] [CrossRef] [Green Version]
- Huang, M.; O’Shaughnessy, J.; Zhao, J.; Haiderali, A.; Cortes, J.; Ramsey, S.D.; Briggs, A.; Hu, P.; Karantza, V.; Aktan, G.; et al. Association of Pathologic Complete Response with Long-Term Survival Outcomes in Triple-Negative Breast Cancer: A Meta-Analysis. Cancer Res. 2020, 80, 5427–5434. [Google Scholar] [CrossRef]
- Gass, P.; Lux, M.P.; Rauh, C.; Hein, A.; Bani, M.R.; Fiessler, C.; Hartmann, A.; Haberle, L.; Pretscher, J.; Erber, R.; et al. Prediction of pathological complete response and prognosis in patients with neoadjuvant treatment for triple-negative breast cancer. BMC Cancer 2018, 18, 1051. [Google Scholar] [CrossRef] [Green Version]
- Chen, K.; Lu, P.; Beeraka, N.M.; Sukocheva, O.A.; Madhunapantula, S.V.; Liu, J.; Sinelnikov, M.Y.; Nikolenko, V.N.; Bulygin, K.V.; Mikhaleva, L.M.; et al. Mitochondrial mutations and mitoepigenetics: Focus on regulation of oxidative stress-induced responses in breast cancers. Semin. Cancer Biol. 2022, 83, 556–569. [Google Scholar] [CrossRef]
- Gao, Y.; Jones, A.; Fasching, P.A.; Ruebner, M.; Beckmann, M.W.; Widschwendter, M.; Teschendorff, A.E. The integrative epigenomic-transcriptomic landscape of ER positive breast cancer. Clin. Epigenetics 2015, 7, 126. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.e.; Chen, C.; Wang, X.; Sun, Y.; Zhang, J.; Chen, J.; Shi, Y. An Epigenetic Role of Mitochondria in Cancer. Cells 2022, 11, 2518. [Google Scholar] [CrossRef]
- Mijnes, J.; Tiedemann, J.; Eschenbruch, J.; Gasthaus, J.; Bringezu, S.; Bauerschlag, D.; Maass, N.; Arnold, N.; Weimer, J.; Anzeneder, T.; et al. SNiPER: A novel hypermethylation biomarker panel for liquid biopsy based early breast cancer detection. Oncotarget 2019, 10, 6494–6508. [Google Scholar] [CrossRef] [Green Version]
- Rekhtman, N.; Bishop, J.A. Quick Clinical References for Pathologists. In Quick Reference Handbook for Surgical Pathologists; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar] [CrossRef]
- Medinger, M.; Kleinschmidt, M.; Mross, K.; Wehmeyer, B.; Unger, C.; Schaefer, H.-E.; Weber, R.; Azemar, M. c-kit (CD117) Expression in Human Tumors and its Prognostic Value: An Immunohistochemical Analysis. Pathol. Oncol. Res. 2010, 16, 295–301. [Google Scholar] [CrossRef]
- Wang, Z. ErbB Receptors and Cancer. Methods Mol. Biol. 2017, 1652, 3–35. [Google Scholar] [CrossRef]
- Foulkes, W.D.; Brunet, J.S.; Stefansson, I.M.; Straume, O.; Chappuis, P.O.; Begin, L.R.; Hamel, N.; Goffin, J.R.; Wong, N.; Trudel, M.; et al. The prognostic implication of the basal-like (cyclin Ehigh/p27low/p53+/glomeruloid-microvascular-proliferation+) phenotype of BRCA1-related breast cancer. Cancer Res. 2004, 64, 830–835. [Google Scholar] [CrossRef] [Green Version]
- Foulkes, W.D.; Stefansson, I.M.; Chappuis, P.O.; Begin, L.R.; Goffin, J.R.; Wong, N.; Trudel, M.; Akslen, L.A. Germline BRCA1 mutations and a basal epithelial phenotype in breast cancer. J. Natl. Cancer Inst. 2003, 95, 1482–1485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blows, F.M.; Driver, K.E.; Schmidt, M.K.; Broeks, A.; van Leeuwen, F.E.; Wesseling, J.; Cheang, M.C.; Gelmon, K.; Nielsen, T.O.; Blomqvist, C.; et al. Subtyping of breast cancer by immunohistochemistry to investigate a relationship between subtype and short and long term survival: A collaborative analysis of data for 10,159 cases from 12 studies. PLoS Med. 2010, 7, e1000279. [Google Scholar] [CrossRef] [PubMed]
- Tischkowitz, M.; Brunet, J.S.; Begin, L.R.; Huntsman, D.G.; Cheang, M.C.; Akslen, L.A.; Nielsen, T.O.; Foulkes, W.D. Use of immunohistochemical markers can refine prognosis in triple negative breast cancer. BMC Cancer 2007, 7, 134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdelrahman, A.E.; Rashed, H.E.; Abdelgawad, M.; Abdelhamid, M.I. Prognostic impact of EGFR and cytokeratin 5/6 immunohistochemical expression in triple-negative breast cancer. Ann. Diagn. Pathol. 2017, 28, 43–53. [Google Scholar] [CrossRef]
- Cheang, M.C.; Voduc, D.; Bajdik, C.; Leung, S.; McKinney, S.; Chia, S.K.; Perou, C.M.; Nielsen, T.O. Basal-like breast cancer defined by five biomarkers has superior prognostic value than triple-negative phenotype. Clin. Cancer Res. 2008, 14, 1368–1376. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, T.O.; Hsu, F.D.; Jensen, K.; Cheang, M.; Karaca, G.; Hu, Z.; Hernandez-Boussard, T.; Livasy, C.; Cowan, D.; Dressler, L.; et al. Immunohistochemical and clinical characterization of the basal-like subtype of invasive breast carcinoma. Clin. Cancer Res. 2004, 10, 5367–5374. [Google Scholar] [CrossRef] [Green Version]
- Fasching, P.A.; Loehberg, C.R.; Strissel, P.L.; Lux, M.P.; Bani, M.R.; Schrauder, M.; Geiler, S.; Ringleff, K.; Oeser, S.; Weihbrecht, S.; et al. Single nucleotide polymorphisms of the aromatase gene (CYP19A1), HER2/neu status, and prognosis in breast cancer patients. Breast Cancer Res. Treat. 2008, 112, 89–98. [Google Scholar] [CrossRef]
- Erber, R.; Rubner, M.; Davenport, S.; Hauke, S.; Beckmann, M.W.; Hartmann, A.; Haberle, L.; Gass, P.; Press, M.F.; Fasching, P.A. Impact of fibroblast growth factor receptor 1 (FGFR1) amplification on the prognosis of breast cancer patients. Breast Cancer Res. Treat. 2020, 184, 311–324. [Google Scholar] [CrossRef]
- Elston, C.W.; Ellis, I.O. Pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef]
- Kashiwagi, S.; Yashiro, M.; Takashima, T.; Aomatsu, N.; Kawajiri, H.; Ogawa, Y.; Onoda, N.; Ishikawa, T.; Wakasa, K.; Hirakawa, K. c-Kit expression as a prognostic molecular marker in patients with basal-like breast cancer. Br. J. Surg. 2013, 100, 490–496. [Google Scholar] [CrossRef]
- Luo, Y.; Huang, W.; Zhang, H.; Liu, G. Prognostic significance of CD117 expression and TP53 missense mutations in triple-negative breast cancer. Oncol. Lett. 2018, 15, 6161–6170. [Google Scholar] [CrossRef] [Green Version]
- Erber, R.; Meyer, J.; Taubert, H.; Fasching, P.A.; Wach, S.; Haberle, L.; Gass, P.; Schulz-Wendtland, R.; Landgraf, L.; Olbricht, S.; et al. PIWI-Like 1 and PIWI-Like 2 Expression in Breast Cancer. Cancers 2020, 12, 2742. [Google Scholar] [CrossRef]
- Wunderle, M.; Pretscher, J.; Brucker, S.Y.; Volz, B.; Hartmann, A.; Fiessler, C.; Hein, A.; Haberle, L.; Jud, S.M.; Lux, M.P.; et al. Association between breast cancer risk factors and molecular type in postmenopausal patients with hormone receptor-positive early breast cancer. Breast Cancer Res. Treat. 2019, 174, 453–461. [Google Scholar] [CrossRef]
- Salmen, J.; Neugebauer, J.; Fasching, P.A.; Haeberle, L.; Huober, J.; Wockel, A.; Rauh, C.; Schuetz, F.; Weissenbacher, T.; Kost, B.; et al. Pooled analysis of the prognostic relevance of progesterone receptor status in five German cohort studies. Breast Cancer Res. Treat. 2014, 148, 143–151. [Google Scholar] [CrossRef]
- Perou, C.M.; Sorlie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef] [Green Version]
- van de Rijn, M.; Perou, C.M.; Tibshirani, R.; Haas, P.; Kallioniemi, O.; Kononen, J.; Torhorst, J.; Sauter, G.; Zuber, M.; Kochli, O.R.; et al. Expression of cytokeratins 17 and 5 identifies a group of breast carcinomas with poor clinical outcome. Am. J. Pathol. 2002, 161, 1991–1996. [Google Scholar] [CrossRef]
- Alshareeda, A.T.; Soria, D.; Garibaldi, J.M.; Rakha, E.; Nolan, C.; Ellis, I.O.; Green, A.R. Characteristics of basal cytokeratin expression in breast cancer. Breast Cancer Res. Treat. 2013, 139, 23–37. [Google Scholar] [CrossRef]
- Inanc, M.; Ozkan, M.; Karaca, H.; Berk, V.; Bozkurt, O.; Duran, A.O.; Ozaslan, E.; Akgun, H.; Tekelioglu, F.; Elmali, F. Cytokeratin 5/6, c-Met expressions, and PTEN loss prognostic indicators in triple-negative breast cancer. Med. Oncol. 2014, 31, 801. [Google Scholar] [CrossRef] [PubMed]
- Dogu, G.G.; Ozkan, M.; Ozturk, F.; Dikilitas, M.; Er, O.; Ozturk, A. Triple-negative breast cancer: Immunohistochemical correlation with basaloid markers and prognostic value of survivin. Med. Oncol. 2010, 27, 34–39. [Google Scholar] [CrossRef]
- Sutton, L.M.; Han, J.S.; Molberg, K.H.; Sarode, V.R.; Cao, D.; Rakheja, D.; Sailors, J.; Peng, Y. Intratumoral expression level of epidermal growth factor receptor and cytokeratin 5/6 is significantly associated with nodal and distant metastases in patients with basal-like triple-negative breast carcinoma. Am. J. Clin. Pathol. 2010, 134, 782–787. [Google Scholar] [CrossRef] [Green Version]
- Thike, A.A.; Iqbal, J.; Cheok, P.Y.; Chong, A.P.; Tse, G.M.; Tan, B.; Tan, P.; Wong, N.S.; Tan, P.H. Triple negative breast cancer: Outcome correlation with immunohistochemical detection of basal markers. Am. J. Surg. Pathol. 2010, 34, 956–964. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, Y.; Ibusuki, M.; Nakano, M.; Kawasoe, T.; Hiki, R.; Iwase, H. Clinical significance of basal-like subtype in triple-negative breast cancer. Breast Cancer 2009, 16, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Adamo, B.; Ricciardi, G.R.R.; Ieni, A.; Franchina, T.; Fazzari, C.; Sano, M.V.; Angelico, G.; Caruso, M.; Tuccari, G.; Adamo, V. Correction: The prognostic significance of combined androgen receptor, E-Cadherin, Ki67 and CK5/6 expression in patients with triple negative breast cancer. Oncotarget 2019, 10, 917. [Google Scholar] [CrossRef]
- Ilie, S.M.; Bacinschi, X.E.; Botnariuc, I.; Anghel, R.M. Potential clinically useful prognostic biomarkers in triple-negative breast cancer: Preliminary results of a retrospective analysis. Breast Cancer Targets Ther. 2018, 10, 177–194. [Google Scholar] [CrossRef] [Green Version]
- Ryu, D.W.; Lee, C.H. Outcome of triple-negative breast cancer in patients with or without markers regulating cell cycle and cell death. J. Korean Surg. Soc. 2012, 83, 187–195. [Google Scholar] [CrossRef] [Green Version]
- Maeda, T.; Nakanishi, Y.; Hirotani, Y.; Fuchinoue, F.; Enomoto, K.; Sakurai, K.; Amano, S.; Nemoto, N. Immunohistochemical co-expression status of cytokeratin 5/6, androgen receptor, and p53 as prognostic factors of adjuvant chemotherapy for triple negative breast cancer. Med. Mol. Morphol. 2016, 49, 11–21. [Google Scholar] [CrossRef]
- Jansson, S.; Bendahl, P.O.; Grabau, D.A.; Falck, A.K.; Ferno, M.; Aaltonen, K.; Ryden, L. The three receptor tyrosine kinases c-KIT, VEGFR2 and PDGFRalpha, closely spaced at 4q12, show increased protein expression in triple-negative breast cancer. PLoS ONE 2014, 9, e102176. [Google Scholar] [CrossRef]
- Johansson, I.; Aaltonen, K.E.; Ebbesson, A.; Grabau, D.; Wigerup, C.; Hedenfalk, I.; Ryden, L. Increased gene copy number of KIT and VEGFR2 at 4q12 in primary breast cancer is related to an aggressive phenotype and impaired prognosis. Genes Chromosomes Cancer 2012, 51, 375–383. [Google Scholar] [CrossRef]
- Charpin, C.; Giusiano, S.; Charfi, S.; Secq, V.; Carpentier, S.; Andrac, L.; Lavaut, M.N.; Allasia, C.; Bonnier, P.; Garcia, S. Quantitative immunohistochemical expression of c Kit in breast carcinomas is predictive of patients’ outcome. Br. J. Cancer 2009, 101, 48–54. [Google Scholar] [CrossRef]
- Park, H.S.; Jang, M.H.; Kim, E.J.; Kim, H.J.; Lee, H.J.; Kim, Y.J.; Kim, J.H.; Kang, E.; Kim, S.-W.; Kim, I.A.; et al. High EGFR gene copy number predicts poor outcome in triple-negative breast cancer. Mod. Pathol. 2014, 27, 1212–1222. [Google Scholar] [CrossRef] [Green Version]
- Sobande, F.; Dušek, L.; Matějková, A.; Rozkoš, T.; Laco, J.; Ryška, A. EGFR in triple negative breast carcinoma: Significance of protein expression and high gene copy number. Cesk Patol 2015, 51, 80–86. [Google Scholar] [PubMed]
- van Reesema, L.L.S.; Zheleva, V.; Winston, J.S.; Jansen, R.J.; O’Connor, C.F.; Isbell, A.J.; Bian, M.; Qin, R.; Bassett, P.T.; Hinson, V.J.; et al. SIAH and EGFR, Two RAS Pathway Biomarkers, are Highly Prognostic in Locally Advanced and Metastatic Breast Cancer. EBioMedicine 2016, 11, 183–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, D.; He, J.; Yuan, Z.; Wang, S.; Peng, R.; Shi, Y.; Teng, X.; Qin, T. EGFR expression correlates with decreased disease-free survival in triple-negative breast cancer: A retrospective analysis based on a tissue microarray. Med. Oncol. 2012, 29, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Yue, Y.; Astvatsaturyan, K.; Cui, X.; Zhang, X.; Fraass, B.; Bose, S. Stratification of Prognosis of Triple-Negative Breast Cancer Patients Using Combinatorial Biomarkers. PLoS ONE 2016, 11, e0149661. [Google Scholar] [CrossRef]
- Tang, Y.; Zhu, L.; Li, Y.; Ji, J.; Li, J.; Yuan, F.; Wang, D.; Chen, W.; Huang, O.; Chen, X.; et al. Overexpression of epithelial growth factor receptor (EGFR) predicts better response to neo-adjuvant chemotherapy in patients with triple-negative breast cancer. J. Transl. Med. 2012, 10 (Suppl. S1), S4. [Google Scholar] [CrossRef] [Green Version]
- Koo, J.S.; Jung, W.; Jeong, J. The predictive role of E-cadherin and androgen receptor on in vitro chemosensitivity in triple-negative breast Cancer. Jpn. J. Clin. Oncol. 2009, 39, 560–568. [Google Scholar] [CrossRef] [Green Version]
- Fasching, P.A.; Heusinger, K.; Haeberle, L.; Niklos, M.; Hein, A.; Bayer, C.M.; Rauh, C.; Schulz-Wendtland, R.; Bani, M.R.; Schrauder, M.; et al. Ki67, chemotherapy response, and prognosis in breast cancer patients receiving neoadjuvant treatment. BMC Cancer 2011, 11, 486. [Google Scholar] [CrossRef] [Green Version]
- Wunderle, M.; Gass, P.; Haberle, L.; Flesch, V.M.; Rauh, C.; Bani, M.R.; Hack, C.C.; Schrauder, M.G.; Jud, S.M.; Emons, J.; et al. BRCA mutations and their influence on pathological complete response and prognosis in a clinical cohort of neoadjuvantly treated breast cancer patients. Breast Cancer Res. Treat. 2018, 171, 85–94. [Google Scholar] [CrossRef]
- Wurfel, F.; Erber, R.; Huebner, H.; Hein, A.; Lux, M.P.; Jud, S.; Kremer, A.; Kranich, H.; Mackensen, A.; Haberle, L.; et al. TILGen: A Program to Investigate Immune Targets in Breast Cancer Patients—First Results on the Influence of Tumor-Infiltrating Lymphocytes. Breast Care 2018, 13, 8–14. [Google Scholar] [CrossRef]
- Heindl, F.; Fasching, P.A.; Hein, A.; Hack, C.C.; Heusinger, K.; Gass, P.; Poschke, P.; Stubs, F.A.; Schulz-Wendtland, R.; Hartmann, A.; et al. Mammographic density and prognosis in primary breast cancer patients. Breast 2021, 59, 51–57. [Google Scholar] [CrossRef]
- Shao, M.-M.; Chan, S.K.; Yu, A.M.C.; Lam, C.C.F.; Tsang, J.Y.S.; Lui, P.C.W.; Law, B.K.B.; Tan, P.-H.; Tse, G.M. Keratin expression in breast cancers. Virchows Arch. 2012, 461, 313–322. [Google Scholar] [CrossRef]
- Sood, N.; Nigam, J.S. Correlation of CK5 and EGFR with Clinicopathological Profile of Triple-Negative Breast Cancer. Patholog. Res. Int. 2014, 2014, 141864. [Google Scholar] [CrossRef] [Green Version]
- Remmele, W.; Stegner, H.E. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Pathologe 1987, 8, 138–140. [Google Scholar]
- Erber, R.; Kailayangiri, S.; Huebner, H.; Ruebner, M.; Hartmann, A.; Haberle, L.; Meyer, J.; Volkl, S.; Mackensen, A.; Landgraf, L.; et al. Variable Expression of the Disialoganglioside GD2 in Breast Cancer Molecular Subtypes. Cancers 2021, 13, 5577. [Google Scholar] [CrossRef]
- Engstrom, M.J.; Valla, M.; Bofin, A.M. Basal markers and prognosis in luminal breast cancer. Breast Cancer Res. Treat. 2017, 163, 207–217. [Google Scholar] [CrossRef] [Green Version]
- Allison, K.H.; Hammond, M.E.H.; Dowsett, M.; McKernin, S.E.; Carey, L.A.; Fitzgibbons, P.L.; Wolff, A.C. Estrogen and Progesterone Receptor Testing in Breast Cancer: ASCO/CAP Guideline Update. J. Clin. Oncol. 2020, 38, 1346–1366. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.H.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Hayes, D.F. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J. Clin. Oncol. 2013, 31, 3997–4013. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.; Dowsett, M. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. J. Clin. Oncol. 2018, 36, 2105–2122. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subgroup | CK5 | CD117 | EGFR |
|---|---|---|---|
| TBN | 0 and | 0 or 1 and | 0 |
| Non-TBN | >0 and/or | >1 and/or | >0 |
| Parameter | Category | TNBC | Total |
|---|---|---|---|
| Patients | n | 84 | 572 |
| Age | Mean (SD) | 55.8 (13.2) | 57.5 (12.3) |
| BMI | Mean (SD) | 26.2 (4.9) | 26.4 (5.2) |
| Ki-67 | Mean (SD) | 43.1 (25.7) | 24.0 (20.9) |
| ER | Positive | 0 (0) | 448 (78.3) |
| PR | Positive | 0 (0) | 419 (73.3) |
| HER2 | Positive | 0 (0) | 70 (12.2) |
| Tumor grade (G) | G1 | 1 (1.2) | 45 (7.9) |
| G2 | 31 (36.9) | 386 (67.5) | |
| G3 | 52 (61.9) | 141 (24.7) | |
| Nodal status (N) | N+ | 36 (42.9) | 243 (42.5) |
| Tumor stage (T) | T1 | 43 (51.2) | 294 (51.4) |
| T2 | 35 (41.7) | 227 (39.7) | |
| T3 | 3 (3.6) | 28 (4.9) | |
| T4 | 3 (3.6) | 23 (4.0) | |
| Molecular subtype | TNBC | 84 (100) | 84 (14.7) |
| Luminal A-like | 0 (0) | 212 (37.1) | |
| Luminal B-like | 0 (0) | 206 (36.0) | |
| HER2+ | 0 (0) | 70 (12.2) | |
| CK5 | Positive | 30 (35.7) | 62 (10.8) |
| CD117 | Positive | 27 (32.1) | 67 (11.7) |
| EGFR | Positive | 8 (9.5) | 14 (2.4) |
| Parameter | Category | Non-TBN | TBN |
|---|---|---|---|
| Patients | n | 43 | 41 |
| Age | Mean (SD) | 52.7 (14.2) | 59.0 (11.3) |
| BMI | Mean (SD) | 25.7 (5.2) | 26.7 (4.6) |
| Ki-67 | Mean (SD) | 52.6 (25.0) | 33.3 (22.7) |
| Tumor grade (G) | G1 | 0 | 1 (2.4) |
| G2 | 10 (23.3) | 21 (51.2) | |
| G3 | 33 (76.7) | 19 (46.3) | |
| Nodal status (N) | N+ | 16 (37.2) | 20 (48.8) |
| Tumor stage (T) | T1 | 27 (62.8) | 16 (39.0) |
| T2 | 15 (34.9) | 20 (48.8) | |
| T3 | 1 (2.3) | 2 (4.9) | |
| T4 | 0 (0.0) | 3 (7.3) | |
| CK5 | Negative | 13 (30.2) | 41 (100) |
| Positive | 30 (69.8) | 0 | |
| CD117 | Negative | 16 (37.2) | 41 (100) |
| Positive | 27 (62.8) | 0 | |
| EGFR | Negative | 35 (81.4) | 41 (100) |
| Positive | 8 (18.6) | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schulmeyer, C.E.; Fasching, P.A.; Häberle, L.; Meyer, J.; Schneider, M.; Wachter, D.; Ruebner, M.; Pöschke, P.; Beckmann, M.W.; Hartmann, A.; et al. Expression of the Immunohistochemical Markers CK5, CD117, and EGFR in Molecular Subtypes of Breast Cancer Correlated with Prognosis. Diagnostics 2023, 13, 372. https://doi.org/10.3390/diagnostics13030372
Schulmeyer CE, Fasching PA, Häberle L, Meyer J, Schneider M, Wachter D, Ruebner M, Pöschke P, Beckmann MW, Hartmann A, et al. Expression of the Immunohistochemical Markers CK5, CD117, and EGFR in Molecular Subtypes of Breast Cancer Correlated with Prognosis. Diagnostics. 2023; 13(3):372. https://doi.org/10.3390/diagnostics13030372
Chicago/Turabian StyleSchulmeyer, Carla E., Peter A. Fasching, Lothar Häberle, Julia Meyer, Michael Schneider, David Wachter, Matthias Ruebner, Patrik Pöschke, Matthias W. Beckmann, Arndt Hartmann, and et al. 2023. "Expression of the Immunohistochemical Markers CK5, CD117, and EGFR in Molecular Subtypes of Breast Cancer Correlated with Prognosis" Diagnostics 13, no. 3: 372. https://doi.org/10.3390/diagnostics13030372