
A Comparison of MGMT Testing by MSP and qMSP in Paired Snap-Frozen and Formalin-Fixed Paraffin-Embedded Gliomas

Abstract
:1. Introduction
2. Materials and Methods
2.1. Tumor Specimens
2.2. Genomic DNA Isolation and Bisulfite Conversion
2.3. Methylation-Specific Polymerase Chain Reaction (MSP)
2.3.1. MSP Analysis of the SF Samples
2.3.2. MSP Analysis of the FFPE Samples
2.3.3. qMSP Analysis of the SF Samples
2.4. Statictical Analyses
3. Results
3.1. Optimization of the MGMT Promoter MSP Reaction Conditions
3.1.1. Semi-Quantitative MSP Analysis of SF Samples
3.1.2. Semi-Quantitative MSP Analysis of FFPE Samples
3.1.3. Semi-Quantitative qMSP Analysis of FF Samples
3.2. Comparison of Three Different MSP Assays in MGMT Promoter Methylation Evaluation
3.2.1. Comparison of Semi-Quantitative MSP and Semi-Quantitative qMSP Analysis of SF Glioma Samples
- True positive rate (sensitivity)—80.0%;
- False negative rate (Type 2 error)—20.0%;
- False positive rate (Type 1 error)—21.1%;
- True negative rate (specificity)—78.9%.
- True positive rate (sensitivity)—85.7%;
- False negative rate (Type 2 error)—14.3%;
- False positive rate (Type 1 error)—14.8%;
- True negative rate (specificity)—85.2%
3.2.2. Comparison of MSP Analysis of FFPE and SF Glioma Samples
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Fan, Y.; Zhang, X.; Gao, C.; Jiang, S.; Wu, H.; Liu, Z.; Dou, T. Burden and trends of brain and central nervous system cancer from 1990 to 2019 at the global, regional, and country levels. Arch. Public Health 2022, 80, 209. [Google Scholar] [CrossRef]
- Low, J.T.; Ostrom, Q.T.; Cioffi, G.; Neff, C.; Waite, K.A.; Kruchko, C.; Barnholtz-Sloan, J.S. Primary brain and other central nervous system tumors in the United States (2014–2018): A summary of the CBTRUS statistical report for clinicians. Neuro-Oncol. Pract. 2022, 9, 165–182. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Demple, B.; Jacobsson, A.; Olsson, M.; Robins, P.; Lindahl, T. Repair of alkylated DNA in Escherichia coli. Physical properties of O6-methylguanine-DNA methyltransferase. J. Biol. Chem. 1982, 257, 13776–13780. [Google Scholar] [CrossRef]
- Sekiguchi, M.; Nakabeppu, Y. Adaptive response: Induced synthesis of DNA repair enzymes by alkylating agents. Trends Genet. 1987, 3, 51–54. [Google Scholar] [CrossRef]
- Sekiguchi, M.; Nakabeppu, Y.; Sakumi, K.; Tuzuki, T. DNA-repair methyltransferase as a molecular device for preventing mutation and cancer. J. Cancer Res. Clin. Oncol. 1996, 122, 199–206. [Google Scholar] [CrossRef]
- Hayakawa, H.; Koike, G.; Sekiguchi, M. Expression and cloning of complementary DNA for a human enzyme that repairs O6-methylguanine in DNA. J. Mol. Biol. 1990, 213, 739–747. [Google Scholar] [CrossRef]
- Tano, K.; Shiota, S.; Collier, J.; Foote, R.S.; Mitra, S. Isolation and structural characterization of a cDNA clone encoding the human DNA repair protein for O6-alkylguanine. Proc. Natl. Acad. Sci. USA 1990, 87, 686–690. [Google Scholar] [CrossRef] [Green Version]
- Rydberg, B.; Spurr, N.; Karran, P. cDNA cloning and chromosomal assignment of the human O6-methylguanine-DNA methyltransferase. cDNA expression in Escherichia coli and gene expression in human cells. J. Biol. Chem. 1990, 265, 9563–9569. [Google Scholar] [CrossRef]
- Citron, M.; Decker, R.; Chen, S.; Schneider, S.; Graver, M.; Kleynerman, L.; Kahn, L.B.; White, A.; Schoenhaus, M.; Yarosh, D. O6-methylguanine-DNA methyltransferase in human normal and tumor tissue from brain, lung, and ovary. Cancer Res. 1991, 51, 4131–4134. [Google Scholar]
- Esteller, M.; Hamilton, S.R.; Burger, P.C.; Baylin, S.B.; Herman, J.G. Inactivation of the DNA repair gene O6-methylguanine-DNA methyltransferase by promoter hypermethylation is a common event in primary human neoplasia. Cancer Res. 1999, 59, 793–797. [Google Scholar]
- Esteller, M.; Garcia-Foncillas, J.; Andion, E.; Goodman, S.N.; Hidalgo, O.F.; Vanaclocha, V.; Baylin, S.B.; Herman, J.G. Inactivation of the DNA-Repair Gene MGMT and the Clinical Response of Gliomas to Alkylating Agents. N. Engl. J. Med. 2000, 343, 1350–1354. [Google Scholar] [CrossRef]
- Hegi, M.E.; Diserens, A.-C.; Godard, S.; Dietrich, P.-Y.; Regli, L.; Ostermann, S.; Otten, P.; Van Melle, G.; de Tribolet, N.; Stupp, R. Clinical Trial Substantiates the Predictive Value of O-6-Methylguanine-DNA Methyltransferase Promoter Methylation in Glioblastoma Patients Treated with Temozolomide. Clin. Cancer Res. 2004, 10, 1871–1874. [Google Scholar] [CrossRef] [Green Version]
- Hegi, M.E.; Diserens, A.-C.; Gorlia, T.; Hamou, M.-F.; De Tribolet, N.; Weller, M.; Kros, J.M.; Hainfellner, J.A.; Mason, W.; Mariani, L.; et al. MGMT Gene Silencing and Benefit from Temozolomide in Glioblastoma. N. Engl. J. Med. 2005, 352, 997–1003. [Google Scholar] [CrossRef] [Green Version]
- Yu, W.; Zhang, L.; Wei, Q.; Shao, A. O6-Methylguanine-DNA Methyltransferase (MGMT): Challenges and New Opportunities in Glioma Chemotherapy. Front. Oncol. 2020, 9, 1547. [Google Scholar] [CrossRef] [Green Version]
- Malley, D.S.; Hamoudi, R.A.; Kocialkowski, S.; Pearson, D.M.; Collins, V.P.; Ichimura, K. A distinct region of the MGMT CpG island critical for transcriptional regulation is preferentially methylated in glioblastoma cells and xenografts. Acta Neuropathol. 2011, 121, 651–661. [Google Scholar] [CrossRef]
- Costello, J.F.; Futscher, B.W.; Tano, K.; Graunke, D.M.; Pieper, R.O. Graded methylation in the promoter and body of the O6-methylguanine DNA methyltransferase (MGMT) gene correlates with MGMT expression in human glioma cells. J. Biol. Chem. 1994, 269, 17228–17237. [Google Scholar] [CrossRef]
- Everhard, S.; Tost, J.; El Abdalaoui, H.; Crinière, E.; Busato, F.; Marie, Y.; Gut, I.G.; Sanson, M.; Mokhtari, K.; Laigle-Donadey, F.; et al. Identification of regions correlating MGMT promoter methylation and gene expression in glioblastomas. Neuro-Oncol. 2009, 11, 348–356. [Google Scholar] [CrossRef] [Green Version]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [Green Version]
- Baumert, B.G.; Hegi, M.E.; van den Bent, M.J.; von Deimling, A.; Gorlia, T.; Hoang-Xuan, K.; Brandes, A.A.; Kantor, G.; Taphoorn, M.J.B.; Ben Hassel, M.; et al. Temozolomide chemotherapy versus radiotherapy in high-risk low-grade glioma (EORTC 22033–26033): A randomised, open-label, phase 3 intergroup study. Lancet Oncol. 2016, 17, 1521–1532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.B.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Lakomy, R.; Kazda, T.; Selingerova, I.; Poprach, A.; Pospisil, P.; Belanova, R.; Fadrus, P.; Vybihal, V.; Smrcka, M.; Jancalek, R.; et al. Real-World Evidence in Glioblastoma: Stupp’s Regimen after a Decade. Front. Oncol. 2020, 10, 840. [Google Scholar] [CrossRef] [PubMed]
- Weller, M.; van den Bent, M.; Preusser, M.; Le Rhun, E.; Tonn, J.C.; Minniti, G.; Bendszus, M.; Balana, C.; Chinot, O.; Dirven, L.; et al. EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat. Rev. Clin. Oncol. 2021, 18, 170–186. [Google Scholar] [CrossRef]
- Malmström, A.; Lysiak, M.; Kristensen, B.W.; Hovey, E.; Henriksson, R.; Söderkvist, P. Do we really know who has an MGMT methylated glioma? Results of an international survey regarding use of MGMT analyses for glioma. Neuro-Oncology Pract. 2020, 7, 68–76. [Google Scholar] [CrossRef]
- Herman, J.G.; Graff, J.R.; Myöhänen, S.; Nelkin, B.D.; Baylin, S.B. Methylation-specific PCR: A novel PCR assay for methylation status of CpG islands. Proc. Natl. Acad. Sci. USA 1996, 93, 9821–9826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christians, A.; Hartmann, C.; Benner, A.; Meyer, J.; Von Deimling, A.; Weller, M.; Wick, W.; Weiler, M. Prognostic Value of Three Different Methods of MGMT Promoter Methylation Analysis in a Prospective Trial on Newly Diagnosed Glioblastoma. PLoS ONE 2012, 7, e33449. [Google Scholar] [CrossRef]
- Håvik, A.B.; Brandal, P.; Honne, H.; Dahlback, H.-S.S.; Scheie, D.; Hektoen, M.; Meling, T.R.; Helseth, E.; Heim, S.; Lothe, R.A.; et al. MGMT promoter methylation in gliomas-assessment by pyrosequencing and quantitative methylation-specific PCR. J. Transl. Med. 2012, 10, 36. [Google Scholar] [CrossRef] [Green Version]
- Jovanović, N.M.; Nikolov, V.; Vidović, N.; Vitorović, J.; Cvetković, V.J.; Mitrović, T.; Jevtović-Stoimenov, T. Optimizing conditions for MGMT promoter methylation status analysis in glioblastoma FFPE samples. Biol. Nyssana 2020, 11, 139–147. [Google Scholar] [CrossRef]
- Rezvani, N.; Alibakhshi, R.; Vaisi-Raygani, A.; Bashiri, H.; Saidijam, M. Detection of SPG20 gene promoter-methylated DNA, as a novel epigenetic biomarker, in plasma for colorectal cancer diagnosis using the MethyLight method. Oncol. Lett. 2017, 13, 3277–3284. [Google Scholar] [CrossRef] [Green Version]
- Pinson, H.; Hallaert, G.; Van der Meulen, J.; Dedeurwaerdere, F.; Vanhauwaert, D.; Van den Broecke, C.; Van Dorpe, J.; Van Roost, D.; Kalala, J.P.; Boterberg, T. Weak MGMT gene promoter methylation confers a clinically significant survival benefit in patients with newly diagnosed glioblastoma: A retrospective cohort study. J. Neuro-Oncol. 2020, 146, 55–62. [Google Scholar] [CrossRef]
- Mansouri, A.; Hachem, L.D.; Mansouri, S.; Nassiri, F.; Laperriere, N.J.; Xia, D.; Lindeman, N.I.; Wen, P.Y.; Chakravarti, A.; Mehta, M.P.; et al. MGMT promoter methylation status testing to guide therapy for glioblastoma: Refining the approach based on emerging evidence and current challenges. Neuro-Oncology 2019, 21, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Yoshioka, M.; Matsutani, T.; Hara, A.; Hirono, S.; Hiwasa, T.; Takiguchi, M.; Iwadate, Y. Real-time methylation-specific PCR for the evaluation of methylation status of MGMT gene in glioblastoma. Oncotarget 2018, 9, 27728–27735. [Google Scholar] [CrossRef] [Green Version]
- Jovanović, N.; Mitrović, T.; Cvetković, V.J.; Tošić, S.; Vitorović, J.; Stamenković, S.; Nikolov, V.; Kostić, A.; Vidović, N.; Krstić, M.; et al. The Impact of MGMT Promoter Methylation and Temozolomide Treatment in Serbian Patients with Primary Glioblastoma. Medicina 2019, 55, 34. [Google Scholar] [CrossRef] [Green Version]
- Jovanović, N.; Mitrovic, T.; Cvetković, V.J.; Tošić, S.; Vitorović, J.; Stamenković, S.; Nikolov, V.; Kostić, A.; Vidović, N.; Jevtović-Stoimenov, T.; et al. Prognostic significance of MGMT promoter methylation in diffuse glioma patients. Biotechnol. Biotechnol. Equip. 2019, 33, 639–644. [Google Scholar] [CrossRef] [Green Version]
- Jovanović, N.; Lazarević, M.; Cvetković, V.J.; Nikolov, V.; Perić, J.K.; Ugrin, M.; Pavlović, S.; Mitrović, T. The Significance of MGMT Promoter Methylation Status in Diffuse Glioma. Int. J. Mol. Sci. 2022, 23, 13034. [Google Scholar] [CrossRef] [PubMed]
- Holmes, E.E.; Jung, M.; Meller, S.; Leisse, A.; Sailer, V.; Zech, J.; Mengdehl, M.; Garbe, L.-A.; Uhl, B.; Kristiansen, G.; et al. Performance Evaluation of Kits for Bisulfite-Conversion of DNA from Tissues, Cell Lines, FFPE Tissues, Aspirates, Lavages, Effusions, Plasma, Serum, and Urine. PLoS ONE 2014, 9, e93933. [Google Scholar] [CrossRef] [Green Version]
- Dietrich, D.; Uhl, B.; Sailer, V.; Holmes, E.E.; Jung, M.; Meller, S.; Kristiansen, G. Improved PCR Performance Using Template DNA from Formalin-Fixed and Paraffin-Embedded Tissues by Overcoming PCR Inhibition. PLoS ONE 2013, 8, e77771. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
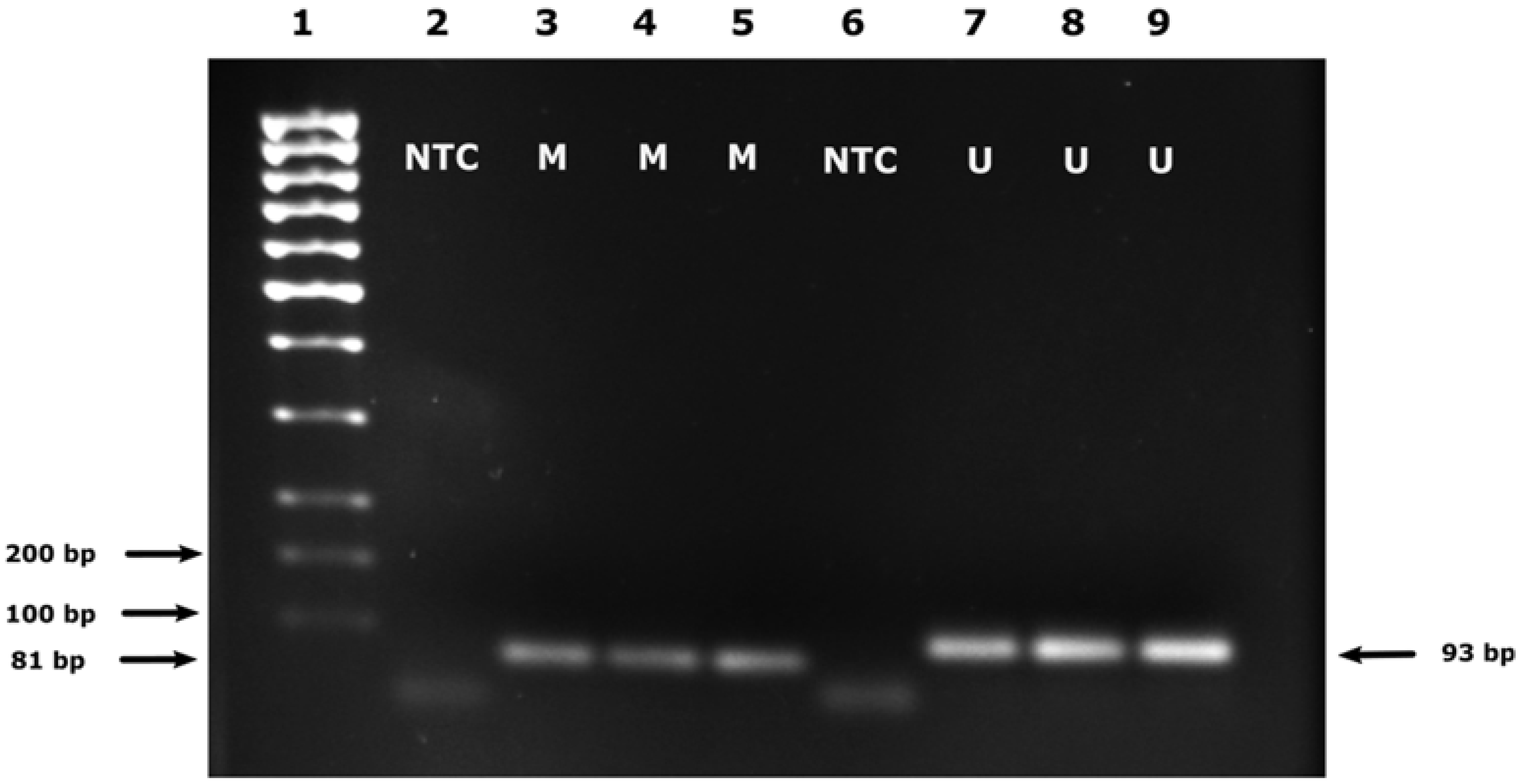
| Gene | Primer Sequence (5′-3′) | Amplicon Size (bp) | Reference |
|---|---|---|---|
| Unmethylated MGMT promoter (U) | F: TTTGTGTTTTGATGTTTGTAGGTTTTTGT R:AACTCCACACTCTTCCAAAAACAAAACA | 93 | [13] |
| Methylated MGMT promoter (M)) | F: TTTCGACGTTCGTAGGTTTTCGC R: GCACTCTTCCGAAAACGAAACG | 81 | [13] |
| Patient No | Diagnosis | IDH Mutation Status | WHO Grade | Conventional MSP (Semi-Quantitative) 1 | qMSP (Quantitative) 2 | qMSP (Semi-Quantitative) 3 | |
|---|---|---|---|---|---|---|---|
| SF MGMT Methylation Status | FFPE MGMT Methylation Status | SF MGMT Methylation Status | SF MGMT Methylation Status | ||||
| 1. | GBM | IDH1 wt 4 | 4 | 0 | N/A | 0 | 0 |
| 2. | GBM | IDH1 wt | 4 | 2 | N/A | 110.70 | 2 |
| 3. | GBM | IDH1 wt | 4 | 0 | 0 | 0 | 0 |
| 4. | GBM | IDH1 wt | 4 | 0 | N/A | 0 | 0 |
| 5. | GBM | IDH1 wt | 4 | 0 | 0 | 0 | 0 |
| 6. | GBM | IDH1 wt | 4 | 2 | N/A | 102.40 | 2 |
| 7. | GBM | IDH1 wt | 4 | 0 | N/A | 0 | 0 |
| 8. | GBM | IDH1 wt | 4 | 0 | N/A | 0 | 0 |
| 9. | GBM | IDH1 wt | 4 | 0 | 0 | 0 | 0 |
| 10. | rGBM 5 | IDH1 wt | 4 | 1 | 1 | 33.27 | 1 |
| 11. | GBM | IDH1 wt | 4 | 1 | 1 | 29.10 | 1 |
| 12. | GBM | IDH1 wt | 4 | 0 | 0 | 0 | 0 |
| 13. | GBM | IDH1 wt | 4 | 0 | 0 | 0 | 0 |
| 14. | GBM | IDH1 wt | 4 | 0 | 0 | 0 | 0 |
| 15. | GBM | IDH1 wt | 4 | 2 | 1 | 103.40 | 2 |
| 16. | GBM | IDH1 wt | 4 | 1 | 2 | 108.08 | 2 |
| 17. | GBM | IDH1 wt | 4 | 0 | 0 | 31.95 | 1 |
| 18. | GBM | IDH1 wt | 4 | 0 | N/A | 0 | 0 |
| 19. | GBM | IDH1 wt | 4 | 2 | 1 | 145.20 | 2 |
| 20. | GBM | IDH1 wt | 4 | 0 | 0 | 82.80 | 1 |
| 21. | GBM | IDH1 wt | 4 | 0 | 1 | 0 | 0 |
| 22. | GBM | IDH1 wt | 4 | 2 | 2 | 51.20 | 1 |
| 23. | rGBM | IDH1 wt | 4 | 1 | 1 | 51.06 | 1 |
| 24. | rGBM | IDH1 wt | 4 | 2 | 1 | 9.30 | 1 |
| 25. | Astrocytoma | IDH-R132H 6 | 3 | 2 | 2 | 145.30 | 2 |
| 26. | GBM | IDH1 wt | 4 | 0 | 0 | 0 | 0 |
| 27. | GBM | IDH1 wt | 4 | 0 | N/A | 0 | 0 |
| 28. | Astrocytoma | IDH-R132H | 3 | 2 | N/A | 0 | 0 |
| 29. | GBM | IDH1 wt | 4 | 2 | 2 | 0 | 0 |
| 30. | GBM | IDH1 wt | 4 | 0 | N/A | 0 | 0 |
| 31. | Astrocytoma | IDH-R132H | 4 | 1 | N/A | 0 | 0 |
| 32. | GBM | IDH1 wt | 4 | 2 | N/A | 103.00 | 2 |
| 33. | GBM | IDH1 wt | 4 | 1 | N/A | 0 | 0 |
| 34. | GBM | IDH1 wt | 4 | 0 | N/A | 22.68 | 1 |
| Outcome of Semi-Quantitative MSP Test | MGMT Promoter Methylation Determined by qMSP | ||
|---|---|---|---|
| Positive | Negative | Raw Total | |
| Positive | 12 (80.0%) | 4 (21.1%) | 16 (47.1%) |
| Negative | 3 (20.0%) | 15 (78.9%) | 18 (52.9%) |
| Column total | 15 (44.11%) | 19 (55.89%) | 34 (100%) |
| Outcome of Semi-Quantitative MSP Test | MGMT Promoter Methylation Determined by qMSP | ||
|---|---|---|---|
| Positive | Negative | Raw Total | |
| Positive | 6 (85.7%) | 4 (14.8%) | 10 (29.4%) |
| Negative | 1 (14.3%) | 23 (85.2%) | 24 (70.6%) |
| Column total | 7 (20.58%) | 27 (79.42%) | 34 (100%) |
| No. Inspected | No. Matched | Percent | 95% CI | |
|---|---|---|---|---|
| 34 | 24 | 70.59 | (52.52, 84.90) | |
| MGMT promoter methylation score | Kappa | SE Kappa | Z | p value (vs. >0) |
| 0 | 0.585004 | 0.171499 | 3.41113 | 0.0003 |
| 1 | 0.280423 | 0.171499 | 1.63513 | 0.0510 |
| 2 | 0.607843 | 0.171499 | 3.54430 | 0.0002 |
| Overall | 0.509025 | 0.125059 | 4.07029 | 0.0000 |
| No. Inspected | No. Matched | Percent | 95% CI | |
|---|---|---|---|---|
| 20 | 14 | 70.00 | (45.72, 88.11) | |
| MGMT promoter methylation score | Kappa | SE Kappa | Z | p value (vs. >0) |
| 0 | 1.00000 | 0.223607 | 4.47214 | 0.0000 |
| 1 | 0.28571 | 0.223607 | 1.27775 | 0.1007 |
| 2 | 0.06250 | 0.223607 | 0.27951 | 0.3899 |
| Overall | 0.51613 | 0.163055 | 3.16537 | 0.0008 |
| No. Inspected | No. Matched | Percent | 95% CI | |
|---|---|---|---|---|
| 20 | 14 | 70.00 | (45.72, 88.11) | |
| MGMT promoter methylation score | Kappa | SE Kappa | Z | p value (vs. >0) |
| 0 | 0.699248 | 0.223607 | 3.12713 | 0.0009 |
| 1 | 0.466667 | 0.223607 | 2.08700 | 0.0184 |
| 2 | 0.215686 | 0.223607 | 0.96458 | 0.1674 |
| Overall | 0.509202 | 0.168957 | 3.01380 | 0.0013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lazarević, M.; Jovanović, N.; Cvetković, V.J.; Tošić, S.; Vitorović, J.; Stamenković, S.; Nikolov, V.; Vidović, N.; Kostić Perić, J.; Jovanović, M.; et al. A Comparison of MGMT Testing by MSP and qMSP in Paired Snap-Frozen and Formalin-Fixed Paraffin-Embedded Gliomas. Diagnostics 2023, 13, 360. https://doi.org/10.3390/diagnostics13030360
Lazarević M, Jovanović N, Cvetković VJ, Tošić S, Vitorović J, Stamenković S, Nikolov V, Vidović N, Kostić Perić J, Jovanović M, et al. A Comparison of MGMT Testing by MSP and qMSP in Paired Snap-Frozen and Formalin-Fixed Paraffin-Embedded Gliomas. Diagnostics. 2023; 13(3):360. https://doi.org/10.3390/diagnostics13030360
Chicago/Turabian StyleLazarević, Milica, Nikola Jovanović, Vladimir J. Cvetković, Svetlana Tošić, Jelena Vitorović, Slaviša Stamenković, Vesna Nikolov, Nataša Vidović, Jelena Kostić Perić, Marija Jovanović, and et al. 2023. "A Comparison of MGMT Testing by MSP and qMSP in Paired Snap-Frozen and Formalin-Fixed Paraffin-Embedded Gliomas" Diagnostics 13, no. 3: 360. https://doi.org/10.3390/diagnostics13030360